
Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma of the Tonsil versus Base of Tongue: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Criteria
2.2. Selection Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Search Results and Study Characteristics
3.2. Patient Characteristics
3.3. Margin Status
3.4. Recurrence
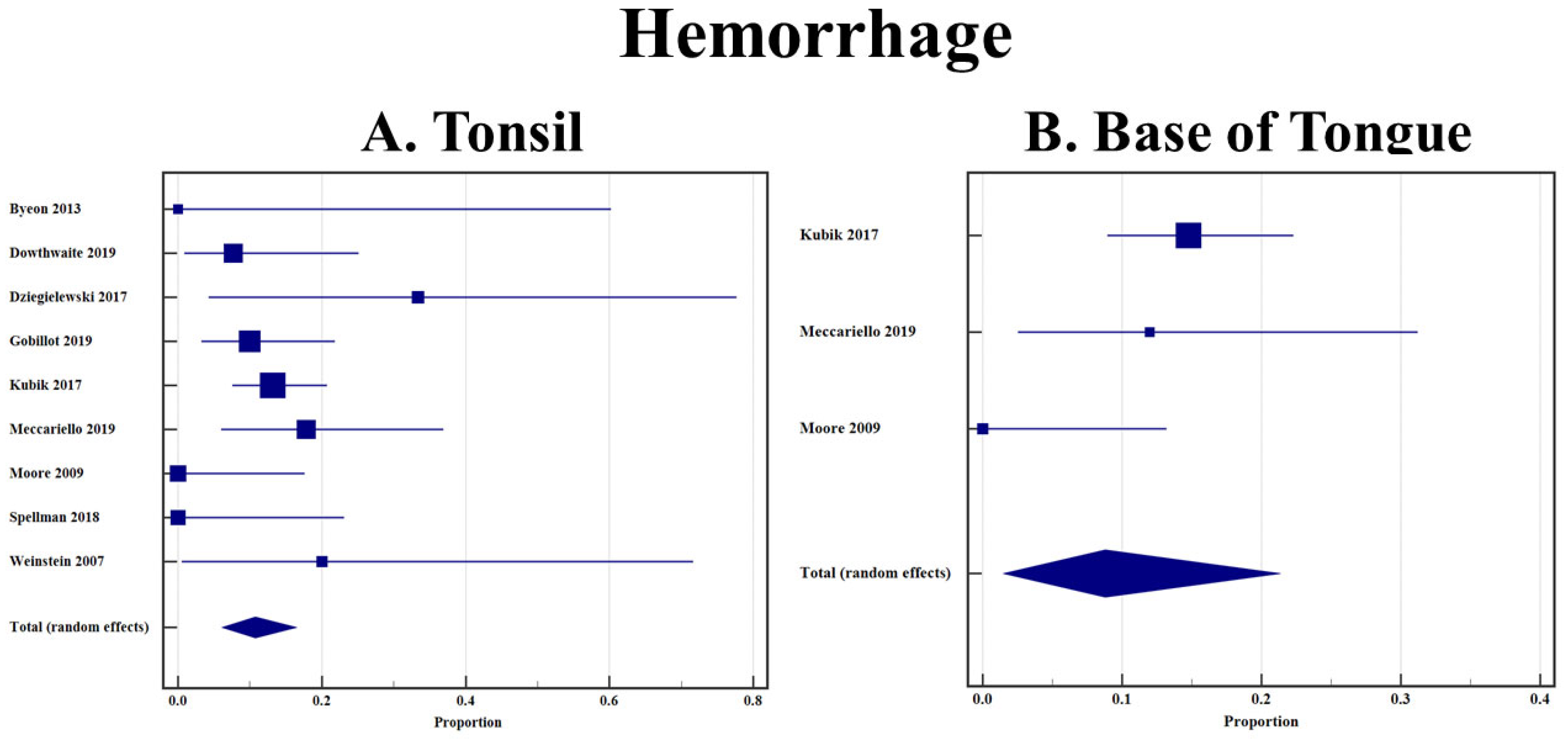
3.5. Hemorrhage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
Appendix A
PubMed (U.S. National Library of Medicine, National Institutes of Health) Search Strategy
- Filters/limits: none
- Date Searched: 28 February 2022
- # of records identified: 1007
Scopus (Elsevier) Search Strategy: (1062 Results)
- Filters/limits: none
- Date Searched: 28 February 2022
- # of records identified: 1062
CINAHL (EBSCOhost) Search Strategy: (286 Results)
- Filters/limits: none
- Date Searched: 28 February 2022
- # of records identified: 286
References
- Osazuwa-Peters, N.; Simpson, M.C.; Massa, S.T.; Boakye, E.A.; Antisdel, J.L.; Varvares, M.A. 40-year incidence trends for oropharyngeal squamous cell carcinoma in the United States. Oral Oncol. 2017, 74, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Craig, S.; Anderson, L.; Schache, A.; Moran, M.; Graham, L.; Currie, K.; Rooney, K.; Robinson, M.; Upile, N.S.; Brooker, R.; et al. Recommendations for determining HPV status in patients with oropharyngeal cancers under TNM8 guidelines: A two-tier approach. Br. J. Cancer 2019, 120, 827–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global burden of cancers attributable to infections in 2012: A synthetic analysis. Lancet Glob. Heal. 2016, 4, e609–e616. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, B.; Huang, S.H.; Su, J.; Garden, A.S.; Sturgis, E.M.; Dahlstrom, K.; Lee, N.; Riaz, N.; Pei, X.; A Koyfman, S.; et al. Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S): A multicentre cohort study. Lancet Oncol. 2016, 17, 440–451. [Google Scholar] [CrossRef]
- Dahlstrom, K.R.; Calzada, G.; Hanby, J.D.; Garden, A.S.; Glisson, B.S.; Li, G.; Roberts, D.B.; Weber, R.S.; Sturgis, E.M. An Evolution in Demographics, Treatment, and Outcomes of Oropharyngeal Cancer at a Major Cancer Center: A Staging System in Need of Repair. Cancer 2013, 119, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.H.; Xu, W.; Waldron, J.; Siu, L.; Shen, X.; Tong, L.; Ringash, J.; Bayley, A.; Kim, J.; Hope, A.; et al. Refining American Joint Committee on Cancer/Union for International Cancer Control TNM Stage and Prognostic Groups for Human Papillomavirus–Related Oropharyngeal Carcinomas. J. Clin. Oncol. 2015, 33, 836–845. [Google Scholar] [CrossRef]
- Bauwens, L.; Baltres, A.; Fiani, D.-J.; Zrounba, P.; Buiret, G.; Fleury, B.; Benzerdjeb, N.; Grégoire, V. Prevalence and distribution of cervical lymph node metastases in HPV-positive and HPV-negative oropharyngeal squamous cell carcinoma. Radiother. Oncol. 2021, 157, 122–129. [Google Scholar] [CrossRef]
- Cracchiolo, J.R.; Baxi, S.S.; Morris, L.G.; Ganly, I.; Patel, S.G.; Cohen, M.A.; Roman, B.R. Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base. Cancer 2016, 122, 1523–1532. [Google Scholar] [CrossRef]
- Cracchiolo, J.R.; Roman, B.R.; Kutler, D.I.; Kuhel, W.I.; Cohen, M.A. Adoption of transoral robotic surgery compared with other surgical modalities for treatment of oropharyngeal squamous cell carcinoma. J. Surg. Oncol. 2016, 114, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Gross, N.D.; Holsinger, F.C.; Magnuson, J.S.; Duvvuri, U.; Genden, E.M.; Ghanem, T.A.; Yaremchuk, K.L.; Goldenberg, D.; Miller, M.C.; Moore, E.J.; et al. Robotics in Otolaryngology and Head and Neck Surgery: Recommendations for Training and Credentialing: A Report of the 2015 Ahns Education Committee, Aao-Hns Robotic Task Force and Aao-Hns Sleep Disorders Committee. Head Neck. 2016, 38, E151–E158. [Google Scholar] [CrossRef]
- Mercante, G.; Ruscito, P.; Pellini, R.; Cristalli, G.; Spriano, G. Transoral robotic surgery (TORS) for tongue base tumours. Acta Otorhinolaryngol. Ital. 2013, 33, 230–235. [Google Scholar]
- Persky, M.J.; Albergotti, W.G.; Rath, T.J.; Kubik, M.W.; Abberbock, S.; Geltzeiler, M.; Kim, S.; Duvvuri, U.; Ferris, R.L. Positive Margins by Oropharyngeal Subsite in Transoral Robotic Surgery for T1/T2 Squamous Cell Carcinoma. Otolaryngol. Head Neck Surg. 2018, 158, 660–666. [Google Scholar] [CrossRef]
- Geltzeiler, M.; Clayburgh, D.; Gleysteen, J.; Gross, N.D.; Hamilton, B.; Andersen, P.; Brickman, D. Predictors of extracapsular extension in HPV-associated oropharyngeal cancer treated surgically. Oral Oncol. 2017, 65, 89–93. [Google Scholar] [CrossRef]
- Howard, F.M.; Kochanny, S.; Koshy, M.; Spiotto, M.; Pearson, A.T. Machine Learning–Guided Adjuvant Treatment of Head and Neck Cancer. JAMA Netw. Open 2020, 3, e2025881. [Google Scholar] [CrossRef]
- Brandwein-Gensler, M.; Teixeira, M.S.; Lewis, C.M.; Lee, B.; Rolnitzky, L.; Hille, J.J.; Genden, E.; Urken, M.L.; Wang, B.Y. Oral Squamous Cell Carcinoma: Histologic Risk Assessment, but Not Margin Status, Is Strongly Predictive of Local Disease-Free and Overall Survival. Am. J. Surg. Pathol. 2005, 29, 167–178. [Google Scholar] [CrossRef]
- Moore, E.J.; Van Abel, K.M.; Price, D.L.; Lohse, C.M.; Olsen, K.D.; Jackson, R.; Martin, E.J. Transoral robotic surgery for oropharyngeal carcinoma: Surgical margins and oncologic outcomes. Head Neck 2018, 40, 747–755. [Google Scholar] [CrossRef]
- Viet, C.T.; Dierks, E.J.; Cheng, A.C.; Patel, A.A.; Chang, S.-C.; Couey, M.A.; Watters, A.L.; Hoang, T.; Xiao, H.D.; Crittenden, M.R.; et al. Transoral robotic surgery and neck dissection for HPV-positive oropharyngeal carcinoma: Importance of nodal count in survival. Oral Oncol. 2020, 109, 104770. [Google Scholar] [CrossRef]
- Molony, P.; Kharytaniuk, N.; Boyle, S.; Woods, R.S.R.; O’Leary, G.; Werner, R.; Heffron, C.; Feeley, L.; Sheahan, P. Impact of positive margins on outcomes of oropharyngeal squamous cell carcinoma according to p16 status. Head Neck 2017, 39, 1680–1688. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Oxford Centre for Evidence-Based Medicine. The Oxford Levels of Evidence 2. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 20 July 2021).
- Sally, G.; Higgins, J.P.T. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons: New York, NY, USA, 2011. [Google Scholar]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Freeman, M.F.; Tukey, J.W. Transformations Related to the Angular and the Square Root. Ann. Math. Stat. 1950, 21, 607–611. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Dowthwaite, S.; Panizza, B.; O’Neill, J.; Porceddu, S.; Jackson, J.E.; Chua, B. Outcomes of primary trans-oral surgical management of early tonsillar squamous cell carcinoma with risk-adapted adjuvant radiotherapy. Aust. J. Otolaryngol. 2019, 2, 7. [Google Scholar] [CrossRef]
- Dziegielewski, P.T.; Boyce, B.J.; Old, M.; Teknos, T.N.; Agrawal, A.; Patwa, H.; Ozer, E. Transoral robotic surgery for tonsillar cancer: Addressing the contralateral tonsil. Head Neck 2017, 39, 2224–2231. [Google Scholar] [CrossRef] [PubMed]
- Gobillot, T.; Kaka, A.S.; Patel, S.A.; Rodriguez, C.; Cannon, R.B.; Futran, N.D.; Houlton, J.J. Treatment of Tonsillar Carcinoma following Nononcologic Tonsillectomy: Efficacy of Transoral Robotic Revision Tonsillectomy. Otolaryngol. Neck Surg. 2018, 160, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Hirshoren, N.; Ruskin, O.; Fua, T.; Kleid, S.; Magarey, M.; Dixon, B. Transoral robotic surgery: Implementation as a tool in head and neck surgery — A single-centre Australian experience. ANZ J. Surg. 2016, 88, 1129–1134. [Google Scholar] [CrossRef]
- Kumar, A.; Laskar, S.G.; Thiagarajan, S. Is Transoral Robotic Surgery (Tors) for Oropharyngeal Squamous Cell Carcinoma Being Done More Often Than Actually Indicated? Head Neck 2021, 43, 1376–1377. [Google Scholar] [CrossRef]
- Olaleye, O.; Jeong, B.; Switajewski, M.; Ooi, E.H.; Krishnan, S.; Foreman, A.; Hodge, J.-C. Trans-oral robotic surgery for head and neck cancers using the Medrobotics Flex® system: The Adelaide cohort. J. Robot. Surg. 2021, 16, 527–536. [Google Scholar] [CrossRef]
- Spellman, J.; Sload, R.; Kim, P.; Martin, P.; Calzada, G. Staging Neck Dissection and Transoral Robotic Surgery Treatment Algorithm in Palatine Tonsil Cancer. Otolaryngol. Neck Surg. 2017, 158, 479–483. [Google Scholar] [CrossRef]
- Subramanian, H.; Park, H.S.; Barbieri, A.; Mahajan, A.; Judson, B.L.; Mehra, S.; Yarbrough, W.G.; Burtness, B.A.; Husain, Z.A. Pretreatment predictors of adjuvant chemoradiation in patients receiving transoral robotic surgery for squamous cell carcinoma of the oropharynx: A case control study. Cancers Head Neck 2016, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, G.S.; O’Malley, B.W., Jr.; Snyder, W.; Sherman, E.; Quon, H. Transoral Robotic Surgery: Radical Tonsillectomy. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 1220–1226. [Google Scholar] [CrossRef] [Green Version]
- Zebolsky, A.L.; George, E.; Gulati, A.; Wai, K.C.; Carpenter, P.; Van Zante, A.; Ha, P.K.; Heaton, C.M.; Ryan, W.R. Risk of Pathologic Extranodal Extension and Other Adverse Features After Transoral Robotic Surgery in Patients With HPV-Positive Oropharynx Cancer. JAMA Otolaryngol. Neck Surg. 2021, 147, 1080. [Google Scholar] [CrossRef]
- Gallitto, M.; Sindhu, K.; Wasserman, I.; De, B.; Gupta, V.; Miles, B.A.; Genden, E.M.; Posner, M.; Misiukiewicz, K.; Bakst, R.L. Trimodality Therapy for Oropharyngeal Cancer in the Tors Era: Is There a Cohort That May Benefit? Head Neck 2019, 41, 3009–3022. [Google Scholar] [CrossRef]
- Bu, D.D.; Ferrandino, R.; Ba, E.M.R.; Liu, S.; Miles, B.A.; Teng, M.S.; Yao, M.; Genden, E.M.; Chai, R.L. Lymph Node Ratio in HPV -Associated Oropharyngeal Cancer: Identification of a Prognostic Threshold. Laryngoscope 2020, 131, E184–E189. [Google Scholar] [CrossRef]
- Carey, R.M.; Brody, R.M.; Ba, D.S.; Shinn, J.R.; Mady, L.J.; Rajasekaran, K.; Cannady, S.B.; Lin, A.; Lukens, J.N.; Bauml, J.M.; et al. Locoregional Recurrence in p16-Positive Oropharyngeal Squamous Cell Carcinoma After TORS. Laryngoscope 2021, 131, E2865–E2873. [Google Scholar] [CrossRef]
- de Almeida, J.R.; Li, R.; Magnuson, J.S.; Smith, R.V.; Moore, E.; Lawson, G.; Remacle, M.; Ganly, I.; Kraus, D.H.; Teng, M.S.; et al. Oncologic Outcomes after Transoral Robotic Surgery: A Multi-Institutional Study. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 1043–1051. [Google Scholar] [CrossRef]
- Fradet, L.; Charters, E.; Gao, K.; Froggatt, C.; Palme, C.; Riffat, F.; Nguyen, K.; Wu, R.; Milross, C.; Clark, J.R. Avoidance of primary site adjuvant radiotherapy following transoral robotic surgery: A cohort study. ANZ J. Surg. 2022, 92, 511–517. [Google Scholar] [CrossRef]
- Funk, R.K.; Moore, E.J.; García, J.J.; Ms, W.S.H.; Stoddard, D.G.; Vencio, E.F.; Foote, R.L.; Price, K.A.; Ma, D.J. Risk factors for locoregional relapse after transoral robotic surgery for human papillomavirus-related oropharyngeal squamous cell carcinoma. Head Neck 2015, 38, E1674–E1679. [Google Scholar] [CrossRef]
- Hobelmann, K.C.; Topf, M.C.; Bar-Ad, V.; Luginbuhl, A.J.; Keane, W.M.; Curry, J.M.; Cognetti, D.M. AJCC-8ed nodal staging does not predict outcomes in surgically managed HPV-associated oropharyngeal cancer. Oral Oncol. 2018, 82, 138–143. [Google Scholar] [CrossRef]
- Holcomb, A.J.; Herberg, M.; Strohl, M.; Ochoa, E.; Feng, A.L.; Abt, N.B.; Mokhtari, T.E.; Suresh, K.; McHugh, C.I.; Parikh, A.S.; et al. Impact of surgical margins on local control in patients undergoing single-modality transoral robotic surgery for HPV-related oropharyngeal squamous cell carcinoma. Head Neck 2021, 43, 2434–2444. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.J.; Olsen, K.D.; Kasperbauer, J.L. Transoral robotic surgery for oropharyngeal squamous cell carcinoma: A prospective study of feasibility and functional outcomes. Laryngoscope 2009, 119, 2156–2164. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.J.; Olsen, S.M.; Laborde, R.R.; García, J.J.; Walsh, F.J.; Price, D.L.; Janus, J.R.; Kasperbauer, J.L.; Olsen, K.D. Long-term Functional and Oncologic Results of Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma. Mayo Clin. Proc. 2012, 87, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pipkorn, P.; Sinha, P.; Kallogjeri, D.; Adkins, D.; Thorstad, W.T.; Rich, J.T.; Jackson, R. Outcomes of relapsed human papillomavirus-related oropharyngeal squamous cell carcinoma treated with curative intent. Head Neck 2018, 41, 1312–1319. [Google Scholar] [CrossRef]
- Sadeghi, N.; Li, N.-W.; Taheri, M.R.; Easley, S.; Siegel, R.S. Neoadjuvant chemotherapy and transoral surgery as a definitive treatment for oropharyngeal cancer: A feasible novel approach. Head Neck 2016, 38, 1837–1846. [Google Scholar] [CrossRef]
- Sims, J.R.; Van Abel, K.; Martin, E.J.; Lohse, C.M.; Price, D.L.; Olsen, K.D.; Moore, E.J. Management of Recurrent and Metastatic HPV-Positive Oropharyngeal Squamous Cell Carcinoma after Transoral Robotic Surgery. Otolaryngol. Neck Surg. 2017, 157, 69–76. [Google Scholar] [CrossRef]
- Su, W.; Rajeev-Kumar, G.; Kang, M.; Posner, M.; Liu, J.; Westra, W.; Miles, B.A.; Gupta, V.; Sharma, S.; Misiukiewicz, K.; et al. Long-term outcomes in patients with recurrent human papillomavirus-positive oropharyngeal cancer after upfront transoral robotic surgery. Head Neck 2020, 42, 3490–3496. [Google Scholar] [CrossRef]
- Byeon, H.K.; Duvvuri, U.; Kim, W.S.; Park, Y.M.; Hong, H.J.; Koh, Y.W.; Choi, E.C. Transoral Robotic Retropharyngeal Lymph Node Dissection With or Without Lateral Oropharyngectomy. J. Craniofacial Surg. 2013, 24, 1156–1161. [Google Scholar] [CrossRef]
- Kubik, M.; Mandal, R.; Albergotti, W.; Duvvuri, U.; Ferris, R.L.; Kim, S. Effect of transcervical arterial ligation on the severity of postoperative hemorrhage after transoral robotic surgery. Head Neck 2017, 39, 1510–1515. [Google Scholar] [CrossRef]
- Meccariello, G.; Cammaroto, G.; Ofo, E.; Calpona, S.; Parisi, E.; D’Agostino, G.; Gobbi, R.; Firinu, E.; Bellini, C.; De Vito, A.; et al. The emerging role of trans-oral robotic surgery for the detection of the primary tumour site in patients with head-neck unknown primary cancers: A meta-analysis. Auris Nasus Larynx 2019, 46, 663–671. [Google Scholar] [CrossRef]
- Chen, M.M.; Roman, S.A.; Kraus, D.H.; Sosa, J.A.; Judson, B.L. Transoral Robotic Surgery: A Population-Level Analysis. Otolaryngol. Head Neck Surg. 2014, 150, 968–975. [Google Scholar] [CrossRef]
- Morisod, B.; Venara-Vulpe, I.I.; Alzuphar, S.; Monnier, Y.; Bongiovanni, M.; Hagmann, P.; Bouchaab, H.; Bourhis, J.; Simon, C. Minimizing adjuvant treatment after transoral robotic surgery through surgical margin revision and exclusion of radiographic extracapsular extension: A Prospective observational cohort study. Head Neck 2017, 39, 965–973. [Google Scholar] [CrossRef]
- Hanna, J.; Morse, E.; Brauer, P.R.; Judson, B.; Mehra, S. Positive margin rates and predictors in transoral robotic surgery after federal approval: A national quality study. Head Neck 2019, 41, 3064–3072. [Google Scholar] [CrossRef]
- Gorphe, P.; Simon, C. A systematic review and meta-analysis of margins in transoral surgery for oropharyngeal carcinoma. Oral Oncol. 2019, 98, 69–77. [Google Scholar] [CrossRef]
- Li, H.; Ba, S.J.T.; Park, H.S.; Yarbrough, W.G.; Mehra, S.; Choi, R.; Judson, B.L. Clinical value of transoral robotic surgery: Nationwide results from the first 5 years of adoption. Laryngoscope 2018, 129, 1844–1855. [Google Scholar] [CrossRef]
- Oliver, J.R.; Persky, M.J.; Wang, B.; Duvvuri, U.; Gross, N.D.; Vaezi, A.E.; Morris, L.G.T.; Givi, B. Transoral robotic surgery adoption and safety in treatment of oropharyngeal cancers. Cancer 2021, 128, 685–696. [Google Scholar] [CrossRef]
- Fiacchini, G.; Vianini, M.; Dallan, I.; Bruschini, L. Is the Da Vinci Xi system a real improvement for oncologic transoral robotic surgery? A systematic review of the literature. J. Robot. Surg. 2020, 15, 1–12. [Google Scholar] [CrossRef]
- Alicandri-Ciufelli, M.; Bonali, M.; Piccinini, A.; Marra, L.; Ghidini, A.; Cunsolo, E.M.; Maiorana, A.; Presutti, L.; Conte, P.F. Surgical Margins in Head and Neck Squamous Cell Carcinoma: What Is ‘Close’? Eur. Arch. Otorhinolaryngol. 2013, 270, 2603–2609. [Google Scholar] [CrossRef]
- Machtay, M.; Perch, S.; Markiewicz, D.; Thaler, E.; Chalian, A.; Goldberg, A.; Kligerman, M.; Weinstein, G. Combined Surgery and Postoperative Radiotherapy for Carcinoma of the Base of Radiotherapy for Carcinoma of the Base of Tongue: Analysis of Treatment Outcome and Prognostic Value of Margin Status. Head Neck 1997, 19, 494–499. [Google Scholar] [CrossRef]
- Cohen, M.A.; Weinstein, G.S.; O’Malley, B.W.; Feldman, M.; Quon, H. Transoral robotic surgery and human papillomavirus status: Oncologic results. Head Neck 2010, 33, 573–580. [Google Scholar] [CrossRef]
- Weinstein, G.S.; O’Malley, B.W., Jr.; Magnuson, J.S.; Carroll, W.R.; Olsen, K.D.; Daio, L.; Moore, E.J.; Holsinger, F.C. Transoral Robotic Surgery: A Multicenter Study to Assess Feasibility, Safety, and Surgical Margins. Laryngoscope 2012, 122, 1701–1707. [Google Scholar] [CrossRef]
- Horwich, P.; MacKay, C.; Bullock, M.; Taylor, S.M.; Hart, R.; Trites, J.; Geldenhuys, L.; Williams, B.; Rigby, M.H. Specimen oriented intraoperative margin assessment in oral cavity and oropharyngeal squamous cell carcinoma. J. Otolaryngol. Head Neck Surg. 2021, 50, 37. [Google Scholar] [CrossRef]
- Iyer, N.G.; Dogan, S.; Palmer, F.; Rahmati, R.; Nixon, I.; Lee, N.; Patel, S.G.; Shah, J.; Ganly, I. Detailed Analysis of Clinicopathologic Factors Demonstrate Distinct Difference in Outcome and Prognostic Factors Between Surgically Treated HPV-Positive and Negative Oropharyngeal Cancer. Ann. Surg. Oncol. 2015, 22, 4411–4421. [Google Scholar] [CrossRef] [Green Version]
- Han, M.; Stanford-Moore, G.B.; Larson, A.R.; Schoppy, D.W.; Cognetti, D.M.; Joshi, A.S.; Houlton, J.J.; Ryan, W.R. Predictors of Mortality in HPV-Associated Oropharynx Carcinoma Treated With Surgery Alone. Laryngoscope 2019, 130, E423–E435. [Google Scholar] [CrossRef] [PubMed]
- Kanakamedala, M.R.; Giri, S.P.G.; Hamilton, R.D.; Bhanat, E.; Vijayakumar, S. Outcomes utilizing intensity-modulated radiotherapy in oropharyngeal cancers: Tonsils versus base of tongue. Head Neck 2018, 40, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Chia, S.H.; Gross, N.D.; Richmon, J.D. Surgeon Experience and Complications with Transoral Robotic Surgery (TORS). Otolaryngol. Neck Surg. 2013, 149, 885–892. [Google Scholar] [CrossRef] [PubMed]
- De Almeida, J.R.; Byrd, J.K.; Wu, R.; Stucken, C.L.; Duvvuri, U.; Goldstein, D.P.; Miles, B.A.; Teng, M.S.; Gupta, V.; Genden, E.M. A systematic review of transoral robotic surgery and radiotherapy for early oropharynx cancer: A systematic review. Laryngoscope 2014, 124, 2096–2102. [Google Scholar] [CrossRef] [PubMed]
- Asher, S.A.; White, H.N.; Kejner, A.E.; Rosenthal, E.L.; Carroll, W.R.; Magnuson, J.S. Hemorrhage after Transoral Robotic-Assisted Surgery. Otolaryngol. Neck Surg. 2013, 149, 112–117. [Google Scholar] [CrossRef]
- Gleysteen, J.; Troob, S.; Light, T.; Brickman, D.; Clayburgh, D.; Andersen, P.; Gross, N. The impact of prophylactic external carotid artery ligation on postoperative bleeding after transoral robotic surgery (TORS) for oropharyngeal squamous cell carcinoma. Oral Oncol. 2017, 70, 1–6. [Google Scholar] [CrossRef]
- Vergez, S.; Lallemant, B.; Ceruse, P.; Moriniere, S.; Aubry, K.; De Mones, E.; Benlyazid, A.; Mallet, Y. Initial Multi-institutional Experience with Transoral Robotic Surgery. Otolaryngol. Neck Surg. 2012, 147, 475–481. [Google Scholar] [CrossRef]
- Hay, A.; Nixon, I.J. Recent Advances in the Understanding and Management of Oropharyngeal Cancer. F1000Research 2018, 7, 72. [Google Scholar] [CrossRef]
- Pollei, T.R.; Hinni, M.L.; Moore, E.J.; Hayden, R.E.; Olsen, K.D.; Casler, J.D.; Walter, L.C. Analysis of Postoperative Bleeding and Risk Factors in Transoral Surgery of the Oropharynx. JAMA Otolaryngol. Neck Surg. 2013, 139, 1212–1218. [Google Scholar] [CrossRef] [Green Version]
- Zenga, J.; Suko, J.; Kallogjeri, D.; Pipkorn, P.; Nussenbaum, B.; Jackson, R.S. Postoperative hemorrhage and hospital revisit after transoral robotic surgery. Laryngoscope 2017, 127, 2287–2292. [Google Scholar] [CrossRef]
- Bernier, J.; Cooper, J.S.; Pajak, T.F.; Van Glabbeke, M.; Bourhis, J.; Forastiere, A.; Ozsahin, E.M.; Jacobs, J.R.; Jassem, J.; Ang, K.-K.; et al. Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 2005, 27, 843–850. [Google Scholar] [CrossRef]
- Ward, M.C.; Koyfman, S.A. Transoral robotic surgery: The radiation oncologist’s perspective. Oral Oncol. 2016, 60, 96–102. [Google Scholar] [CrossRef]
- Weinstein, G.S.; Quon, H.; Newman, H.J.; Chalian, J.A.; Malloy, K.; Lin, A.; Desai, A.; Livolsi, V.A.; Montone, K.T.; Cohen, K.R.; et al. Transoral Robotic Surgery Alone for Oropharyngeal Cancer: An Analysis of Local Control. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Kaczmar, J.M.; Tan, K.S.; Heitjan, D.F.; Lin, A.; Ahn, P.H.; Newman, J.G.; Rassekh, C.H.; Chalian, A.A.; O’Malley, B.W.; Cohen, R.B.; et al. HPV-related oropharyngeal cancer: Risk factors for treatment failure in patients managed with primary transoral robotic surgery. Head Neck 2014, 38, 59–65. [Google Scholar] [CrossRef]
- Zenga, J.; Graboyes, E.; Janz, T.; Drake, V.; Rettig, E.; Desai, S.; Nickel, C.; Shabani, S.; Padhya, T.; Scarpinato, M.; et al. Salvage of Recurrence after Surgery and Adjuvant Therapy: A Multi-institutional Study. Otolaryngol. Neck Surg. 2019, 161, 74–81. [Google Scholar] [CrossRef]
- Dziegielewski, P.T.; Teknos, T.N.; Durmus, K.; Old, M.; Agrawal, A.; Kakarala, K.; Marcinow, A.; Ozer, E. Transoral Robotic Surgery for Oropharyngeal Cancer: Long-Term Quality of Life and Functional Outcomes. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 1099–1108. [Google Scholar] [CrossRef]
- Sethia, R.; Yumusakhuylu, A.C.; Ozbay, I.; Diavolitsis, V.; Brown, N.V.; Zhao, S.; Wei, L.; Old, M.; Agrawal, A.; Teknos, T.N.; et al. Quality of life outcomes of transoral robotic surgery with or without adjuvant therapy for oropharyngeal cancer. Laryngoscope 2017, 128, 403–411. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | OLE | Study Design | Total Tonsil (N) | Total BOT (N) | P16/HPV (%) | Age Mean or Median, Year (Range) | Male (%) | Never Smoked (%) | Neck Dissection (%) | T3 or T4 (%) | N2 or N3 (%) | Perineural Invasion (%) | Extra-nodal Extension (%) | Lympho-vascular Invasion (%) | Extra-capsular Spread (%) | Adjuvant Radiotherapy (%) | Adjuvant Chemoradiotherapy (%) | Follow-Up Mean or Median, Year (Range) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bu 2021 | 4 | Case Series | 94 | 70 | 100.0 | 60.0 (15.0–85.0) | 88.2 | NR | NR | 3.0 | 58.6 | NR | NR | NR | 24.9 | 42.0 | 35.5 | NR (NR) |
| Byeon 2013 | 4 | Case Series | 4 | 0 | NR | 54.0 (38.0–64.0) | 75.0 | NR | 100.0 | 25.0 | 100.0 | NR | NR | NR | 25.0 | NR | NR | NR (NR) |
| Carey 2021 | 4 | Case Series | 278 | 202 | 100.0 | 59.1 (NR) | 86.7 | 32.5 | NR | 7.6 | 16.1 | 15.3 | 30.1 | 29.2 | NR | 45.8 | 37.7 | NR (NR) |
| de Almeida 2015 | 4 | Case Series | 186 | 130 | 69.4 | 59.6 (NR) | 82.4 | 33.7 | 80.8 | 9.3 | 48.0 | 22.3 | 31.3 | 26.4 | 36.7 | 25.9 | 17.6 | 20.0 (1.0–74.0) |
| Dowthwaite 2019 | 4 | Case Series | 26 | 0 | 92.3 | 63.0 (41.0–77.0) | 80.8 | 76.9 | 26.9 | 0.0 | 0.0 | NR | NR | NR | NR | 11.5 | 7.7 | 36.0 (6.0–54.0) |
| Dziegielewski 2017 | 4 | Case Series | 79 | 0 | 85.9 | 55.6 (39.2–78.5) | 77.2 | 15.2 | NR | 8.9 | 78.5 | 31.6 | NR | 40.5 | 35.1 | 30.4 | 53.2 | 10.5 (0.0–42.3) |
| Fradet 2022 | 4 | Case Series | 55 | 44 | 91.3 | 59.0 (NR) | 85.4 | NR | 93.2 | 2.9 | 40.8 | 8.7 | 47.6 | 50.5 | NR | 16.5 | 41.7 | 31.2 (3.0–9.2) |
| Funk 2016 | 4 | Case Series | 16 | 9 | 100.0 | 58.0 (39.0–91.0) | NR | NR | NR | NR | 68.0 | 12.0 | NR | 92.0 | 28.0 | NR | 0.0 | 31.5 (4.9–73.1) |
| Gallitto 2019 | 4 | Case Series | 26 | 19 | 79.5 | 54.0 (NR) | 95.7 | 51.1 | 100.0 | 4.3 | 17.4 | 26.1 | 97.8 | 32.5 | 67.4 | 100.0 | 0.0 | 48.4 (NR) |
| Gobillot 2019 | 4 | Case Series | 58 | 0 | 92.7 | NR (NR) | 89.7 | NR | 94.8 | 0.0 | 8.6 | NR | 19.0 | NR | NR | 36.2 | 24.1 | 19.5 (6.2–86.0) |
| Hirshoren 2018 | 4 | Case Series | 9 | 18 | 62.5 | 63.7 (28.0–87.0) | 62.9 | NR | NR | 4.2 | 21.7 | NR | NR | NR | NR | NR | NR | NR (NR) |
| Hobelmann 2018 | 4 | Case Series | 63 | 52 | 100.0 | 58.0 (38.0–87.0) | 87.1 | 44.8 | NR | NR | NR | NR | 43.1 | NR | NR | 32.8 | 58.6 | 30.0 (8.0–82.0) |
| Holcomb 2021 | 4 | Case Series | 55 | 42 | 100.0 | 60.9 (NR) | 82.8 | 45.9 | NR | 2.0 | 46.4 | 3.5 | 89.9 | 18.7 | NR | 0.0 | 0.0 | 28.5 (6.0–121.0) |
| Kubik 2017 | 4 | Case Series | 114 | 122 | 82.6 | 59.0 (NR) | 81.1 | NR | NR | 10.2 | NR | NR | NR | NR | NR | NR | NR | NR (NR) |
| Kumar 2021 | 4 | Case Series | 49 | 9 | 100.0 | 59.8 (40.0–78.0) | 76.3 | NR | NR | 1.7 | 39.7 | NR | NR | NR | NR | NR | NR | NR (NR) |
| Meccariello 2019 | 4 | Case Series | 28 | 25 | 55.0 | NR (NR) | NR | NR | NR | 12.2 | 24.5 | NR | NR | NR | NR | 33.3 | 36.7 | 30.3 (NR) |
| Moore 2009 | 4 | Case Series | 19 | 26 | NR | 57.0 (38.0–88.0) | 88.9 | 66.7 | 95.6 | 24.4 | 68.9 | NR | NR | NR | NR | 17.8 | 55.6 | 12.3 (1.0–16.0) |
| Moore 2012 | 4 | Case Series | 40 | 26 | 71.7 | 55.2 (36.0–80.0) | 89.4 | 50.0 | 100.0 | 9.7 | 74.2 | 3.0 | NR | 12.1 | 56.1 | 21.2 | 62.1 | 36.0 (24.0–45.0) |
| Olaleye 2021 | 4 | Case Series | 21 | 22 | 87.8 | 60.5 (NR) | 82.6 | NR | 61.2 | 10.6 | 10.0 | NR | NR | NR | NR | 0.0 | 83.7 | NR (NR-54.0) |
| Persky 2018 | 4 | Cohort | 89 | 51 | 88.5 | 58.0 (NR) | 80.0 | 34.5 | NR | NR | 36.4 | 16.8 | NR | 16.9 | NR | NR | NR | NR (NR) |
| Pipkorn 2019 | 4 | Cohort | 133 | 108 | 100.0 | 54.0 (27.0–83.0) | 86.0 | 47.3 | 100.0 | 22.6 | NR | 11.0 | NR | 31.3 | 78.4 | 41.9 | 34.1 | 33.0 (5.0–65.0) |
| Sadeghi 2016 | 4 | Case Series | 4 | 6 | 80.0 | 59.8 (NR) | 80.0 | NR | NR | 20.0 | 0.0 | NR | NR | NR | NR | 0.0 | 100.0 | NR (NR) |
| Sims 2017 | 4 | Case Series | 19 | 5 | 100.0 | 59.6 (NR) | 82.6 | NR | NR | 26.1 | 56.5 | NR | NR | NR | NR | 17.4 | 30.4 | 13.2 (0.0–74.4) |
| Spellman 2018 | 4 | Case Series | 14 | 0 | 100.0 | 57.6 (32.0–72.0) | 78.6 | 78.6 | 100.0 | 0.0 | 0.0 | 7.1 | NR | 0.0 | NR | 7.1 | NR | 28.0 (1.0–56.0) |
| Subramanian 2016 | 4 | Case Series | 17 | 16 | 90.3 | 56.5 (NR) | 73.5 | 38.2 | 85.3 | 12.1 | 52.9 | NR | NR | NR | 51.7 | 20.6 | 50.0 | NR (NR) |
| Su 2020 | 4 | Case Series | 194 | 99 | 100.0 | 60.0 (28.0–86.6) | 84.9 | NR | NR | 3.2 | 48.6 | NR | NR | NR | NR | 0.0 | NR | 20.0 (NR) |
| Weinstein 2007 | 4 | Case Series | 27 | 0 | NR | NR (NR) | 92.6 | NR | 96.3 | 22.2 | 37.0 | 7.4 | NR | NR | NR | 33.3 | 55.6 | NR (NR) |
| Zebolsky 2021 | 4 | Case Series | 52 | 38 | 100.0 | 63.0 (36.0–87.0) | 83.1 | 47.1 | 100.0 | 2.2 | 70.6 | 8.8 | 19.9 | 25.0 | NR | NR | NR | NR (NR) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poupore, N.S.; Chen, T.; Nguyen, S.A.; Nathan, C.-A.O.; Newman, J.G. Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma of the Tonsil versus Base of Tongue: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 3837. https://doi.org/10.3390/cancers14153837
Poupore NS, Chen T, Nguyen SA, Nathan C-AO, Newman JG. Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma of the Tonsil versus Base of Tongue: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(15):3837. https://doi.org/10.3390/cancers14153837
Chicago/Turabian StylePoupore, Nicolas S., Tiffany Chen, Shaun A. Nguyen, Cherie-Ann O. Nathan, and Jason G. Newman. 2022. "Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma of the Tonsil versus Base of Tongue: A Systematic Review and Meta-Analysis" Cancers 14, no. 15: 3837. https://doi.org/10.3390/cancers14153837
APA StylePoupore, N. S., Chen, T., Nguyen, S. A., Nathan, C.-A. O., & Newman, J. G. (2022). Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma of the Tonsil versus Base of Tongue: A Systematic Review and Meta-Analysis. Cancers, 14(15), 3837. https://doi.org/10.3390/cancers14153837