
Newly Diagnosed Children with Cancer Have Lower 25-Vitamin D Levels than Their Cancer-Free Peers: A Comparison across Age, Race, and Sex


 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data
2.3. Data Analysis
3. Results
3.1. Within-Group Comparisons
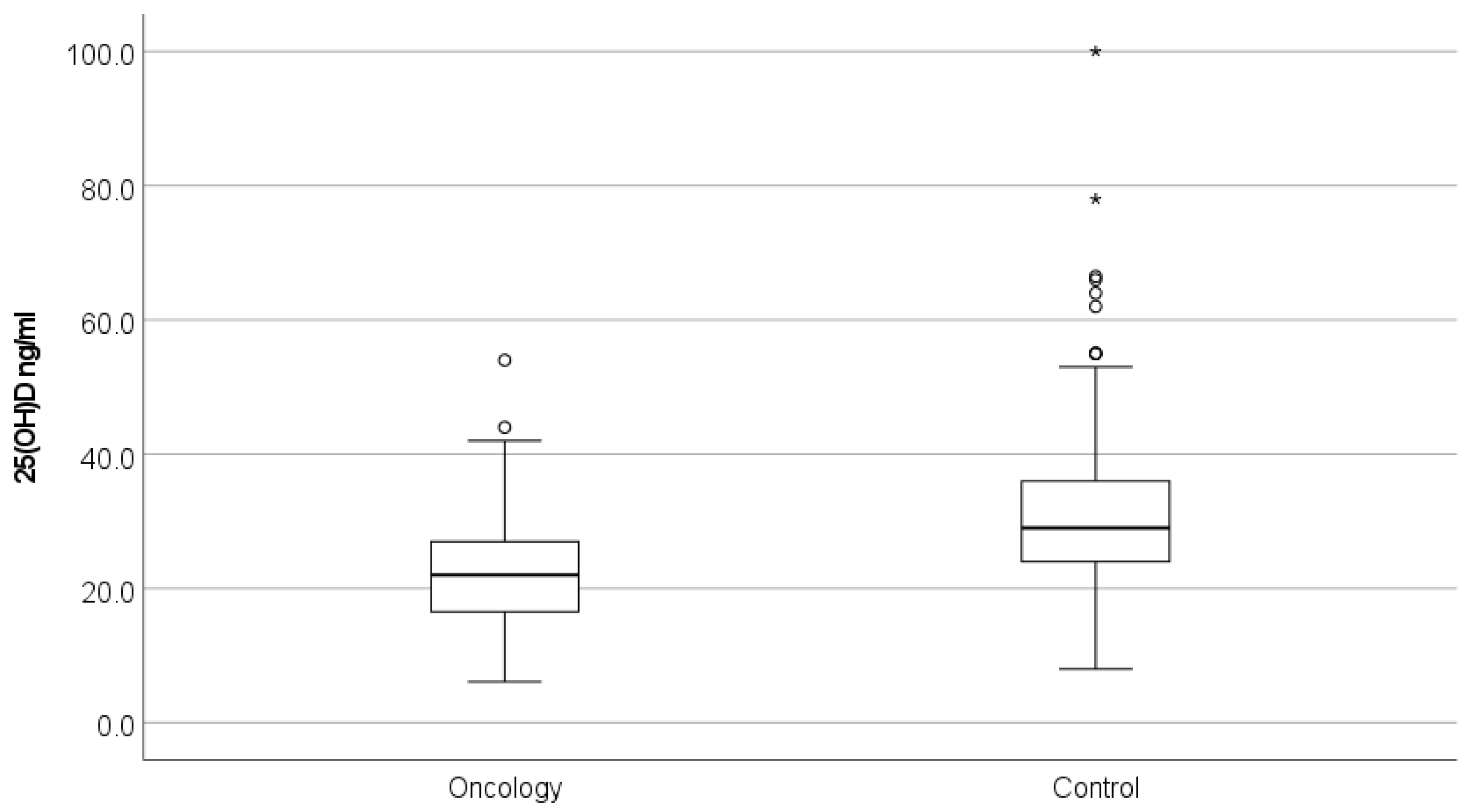
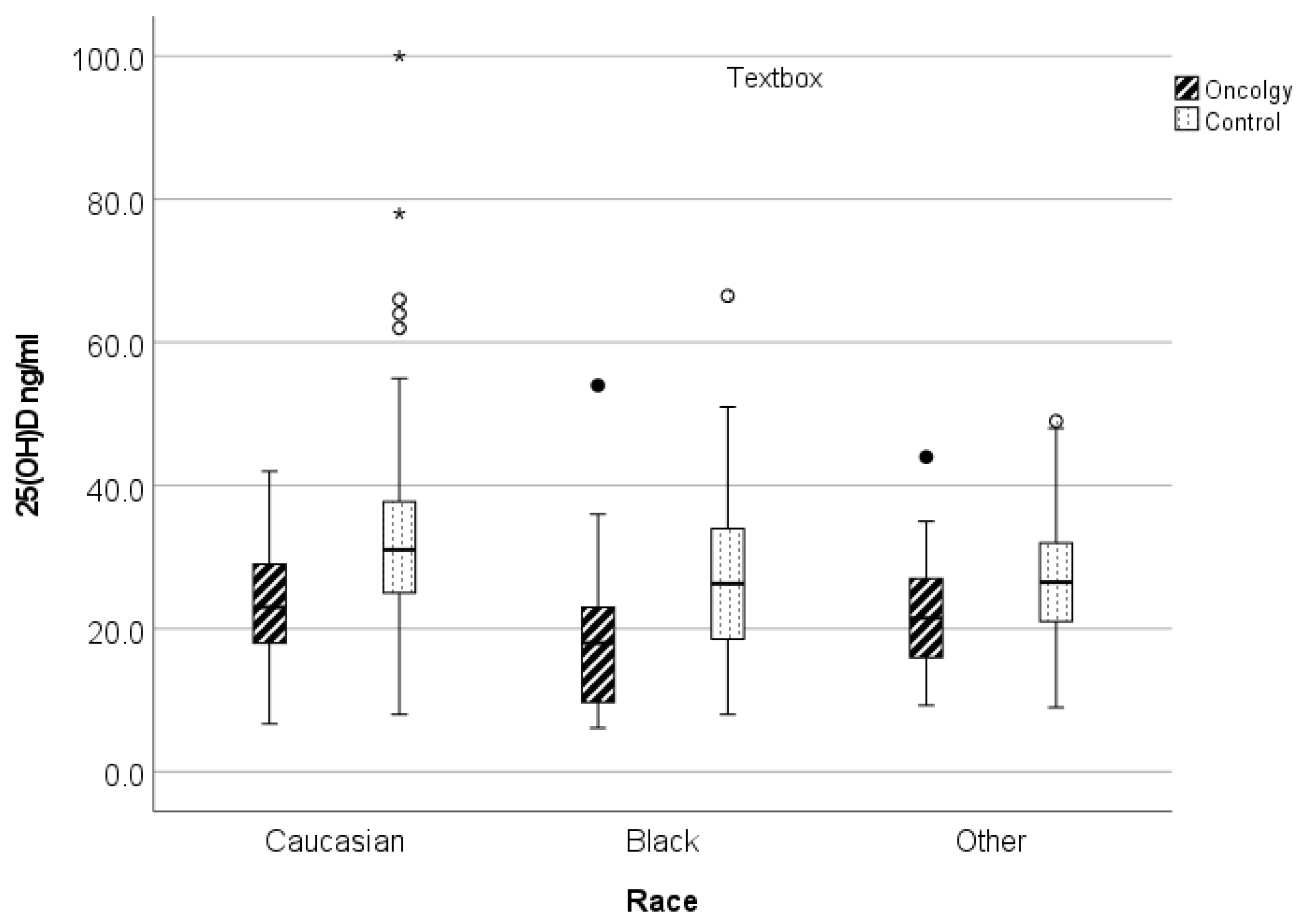
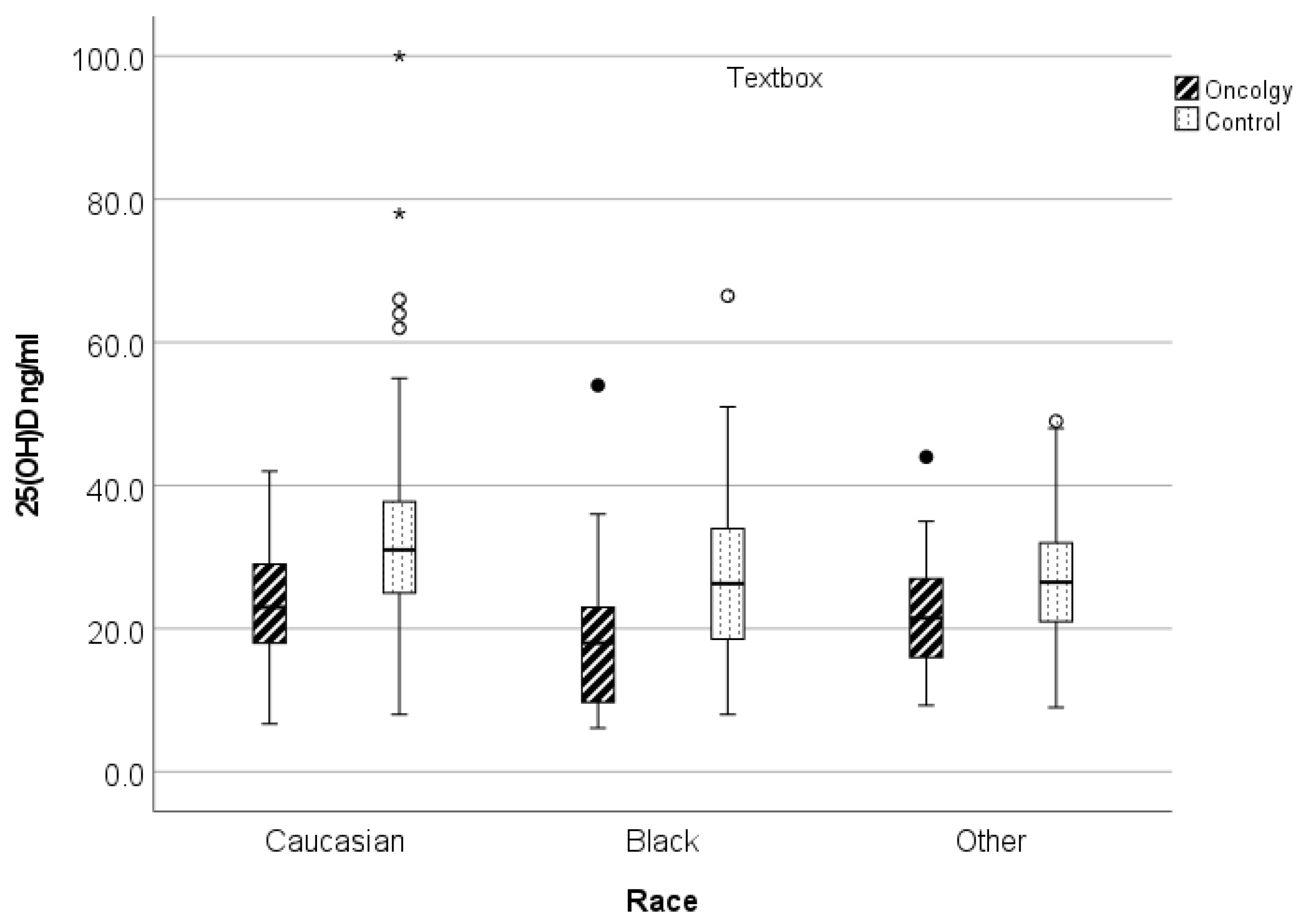
3.2. Oncology versus Control 25(OH)D Levels by Variable
3.3. Classification of 25(OH)D Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global consensus recommendations on prevention and management of nutritional rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.M.; Feldman, H.A.; Sinclair, L.; Williams, A.L.; Kleinman, P.K.; Perez-Rossello, J.; Cox, J.E. Prevalence of Vitamin D Deficiency Among Healthy Infants and Toddlers. Arch. Pediatr. Adolesc. Med. 2008, 162, 505–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, J.; Muntner, P.; Kaskel, F.J.; Hailpern, S.M.; Melamed, M.L. Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001–2004. Pediatrics 2009, 124, e362–e370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A., Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef] [Green Version]
- Wagner, C.L.; Greer, F.R.; American Academy of Pediatrics Section on Breastfeeding; American Academy of Pediatrics Committee on Nutrition. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics 2008, 122, 1142–1152. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press: Washington, WA, USA, 2011. [Google Scholar]
- Drake, M.T.; Maurer, M.J.; Link, B.K.; Habermann, T.M.; Ansell, S.M.; Micallef, I.N.; Kelly, J.L.; Macon, W.R.; Nowakowski, G.S.; Inwards, D.J.; et al. Vitamin D insufficiency and prognosis in non-Hodgkin’s lymphoma. J. Clin. Oncol. 2010, 28, 4191–4198. [Google Scholar] [CrossRef] [Green Version]
- Díaz, L.; Díaz-Muñoz, M.; García-Gaytán, A.C.; Méndez, I. Mechanistic effects of calcitriol in cancer biology. Nutrients 2015, 7, 5020–5050. [Google Scholar] [CrossRef] [Green Version]
- Duncan, C.N.; Vrooman, L.; Apfelbaum, E.M.; Whitley, K.; Bechard, L.; Lehmann, L.E. 25-hydroxy vitamin D deficiency following pediatric hematopoietic stem cell transplant. Biol. Blood Marrow Transplant. 2011, 17, 749–753. [Google Scholar] [CrossRef] [Green Version]
- Garland, C.F.; Garland, F.C.; Gorham, E.D.; Lipkin, M.; Newmark, H.; Mohr, S.B.; Holick, M.F. The role of vitamin D in cancer prevention. Am. J. Public Health 2006, 96, 252–261. [Google Scholar] [CrossRef]
- Ma, Y.; Trump, D.L.; Johnson, C.S. Vitamin D in combination cancer treatment. J. Cancer 2010, 1, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakos, S.; Ajibade, D.V.; Dhawan, P.; Fechner, A.J.; Mady, L.J. Vitamin D: Metabolism. Endocrinol. Metab. Clin. N. Am. 2010, 39, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Giammanco, M.; Di Majo, D.; La Guardia, M.; Aiello, S.; Crescimannno, M.; Flandina, C.; Tumminello, F.M.; Leto, G. Vitamin D in cancer chemoprevention. Pharm. Biol. 2015, 53, 1399–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iniesta, R.R.; Rush, R.; Paciarotti, I.; Rhatigan, E.; Brougham, F.; McKenzie, J.; Wilson, D. Systematic review and meta-analysis: Prevalence and possible causes of vitamin D deficiency and insufficiency in pediatric cancer patients. Clin. Nutr. 2016, 35, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.M.; Shin, E.A. Exploring vitamin D metabolism and function in cancer. Exp. Mol. Med. 2018, 50, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Stambolsky, P.; Tabach, Y.; Fontemaggi, G.; Weisz, L.; Maor-Aloni, R.; Sigfried, Z.; Shiff, I.; Kogan, I.; Shay, M.; Kalo, E.; et al. Modulation of the vitamin D3 response by cancer-associated mutant p53. Cancer Cell 2010, 17, 273–285. [Google Scholar] [CrossRef] [Green Version]
- Lappe, J.M.; Travers-Gustafson, D.; Davies, K.M.; Recker, R.R.; Heaney, R.P. Vitamin D and calcium supplementation reduces cancer risk: Results of a randomized trial. Am. J. Clin. Nutr. 2007, 85, 1586–1591. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, S.; Verma, N.; Kumar, A. Prevalence of vitamin D deficiency in childhood acute lymphoblastic leukemia and its association with adverse outcomes during induction phase of treatment. Nutr. Cancer 2020, 72, 1321–1325. [Google Scholar] [CrossRef]
- Simmons, J.H.; Chow, E.; Koehler, E.; Esbenshade, A.; Smith, L.-A.; Sanders, J.; Friedman, D. Significant 25-hydroxyvitamin D deficiency in child and adolescent survivors of acute lymphoblastic leukemia: Treatment with chemotherapy compared with allogeneic stem cell transplant. Pediatr. Blood Cancer 2011, 56, 1114–1119. [Google Scholar] [CrossRef] [Green Version]
- Wasilewski-Masker, K.; Kaste, S.C.; Hudson, M.M.; Esiashvili, N.; Mattano, L.A.; Meacham, L.R. Bone mineral density deficits in survivors of childhood cancer: Long-term follow-up guidelines and review of the literature. Pediatrics 2008, 121, e705–e713. [Google Scholar] [CrossRef] [PubMed]
- Bilariki, K.; Anagnostou, E.; Masse, V.; Elie, C.; Grill, J.; Valteau-Couanet, D.; Kalifa, C.; Doz, F.; Sainte-Rose, C.; Zerah, M.; et al. Low bone mineral density and high incidences of fractures and vitamin D deficiency in 52 pediatric cancer survivors. Horm. Res. Paediatr. 2010, 74, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Cummings, E.; Ma, J.; Fernandez, C.V.; Halton, J.; Alos, N.; Miettunen, P.M.; Jaremko, J.L.; Ho, J.; Shenouda, N.; Matzinger, M.A.; et al. Incident vertebral fractures in children with leukemia during the four years following diagnosis. J. Clin. Endocrinol. Metab. 2015, 100, 3408–3417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayar, M.S.; Nayiager, T.; Webber, C.E.; Barr, R.D.; Athale, U.H. Predictors of bony morbidity in children with acute lymphoblastic leukemia. Pediatr. Blood Cancer 2012, 59, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Beebe, K.; Magee, K.; McNulty, A.; Stahlecker, J.; Salzberg, D.; Miller, H.; Mirea, L.; Adams, R.; Ngwube, A. Vitamin D deficiency and outcomes in pediatric hematopoietic stem cell transplantation. Pediatr. Blood Cancer 2018, 65, e26817. [Google Scholar] [CrossRef]
- Genc, D.B.; Vural, S.; Yagar, G. The incidence of and factors associated with vitamin D deficiency in newly diagnosed children with cancer. Nutr. Cancer 2016, 68, 756–761. [Google Scholar] [CrossRef]
- Gokcebay, D.G.; Emir, L.; Bayhan, T.; Demir, H.A.; Özyörük, D.; Gunduz, M.; Koc, N. Evaluation of serum trace element and vitamin levels in children with cancer in the first 6 months after diagnosis. J. Pediatr. Hematol. Oncol. 2018, 40, e343–e347. [Google Scholar] [CrossRef]
- Aristizabal, P.; Sherer, M.; Perdomo, B.P.; Castelao, E.; Thornburg, C.D.; Proudfoot, J.; Jacobs, E.; Newfield, R.S.; Zage, P.; Roberts, W.; et al. Sociodemographic and clinical characteristics associated with vitamin D status in newly diagnosed pediatric cancer patients. Pediatr. Hematol. Oncol. 2020, 37, 314–325. [Google Scholar] [CrossRef]
- Mansbach, J.M.; Ginde, A.A.; Camargo, C.A., Jr. Serum 25-hydroxyvitamin D levels among US children aged 1 to 11 years: Do children need more vitamin D? Pediatrics 2009, 124, 1404–1410. [Google Scholar] [CrossRef] [Green Version]
- Helou, M.; Ning, Y.; Yang, S.; Irvine, P.; Bachmann, L.M.; Godder, K.; Massey, G. Vitamin d deficiency in children with cancer. J. Pediatr. Hematol. Oncol. 2014, 36, 212–217. [Google Scholar] [CrossRef]
- Herrick, K.A.; Storandt, R.; Afful, J.; Pfeiffer, C.M.; Schleicher, R.L.; Gahche, J.J.; Potischman, N. Vitamin D status in the United States, 2011–2014. Am. J. Clin. Nutr. 2019, 110, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhary, A.; Chou, J.; Heller, G.; Sklar, C. Prevalence of vitamin D insufficiency in survivors of childhood cancer. Pediatr. Blood Cancer 2013, 60, 1237–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, G.P.; Beebe, K.L.; Shaibi, G.Q. Vitamin D levels differ by cancer diagnosis and decline over time in survivors of childhood cancer. Pediatr. Blood Cancer 2013, 60, 949–952. [Google Scholar] [CrossRef] [PubMed]
- Jackmann, N.; Mäkitie, O.; Harila-Saari, A.; Gustafsson, J.; Nezirevic Dernroth, D.; Frisk, P. Vitamin D status in children with leukemia, its predictors, and association with outcome. Pediatr. Blood Cancer 2020, 67, e28163. [Google Scholar] [CrossRef]
- Kampman, M.T.; Wilsgaard, T.; Mellgren, S.I. Outdoor activities and diet in childhood and adolescence relate to MS risk above the Arctic Circle. J. Neurol. 2007, 254, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Kimm, S.Y.; Glynn, N.; Kriska, A.; Barton, B.; Kronsberg, S.S.; Daniels, S.R.; Crawford, P.B.; Sabry, Z.I.; Liu, K. Decline in physical activity in black girls and white girls during adolescence. N. Engl. J. Med. 2002, 347, 709–715. [Google Scholar] [CrossRef]
- Prentice, A. Vitamin D deficiency: A global perspective. Nutr. Rev. 2008, 66, S153–S164. [Google Scholar] [CrossRef]
- Shliakhtsitsava, K.; Fisher, E.S.; Trovillion, E.M.; Bush, K.; Kuo, D.J.; Newfield, R.S.; Thornburg, C.D.; Roberts, W.; Aristizabal, P. Improving vitamin D testing and supplementation in children with newly diagnosed cancer: A quality improvement initiative at Rady Children’s Hospital San Diego. Pediatr. Blood Cancer 2021, 68, e29217. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Included Cancers |
|---|
| Acute lymphocytic leukemia Acute myeloid leukemia |
| Neuroblastoma |
| Osteosarcoma |
| Ewing’s sarcoma |
| Medulloblastoma |
| Rhabdomyosarcoma |
| Glioblastoma |
| Lymphomas (all) |
| Wilms tumor |
| Germ cell tumors |
| Atypical teratoid/rhabdoid tumor |
| Hepatocellular carcinoma |
| Yolk sac tumor |
| Embryonal carcinoma |
| Excluded Diagnoses | |
|---|---|
| Anorexia nervosa Aplastic anemia | Jejunostomy tube Juvenile idiopathic arthritis |
| Bulimia | Juvenile rheumatoid arthritis |
| Cerebral palsy | Kidney transplant |
| Chronic arthritis | Laparoscopic gastric band |
| Chronic renal disease | Liver transplant |
| Colostomy | Malabsorption |
| Crohn’s disease | Metabolic disorders |
| Cystic fibrosis | Morbid obesity |
| Gastric sleeve | Necrotizing enterocolitis |
| Gastroschisis | Osteogenesis imperfecta |
| Gastrostomy tube | Short gut syndrome |
| Grave’s disease | Sickle cell anemia |
| Hypophosphatemic rickets | Systemic lupus erythematosus |
| Ileostomy | Thalassemia |
| Inflammatory bowel disease | Ulcerative colitis |
| Oncology | Control | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Grouping | n | Mean Age (yrs) | Range | Mean 25(OH)D (ng/mL) | SD | n | Mean Age (yrs) | Range | Mean 25(OH)D (ng/mL) | SD |
| Black (all) | 25 | 9.4 | 0.5–17.9 | 18.4 | 10.8 | 75 | 9.3 | 0.5–17.2 | 27.6 | 11.8 |
| Female | 11 | 8.2 | 0.5–16.3 | 18.4 | 8.3 | 33 | 8.3 | 0.5–16.8 | 27.7 | 13.0 |
| Male | 14 | 10.3 | 3.0–17.9 | 18.4 | 12.8 | 42 | 10 | 2.0–17.2 | 27.5 | 10.9 |
| Other (all) | 26 | 8.3 | 1.4–16.3 | 21.9 | 8.2 | 78 | 8.2 | 1.3–16.5 | 26.9 | 8.3 |
| Female | 8 | 6.3 | 1.4–13.6 | 22.5 | 7.4 | 24 | 6.2 | 1.3–13.5 | 28.1 | 8.3 |
| Male | 18 | 9.2 | 2.3–16.3 | 21.6 | 8.7 | 54 | 9.1 | 2.0–16.5 | 26.4 | 5.1 |
| Caucasian (all) | 85 | 8.3 | 0.6–19.2 | 23.8 | 7.8 | 255 | 8.2 | 0.1–19.8 | 31.8 | 10.7 |
| Female | 39 | 8.5 | 0.6–17.3 | 24.4 | 7.9 | 117 | 8.4 | 0.1–17.8 | 33.0 | 11.7 |
| Male | 46 | 8.1 | 0.5–19.2 | 23.3 | 7.8 | 138 | 8.0 | 0.03–19.8 | 30.7 | 9.8 |
| Total | 136 | 8.5 | 0.5–19.2 | 22.4 | 8.7 | 408 | 8.4 | 0.03–19.8 | 30.1 | 10.7 |
| Variable | Oncology | Control | Overall | p-Value |
|---|---|---|---|---|
| (n = 136) | (n = 408) | (n = 544) | ||
| Race | >0.99 | |||
| Caucasian | 85 (62.5%) | 255 (62.5%) | 340 (62.5%) | |
| Black | 25 (18.4%) | 75 (18.4%) | 100 (18.4%) | |
| Other | 26 (19.1%) | 78 (19.1%) | 104 (19.1%) | |
| Sex | >0.99 | |||
| Female | 58 (42.6%) | 174 (42.6%) | 232 (42.6%) | |
| Male | 78 (57.4%) | 234 (57.4%) | 312 (57.4%) | |
| Age | 0.8 | |||
| Mean (SD) | 8.50 (4.98) | 8.38 (4.93) | 8.41 (4.94) | |
| Median [min, max] | 8.33 [0.493, 19.2] | 8.08 [0.0329, 19.8] | 8.10 [0.0329, 19.8] |
| Variable | Overall (%) | 25(OH)D Classification | Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|---|---|---|
| Deficient (%) | Insufficient (%) | Sufficient (%) | |||||||
| n = 544 | n = 113 | n = 208 | n = 223 | POR (95% CI) | p-Value | Adjusted POR (95% CI) | p-Value | ||
| Group | Oncology | 136 (25) | 54 (39.7) | 57 (41.9) | 25 (18.4) | 0.25 (0.17, 0.36) | <0.001 | 0.22 (0.15, 0.32) | <0.001 |
| Control | 408 (75) | 59 (14.5) | 151 (37.0) | 198 (48.5) | ref | ref | |||
| Race | Caucasian | 340 (62.5) | 50 (14.7) | 130 (38.2) | 160 (47.1) | ref | ref | ||
| Black | 100 (18.4) | 39 (39.0) | 28 (28.0) | 33 (33.0) | 0.39 (0.25, 0.59) | <0.001 | 0.40 (0.26, 0.62) | <0.001 | |
| Other | 104 (19.1) | 24 (23.1) | 50 (48.1) | 30 (28.8) | 0.52(0.34, 0.78) | 0.002 | 0.49 (0.32, 0.75) | 0.001 | |
| Sex | Female | 232 (42.6) | 43 (18.5) | 84 (36.2) | 105 (45.3) | 1.33 (0.97, 1.83) | 0.078 | 1.24 (0.89, 1.74) | 0.204 |
| Male | 312 (57.4) | 70 (22.4) | 124 (39.7) | 118 (37.8) | ref | ref | |||
| Age | mean (SEM) | 8.41 (0.21) | 10.50 (0.45) | 8.90 (0.34) | 6.90 (0.31) | 0.89 (0.87, 0.92) | <0.001 | 0.89 (0.86, 0.92) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fullmer, M.; Su, A.; Bachrach, S.; Hossain, J.; Kecskemethy, H.H. Newly Diagnosed Children with Cancer Have Lower 25-Vitamin D Levels than Their Cancer-Free Peers: A Comparison across Age, Race, and Sex. Cancers 2022, 14, 2378. https://doi.org/10.3390/cancers14102378
Fullmer M, Su A, Bachrach S, Hossain J, Kecskemethy HH. Newly Diagnosed Children with Cancer Have Lower 25-Vitamin D Levels than Their Cancer-Free Peers: A Comparison across Age, Race, and Sex. Cancers. 2022; 14(10):2378. https://doi.org/10.3390/cancers14102378
Chicago/Turabian StyleFullmer, Michell, Annelise Su, Steven Bachrach, Jobayer Hossain, and Heidi H. Kecskemethy. 2022. "Newly Diagnosed Children with Cancer Have Lower 25-Vitamin D Levels than Their Cancer-Free Peers: A Comparison across Age, Race, and Sex" Cancers 14, no. 10: 2378. https://doi.org/10.3390/cancers14102378
APA StyleFullmer, M., Su, A., Bachrach, S., Hossain, J., & Kecskemethy, H. H. (2022). Newly Diagnosed Children with Cancer Have Lower 25-Vitamin D Levels than Their Cancer-Free Peers: A Comparison across Age, Race, and Sex. Cancers, 14(10), 2378. https://doi.org/10.3390/cancers14102378