
Amino Acid Solutions for 177Lu-Oxodotreotide Premedication: A Tolerance Study

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
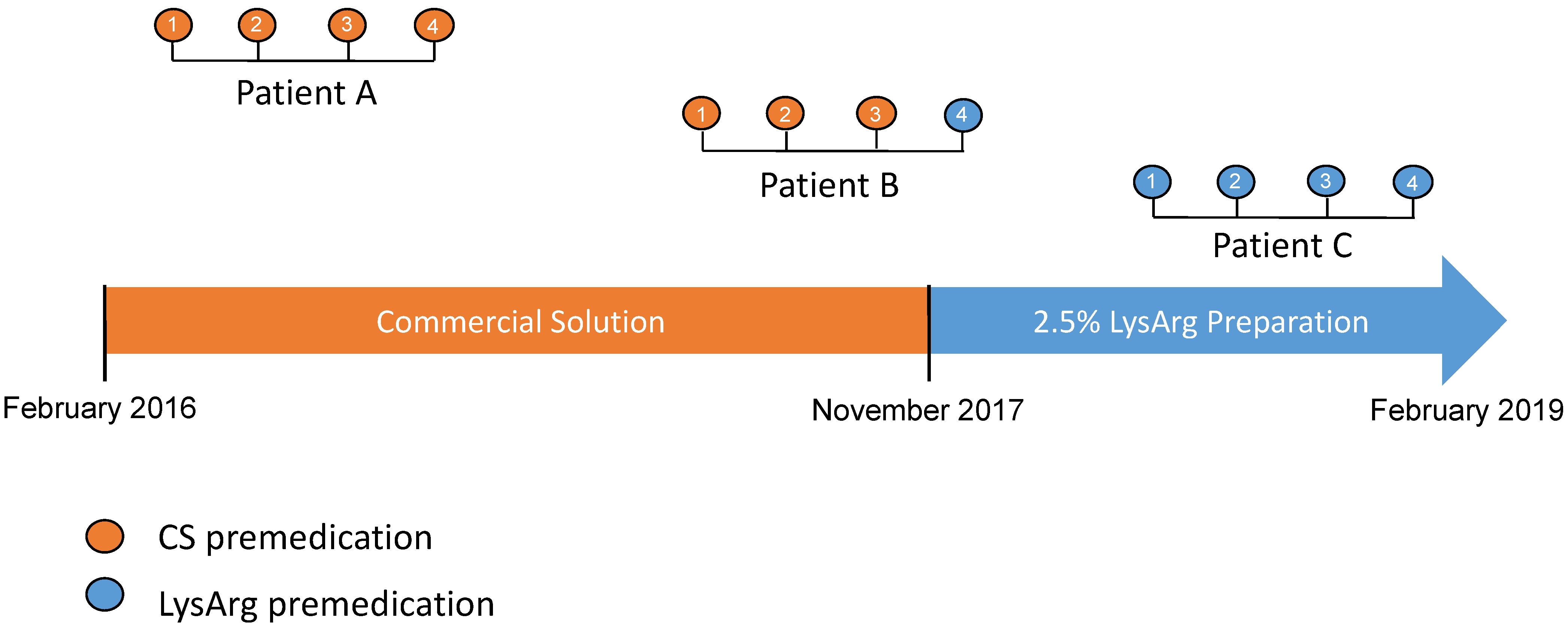
2.1. Patients
2.2. Data Collection
2.3. Assessment of Adverse Events
2.4. Amino acid Composition
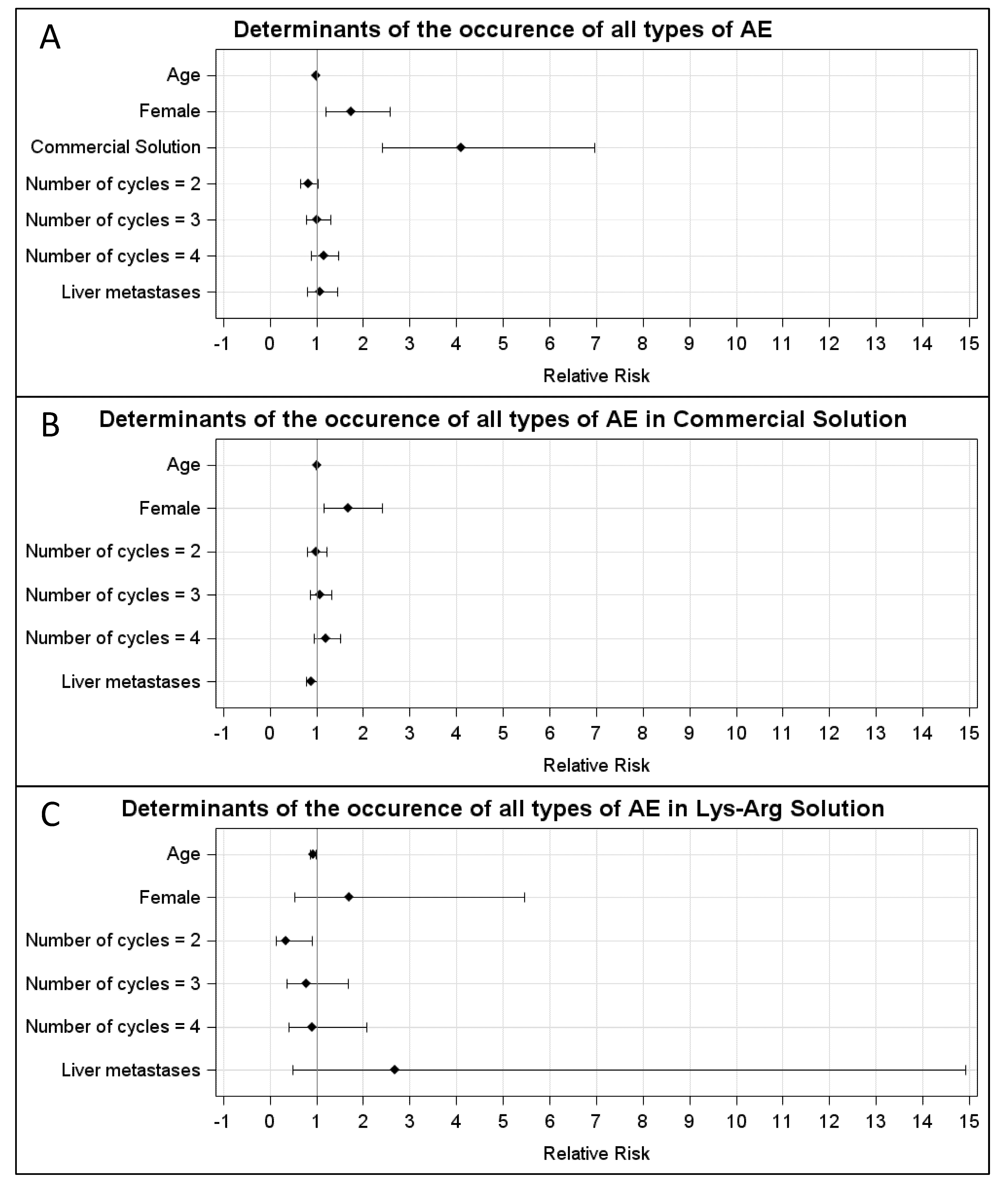
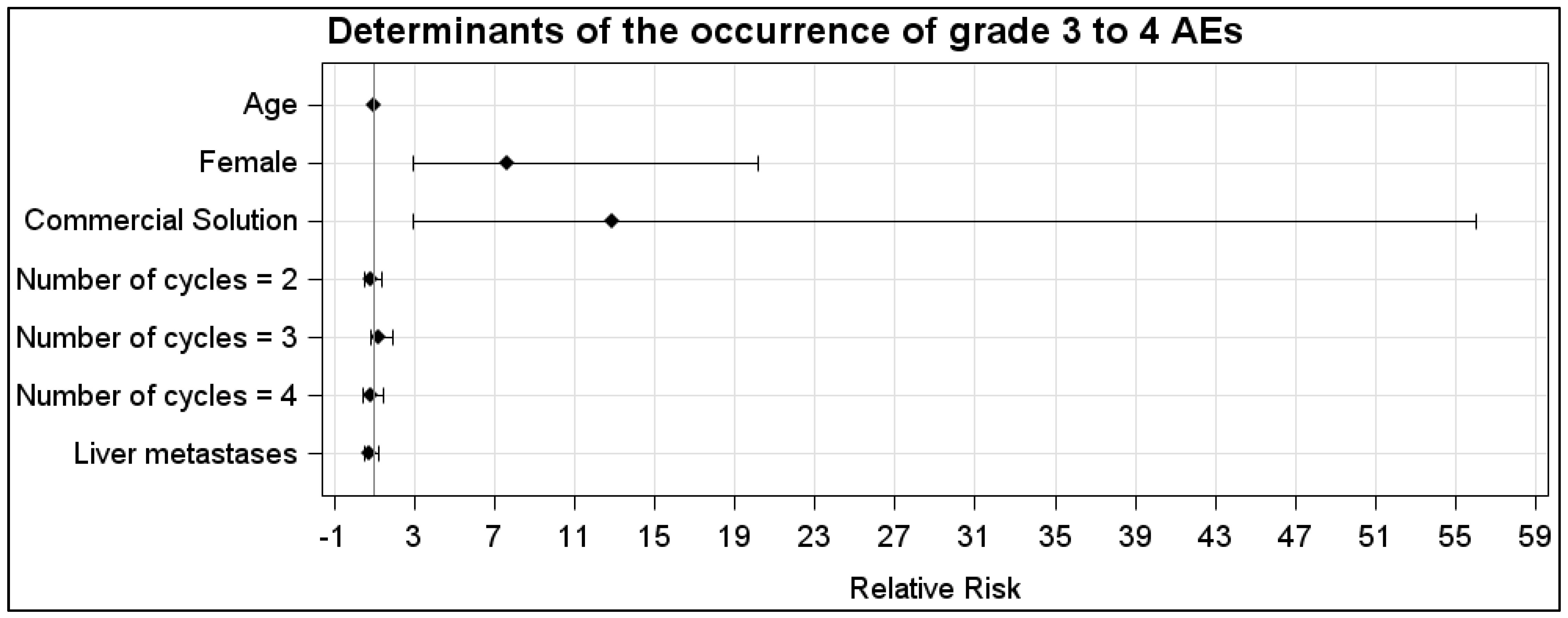
2.5. Data Analysis
3. Results
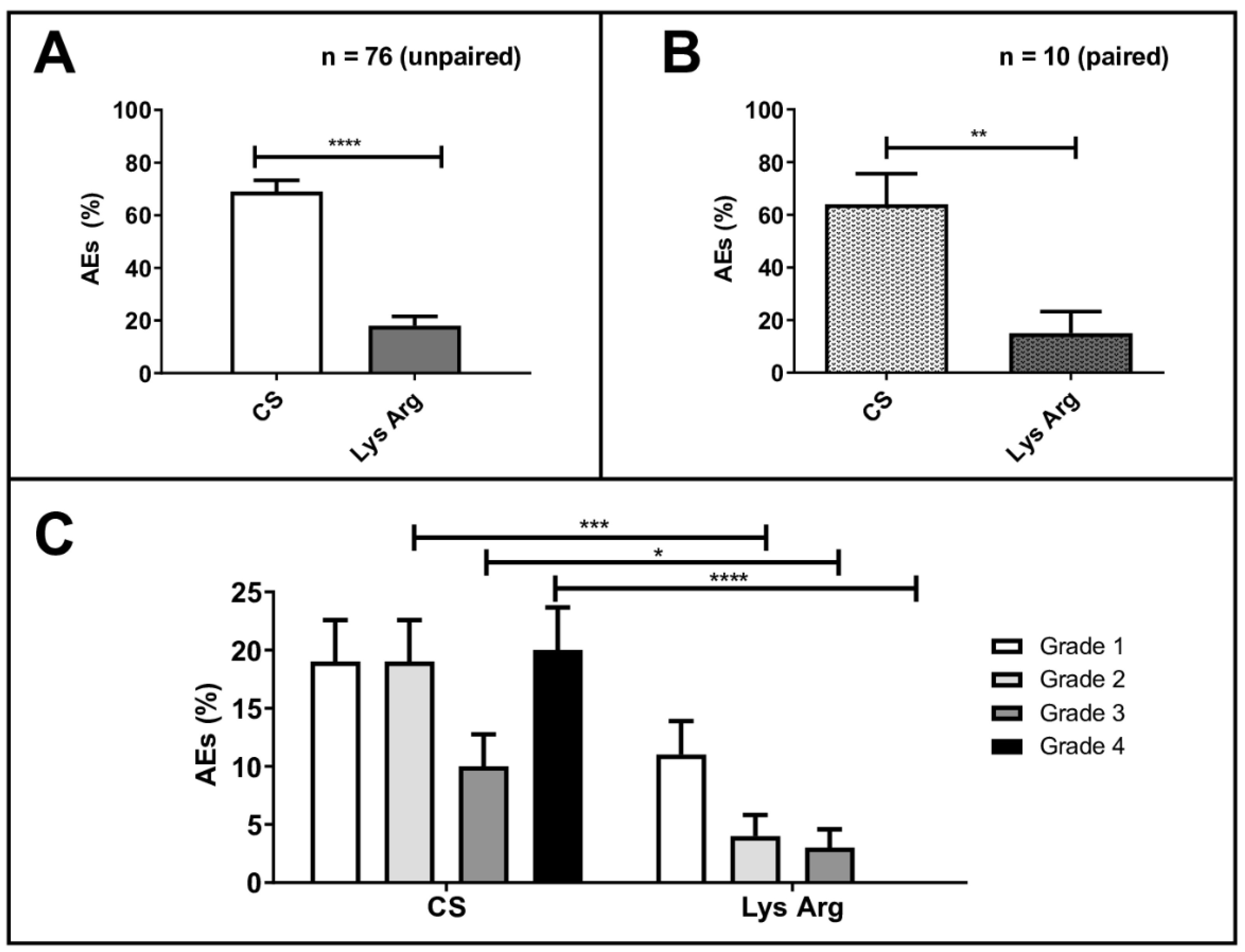
3.1. Adverse Events
3.2. Paraclinical Parameters
3.3. Antiemetic Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hallet, J.; Law, C.H.L.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the Rising Incidence of Neuroendocrine Tumors: A Population-Based Analysis of Epidemiology, Metastatic Presentation, and Outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- De Mestier, L.; Lepage, C.; Baudin, E.; Coriat, R.; Courbon, F.; Couvelard, A.; Do Cao, C.; Frampas, E.; Gaujoux, S.; Gincul, R.; et al. Digestive Neuroendocrine Neoplasms (NEN): French Intergroup Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up (SNFGE, GTE, RENATEN, TENPATH, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO, SFR). Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2020, 52, 473–492. [Google Scholar] [CrossRef]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef]
- Kaderli, R.M.; Spanjol, M.; Kollár, A.; Bütikofer, L.; Gloy, V.; Dumont, R.A.; Seiler, C.A.; Christ, E.R.; Radojewski, P.; Briel, M.; et al. Therapeutic Options for Neuroendocrine Tumors: A Systematic Review and Network Meta-Analysis. JAMA Oncol. 2019, 5, 480. [Google Scholar] [CrossRef]
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Busam, K.J.; de Krijger, R.R.; Dietel, M.; El-Naggar, A.K.; et al. A Common Classification Framework for Neuroendocrine Neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) Expert Consensus Proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. The WHO Classification of Tumours Editorial Board The 2019 WHO Classification of Tumours of the Digestive System. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Hicks, R.J.; Kwekkeboom, D.J.; Krenning, E.; Bodei, L.; Grozinsky-Glasberg, S.; Arnold, R.; Borbath, I.; Cwikla, J.; Toumpanakis, C.; Kaltsas, G.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Neoplasms: Peptide Receptor Radionuclide Therapy with Radiolabelled Somatostatin Analogues. Neuroendocrinology 2017, 105, 295–309. [Google Scholar] [CrossRef]
- Cives, M.; Strosberg, J.R. Gastroenteropancreatic Neuroendocrine Tumors. CA Cancer J. Clin. 2018, 68, 471–487. [Google Scholar] [CrossRef]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic Neuroendocrine Neoplasms: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Strosberg, J.R.; Caplin, M.E.; Kunz, P.L.; Ruszniewski, P.B.; Bodei, L.; Hendifar, A.; Mittra, E.; Wolin, E.M.; Yao, J.C.; Pavel, M.E.; et al. 177Lu-Dotatate plus Long-Acting Octreotide versus High-dose Long-Acting Octreotide in Patients with Midgut Neuroendocrine Tumours (NETTER-1): Final Overall Survival and Long-Term Safety Results from an Open-Label, Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 2021, 22, 1752–1763. [Google Scholar] [CrossRef]
- Lutathera, INN-Lutetium (177Lu) Oxodotreotide—European Medicines Agency—Assessment Report. 2017. Available online: https://www.ema.europa.eu/en/documents/assessment-report/lutathera-epar-public-assessment-report_en.pdf (accessed on 7 May 2020).
- WHO. WHO Handbook for Reporting Results of Cancer Treatment. WHO Offset Publication No. 48 Neoplasma; WHO: Geneva, Switzerland, 1980; Volume 20. [Google Scholar]
- Warr, D. Prognostic Factors for Chemotherapy Induced Nausea and Vomiting. Eur. J. Pharmacol. 2014, 722, 192–196. [Google Scholar] [CrossRef]
- Roila, F. Control of Acute Cisplatin-Lnduced Emesis over Repeat Courses of Chemotherapy. Oncology 1996, 53, 65–72. [Google Scholar] [CrossRef]
- Gielkens, H.A.; Lamers, C.B.; Masclee, A.A. Effect of Amino Acids on Lower Esophageal Sphincter Characteristics and Gastroesophageal Reflux in Humans. Dig. Dis. Sci. 1998, 43, 840–846. [Google Scholar] [CrossRef]
- McArthur, K.E.; Isenberg, J.I.; Hogan, D.L.; Dreier, S.J. Intravenous Infusion of L-Isomers of Phenylalanine and Tryptophan Stimulate Gastric Acid Secretion at Physiologic Plasma Concentrations in Normal Subjects and after Parietal Cell Vagotomy. J. Clin. Invest. 1983, 71, 1254–1262. [Google Scholar] [CrossRef]
- Rolleman, E.J.; Valkema, R.; de Jong, M.; Kooij, P.P.M.; Krenning, E.P. Safe and Effective Inhibition of Renal Uptake of Radiolabelled Octreotide by a Combination of Lysine and Arginine. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 9–15. [Google Scholar] [CrossRef]
- Barone, R.; Pauwels, S.; De Camps, J.; Krenning, E.P.; Kvols, L.K.; Smith, M.C.; Bouterfa, H.; Devuyst, O.; Jamar, F. Metabolic Effects of Amino Acid Solutions Infused for Renal Protection during Therapy with Radiolabelled Somatostatin Analogues. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2004, 19, 2275–2281. [Google Scholar] [CrossRef]
- Sartori, S.; Nielsen, I.; Pennacchio, G.; Pazzi, P.; Trevisani, L. Hyperkalaemia during Infusion of Hyperosmolar Amino Acid Solutions Enriched with Branched Chain Amino Acids. Report of Two Cases. Recenti Prog. Med. 1991, 82, 275–277. [Google Scholar]
- Pfob, C.H.; Eiber, M.; Luppa, P.; Maurer, F.; Maurer, T.; Tauber, R.; D’Alessandria, C.; Feuerecker, B.; Scheidhauer, K.; Ott, A.; et al. Hyperkalemia in Patients Treated with Endoradiotherapy Combined with Amino Acid Infusion Is Associated with Severe Metabolic Acidosis. EJNMMI Res. 2018, 8, 17. [Google Scholar] [CrossRef]
- Melis, M.; Krenning, E.P.; Bernard, B.F.; Barone, R.; Visser, T.J.; de Jong, M. Localisation and Mechanism of Renal Retention of Radiolabelled Somatostatin Analogues. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Jamar, F.; Barone, R.; Mathieu, I.; Walrand, S.; Labar, D.; Carlier, P.; de Camps, J.; Schran, H.; Chen, T.; Smith, M.C.; et al. 86Y-DOTA0)-D-Phe1-Tyr3-Octreotide (SMT487)—A Phase 1 Clinical Study: Pharmacokinetics, Biodistribution and Renal Protective Effect of Different Regimens of Amino Acid Co-Infusion. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Hammond, P.J.; Wade, A.F.; Gwilliam, M.E.; Peters, A.M.; Myers, M.J.; Gilbey, S.G.; Bloom, S.R.; Calam, J. Amino Acid Infusion Blocks Renal Tubular Uptake of an Indium-Labelled Somatostatin Analogue. Br. J. Cancer 1993, 67, 1437–1439. [Google Scholar] [CrossRef] [PubMed][Green Version]
- De Jong, M.; Rolleman, E.J.; Bernard, B.F.; Visser, T.J.; Bakker, W.H.; Breeman, W.A.; Krenning, E.P. Inhibition of Renal Uptake of Indium-111-DTPA-Octreotide in Vivo. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1996, 37, 1388–1392. [Google Scholar]
- Mogensen, C.E.; Sølling, K. Studies on Renal Tubular Protein Reabsorption: Partial and near Complete Inhibition by Certain Amino Acids. Scand. J. Clin. Lab. Invest. 1977, 37, 477–486. [Google Scholar] [CrossRef]
- Behr, T.M.; Goldenberg, D.M.; Becker, W. Reducing the Renal Uptake of Radiolabeled Antibody Fragments and Peptides for Diagnosis and Therapy: Present Status, Future Prospects and Limitations. Eur. J. Nucl. Med. 1998, 25, 201–212. [Google Scholar] [CrossRef]
- Krenning, E.P.; de Jong, M.; Kooij, P.P.; Breeman, W.A.; Bakker, W.H.; de Herder, W.W.; van Eijck, C.H.; Kwekkeboom, D.J.; Jamar, F.; Pauwels, S.; et al. Radiolabelled somatostatin analogue(s) for peptide receptor scintigraphy and radionuclide therapy. Ann. Oncol. 1999, 10, S23–S29. [Google Scholar] [CrossRef]
- Christensen, E.I.; Birn, H.; Verroust, P.; Moestrup, S.K. Megalin-Mediated Endocytosis in Renal Proximal Tubule. Ren. Fail. 1998, 20, 191–199. [Google Scholar] [CrossRef]
- Barone, R.; Van Der Smissen, P.; Devuyst, O.; Beaujean, V.; Pauwels, S.; Courtoy, P.J.; Jamar, F. Endocytosis of the Somatostatin Analogue, Octreotide, by the Proximal Tubule-Derived Opossum Kidney (OK) Cell Line. Kidney Int. 2005, 67, 969–976. [Google Scholar] [CrossRef]
- Gotthardt, M.; van Eerd-Vismale, J.; Oyen, W.J.G.; de Jong, M.; Zhang, H.; Rolleman, E.; Maecke, H.R.; Béhé, M.; Boerman, O. Indication for Different Mechanisms of Kidney Uptake of Radiolabeled Peptides. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 596–601. [Google Scholar] [CrossRef]
- Christensen, E.I.; Birn, H. Megalin and Cubilin: Multifunctional Endocytic Receptors. Nat. Rev. Mol. Cell Biol. 2002, 3, 256–266. [Google Scholar] [CrossRef]
- Ballatori, E.; Roila, F. Impact of Nausea and Vomiting on Quality of Life in Cancer Patients during Chemotherapy. Health Qual. Life Outcomes 2003, 1, 46. [Google Scholar] [CrossRef]
- Strosberg, J.; Wolin, E.; Chasen, B.; Kulke, M.; Bushnell, D.; Caplin, M.; Baum, R.P.; Kunz, P.; Hobday, T.; Hendifar, A.; et al. Health-Related Quality of Life in Patients with Progressive Midgut Neuroendocrine Tumors Treated with 177 Lu-Dotatate in the Phase III NETTER-1 Trial. J. Clin. Oncol. 2018, 36, 2578–2584. [Google Scholar] [CrossRef]
- Umar, R.M. Drug-Drug Interactions between Antiemetics Used in Cancer Patients. J. Oncol. Sci. 2018, 4, 142–146. [Google Scholar] [CrossRef]
- Strosberg, J.; Kunz, P.L.; Hendifar, A.; Yao, J.; Bushnell, D.; Kulke, M.H.; Baum, R.P.; Caplin, M.; Ruszniewski, P.; Delpassand, E.; et al. Impact of liver tumour burden, alkaline phosphatase elevation, and target lesion size on treatment outcomes with 177Lu-Dotatate: An analysis of the NETTER-1 study. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2372–2382. [Google Scholar] [CrossRef] [PubMed]
- Khatami, A.; Sistani, G.; Sutherland, D.E.K.; DeBrabandere, S.; Reid, R.H.; Laidley, D.T. Toxicity and Tolerability of 177Lu-DOTA-TATE PRRT with a Modified Administered Activity Protocol in NETs of Variable Origin—A Phase 2 Registry Study. Curr. Radiopharm. 2021, 14, 123–133. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Commercial Solution 10% | Lysine-Arginine 2.5% Preparation | |
|---|---|---|---|
| Amino Acid Composition (g/L) | L-Lysine | 11.00 | 25 |
| L-Arginine | 8.40 | 25 | |
| L-Isoleucine | 6.70 | - | |
| L-leucine | 10.00 | - | |
| L-Valine | 7.60 | - | |
| L-Methionine | 2.40 | - | |
| L-phenylalanine | 4.20 | - | |
| L-Threonine | 3.70 | - | |
| L-Tryptophan | 2.00 | - | |
| L-Histidine | 3.80 | - | |
| L-Alanine | 8.00 | - | |
| L-Aspartic acid | 6.00 | - | |
| L-Cysteine | 1.89 | - | |
| L-Glutamic Acid | 10.00 | - | |
| Glycine | 4.00 | - | |
| L-Proline | 3.00 | - | |
| L-Serine | 4.00 | - | |
| L-Tyrosine | 0.45 | - | |
| L-Ornithine hydrochloride | 3.18 | - | |
| L-Taurine | 0.60 | - | |
| Osmolarity (mOsm/L) | 780 | 420–480 | |
| Volume administered (L) | 2 | 1 | |
| Amino Acid Group | LysArg Preparation | Commercial Solution | Total |
|---|---|---|---|
| n patients | 46 | 40 | 76 |
| n cycles | 119 | 116 | 235 |
| Mean Age | 64 ± 9 | 65 ± 11 | 64 ± 10 |
| Gender M/F | 27/19 | 20/20 | 42/34 |
| Primary Tumor Site | LysArg Preparation | Commercial Solution | Total |
|---|---|---|---|
| Intestine | 32 (70%) | 30 (74%) | 62 (72%) |
| Pancreas | 7 (15%) | 6 (15%) | 13 (15%) |
| Bronchi | 3 (6.5%) | 2 (5%) | 5 (6%) |
| Rectum | 3 (6.5%) | 1 (2.5%) | 4 (5%) |
| Unknown | 1 (2%) | 1 (2.5%) | 2 (2%) |
| Adverse Events | LysArg Preparation | Commercial Solution | p-Value | Total |
|---|---|---|---|---|
| Nausea-vomiting | 13 (11%) | 70 (60.5%) | <0.001 | 83 |
| Flush | 6 (5%) | 3 (2.6%) | 0.50 | 9 |
| Diarrhea | 2 (2%) | 4 (3.4%) | 0.44 | 6 |
| Headache | 0 | 5 (4.5%) | 0.02 | 5 |
| Total | 21 (18%) | 82 (71%) | <0.001 | 103 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courault, P.; Deville, A.; Habouzit, V.; Gervais, F.; Bolot, C.; Bournaud, C.; Levigoureux, E. Amino Acid Solutions for 177Lu-Oxodotreotide Premedication: A Tolerance Study. Cancers 2022, 14, 5212. https://doi.org/10.3390/cancers14215212
Courault P, Deville A, Habouzit V, Gervais F, Bolot C, Bournaud C, Levigoureux E. Amino Acid Solutions for 177Lu-Oxodotreotide Premedication: A Tolerance Study. Cancers. 2022; 14(21):5212. https://doi.org/10.3390/cancers14215212
Chicago/Turabian StyleCourault, Pierre, Agathe Deville, Vincent Habouzit, Frédéric Gervais, Claire Bolot, Claire Bournaud, and Elise Levigoureux. 2022. "Amino Acid Solutions for 177Lu-Oxodotreotide Premedication: A Tolerance Study" Cancers 14, no. 21: 5212. https://doi.org/10.3390/cancers14215212
APA StyleCourault, P., Deville, A., Habouzit, V., Gervais, F., Bolot, C., Bournaud, C., & Levigoureux, E. (2022). Amino Acid Solutions for 177Lu-Oxodotreotide Premedication: A Tolerance Study. Cancers, 14(21), 5212. https://doi.org/10.3390/cancers14215212