
Substantial Sparing of Organs at Risk with Modern Proton Therapy in Lung Cancer, but Altered Breathing Patterns Can Jeopardize Target Coverage


 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Material and Clinical IMRT Planning
2.2. Proton Therapy Planning
2.3. Robustness Evaluation
2.4. Dosimetric Evaluation
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Breathing Motion
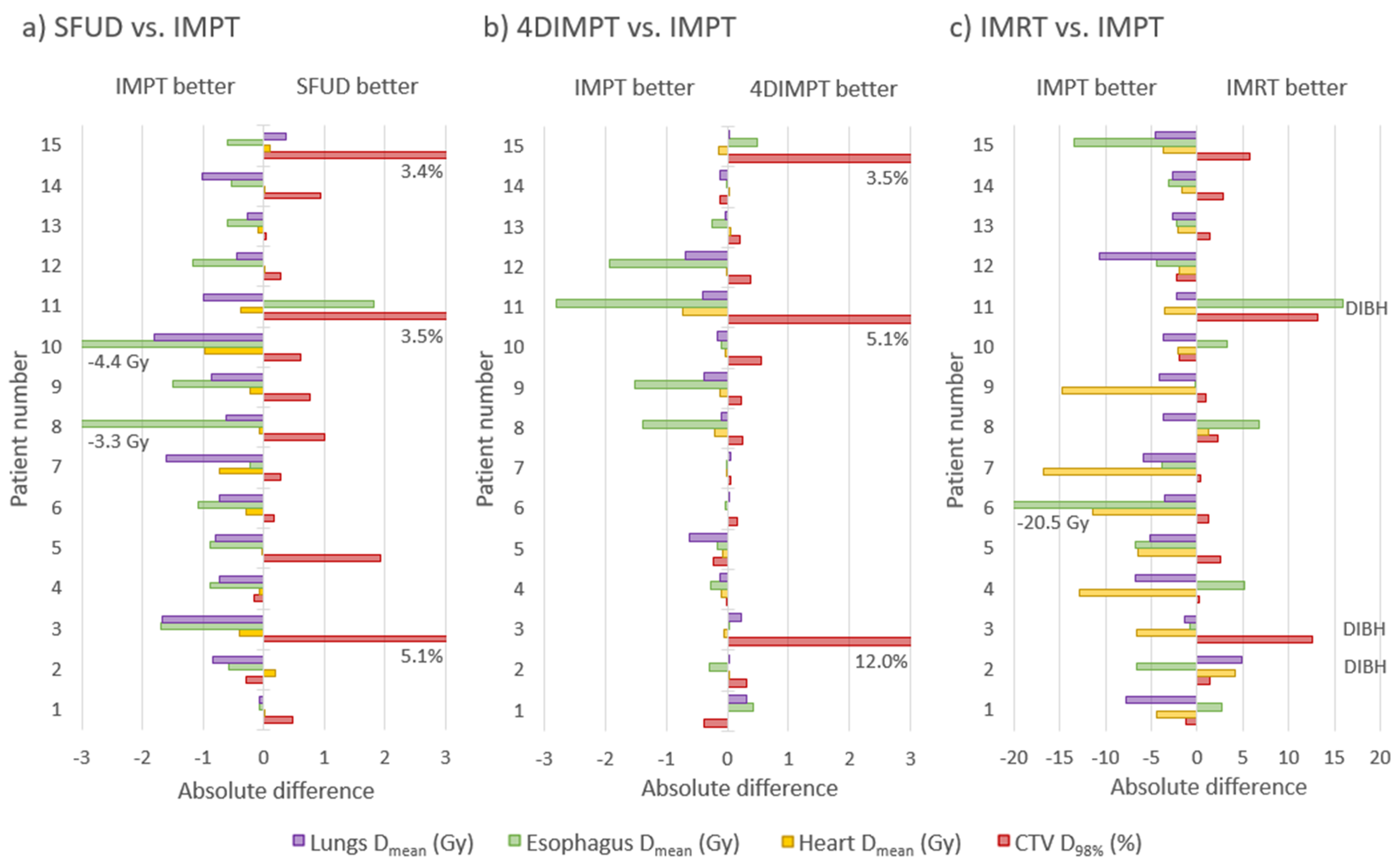
3.2. Target Coverage and OAR Sparing at Plan
3.3. Target Dose Robustness at Plan and Start
3.4. OAR Dose Robustness at Plan and Start
3.5. Target Coverage and OAR Sparing at Start
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ | Dose Constraint |
|---|---|
| Lungs | V5Gy < 65% V20Gy < 35% Dmean < 20 Gy |
| Esophagus | Dmean < 34 Gy |
| Heart | V30Gy < 40% |
| Spinal canal | Dmax < 50 Gy |
| Brachial plexus | Dmax < 66 Gy |
| Evaluations of | Evaluations at Plan | Evaluations at Start | Evaluation Criteria |
|---|---|---|---|
| Target coverage and OAR sparing at Plan | Plan AIP | CTV D98% > 95% CTV D2% < 107% Body D2cc < 107% OARs within constraints * | |
| Target dose robustness | Plan S/R Plan CT0/50 Plan Interplay | Start AIP Start CT0/50 | CTV D98% > 95% (90%) CTV D2% < 107% (110%) |
| OAR dose robustness | Plan S/R Plan CT0/50 Plan Interplay | Start AIP Start CT0/50 | Body D2cc < 107% (110%) OARs within constraints * |
| Target coverage and OAR sparing at Start | Start AIP | CTV D98% > 95% CTV D2% < 107% Body D2cc < 107% OARs within constraints * |
| Direction | Motion—Plan | Motion—Start |
|---|---|---|
| x (left–right) | 1 mm (0–5) | 1 mm (0–6) |
| y (anterior–posterior) | 2 mm (1–4) | 2 mm (1–4) |
| z (cranio–caudal) | 4 mm (1–15) | 4 mm (1–13) |
| Parameter | Evaluation | SFUD | 4DIMPT | IMPT |
|---|---|---|---|---|
| CTV D98% (%) | Plan CT0/50 | 97.5 (94.8–98.8) | 98.0 (97.0–99.0) | 97.8 (96.5–98.5) |
| Plan setup/range | 97.0 (95.6–97.7) | 97.2 (95.6–97.7) | 97.3 (95.1–98.1) | |
| Plan interplay | 93.6 (90.7–97.5) | 95.0 (93.5–97.0) | 94.6 (91.8–97.0) | |
| Start | 97.6 (85.3–98.8) | 97.6 (86.2–98.7) | 97.5 (81.8–98.2) | |
| Start CT0/50 | 97.4 (43.2–98.8) | 97.4 (61.3–98.9) | 97.1 (35.6–98.4) | |
| CTV D2% (%) | Plan CT0/50 | 102.2 (101.2–103.2) | 102.5 (102.0–103.5) | 102.5 (102.0–103.9) |
| Plan setup/range | 103.3 (102.2–104.5) | 103.2 (102.3–104.2) | 103.3 (102.5–105.5) | |
| Plan interplay | 104.9 (102.7–107.6) | 105.3 (103.2–107.5) | 105.5 (104.1–106.7) | |
| Start | 102.6 (101.4–104.4) | 102.8 (102.0–103.7) | 102.6 (101.8–103.7) | |
| Start CT0/50 | 102.3 (101.1–104.9) | 102.5 (102.0–104.0) | 102.5 (101.8–103.8) |
| Structure | Difference, Plan vs. Start | |||
|---|---|---|---|---|
| IMRT | SFUD | 4DIMPT | IMPT | |
| Lungs Dmean (Gy) | 1 (−6/20) | 0 (−11/20) | 0 (−11/33) | 0 (−12/32) |
| Lungs V5Gy (%) | −1 (−5/7) | −1 (−11/26) | −2 (−11/26) | −1 (−12/28) |
| Lungs V20Gy (%) | 1 (−7/29) | 3 (−13/30) | 2 (−10/30) | 3 (−11/31) |
| Heart Dmean (Gy) | −4 (−13/68) | −6 (−55/70) | −4 (−47/78) | −6 (−51/78) |
| Heart V30Gy (%) | 0 (−29/162) | 0 (−58/84) | 0 (−42/97) | 0 (−50/103) |
| Esophagus Dmean (Gy) | −3 (−17/28) | −5 (−27/30) | −4 (−31/31) | −4 (−31/35) |
| Spinal canal Dmax (Gy) | −1 (−9/6) | 1 (−14/6) | 0 (−16/9) | 1 (−21/8) |
| Body D2cc (Gy) | 0 (−2/6) | 0 (−1/4) | 0 (0/1) | 0 (−3/1) |
References
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-Term Results of NRG Oncology RTOG 0617: Standard-versus High-Dose Chemoradiotherapy with or without Cetuximab for Unresectable Stage III Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Men, Y.; Feng, L.; Kang, J.; Sun, X.; Yuan, M.; Jiang, W.; Hui, Z. A Current Review of Dose-Escalated Radiotherapy in Locally Advanced Non-Small Cell Lung Cancer. Radiol. Oncol. 2019, 53, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjyshi, O.; Liao, Z. Proton Therapy for Locally Advanced Non-Small Cell Lung Cancer. Br. J. Radiol. 2020, 93, 20190378. [Google Scholar] [CrossRef] [PubMed]
- Ramella, S.; D’Angelillo, R.M. Proton Beam or Photon Beam Radiotherapy in the Treatment of Non-Small-Cell Lung Cancer. Lancet Oncol. 2020, 21, 873–875. [Google Scholar] [CrossRef]
- Chang, J.Y.; Zhang, X.; Wang, X.; Kang, Y.; Riley, B.; Bilton, S.; Mohan, R.; Komaki, R.; Cox, J.D. Significant Reduction of Normal Tissue Dose by Proton Radiotherapy Compared with Three-Dimensional Conformal or Intensity-Modulated Radiation Therapy in Stage I or Stage III Non–Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1087–1096. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Pan, X.; Xiaoqiang, L.; Mohan, R.; Komaki, R.; Cox, J.D.; Chang, J.Y. Intensity-Modulated Proton Therapy Reduces the Dose to Normal Tissue Compared with Intensity-Modulated Radiation Therapy or Passive Scattering Proton Therapy and Enables Individualized Radical Radiotherapy for Extensive Stage IIIB Non-Small-Cell Lung Cancer: A Virtual Clinical Study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 357–366. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.; Myoung Noh, J.; Lee, W.; Park, B.; Park, H.; Young Park, J.; Pyo, H. Proton Beam Therapy Reduces the Risk of Severe Radiation-Induced Lymphopenia during Chemoradiotherapy for Locally Advanced Non-Small Cell Lung Cancer: A Comparative Analysis of Proton versus Photon Therapy. Radiother. Oncol. 2021, 156, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Iwata, H.; Akita, K.; Yamaba, Y.; Kunii, E.; Takakuwa, O.; Yoshihara, M.; Hattori, Y.; Nakajima, K.; Hayashi, K.; Toshito, T.; et al. Concurrent Chemo-Proton Therapy Using Adaptive Planning for Unresectable Stage 3 Non-Small Cell Lung Cancer: A Phase 2 Study. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 1359–1367. [Google Scholar] [CrossRef]
- Chang, J.Y.; Verma, V.; Li, M.; Zhang, W.; Komaki, R.; Lu, C.; Allen, P.K.; Liao, Z.; Welsh, J.; Lin, S.H.; et al. Proton Beam Radiotherapy and Concurrent Chemotherapy for Unresectable Stage III Non–Small Cell Lung Cancer: Final Results of a Phase 2 Study. JAMA Oncol. 2017, 3, e172032. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.-N.; Ly, N.B.; Komaki, R.; Levy, L.B.; Gomez, D.R.; Chang, J.Y.; Allen, P.K.; Mehran, R.J.; Lu, C.; Gillin, M.; et al. Long-Term Outcomes after Proton Therapy, with Concurrent Chemotherapy, for Stage II–III Inoperable Non-Small Cell Lung Cancer. Radiother. Oncol. 2015, 115, 367–372. [Google Scholar] [CrossRef] [Green Version]
- Liao, Z.; Lee, J.J.; Komaki, R.; Gomez, D.R.; O’Reilly, M.S.; Fossella, F.V.; Blumenschein, G.R.; Heymach, J.V.; Vaporciyan, A.A.; Swisher, S.G.; et al. Bayesian Adaptive Randomization Trial of Passive Scattering Proton Therapy and Intensity-Modulated Photon Radiotherapy for Locally Advanced Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 1813–1822. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Xu, T.; Gomez, D.R.; Deng, W.; Wei, X.; Elhalawani, H.; Jin, H.; Guan, F.; Mirkovic, D.; Xu, Y.; et al. Patterns of Local-Regional Failure after Intensity Modulated Radiation Therapy or Passive Scattering Proton Therapy with Concurrent Chemotherapy for Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 123–131. [Google Scholar] [CrossRef]
- Gjyshi, O.; Xu, T.; Elhammali, A.; Boyce-Fappiano, D.; Chun, S.G.; Gandhi, S.; Lee, P.; Chen, A.B.; Lin, S.H.; Chang, J.Y.; et al. Toxicity and Survival after Intensity-Modulated Proton Therapy versus Passive Scattering Proton Therapy for NSCLC. J. Thorac. Oncol. 2021, 16, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Zhang, X.; Knopf, A.; Li, H.; Mori, S.; Dong, L.; Lu, H.-M.; Liu, W.; Badiyan, S.N.; Both, S.; et al. Consensus Guidelines for Implementing Pencil-Beam Scanning Proton Therapy for Thoracic Malignancies on Behalf of the PTCOG Thoracic and Lymphoma Subcommittee. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Meijers, A.; Knopf, A.-C.; Crijns, A.P.G.; Ubbels, J.F.; Niezink, A.G.H.; Langendijk, J.A.; Wijsman, R.; Both, S. Evaluation of Interplay and Organ Motion Effects by Means of 4D Dose Reconstruction and Accumulation. Radiother. Oncol. 2020, 150, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Jie, A.W.; Marignol, L. Pro-Con of Proton: Dosimetric Advantages of Intensity-Modulation over Passive Scatter for Thoracic Malignancies. Tech. Innov. Patient Support Radiat. Oncol. 2020, 15, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Paganetti, H.; Grassberger, C.; Sharp, G.C. Physics of Particle Beam and Hypofractionated Beam Delivery in NSCLC. Semin. Radiat. Oncol. 2021, 31, 162–169. [Google Scholar] [CrossRef]
- Selvaraj, J.; Uzan, J.; Baker, C.; Nahum, A. 4D Radiobiological Modelling of the Interplay Effect in Conventionally and Hypofractionated Lung Tumour IMRT. Br. J. Radiol. 2015, 88, 20140372. [Google Scholar] [CrossRef] [Green Version]
- Den Otter, L.A.; Anakotta, R.M.; Weessies, M.; Roos, C.T.G.; Sijtsema, N.M.; Muijs, C.T.; Dieters, M.; Wijsman, R.; Troost, E.G.C.; Richter, C.; et al. Investigation of Inter-fraction Target Motion Variations in the Context of Pencil Beam Scanned Proton Therapy in Non-small Cell Lung Cancer Patients. Med. Phys. 2020, 47, 3835–3844. [Google Scholar] [CrossRef] [PubMed]
- Møller, D.S.; Khalil, A.A.; Knap, M.M.; Hoffmann, L. Adaptive Radiotherapy of Lung Cancer Patients with Pleural Effusion or Atelectasis. Radiother. Oncol. 2014, 110, 517–522. [Google Scholar] [CrossRef]
- Kwint, M.; Conijn, S.; Schaake, E.; Knegjens, J.; Rossi, M.; Remeijer, P.; Sonke, J.-J.; Belderbos, J. Intra Thoracic Anatomical Changes in Lung Cancer Patients during the Course of Radiotherapy. Radiother. Oncol. 2014, 113, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Fredriksson, A.; Forsgren, A.; Hårdemark, B. Minimax Optimization for Handling Range and Setup Uncertainties in Proton Therapy: Minimax Optimization for Handling Uncertainties in Proton Therapy. Med. Phys. 2011, 38, 1672–1684. [Google Scholar] [CrossRef] [PubMed]
- Engwall, E.; Fredriksson, A.; Glimelius, L. 4D Robust Optimization Including Uncertainties in Time Structures Can Reduce the Interplay Effect in Proton Pencil Beam Scanning Radiation Therapy. Med. Phys. 2018, 45, 4020–4029. [Google Scholar] [CrossRef] [Green Version]
- Ge, S.; Wang, X.; Liao, Z.; Zhang, L.; Sahoo, N.; Yang, J.; Guan, F.; Mohan, R. Potential for Improvements in Robustness and Optimality of Intensity-Modulated Proton Therapy for Lung Cancer with 4-Dimensional Robust Optimization. Cancers 2019, 11, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teoh, S.; Fiorini, F.; George, B.; Vallis, K.A.; Van den Heuvel, F. Proton vs Photon: A Model-Based Approach to Patient Selection for Reduction of Cardiac Toxicity in Locally Advanced Lung Cancer. Radiother. Oncol. 2020, 152, 151–162. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Yang, J.; Liao, Z.; Chen, J.; Xu, C.; He, X.; Zhang, X.; Zhu, R.X.; Li, H. Anatomic Change over the Course of Treatment for Non–Small Cell Lung Cancer Patients and Its Impact on Intensity-Modulated Radiation Therapy and Passive-Scattering Proton Therapy Deliveries. Radiat. Oncol 2020, 15, 55. [Google Scholar] [CrossRef]
- Ribeiro, C.O.; Visser, S.; Korevaar, E.W.; Sijtsema, N.M.; Anakotta, R.M.; Dieters, M.; Both, S.; Langendijk, J.A.; Wijsman, R.; Muijs, C.T.; et al. Towards the Clinical Implementation of Intensity-Modulated Proton Therapy for Thoracic Indications with Moderate Motion: Robust Optimised Plan Evaluation by Means of Patient and Machine Specific Information. Radiother. Oncol. 2021, 157, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, L.; Alber, M.; Jensen, M.F.; Holt, M.I.; Møller, D.S. Adaptation Is Mandatory for Intensity Modulated Proton Therapy of Advanced Lung Cancer to Ensure Target Coverage. Radiother. Oncol. 2017, 122, 400–405. [Google Scholar] [CrossRef]
- Kong, F.-M.; Ritter, T.; Quint, D.J.; Senan, S.; Gaspar, L.E.; Komaki, R.U.; Hurkmans, C.W.; Timmerman, R.; Bezjak, A.; Bradley, J.D.; et al. Consideration of Dose Limits for Organs at Risk of Thoracic Radiotherapy: Atlas for Lung, Proximal Bronchial Tree, Esophagus, Spinal Cord, Ribs, and Brachial Plexus. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 1442–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feuvret, L.; Noël, G.; Mazeron, J.-J.; Bey, P. Conformity Index: A Review. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.B.; Bentzen, S.M.; Deasy, J.O.; Kong, F.-M.; Bradley, J.D.; Vogelius, I.S.; El Naqa, I.; Hubbs, J.L.; Lebesque, J.V.; Timmerman, R.D.; et al. Radiation Dose–Volume Effects in the Lung. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S70–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- Atkins, K.M.; Rawal, B.; Chaunzwa, T.L.; Lamba, N.; Bitterman, D.S.; Williams, C.L.; Kozono, D.E.; Baldini, E.H.; Chen, A.B.; Nguyen, P.L.; et al. Cardiac Radiation Dose, Cardiac Disease, and Mortality in Patients with Lung Cancer. J. Am. Coll. Cardiol. 2019, 73, 2976–2987. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, M.; Sun, J.; Jiang, S.; Wang, L.; Wang, X.; Sahoo, N.; Gunn, G.B.; Frank, S.J.; Nguyen, Q.-N.; et al. Lyman–Kutcher–Burman Normal Tissue Complication Probability Modeling for Radiation-Induced Esophagitis in Non-Small Cell Lung Cancer Patients Receiving Proton Radiotherapy. Radiother. Oncol. 2020, 146, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Widder, J.; van Dijk, L.V.; Takegawa, H.; Koizumi, M.; Takashina, M.; Usui, K.; Kurokawa, C.; Sugimoto, S.; Saito, A.I.; et al. Limited Impact of Setup and Range Uncertainties, Breathing Motion, and Interplay Effects in Robustly Optimized Intensity Modulated Proton Therapy for Stage III Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Møller, D.S.; Holt, M.I.; Alber, M.; Tvilum, M.; Khalil, A.A.; Knap, M.M.; Hoffmann, L. Adaptive Radiotherapy for Advanced Lung Cancer Ensures Target Coverage and Decreases Lung Dose. Radiother. Oncol. 2016, 121, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Van der Weide, L.; van Sörnsen de Koste, J.R.; Lagerwaard, F.J.; Vincent, A.; van Triest, B.; Slotman, B.J.; Senan, S. Analysis of Carina Position as Surrogate Marker for Delivering Phase-Gated Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1111–1117. [Google Scholar] [CrossRef]
- Kouwenberg, J.; Penninkhof, J.; Habraken, S.; Zindler, J.; Hoogeman, M.; Heijmen, B. Model Based Patient Pre-Selection for Intensity-Modulated Proton Therapy (IMPT) Using Automated Treatment Planning and Machine Learning. Radiother. Oncol. 2021, 158, 224–229. [Google Scholar] [CrossRef] [PubMed]



| IMRT | SFUD | 4DIMPT | IMPT | |||||
|---|---|---|---|---|---|---|---|---|
| Median (Range) | Mean Rank | Median (Range) | Mean Rank | Median (Range) | Mean Rank | Median (Range) | Mean Rank | |
| CTV D98% (%) | 98.6 (98.2–98.8) | 1.20 | 98 (97.4–98.8) | 2.93 | 98 (97.1–98.9) | 2.93 | 98 (97.1–98.7) | 2.93 |
| CTV D2% (%) | 102.2 (101.7–102.7) | 1.93 | 102.5 (101.5–103.0) | 2.13 | 102.6 (102–103.4) | 2.93 | 102.4 (102.2–103.9) | 3.00 |
| CTV CI | 0.41 (0.33–0.62) | 1.70 | 0.34 (0.26–0.53) | 3.33 | 0.34 (0.25–0.64) | 2.50 | 0.34 (0.26–0.61) | 2.47 |
| CTV HI | 0.036 (0.030–0.044) | 1.27 | 0.046 (0.027–0.051) | 2.53 | 0.047 (0.038–0.059) | 3.13 | 0.044 (0.036–0.068) | 3.07 |
| Body D2cc (Gy) | 67.5 (61.3–68.4) | 1.20 | 68.3 (61.1–69.0) | 2.47 | 68.1 (62.1–69.7) | 3.07 | 68.5 (61.9–69.4) | 3.27 |
| Lungs Dmean (Gy) | 13.6 (6.6–16.8) | 3.93 | 10.2 (4.5–14.5) * | 2.87 | 9.6 (4.1–13.2) | 1.87 | 9.2 (4.5–13.1) | 1.33 |
| Lungs V5Gy (%) | 54.9 (31.8–63.2) | 4.00 | 28.3 (14.0–41.9) | 2.47 | 27.5 (13.1–41.6) | 2.00 | 27.6 (13.7–40.9) | 1.53 |
| Lungs V20Gy (%) | 22.6 (9.6–30.6) | 3.80 | 19.0 (9.0–29.0) * | 2.93 | 18.0 (8.2–25.1) | 1.93 | 17.6 (8.8–25.5) | 1.33 |
| Heart Dmean (Gy) | 8.1 (0.9- 20.7) | 4.00 | 2.8 (0.5–10.1) | 2.53 | 2.8 (0.5–10.0) | 1.93 | 2.8 (0.5–10.0) | 1.53 |
| Heart V30Gy (%) | 8.6 (0.0–28.2) | 3.90 | 3.2 (0.0–13.7) | 2.30 | 3.3 (0.9–13.9) | 2.37 | 3.3 (0.0–13.7) | 1.43 |
| Esophagus Dmean (Gy) | 20.4 (14.1–32.2) | 3.33 | 20.0 (10.0–30.8) * | 3.00 | 19.5 (8.9–31.8) | 2.27 | 20.0 (9.0–29.9) | 1.40 |
| Spinal Canal Dmax (Gy) | 46.0 (31.8–53.9) | 4.00 | 32.3 (18.8–41.1) | 2.40 | 31.4 (20.6–40.3) | 2.00 | 32.5 (12.8–39.6) | 1.60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boer, C.G.; Fjellanger, K.; Sandvik, I.M.; Ugland, M.; Engeseth, G.M.; Hysing, L.B. Substantial Sparing of Organs at Risk with Modern Proton Therapy in Lung Cancer, but Altered Breathing Patterns Can Jeopardize Target Coverage. Cancers 2022, 14, 1365. https://doi.org/10.3390/cancers14061365
Boer CG, Fjellanger K, Sandvik IM, Ugland M, Engeseth GM, Hysing LB. Substantial Sparing of Organs at Risk with Modern Proton Therapy in Lung Cancer, but Altered Breathing Patterns Can Jeopardize Target Coverage. Cancers. 2022; 14(6):1365. https://doi.org/10.3390/cancers14061365
Chicago/Turabian StyleBoer, Camilla Grindeland, Kristine Fjellanger, Inger Marie Sandvik, Maren Ugland, Grete May Engeseth, and Liv Bolstad Hysing. 2022. "Substantial Sparing of Organs at Risk with Modern Proton Therapy in Lung Cancer, but Altered Breathing Patterns Can Jeopardize Target Coverage" Cancers 14, no. 6: 1365. https://doi.org/10.3390/cancers14061365
APA StyleBoer, C. G., Fjellanger, K., Sandvik, I. M., Ugland, M., Engeseth, G. M., & Hysing, L. B. (2022). Substantial Sparing of Organs at Risk with Modern Proton Therapy in Lung Cancer, but Altered Breathing Patterns Can Jeopardize Target Coverage. Cancers, 14(6), 1365. https://doi.org/10.3390/cancers14061365