
Fecal microRNAs, Fecal microRNA Panels, or Combinations of Fecal microRNAs with Fecal Hemoglobin for Early Detection of Colorectal Cancer and Its Precursors: A Systematic Review

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment of Each Study
3. Results
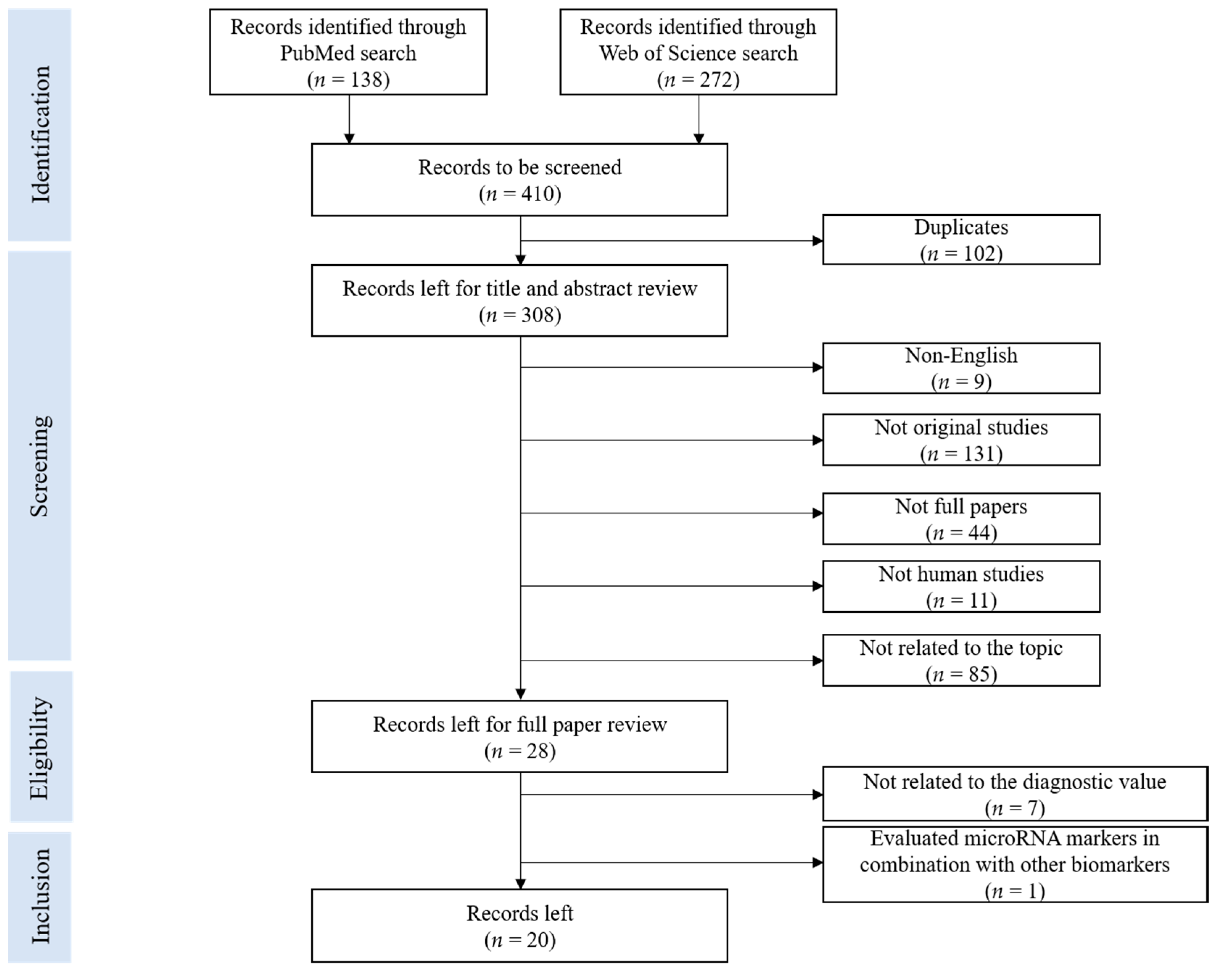
3.1. Literature Search Result
3.2. Study Characteristics
3.3. Fecal miRNA Detection Methods
3.4. Diagnostic Performance of Fecal miRNA Markers for Detection of Colorectal Neoplasms
3.5. Assessment of Risk of Bias across Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Shaukat, A.; Mongin, S.J.; Geisser, M.S.; Lederle, F.A.; Bond, J.H.; Mandel, J.S.; Church, T.R. Long-term mortality after screening for colorectal cancer. N. Engl. J. Med. 2013, 369, 1106–1114. [Google Scholar] [CrossRef]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Krist, A.H.; Kubik, M.; et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 1965–1977. [Google Scholar] [CrossRef] [PubMed]
- Reumkens, A.; Rondagh, E.J.; Bakker, C.M.; Winkens, B.; Masclee, A.A.; Sanduleanu, S. Post-Colonoscopy Complications: A Systematic Review, Time Trends, and Meta-Analysis of Population-Based Studies. Am. J. Gastroenterol. 2016, 111, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O’Connor, E.; Smith, N.; Whitlock, E.P. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 2576–2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Kim, H.S.; Park, H.J. Adverse events related to colonoscopy: Global trends and future challenges. World J. Gastroenterol. 2019, 25, 190–204. [Google Scholar] [CrossRef] [PubMed]
- Paszat, L.F.; Sutradhar, R.; Luo, J.; Rabeneck, L.; Tinmouth, J. Perforation and post-polypectomy bleeding complicating colonoscopy in a population-based screening program. Endosc. Int. Open 2021, 9, E637–E645. [Google Scholar] [CrossRef] [PubMed]
- Helsingen, L.; Vandvik, P.; Jodal, H.; Agoritsas, T.; Lytvyn, L.; Anderson, J.; Auer, R.; Murphy, S.; Almadi, M.; Corley, D.; et al. Colorectal cancer screening with faecal immunochemical testing, sigmoidoscopy or colonoscopy: A clinical practice guideline. BMJ 2019, 367, l5515. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, R.; Guo, F.; Heisser, T.; Hoffmeister, M.; Brenner, H. Utilisation of Colorectal Cancer Screening Tests in European Countries by Type of Screening Offer: Results from the European Health Interview Survey. Cancers 2020, 12, 1409. [Google Scholar] [CrossRef]
- Niedermaier, T.; Balavarca, Y.; Brenner, H. Stage-Specific Sensitivity of Fecal Immunochemical Tests for Detecting Colorectal Cancer: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2020, 115, 56–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niedermaier, T.; Tikk, K.; Gies, A.; Bieck, S.; Brenner, H. Sensitivity of Fecal Immunochemical Test for Colorectal Cancer Detection Differs According to Stage and Location. Clin. Gastroenterol. Hepatol. 2020, 18, 2920–2928.e6. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. Metazoan MicroRNAs. Cell 2018, 173, 20–51. [Google Scholar] [CrossRef] [Green Version]
- Bracken, C.P.; Scott, H.S.; Goodall, G.J. A network-biology perspective of microRNA function and dysfunction in cancer. Nat. Rev. Genet. 2016, 17, 719–732. [Google Scholar] [CrossRef]
- Peng, Y.; Croce, C.M. The role of MicroRNAs in human cancer. Signal Transduct. Target. Ther. 2016, 1, 15004. [Google Scholar] [CrossRef] [Green Version]
- Strubberg, A.M.; Madison, B.B. MicroRNAs in the etiology of colorectal cancer: Pathways and clinical implications. Dis. Model. Mech. 2017, 10, 197–214. [Google Scholar] [CrossRef] [Green Version]
- Dragomir, M.P.; Kopetz, S.; Ajani, J.A.; Calin, G.A. Non-coding RNAs in GI cancers: From cancer hallmarks to clinical utility. Gut 2020, 69, 748–763. [Google Scholar] [CrossRef] [PubMed]
- Al-Akhrass, H.; Christou, N. The Clinical Assessment of MicroRNA Diagnostic, Prognostic, and Theranostic Value in Colorectal Cancer. Cancers 2021, 13, 13122916. [Google Scholar] [CrossRef]
- Duran-Sanchon, S.; Moreno, L.; Auge, J.M.; Serra-Burriel, M.; Cuatrecasas, M.; Moreira, L.; Martin, A.; Serradesanferm, A.; Pozo, A.; Costa, R.; et al. Identification and Validation of MicroRNA Profiles in Fecal Samples for Detection of Colorectal Cancer. Gastroenterology 2020, 158, 947–957.e4. [Google Scholar] [CrossRef]
- Raut, J.R.; Schöttker, B.; Holleczek, B.; Guo, F.; Bhardwaj, M.; Miah, K.; Schrotz-King, P.; Brenner, H. A microRNA panel compared to environmental and polygenic scores for colorectal cancer risk prediction. Nat. Commun. 2021, 12, 4811. [Google Scholar] [CrossRef]
- Bandini, E. Urinary microRNA and mRNA in Tumors. Methods Mol. Biol. 2021, 2292, 57–72. [Google Scholar] [CrossRef]
- Glinge, C.; Clauss, S.; Boddum, K.; Jabbari, R.; Jabbari, J.; Risgaard, B.; Tomsits, P.; Hildebrand, B.; Kääb, S.; Wakili, R.; et al. Stability of Circulating Blood-Based MicroRNAs-Pre-Analytic Methodological Considerations. PLoS ONE 2017, 12, e0167969. [Google Scholar] [CrossRef]
- Wu, C.W.; Ng, S.S.; Dong, Y.J.; Ng, S.C.; Leung, W.W.; Lee, C.W.; Wong, Y.N.; Chan, F.K.; Yu, J.; Sung, J.J. Detection of miR-92a and miR-21 in stool samples as potential screening biomarkers for colorectal cancer and polyps. J. Gut 2012, 61, 739–745. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.J.; Ren, L.L.; Wang, Z.H.; Sun, T.T.; Yu, Y.N.; Wang, Y.C.; Yan, T.T.; Zou, W.; He, J.; Zhang, Y.; et al. MiR-194 deregulation contributes to colorectal carcinogenesis via targeting AKT2 pathway. Theranostics 2014, 4, 1193–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yau, T.O.; Wu, C.W.; Dong, Y.; Tang, C.M.; Ng, S.S.; Chan, F.K.; Sung, J.J.; Yu, J. microRNA-221 and microRNA-18a identification in stool as potential biomarkers for the non-invasive diagnosis of colorectal carcinoma. Br. J. Cancer 2014, 111, 1765–1771. [Google Scholar] [CrossRef]
- Wu, C.W.; Ng, S.C.; Dong, Y.; Tian, L.; Ng, S.S.; Leung, W.W.; Law, W.T.; Yau, T.O.; Chan, F.K.; Sung, J.J.; et al. Identification of microRNA-135b in stool as a potential noninvasive biomarker for colorectal cancer and adenoma. Clin. Cancer Res. 2014, 20, 2994–3002. [Google Scholar] [CrossRef] [Green Version]
- Yau, T.O.; Wu, C.W.; Tang, C.M.; Chen, Y.; Fang, J.; Dong, Y.; Liang, Q.; Ng, S.S.; Chan, F.K.; Sung, J.J.; et al. MicroRNA-20a in human faeces as a non-invasive biomarker for colorectal cancer. Oncotarget 2016, 7, 1559–1568. [Google Scholar] [CrossRef] [Green Version]
- Chang, P.Y.; Chen, C.C.; Chang, Y.S.; Tsai, W.S.; You, J.F.; Lin, G.P.; Chen, T.W.; Chen, J.S.; Chan, E.C. MicroRNA-223 and microRNA-92a in stool and plasma samples act as complementary biomarkers to increase colorectal cancer detection. Oncotarget 2016, 7, 10663–10675. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Xu, A.; Li, J.; Fu, J.; Wang, G.; Yang, Y.; Cui, L.; Sun, J. Fecal miR-29a and miR-224 as the noninvasive biomarkers for colorectal cancer. Cancer Biomark. 2016, 16, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Gong, W.; Lou, J.; Ju, H.; Yin, X.; Liu, Y.; Tian, Z. MicroRNA-21 and microRNA-146a identification in stool and its clinical significance in colorectal neoplasms. Int. J. Clin. Exp. Med. 2016, 9, 16441–16449. [Google Scholar]
- Li, L.; Wang, A.; Cai, M.; Tong, M.; Chen, F.; Huang, L. Identification of stool miR-135b-5p as a non-invasive diaognostic biomarker in later tumor stage of colorectal cancer. Life Sci. 2020, 260, 118417. [Google Scholar] [CrossRef] [PubMed]
- Ghanbari, R.; Mosakhani, N.; Sarhadi, V.K.; Armengol, G.; Nouraee, N.; Mohammadkhani, A.; Khorrami, S.; Arefian, E.; Paryan, M.; Malekzadeh, R.; et al. Simultaneous Underexpression of let-7a-5p and let-7f-5p microRNAs in Plasma and Stool Samples from Early Stage Colorectal Carcinoma. Biomark. Cancer 2015, 7, 39–48. [Google Scholar] [CrossRef] [Green Version]
- Ghanbari, R.; Mosakhani, N.; Asadi, J.; Nouraee, N.; Mowla, S.J.; Poustchi, H.; Malekzadeh, R.; Knuutila, S. Decreased expression of fecal miR-4478 and miR-1295b-3p in early-stage colorectal cancer. Cancer Biomark. 2015, 15, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Bastaminejad, S.; Taherikalani, M.; Ghanbari, R.; Akbari, A.; Shabab, N.; Saidijam, M. Investigation of MicroRNA-21 Expression Levels in Serum and Stool as a Potential Non-Invasive Biomarker for Diagnosis of Colorectal Cancer. Iran. Biomed. J. 2017, 21, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Koga, Y.; Yasunaga, M.; Takahashi, A.; Kuroda, J.; Moriya, Y.; Akasu, T.; Fujita, S.; Yamamoto, S.; Baba, H.; Matsumura, Y. MicroRNA Expression Profiling of Exfoliated Colonocytes Isolated from Feces for Colorectal Cancer Screening. Cancer Prev. Res. 2010, 3, 1435–1442. [Google Scholar] [CrossRef] [Green Version]
- Koga, Y.; Yamazaki, N.; Yamamoto, Y.; Yamamoto, S.; Saito, N.; Kakugawa, Y.; Otake, Y.; Matsumoto, M.; Matsumura, Y. Fecal miR-106a Is a Useful Marker for Colorectal Cancer Patients with False-Negative Results in Immunochemical Fecal Occult Blood Test. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1844–1852. [Google Scholar] [CrossRef] [Green Version]
- Phua, L.C.; Chue, X.P.; Koh, P.K.; Cheah, P.Y.; Chan, E.C.; Ho, H.K. Global fecal microRNA profiling in the identification of biomarkers for colorectal cancer screening among Asians. Oncol. Rep. 2014, 32, 97–104. [Google Scholar] [CrossRef]
- Choi, H.H.; Cho, Y.S.; Choi, J.H.; Kim, H.K.; Kim, S.S.; Chae, H.S. Stool-Based miR-92a and miR-144* as Noninvasive Biomarkers for Colorectal Cancer Screening. Oncology 2019, 97, 173–179. [Google Scholar] [CrossRef]
- Wu, C.W.; Cao, X.; Berger, C.K.; Foote, P.H.; Mahoney, D.W.; Simonson, J.A.; Anderson, B.W.; Yab, T.C.; Taylor, W.R.; Boardman, L.A.; et al. Novel Approach to Fecal Occult Blood Testing by Assay of Erythrocyte-Specific microRNA Markers. Dig. Dis. Sci. 2017, 62, 1985–1994. [Google Scholar] [CrossRef]
- Kalimutho, M.; Blanco, G.D.V.; Di Cecilia, S.; Sileri, P.; Cretella, M.; Pallone, F.; Federici, G.; Bernardini, S. Differential expression of miR-144* as a novel fecal-based diagnostic marker for colorectal cancer. J. Gastroenterol. 2011, 46, 1391–1402. [Google Scholar] [CrossRef]
- Rotelli, M.T.; Di Lena, M.; Cavallini, A.; Lippolis, C.; Bonfrate, L.; Chetta, N.; Portincasa, P.; Altomare, D.F. Fecal microRNA profile in patients with colorectal carcinoma before and after curative surgery. Int. J. Colorectal Dis. 2015, 30, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Duran-Sanchon, S.; Moreno, L.; Gómez-Matas, J.; Augé, J.M.; Serra-Burriel, M.; Cuatrecasas, M.; Moreira, L.; Serradesanferm, A.; Pozo, À.; Grau, J.; et al. Fecal MicroRNA-Based Algorithm Increases Effectiveness of Fecal Immunochemical Test-Based Screening for Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2021, 19, 323–330.e1. [Google Scholar] [CrossRef]
- miRBase. Available online: https://www.mirbase.org/ (accessed on 20 September 2021).
- Koga, Y.; Yasunaga, M.; Moriya, Y.; Akasu, T.; Fujita, S.; Yamamoto, S.; Matsumura, Y. Exosome can prevent RNase from degrading microRNA in feces. J. Gastrointest. Oncol. 2011, 2, 215–222. [Google Scholar] [CrossRef]
- Liu, S.; da Cunha, A.P.; Rezende, R.M.; Cialic, R.; Wei, Z.; Bry, L.; Comstock, L.E.; Gandhi, R.; Weiner, H.L. The Host Shapes the Gut Microbiota via Fecal microRNA. Cell Host Microbe 2016, 19, 32–43. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.; Rutjes, A.W.; Reitsma, J.B.; Glas, A.S.; Bossuyt, P.M.; Kleijnen, J. Sources of variation and bias in studies of diagnostic accuracy: A systematic review. Ann. Intern. Med. 2004, 140, 189–202. [Google Scholar] [CrossRef]
- Backes, C.; Meese, E.; Keller, A. Specific miRNA Disease Biomarkers in Blood, Serum and Plasma: Challenges and Prospects. Mol. Diagn. Ther. 2016, 20, 509–518. [Google Scholar] [CrossRef]
- Jenike, A.E.; Halushka, M.K. miR-21: A non-specific biomarker of all maladies. Biomark. Res. 2021, 9, 18. [Google Scholar] [CrossRef]
- Kohn, M.A.; Carpenter, C.R.; Newman, T.B. Understanding the direction of bias in studies of diagnostic test accuracy. Acad. Emerg. Med. 2013, 20, 1194–1206. [Google Scholar] [CrossRef]
- Yamazaki, N.; Koga, Y.; Yamamoto, S.; Kakugawa, Y.; Otake, Y.; Hayashi, R.; Saito, N.; Matsumura, Y. Application of the Fecal MicroRNA Test to the Residuum from the Fecal Occult Blood Test. Jpn. J. Clin. Oncol. 2013, 43, 726–733. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Kowdley, K.V. Method for microRNA isolation from clinical serum samples. Anal. Biochem. 2012, 431, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meerson, A.; Ploug, T. Assessment of six commercial plasma small RNA isolation kits using qRT-PCR and electrophoretic separation: Higher recovery of microRNA following ultracentrifugation. Biol. Methods Protoc. 2016, 1, bpw003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzenbach, H.; da Silva, A.M.; Calin, G.; Pantel, K. Data Normalization Strategies for MicroRNA Quantification. Clin. Chem. 2015, 61, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Calin, G.A.; Croce, C.M. Genomics of chronic lymphocytic leukemia microRNAs as new players with clinical significance. Semin. Oncol. 2006, 33, 167–173. [Google Scholar] [CrossRef] [PubMed]
- McGauran, N.; Wieseler, B.; Kreis, J.; Schüler, Y.B.; Kölsch, H.; Kaiser, T. Reporting bias in medical research—A narrative review. Trials 2010, 11, 37. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| First Author (Year) [Ref.] | Case-Finding Country | Cases vs. Controls | miRNA | AUC | p-Value | SEN (%) | SPE (%) | Validation | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Study Group | N | Internal | External | |||||||
| Wu, C.W., et al. (2012) [23] | CS + TS Hong Kong (China) | CRC Cn | 88 101 | miR-21 | 0.64 | - | 56 | 73 | - | - |
| miR-92a | 0.78 | - | 72 | 73 | ||||||
| Zhao, H.J., et al. (2014) [26] | CS China | CRC Cn | 28 20 | miR-194 | 0.74 | <0.0001 | 60 | 88 | - | - |
| Yau, T.O., et al. (2014) [27] | CS Hong Kong (China) | CRC Cn | 198 198 | miR-18a | 0.67 | - | 61 | 69 | - | - |
| miR-221 | 0.73 | - | 62 | 74 | ||||||
| Wu, C.W., et al. (2014) [28] | CS Hong Kong (China) | CRC Cn | 104 109 | miR-135b | 0.79 | - | 78 | 68 | - | - |
| Yau, T.O., et al. (2016) [29] | CS Hong Kong (China) | CRC Cn | 198 198 | miR-20a | 0.73 | - | 55 | 82 | - | - |
| Chang, P.Y., et al. (2016) [30] | CS Taiwan (China) | CRC Cn | 62/76 62/247 | miR-223 | 0.79/0.80 | <0.001 | - | - | Yes | - |
| miR-92a | 0.79/0.75 | <0.001 | - | - | ||||||
| miR-16 | 0.73/0.70 | <0.001 | - | - | ||||||
| miR-20a | 0.72/0.64 | <0.001 | - | - | ||||||
| miR-106b | 0.71/0.71 | <0.001 | - | - | ||||||
| Zhu, Y., et al. (2016) [31] | CS China | CRC Cn | 80 51 | miR-29a | 0.78 | <0.001 | 85 | 61 | - | - |
| miR-223 | 0.65 | 0.004 | 60 | 71 | ||||||
| miR-224 | 0.75 | <0.001 | 75 | 63 | ||||||
| Liu, H., et al. (2016) [32] | CS China | CRC Cn | 150 98 | miR-21 | 0.88 | - | 90 | 75 | - | - |
| miR-146a | 0.79 | - | 77 | 68 | ||||||
| Li, L., et al. (2020) [33] | CS China | CRC Cn | 77 29 | miR-135b-5p | 0.87 | - | 97 | 74 | - | - |
| Ghanbari, R., et al. (2015) [34] | CS Iran | CRC Cn | 51 26 | let-7f-5p | 0.71 | 0.003 | - | - | - | - |
| Ghanbari, R., et al. (2015) [35] | CS Iran | CRC Cn | 40 16 | miR-4478 | 0.7 | 0.017 | - | - | - | - |
| miR-1295b-3p | 0.71 | 0.014 | - | - | ||||||
| Bastaminejad, S., et al. (2017) [36] | CS Iran | CRC Cn | 40 40 | miR-21 | 0.83 | - | 86 | 81 | - | - |
| Koga, Y., et al. (2010) [37] a | CS Japan | CRC Cn | 206 134 | miR-17 | - | - | 16 | 89 | - | - |
| miR-18a | - | - | 47 | 94 | ||||||
| miR-19a | - | - | 53 | 89 | ||||||
| miR-19b | - | - | 16 | 91 | ||||||
| miR-20a | - | - | 18 | 92 | ||||||
| miR-92a | - | - | 22 | 91 | ||||||
| miR-21 | - | - | 15 | 92 | ||||||
| miR-135a | - | - | 15 | 100 | ||||||
| miR-135b | - | - | 46 | 95 | ||||||
| Koga, Y., et al. (2013) [38] | CS Japan | CRC Cn | 117 107 | miR-106a | - | - | 34 | 97 | - | - |
| Phua, L.C., et al. (2014) [39] | CS Singapore | CRC Cn | 17 28 | miR-223 | 0.94 | - | 77 | 96 | - | - |
| miR-451 | 0.97 | - | 88 | 100 | ||||||
| Choi, H.H., et al. (2019) [40] | CS Korea | CRC Cn | 29 29 | miR-21 | 0.69 | - | 79 | 48 | - | - |
| miR-92a | 0.76 | - | 90 | 52 | ||||||
| miR-144* | 0.77 | - | 79 | 67 | ||||||
| miR-17-3p | 0.71 | - | 68 | 71 | ||||||
| Kalimutho, M., et al. (2011) [42] | CS Italy | CRC Cn | 35 40 | miR-144* | 0.83 | - | 74 | 87 | - | - |
| Rotelli, M., et al. (2015) [43] b | CS Italy | CRC Cn | 20 20 | miR-20a-5p | 0.84 | - | - | - | - | - |
| miR-21-3p | 0.66 | - | - | - | ||||||
| miR-141 | 0.84 | - | - | - | ||||||
| First Author (Year) [Ref.] | Cases vs. Controls | Panel | No. of miRNA | AUC | p-Value | SEN (%) | SPE (%) | |
|---|---|---|---|---|---|---|---|---|
| Study Group | N | |||||||
| Wu, C.W., et al. (2012) [23] | CRC Cn | 88 101 | Panel A | 2 | - | - | 82 | 57 |
| Yau, T.O., et al. (2014) [27] | CRC Cn | 198 198 | Panel B | 2 | 0.75 | - | 66 | 75 |
| Panel C | 2 | 0.78 | - | 66 | 80 | |||
| Panel D | 2 | 0.75 | - | 66 | 75 | |||
| Panel E | 3 | 0.79 | - | 71 | 74 | |||
| Yau, T.O., et al. (2016) [29] | CRC Cn | 198 198 | Panel F | 2 | 0.79 | - | 79 | 65 |
| Panel G | 2 | 0.77 | - | 57 | 84 | |||
| Chang, P.Y., et al. (2016) [30] | CRC Cn | 62 62 | Panel H | 4 | 0.84 | - | - | - |
| Panel I | 2 | 0.81 | - | - | - | |||
| Liu, H., et al. (2016) [32] | CRC Cn | 150 98 | Panel J | 2 | 0.88 | - | 87 | 82 |
| Koga, Y., et al. (2010) [37] a | CRC Cn | 206 134 | Panel K | 2 | - | - | 46 | 95 |
| Panel L | 9 | - | - | 74 | 79 | |||
| Panel M | 6 | - | - | 70 | 82 | |||
| Choi, H., et al. (2019) [40] | CRC Cn | 29 29 | Panel N | 2 | - | - | 97 | 38 |
| Wu, C.W., et al. (2017) [41] | CRC Cn | 29 115 | Panel O | 2 | 0.89 | <0.0001 | 66 | 95 |
| First Author (Year) [Ref.] | Case-Finding Country | Cases vs. Controls | miRNAs | AUC | p-Value | SEN (%) | SPE (%) | |
|---|---|---|---|---|---|---|---|---|
| Study Group | N | |||||||
| Wu, C.W., et al. (2012) [23] | CS + TS Hong Kong (China) | CRA Cn | 57 101 | miR-92a | - | - | 56 | 73 |
| Panel A | - | - | 68 | 57 | ||||
| Wu, C.W., et al. (2014) [28] | CS Hong Kong (China) | AA NAA Cn | 59 110 109 | miR-135b | - | - | 61 a 73 b | 68 a 68 b |
| Yau, T.O., et al. (2016) [29] | CS Hong Kong (China) | CRA Cn | 199 198 | miR-20a | 0.41 | - | - | - |
| Liu, H., et al. (2016) [32] | CS China | CRA Cn | 120 98 | miR-21 | 0.77 | - | 85 | 63 |
| Panel J | 0.76 | - | 79 | 67 | ||||
| Wu, C.W., et al. (2017) [41] | CS USA | AA Cn | 31 115 | Panel O | 0.58 | 0.24 | - | - |
| First Author (Year) Ref. | Biomarker | Outcomes | AUC | p-Value | SEN (%) | SPE (%) | NPV (%) | PPV (%) |
|---|---|---|---|---|---|---|---|---|
| Duran-Sanchon, S., et al. (2020) [19] Duran-Sanchon, S., et al. (2021) [44] | miR-221-3p | CRC | 0.70 | <0.01 | - | - | - | - |
| miR-25-3p | CRC | 0.70 | <0.05 | - | - | - | - | |
| miR-29a-3p | CRC | 0.69 | <0.05 | - | - | - | - | |
| miR-34a-5p | CRC | 0.71 | <0.01 | - | - | - | - | |
| miR-27a-3p | CRC | 0.69 | <0.05 | - | - | - | - | |
| AA+CRC a | 0.63 | <0.05 | 69 | 52 | - | - | ||
| miR-130b-3p | AA | 0.69 | <0.01 | - | - | - | - | |
| CRC | 0.71 | <0.05 | - | - | - | - | ||
| AA+CRC a | 0.64 | <0.01 | 82 | 39 | - | - | ||
| miR-421 | AA | 0.71 | <0.001 | - | - | - | - | |
| CRC | 0.77 | <0.001 | - | - | - | - | ||
| AA+CRC a | 0.68 | <0.001 | 81 | 43 | - | - | ||
| Panel P | AA | 0.71/0.64 | - | 61/59 | 71/69 | 81/83 | 47/41 | |
| CRC | 0.86/0.74 | - | 96/96 | 36/33 | 94/94 | 47/41 | ||
| AA+CRC | 0.74/0.63 | - | 64/42 | 77/73 | 93/92 | 30/15 | ||
| AA+CRC a | 0.74/0.63 | 74/67 | 63/60 | 88/85 | 40/34 | |||
| Fecal hemoglobin | AA | 0.64/0.59 | - | 50/43 | 68/63 | 72/72 | 45/33 | |
| CRC | 0.70/0.67 | - | 89/100 | 33/31 | 82/100 | 45/33 | ||
| AA+CRC | 0.67/0.59 | - | 53/45 | 75/74 | 93/92 | 19/17 | ||
| AA+CRC a | 0.61/0.62 | 60/62 | 59/58 | 81/85 | 32/27 | |||
| miRFec | AA | 0.70/0.64 | - | 50/49 | 75/71 | 56/58 | 70/63 | |
| CRC | 0.90/0.93 | - | 96/97 | 48/43 | 90/94 | 70/63 | ||
| CRC a | - | - | 70 b | 90 | 94 | - | ||
| - | - | 85 b | 80 | 97 | - | |||
| - | - | 90 b | 70 | 97 | - | |||
| - | - | 93 b | 60 | 98 | - | |||
| - | - | 97 b | 50 | 99 | - | |||
| AA+CRC | 0.74/0.67 | - | 63/48 | 79/75 | 91/90 | 40/22 | ||
| AA+CRC a | 0.72/0.70 | - | 67/68 | 66/64 | 78/81 | 54/47 | ||
| - | - | 30 b | 90 | 52 | - | |||
| - | - | 44 b | 80 | 55 | - | |||
| - | - | 56 b | 70 | 58 | - | |||
| - | - | 70 b | 60 | 63 | - | |||
| - | - | 79 b | 50 | 67 | - | |||
| Probability of detection and positive predictive value for AA and CRC according to the miRFec score | ||||||||
| miRFec Score | Odds Ratio (95% CI) | p-Value | PPV (%) | |||||
| <2.14 | 1 c | - | 29 | |||||
| 2.14–2.64 | 2.71 (1.78–4.13) | <0.001 | 52 | |||||
| 2.65–3.09 | 3.56 (2.33–5.45) | <0.001 | 59 | |||||
| >3.09 | 8.08 (5.11–12.77) | <0.001 | 76 | |||||
| Markers | Duran-Sanchon, S., et al. (2020) [19] | Wu, C.W., et al. (2012) [23] | Zhao, H.J., et al. (2014) [26] | Yau, T.O., et al. (2014) [27] | Wu, C.W., et al. (2014) [28] | Yau, T.O., et al. (2016) [29] | Chang, P.Y., et al. (2016) [30] | Zhu, Y., et al. (2016) [31] | Liu, H., et al. (2016) [32] | Li, L., et al. (2020) [33] | Ghanbari, R., et al. (2015) [34] | Ghanbari, R., et al. (2015) [35] | Bastaminejad, S., et al. (2017) [36] | Koga, Y., et al. (2010) [37] | Koga, Y., et al. (2013) [38] | Phua, L.C., et al. (2014) [39] | Choi, H., et al. (2019) [40] | Wu, C.W., et al. (2017) [41] | Kalimutho, M., et al. (2011) [42] | Rotelli, M., et al. (2015) [43] | Number of Studies |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| miR-21 | ↑○ | ↑○ | ↑△ | ↑○ | ↑△ | 5 | |||||||||||||||
| miR-92a | ↑○ | ↑○ | ↑○ | ↑○ | 4 | ||||||||||||||||
| miR-20a | ↑○ | ↑△ | ↑○ | ↑△ | 4 | ||||||||||||||||
| miR-223 | ↑○ | ↓△ | ↑△ | 3 | |||||||||||||||||
| miR-144-5p | ↑○ | ↑○ | ↑○ | 3 | |||||||||||||||||
| miR-135b | ↑△ | ↑△ | ↑○ | 3 | |||||||||||||||||
| miR-18a | ↑○ | ↑○ | 2 | ||||||||||||||||||
| miR-29a | ↑△ | ↓△ | 2 | ||||||||||||||||||
| miR-451 | ↑△ | ↑○ | 2 | ||||||||||||||||||
| miR-221 | ↑△ | ↑○ | 2 | ||||||||||||||||||
| let-7f-5p | ↓△ | 1 | |||||||||||||||||||
| miR-106a | ↑△ | 1 | |||||||||||||||||||
| miR-1295b-3p | ↓△ | 1 | |||||||||||||||||||
| miR-130b-3p | ↑△ | 1 | |||||||||||||||||||
| miR-135a | ↑○ | 1 | |||||||||||||||||||
| miR-141 | ↑△ | 1 | |||||||||||||||||||
| miR-146a | ↓○ | 1 | |||||||||||||||||||
| miR-16 | ↑○ | 1 | |||||||||||||||||||
| miR-17 | ↑○ | 1 | |||||||||||||||||||
| miR-17-3p | ↑△ | 1 | |||||||||||||||||||
| miR-106b | ↑○ | 1 | |||||||||||||||||||
| miR-194 | ↓△ | 1 | |||||||||||||||||||
| miR-19a | ↑○ | 1 | |||||||||||||||||||
| miR-19b | ↑○ | 1 | |||||||||||||||||||
| miR-21-3p | ↑△ | 1 | |||||||||||||||||||
| miR-224 | ↓△ | 1 | |||||||||||||||||||
| miR-25-3p | ↑△ | 1 | |||||||||||||||||||
| miR-27a-3p | ↑○ | 1 | |||||||||||||||||||
| miR-34a-5p | ↑△ | 1 | |||||||||||||||||||
| miR-421 | ↑○ | 1 | |||||||||||||||||||
| miR-4478 | ↓△ | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Z.; Zhu, A.; Bhardwaj, M.; Schrotz-King, P.; Brenner, H. Fecal microRNAs, Fecal microRNA Panels, or Combinations of Fecal microRNAs with Fecal Hemoglobin for Early Detection of Colorectal Cancer and Its Precursors: A Systematic Review. Cancers 2022, 14, 65. https://doi.org/10.3390/cancers14010065
Zhao Z, Zhu A, Bhardwaj M, Schrotz-King P, Brenner H. Fecal microRNAs, Fecal microRNA Panels, or Combinations of Fecal microRNAs with Fecal Hemoglobin for Early Detection of Colorectal Cancer and Its Precursors: A Systematic Review. Cancers. 2022; 14(1):65. https://doi.org/10.3390/cancers14010065
Chicago/Turabian StyleZhao, Zitong, Anna Zhu, Megha Bhardwaj, Petra Schrotz-King, and Hermann Brenner. 2022. "Fecal microRNAs, Fecal microRNA Panels, or Combinations of Fecal microRNAs with Fecal Hemoglobin for Early Detection of Colorectal Cancer and Its Precursors: A Systematic Review" Cancers 14, no. 1: 65. https://doi.org/10.3390/cancers14010065
APA StyleZhao, Z., Zhu, A., Bhardwaj, M., Schrotz-King, P., & Brenner, H. (2022). Fecal microRNAs, Fecal microRNA Panels, or Combinations of Fecal microRNAs with Fecal Hemoglobin for Early Detection of Colorectal Cancer and Its Precursors: A Systematic Review. Cancers, 14(1), 65. https://doi.org/10.3390/cancers14010065