Can We Efficiently Target HDAC in Cancer?



- (i)
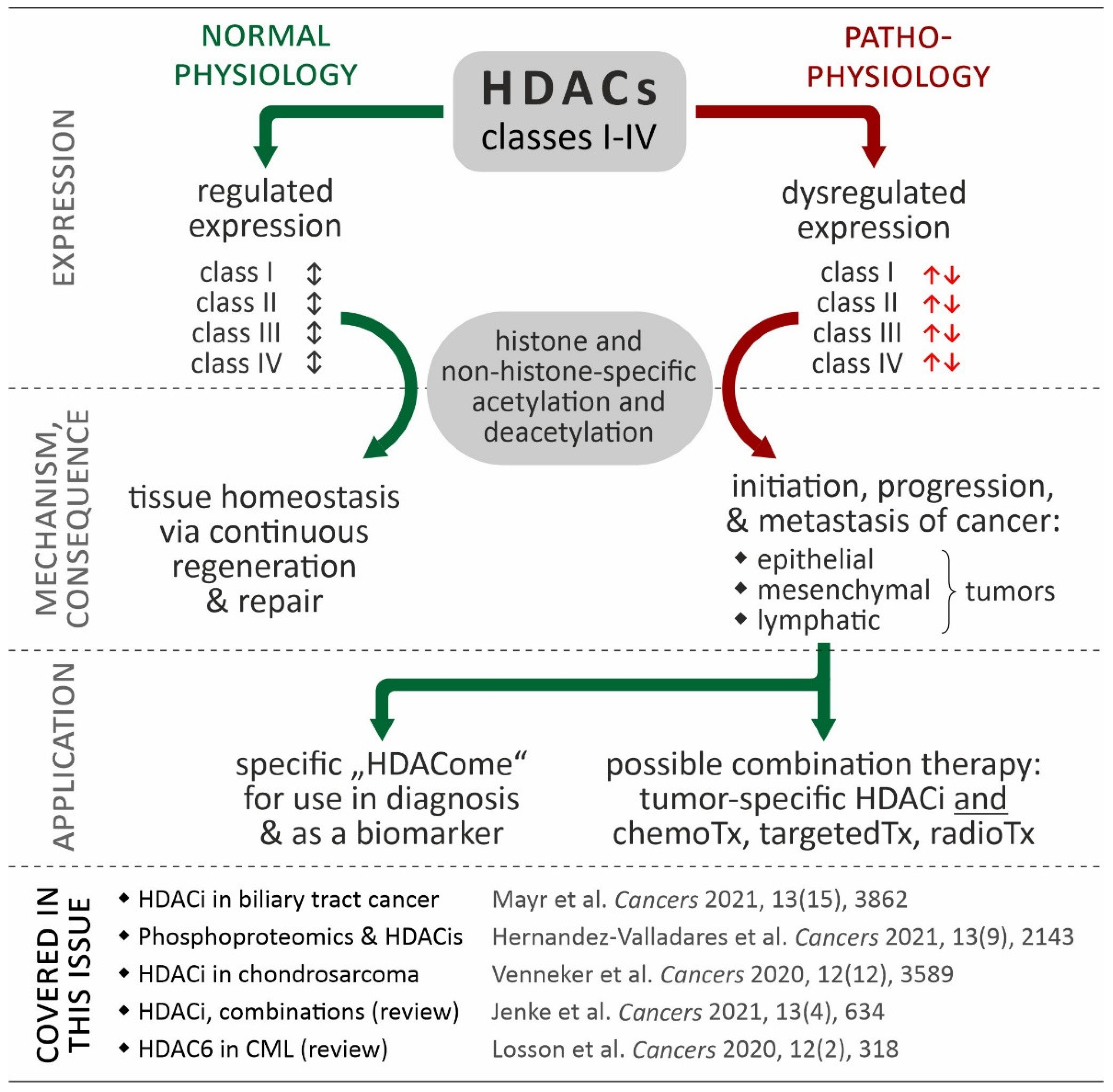
- Mayr et al. investigated the HDAC expression in biliary tract cancer (BTC) in relation to effects of HDAC inhibitors in-vitro (using established BTC cell lines) and to clinical endpoints in-situ (using BTC specimens). They could demonstrate that: (i) HDAC inhibition show a significant cytotoxic effect alone; and that (ii) especially the HDAC class I (HDACs 1, 2) inhibitor romidepsin could significantly augmented the cytotoxic effect of the standard chemotherapeutic cisplatin on the BTC cell lines. Furthermore, HDAC2 expression in human BTC specimen could be used as the diagnostic and prognostic biomarker. From this study, the conclusion could be that HDAC inhibition might be a promising combinatory drug approach in BTC as a cancer entity with dismal prognosis and that the tissue expression levels of HDACs seems to be an interesting biomarker in BTC [13].
- (ii)
- Maria Hernandez-Valladares et al. studied the in vivo proteomic/phosphoproteomic effects of all-trans retinoic acid (ATRA) and valproic acid (VP) on primary acute myeloid leukemia cells derived from patients before and during disease-stabilizing treatment. Prior to epigenetic therapy, the proteome and phosphoproteome profiling of the AML responders/non-responders cases revealed significant difference in processes of neutrophil degranulation/differentiation, M phase regulation and the interconversion of nucleotide di- and triphosphates (i.e., DNA synthesis and binding), as well as RNA metabolism and apoptosis. Treatment of AML cell lines with the combination of ATRA and VP leads to proteomic and phosphoproteomic modulation of DNA strand elongation, RNA processing, actin/cytoskeleton and cholesterol metabolism as well as GTPase/intracellular signaling in relation to results from AML responders and non-responders. Therefore, the authors suggested that proteomic and phosphoproteomic profiling can be applied as a predictive “tool” for identification of responders to ATRA/VP-based treatment [14].
- (iii)
- Sanne Venneker et al. investigated the changes of the methylome from IDH-mutant enchondroma towards high-grade chondrosarcoma in situ and performed an epigenetics and combinatory compound screening in chondrosarcoma cell lines in vitro, too. They could show that: (i) methylation is increased with the grading of IDH-mutant chondroid-derived neoplasm; and (ii) that chondrosarcoma cell lines were sensitive to HDAC inhibition in 2D and 3D in vitro models independent to their IDH mutation status. Detailed analysis with drug screenings revealed specific pro-apoptotic effects of class 1 HDAC inhibition on chondrosarcoma cells leading to synergistic effects in the combination with Bcl-2 family member inhibitors. Therefore, the authors concluded that combination therapies of specific HDAC inhibitors and small molecule inhibitors could be a promising strategy to improve therapeutic efficacy in chondrosarcoma [15].
- (iv)
- Robert Jenke et al. provided an up-to-date, comprehensive, and very structured overview of recent status and ongoing developments of HDAC inhibitors in the field of anticancer therapy. They summarized the molecular mechanisms of HDACi-linked anticancer effects to “classically” induce apoptosis and autophagy as well as senescence, whereby new insights on DNA damage, hormone signaling, and immune regulation by HDACi are presented. Regarding therapeutic aspects, the authors of this review display how combinatory approaches of HDACi with phosphoinositide 3-kinase-EGFR inhibitors and hormone or immunotherapy could improve therapeutic efficacy. Finally, very interesting developments regarding new bifunctional inhibitors as well as novel approaches for HDAC degradation via PROteolysis-TArgeting Chimeras (PROTACs) are discussed in detail. Based on the pre-clinical and clinical results of bifunctional HDAC inhibitors, the authors postulate that the upcoming concept of polypharmacy with HDACs is very promising for the field of cancer therapy [16].
- (v)
- Hélène Losson et al. focus in their review on the possible role of HDAC6 as a new and clinically relevant target in chronic myeloid leukemia (CML). First of all, the authors could definitively demonstrate the specific involvement of HDAC6 in human oncogenesis of human tumors via different mode of actions. Looking in detail at CML: (i) nuclear shuttling of HDAC6 with p53-HDAC6 interactions; (ii) the HDAC6 related acetylation status of HSP90 for degradation of BCR-ABL; and (iii) the overexpression of HDAC6 in CML stem cells make especially HDAC6 an interesting target in CML [17].
Author Contributions
Funding
Conflicts of Interest
References
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, M.A.; Kouzarides, T. Cancer epigenetics: From mechanism to therapy. Cell 2012, 150, 12–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Ropero, S.; Esteller, M. The role of histone deacetylases (HDACs) in human cancer. Mol. Oncol. 2007, 1, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Audia, J.E.; Campbell, R.M. Histone Modifications and Cancer. Cold Spring Harb. Perspect. Biol. 2016, 8, a019521. [Google Scholar] [CrossRef] [PubMed]
- Milazzo, G.; Mercatelli, D.; Di Muzio, G.; Triboli, L.; De Rosa, P.; Perini, G.; Giorgi, F.M. Histone Deacetylases (HDACs): Evolution, Specificity, Role in Transcriptional Complexes, and Pharmacological Actionability. Genes 2020, 11, 556. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Seto, E. HDACs and HDAC Inhibitors in Cancer Development and Therapy. Cold Spring Harb. Perspect. Med. 2016, 6, a026831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutt, D.M.; Roth, D.M.; Marchal, C.; Bouchecareilh, M. Using Histone Deacetylase Inhibitors to Analyze the Relevance of HDACs for Translation. Methods Mol. Biol. 2017, 1510, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Ganai, S.A. Histone Deacetylase Inhibitors Modulating Non-epigenetic Players: The Novel Mechanism for Small Molecule Based Therapeutic Intervention. Curr. Drug. Targets 2018, 19, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.C.S.; Chan, A.H.Y.; Ganesan, A. Thirty Years of HDAC Inhibitors: 2020 Insight and Hindsight. J. Med. Chem. 2020, 63, 12460–12484. [Google Scholar] [CrossRef] [PubMed]
- Gruber, W.; Peer, E.; Elmer, D.P.; Sternberg, C.; Tesanovic, S.; Del Burgo, P.; Coni, S.; Canettieri, G.; Neureiter, D.; Bartz, R.; et al. Targeting class I histone deacetylases by the novel small molecule inhibitor 4SC-202 blocks oncogenic hedgehog-GLI signaling and overcomes smoothened inhibitor resistance. Int. J. Cancer 2018, 142, 968–975. [Google Scholar] [CrossRef] [PubMed]
- Gomez, S.; Tabernacki, T.; Kobyra, J.; Roberts, P.; Chiappinelli, K.B. Combining epigenetic and immune therapy to overcome cancer resistance. Semin. Cancer Biol. 2020, 65, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Mayr, C.; Kiesslich, T.; Erber, S.; Bekric, D.; Dobias, H.; Beyreis, M.; Ritter, M.; Jager, T.; Neumayer, B.; Winkelmann, P.; et al. HDAC Screening Identifies the HDAC Class I Inhibitor Romidepsin as a Promising Epigenetic Drug for Biliary Tract Cancer. Cancers 2021, 13, 3862. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Valladares, M.; Wangen, R.; Aasebo, E.; Reikvam, H.; Berven, F.S.; Selheim, F.; Bruserud, O. Proteomic Studies of Primary Acute Myeloid Leukemia Cells Derived from Patients Before and during Disease-Stabilizing Treatment Based on All-Trans Retinoic Acid and Valproic Acid. Cancers 2021, 13, 2143. [Google Scholar] [CrossRef] [PubMed]
- Venneker, S.; Kruisselbrink, A.B.; Baranski, Z.; Palubeckaite, I.; Briaire-de Bruijn, I.H.; Oosting, J.; French, P.J.; Danen, E.H.J.; Bovee, J. Beyond the Influence of IDH Mutations: Exploring Epigenetic Vulnerabilities in Chondrosarcoma. Cancers 2020, 12, 3589. [Google Scholar] [CrossRef] [PubMed]
- Jenke, R.; Ressing, N.; Hansen, F.K.; Aigner, A.; Buch, T. Anticancer Therapy with HDAC Inhibitors: Mechanism-Based Combination Strategies and Future Perspectives. Cancers 2021, 13, 634. [Google Scholar] [CrossRef] [PubMed]
- Losson, H.; Schnekenburger, M.; Dicato, M.; Diederich, M. HDAC6-an Emerging Target Against Chronic Myeloid Leukemia? Cancers 2020, 12, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiesslich, T.; Neureiter, D. HDAC inhibitors in liver cancer: Which route to take? Expert Rev. Gastroenterol. Hepatol. 2019, 13, 515–517. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Rank | Tumor Entities | Tumor Stage | HDACi | Target (s) | Combinatory Drug Intervention | Phase | Identifier (NCT-): |
|---|---|---|---|---|---|---|---|
| 1 | Cervical cancer | A | Chidamide | class I, IIb | Toripalimab (PD-1 Inhibitor) | 1–2 | 04651127 |
| 2 | Solid tumors | A | JBI-802 | HDAC6 | 1–2 | 05268666 | |
| 3 | Breast and ovarian cancer | A/R | Belinostat | pan | Ribociclib (inhibitor of cyclin D1/CDK4 and CDK6) | 1 | 04315233 |
| 4 | Multiple myeloma | E | Citarinostat | AC6 | Hiltonol (immunostimulant), Lenalidomide (immune modulation), PVX-410 (multi-peptide vaccine) | 1 | 02886065 |
| 5 | Advanced solid tumors | A | Tinostamustine | class I | 1-2 | 03345485 | |
| 6 | Hematologic malignancies | R | 1 | 02576496 | |||
| 7 | NSCLC and esophageal carcinomas | A | Decitabine (a DNMTi), Tetrahydrouridine (inhibitor of cytidine deaminase) | n.a. | Pembrolizumab (PD-1 Inhibitor) | 1–2 | 03233724 |
| 8 | T-cell malignancies | R | Romidepsin | class I | Lenalidomide (immune modulation), 5-Aza (DNA methyltransferase inhibitor) | 1 | 04447027 |
| 9 | Follicular lymphoma | R | Abexinostat | pan | 2 | 03934567 | |
| 10 | Extrapulmonary neuroendocrine carcinoma | A | Chidamide | class I, IIb | Etoposide (DNA topoisomerase II-inhibitor), Cisplatin/ Carboplatin (DNA replication interfering) | 2 | 05076786 |
| 11 | Neuroendocrine neoplasm | A | Sintilimab (PD-1 inhibitor) | 2 | 05113355 | ||
| 12 | T-cell lymphoma | n.a. | 2 | 04512534 | |||
| 13 | Extranodal NK/T-cell Lymphoma | n.a. | 2 | 04994210 | |||
| 14 | Multiple myeloma | R | HG146 | 1 | 03710915 | ||
| 15 | Adult Ph-like ALL | n.a. | Chidamide | Dasatinib (tryosinkinase inhibitor) | 2–3 | 03564470 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiesslich, T.; Neureiter, D. Can We Efficiently Target HDAC in Cancer? Cancers 2022, 14, 4058. https://doi.org/10.3390/cancers14164058
Kiesslich T, Neureiter D. Can We Efficiently Target HDAC in Cancer? Cancers. 2022; 14(16):4058. https://doi.org/10.3390/cancers14164058
Chicago/Turabian StyleKiesslich, Tobias, and Daniel Neureiter. 2022. "Can We Efficiently Target HDAC in Cancer?" Cancers 14, no. 16: 4058. https://doi.org/10.3390/cancers14164058
APA StyleKiesslich, T., & Neureiter, D. (2022). Can We Efficiently Target HDAC in Cancer? Cancers, 14(16), 4058. https://doi.org/10.3390/cancers14164058