
Risk of Pharmacological or Hospital Treatment for Depression in Patients with Colorectal Cancer–Associations with Pre-Cancer Lifestyle, Comorbidity and Clinical Factors

 , , ,
, , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
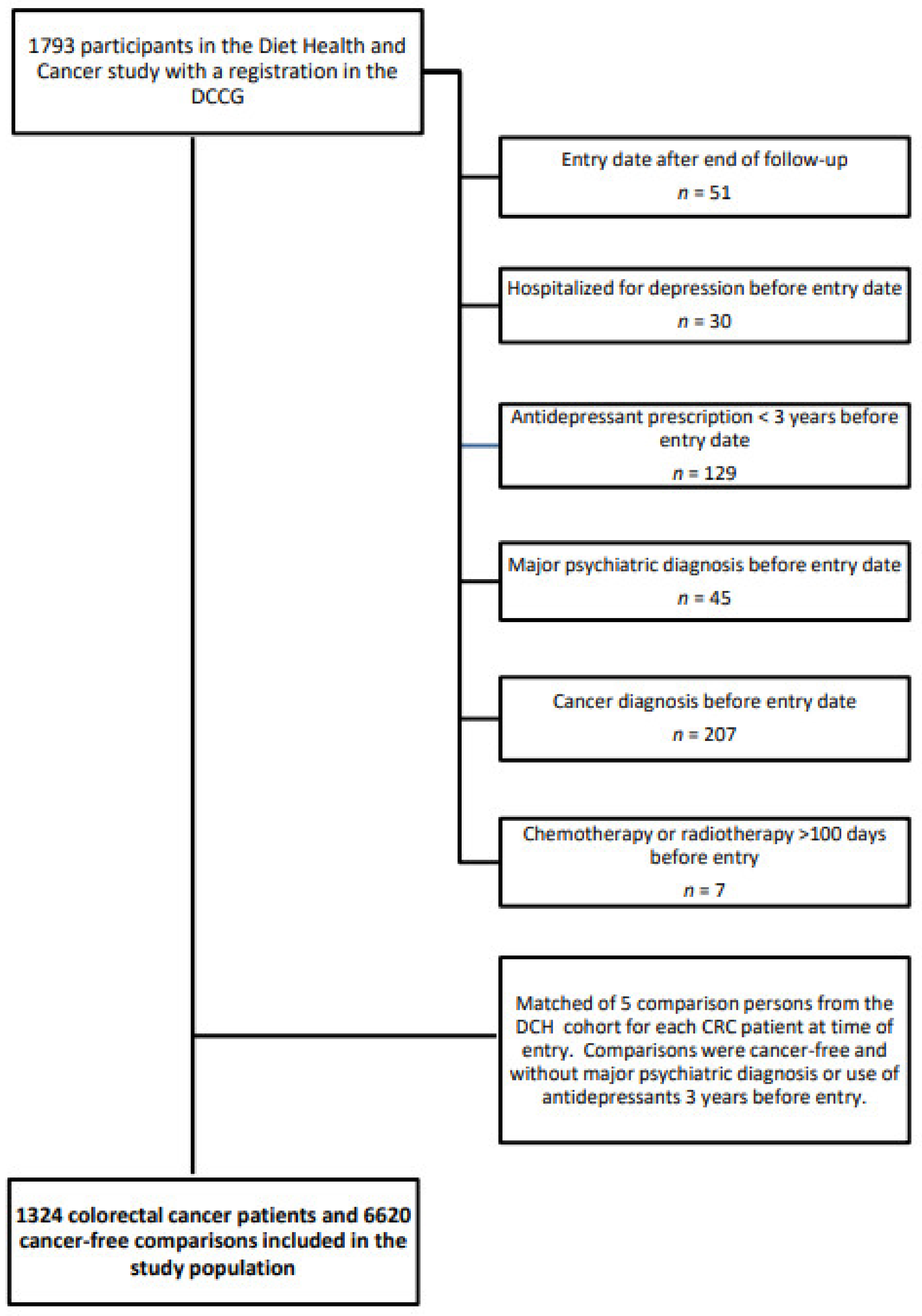
2.1. Study Population
2.2. Information on Hospitalization for Depression and Redeemed Prescription for an Antidepressant
2.3. Covariates
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Przeglad gastroenterologiczny 2019, 14, 89–103. [Google Scholar] [CrossRef]
- El-Shami, K.; Oeffinger, K.C.; Erb, N.L.; Willis, A.; Bretsch, J.K.; Pratt-Chapman, M.L.; Cannady, R.S.; Wong, S.L.; Rose, J.; Barbour, A.L.; et al. American Cancer Society Colorectal Cancer Survivorship Care Guidelines. CA Cancer J. Clin. 2015, 65, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Denlinger, C.S.; Barsevick, A.M. The challenges of colorectal cancer survivorship. J. Natl. Compr. Cancer Netw 2009, 7, 883–893, quiz 94. [Google Scholar] [CrossRef]
- Van Heinsbergen, M.; den Haan, N.; Maaskant-Braat, A.J.; Melenhorst, J.; Belgers, E.H.; Leijtens, J.W.; Bloemen, J.G.; Rutten, H.J.; Bouvy, N.D.; Janssen-Heijnen, M.L.; et al. Functional bowel complaints and quality of life after surgery for colon cancer: Prevalence and predictive factors. Colorectal Dis. 2020, 22, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Eid, Y.; Bouvier, V.; Menahem, B.; Thobie, A.; Dolet, N.; Finochi, M.; Renier, M.; Gardy, J.; Launoy, G.; Dejardin, O.; et al. Digestive and genitourinary sequelae in rectal cancer survivors and their impact on health-related quality of life: Outcome of a high-resolution population-based study. Surgery 2019, 166, 327–335. [Google Scholar] [CrossRef]
- Buccafusca, G.; Proserpio, I.; Tralongo, A.C.; Rametta Giuliano, S.; Tralongo, P. Early colorectal cancer: Diagnosis, treatment and survivorship care. Crit. Rev. Oncol. Hematol. 2019, 136, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Canty, J.; Stabile, C.; Milli, L.; Seidel, B.; Goldfrank, D.; Carter, J. Sexual Function in Women with Colorectal/Anal Cancer. Sex. Med. Rev. 2019, 7, 202–222. [Google Scholar] [CrossRef]
- Bonhof, C.S.; Trompetter, H.R.; Vreugdenhil, G.; van de Poll-Franse, L.V.; Mols, F. Painful and non-painful chemotherapy-induced peripheral neuropathy and quality of life in colorectal cancer survivors: Results from the population-based PROFILES registry. Support. Care Cancer 2020, 28, 5933–5941. [Google Scholar] [CrossRef] [PubMed]
- Beijers, A.J.; Mols, F.; Tjan-Heijnen, V.C.; Faber, C.G.; van de Poll-Franse, L.V.; Vreugdenhil, G. Peripheral neuropathy in colorectal cancer survivors: The influence of oxaliplatin administration. Results from the population-based PROFILES registry. Acta Oncol. 2015, 54, 463–469. [Google Scholar] [CrossRef]
- Mosher, C.E.; Winger, J.G.; Given, B.A.; Helft, P.R.; O’Neil, B.H. Mental health outcomes during colorectal cancer survivorship: A review of the literature. Psychooncology 2016, 25, 1261–1270. [Google Scholar] [CrossRef]
- Peng, Y.N.; Huang, M.L.; Kao, C.H. Prevalence of Depression and Anxiety in Colorectal Cancer Patients: A Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 411. [Google Scholar] [CrossRef]
- Mols, F.; Schoormans, D.; de Hingh, I.; Oerlemans, S.; Husson, O. Symptoms of anxiety and depression among colorectal cancer survivors from the population-based, longitudinal PROFILES Registry: Prevalence, predictors, and impact on quality of life. Cancer 2018, 124, 2621–2628. [Google Scholar] [CrossRef] [PubMed]
- Tjonneland, A.; Olsen, A.; Boll, K.; Stripp, C.; Christensen, J.; Engholm, G.; Overvad, K. Study design, exposure variables, and socioeconomic determinants of participation in Diet, Cancer and Health: A population-based prospective cohort study of 57,053 men and women in Denmark. Scand. J. Public Health 2007, 35, 432–441. [Google Scholar] [CrossRef]
- Pedersen, C.B. The Danish Civil Registration System. Scand. J. Public Health 2011, 39, 22–25. [Google Scholar] [CrossRef]
- Ingeholm, P.; Gogenur, I.; Iversen, L.H. Danish Colorectal Cancer Group Database. Clin. Epidemiol. 2016, 8, 465–468. [Google Scholar] [CrossRef]
- Gjerstorff, M.L. The Danish Cancer Registry. Scand. J. Public Health 2011, 39, 42–45. [Google Scholar] [CrossRef]
- Lynge, E.; Sandegaard, J.L.; Rebolj, M. The Danish National Patient Register. Scand. J. Public Health 2011, 39, 30–33. [Google Scholar] [CrossRef]
- Pottegard, A.; Schmidt, S.A.J.; Wallach-Kildemoes, H.; Sorensen, H.T.; Hallas, J.; Schmidt, M. Data Resource Profile: The Danish National Prescription Registry. Int. J. Epidemiol. 2017, 46, 798-f. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Jensen, V.M.; Rasmussen, A.W. Danish Education Registers. Scand. J. Public Health 2011, 39, 91–94. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Sun, L.M.; Liang, J.A.; Lin, C.L.; Sun, S.; Kao, C.H. Risk of mood disorders in patients with colorectal cancer. J. Affect. Disord. 2017, 218, 59–65. [Google Scholar] [CrossRef]
- Khan, N.F.; Ward, A.M.; Watson, E.; Rose, P.W. Consulting and prescribing behaviour for anxiety and depression in long-term survivors of cancer in the UK. Eur. J. Cancer 2010, 46, 3339–3344. [Google Scholar] [CrossRef] [PubMed]
- Thielen, K.; Nygaard, E.; Andersen, I.; Rugulies, R.; Heinesen, E.; Bech, P.; Bültmann, U.; Diderichsen, F. Misclassification and the use of register-based indicators for depression. Acta Psychiatr. Scand. 2009, 119, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Dalton, S.O.; Laursen, T.M.; Ross, L.; Mortensen, P.B.; Johansen, C. Risk for hospitalization with depression after a cancer diagnosis: A nationwide, population-based study of cancer patients in Denmark from 1973 to 2003. J. Clin. Oncol. 2009, 27, 1440–1445. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.Y.; Cooper, G.S. Recognition of Depression and Anxiety among Elderly Colorectal Cancer Patients. Nurs. Res. Pract. 2010, 2010, 693961. [Google Scholar] [CrossRef]
- Loosbrock, D.L.; Tomlin, M.E.; Robinson, R.L.; Obenchain, R.L.; Croghan, T.W. Appropriateness of prescribing practices for serotonergic antidepressants. Psychiatr. Serv. 2002, 53, 179–184. [Google Scholar] [CrossRef]
- Charles, J.; Britt, H.; Fahridin, S.; Miller, G. Mental health in general practice. Aust. Fam. Physician 2007, 36, 200–201. [Google Scholar]
- Trifiro, G.; Tillati, S.; Spina, E.; Ferrajolo, C.; Alacqua, M.; Aguglia, E.; Rizzi, L.; Caputi, A.P.; Cricelli, C.; Samani, F. A nationwide prospective study on prescribing pattern of antidepressant drugs in Italian primary care. Eur. J. Clin. Pharmacol. 2013, 69, 227–236. [Google Scholar] [CrossRef]
- Larsen, S.B.; Dalton, S.O.; Schuz, J.; Christensen, J.; Overvad, K.; Tjonneland, A.; Johansen, C.; Olsen, A. Mortality among participants and non-participants in a prospective cohort study. Eur. J. Epidemiol. 2012, 27, 837–845. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients with Colorectal Cancer n (%) | Cancer-Free Comparison Persons n (%) | |
|---|---|---|
| Mean age at study entry (SD) | 71.3 (5.98) | 71.3 (5.97) |
| Sex | ||
| Women | 563 (43) | 2815 (43) |
| Men | 761 (58) | 3805 (58) |
| Education 1 | ||
| Long | 337 (26) | 1845 (28) |
| Medium | 743 (57) | 3551 (54) |
| Short | 231 (18) | 1145 (18) |
| Cohabiting 2 | ||
| Yes | 903 (68) | 4479 (68) |
| No | 421 (32) | 2141 (32) |
| Charlson Comorbidity Index Score 3 | ||
| 0–1 | 843 (64) | 4613 (70) |
| 2 | 377 (29) | 1691 (26) |
| ≥3 | 104 (8) | 316 (5) |
| Smoking | ||
| Current | 481 (36) | 2025 (31) |
| Former | 431 (33) | 2171 (33) |
| Never | 411 (31) | 2415 (37) |
| Body Mass Index | ||
| <25 kg/m3 | 506 (38) | 2866 (43) |
| 25–30 kg/m3 | 600 (45) | 2854 (43) |
| >30 kg/m3 | 217 (16) | 896 (14) |
| Alcohol consumption per week 4 | ||
| Abstainers | 83 (6) | 426 (7) |
| Moderate use | 1016 (77) | 5188 (79) |
| Excessive use | 218 (17) | 977 (15) |
| Physical activity (MET-score) 5 | ||
| 4th quartile (most active) | 322 (24) | 1657 (25) |
| 3rd quartile | 327 (25) | 1739 (26) |
| 2nd quartile | 347 (26) | 1603 (24) |
| 1st quartile (least active) | 326 (25) | 1604 (24) |
| Cancer Type | ||
|---|---|---|
| Colon | Rectum | |
| n = 879 (%) | n = 445 (%) | |
| Disease stage | ||
| I | 119 (14) | 97 (24) |
| II | 302 (36) | 99 (24) |
| III | 228 (27) | 121 (30) |
| IV | 186 (22) | 90 (22) |
| Surgery 1 | ||
| No | 90 (10) | 59 (13) |
| Yes | 789 (90) | 386 (87) |
| Surgical complications 1 | ||
| Yes | 404 (46) | 139 (30) |
| Stoma 1 | ||
| Yes | 87 (10) | 203 (46) |
| Chemotherapy 1 | ||
| Yes | 370 (42) | 192 (43) |
| No | 509 (60) | 253 (57) |
| Radiotherapy 1 | ||
| Yes | 68 (8) | 149 (34) |
| No | 811 (92) | 296 (67) |
| Time Since Inclusion | Model 1 1 HR (95% CI) | Model 2 2 HR (95% CI) | Model 3 3 HR (95% CI) |
|---|---|---|---|
| 0–1 year | 13.50 (8.89–20.51) | 13.06 (8.59–19.68) | 12.01 (7.89–18.28) |
| 1–3 years | 9.08 (6.17–13.36) | 9.09 (6.13–13.51) | 8.40 (5.65–12.49) |
| 3–5 years | 6.25 (3.90–10.01) | 6.18 (3.86–9.90) | 5.77 (3.60–9.25) |
| More than 5 years | 2.73 (1.66–4.47) | 2.80 (1.70–4.60) | 2.65 (1.61–4.36) |
| - | Person Years | No Events | Model 1 1 HR (95% CI) | Model 2 2 HR (95% CI) | Model 3 3 HR (95% CI) |
|---|---|---|---|---|---|
| Lifestyle 4 | |||||
| Smoking | |||||
| Current | 1821 | 75 | 1.33 (0.93–1.89) | 1.03 (0.91–1.86) | 1.29 (0.90–1.86) |
| Former | 1920 | 61 | 1.09 (0.75–1.58) | 1.07 (0.74–1.56) | 1.07 (0.73–1.57) |
| Never | 1807 | 55 | reference | reference | reference |
| Alcohol consumption per week 5 | |||||
| Abstainers | 354 | 11 | 0.82 (0.44–1.52) | 0.83 (0.45–1.54) | 0.89 (0.48–1.66) |
| Moderate use | 4286 | 147 | reference | reference | reference |
| Excessive use | 877 | 32 | 1.08 (0.73–1.59) | 1.11 (0.75–1.64) | 1.18 (0.79–1.76) |
| Body Mass Index (kg/m3) | |||||
| <25 | 2121 | 78 | reference | reference | reference |
| >25–30 | 2516 | 80 | 0.88 (0.64–1.21) | 0.85 (0.61–1.17) | 0.89 (0.64–1.23) |
| >30 | 913 | 33 | 0.98 (0.65–1.47) | 0.91 (0.60–1.38) | 1.03 (0.67–1.57) |
| Physical activityMET-score in quartiles 6 | |||||
| 1st quartile (least active) | 1314 | 53 | 1.30 (0.87–1.95) | 1.33 (0.88–1.99) | 1.23 (0.81–1.86) |
| 2nd quartile | 1601 | 50 | 0.98 (0.65–1.48) | 1.02 (0.68–1.54) | 1.04 (0.69–1.59) |
| 3rd quartile | 1279 | 44 | 1.08 (0.71–1.64) | 1.11 (0.72–1.70) | 1.16 (0.76–1.79) |
| 4th quartile (most active) | 1355 | 43 | reference | reference | reference |
| Charlson Comorbidity Index Score 7 | |||||
| 0 | 3307 | 84 | reference | reference | reference |
| 1–2 | 1625 | 67 | 1.77 (1.28–2.46) | 1.72 (1.24–2.40) | 1.74 (1.24–2.43) |
| 3+ | 617 | 40 | 2.73 (1.86–4.02) | 2.63 (1.79–3.88) | 2.74 (1.84–4.09) |
| Clinical factors | |||||
| Cancer type | |||||
| Colon | 3326 | 120 | reference | reference | reference |
| Rectum | 2223 | 71 | 0.96 (0.71–1.30) | 0.94 (0.70–1.28) | 0.90 (0.65–1.23) |
| Stage | |||||
| 1 | 1224 | 32 | reference | reference | reference |
| 2 | 2055 | 50 | 0.90 (0.57–1.40) | 0.90 (0.58–1.40) | 0.88 (0.56–1.38) |
| 3 | 1591 | 50 | 1.14 (0.73–1.78) | 1.12 (0.72–1.76) | 1.10 (0.70–1.73) |
| 4 | 449 | 53 | 3.08 (1.96–4.84) | 3.10 (1.97–4.88) | 3.07 (1.95–4.83) |
| Treatment | |||||
| Surgery | |||||
| no | 337 | 23 | reference | reference | reference |
| yes | 5212 | 168 | 0.77 (0.48–1.26) | 0.77 (0.47–1.24) | 1.28 (0.74–2.24) |
| Surgical complications | |||||
| no | 4474 | 134 | 0.72 (0.44–1.17) | 0.71 (0.44–1.16) | 1.20 (0.68–2.11) |
| yes | 738 | 34 | 1.12 (0.63–1.97) | 1.09 (0.62–1.93) | 1.64 (0.87–3.08) |
| Stoma | |||||
| no | 4253 | 125 | 0.71 (0.44–1.17) | 0.71 (0.44–1.17) | 1.13 (0.64–2.01) |
| yes | 959 | 43 | 1.03 (0.59–1.784 | 0.99 (0.58–1.74) | 1.61 (0.88–2.96) |
| Radiotherapy | |||||
| no | 4863 | 150 | reference | reference | reference |
| yes | 686 | 41 | 2.29 (1.60–3.27) | 2.27 (1.59–3.24) | 2.76 (1.82–4.19) |
| Chemotherapy | |||||
| no | 3608 | 111 | reference | reference | reference |
| yes | 1941 | 80 | 1.42 (1.05–1.92) | 1.42 (1.05–1.93) | 0.98 (0.67–1.42) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kjaer, T.K.; Moustsen-Helms, I.R.; Albieri, V.; Larsen, S.B.; Degett, T.H.; Tjønneland, A.; Johansen, C.; Kjaer, S.K.; Gogenur, I.; Dalton, S.O. Risk of Pharmacological or Hospital Treatment for Depression in Patients with Colorectal Cancer–Associations with Pre-Cancer Lifestyle, Comorbidity and Clinical Factors. Cancers 2021, 13, 1979. https://doi.org/10.3390/cancers13081979
Kjaer TK, Moustsen-Helms IR, Albieri V, Larsen SB, Degett TH, Tjønneland A, Johansen C, Kjaer SK, Gogenur I, Dalton SO. Risk of Pharmacological or Hospital Treatment for Depression in Patients with Colorectal Cancer–Associations with Pre-Cancer Lifestyle, Comorbidity and Clinical Factors. Cancers. 2021; 13(8):1979. https://doi.org/10.3390/cancers13081979
Chicago/Turabian StyleKjaer, Trille Kristina, Ida Rask Moustsen-Helms, Vanna Albieri, Signe Benzon Larsen, Thea Helene Degett, Anne Tjønneland, Christoffer Johansen, Susanne K. Kjaer, Ismail Gogenur, and Susanne Oksbjerg Dalton. 2021. "Risk of Pharmacological or Hospital Treatment for Depression in Patients with Colorectal Cancer–Associations with Pre-Cancer Lifestyle, Comorbidity and Clinical Factors" Cancers 13, no. 8: 1979. https://doi.org/10.3390/cancers13081979
APA StyleKjaer, T. K., Moustsen-Helms, I. R., Albieri, V., Larsen, S. B., Degett, T. H., Tjønneland, A., Johansen, C., Kjaer, S. K., Gogenur, I., & Dalton, S. O. (2021). Risk of Pharmacological or Hospital Treatment for Depression in Patients with Colorectal Cancer–Associations with Pre-Cancer Lifestyle, Comorbidity and Clinical Factors. Cancers, 13(8), 1979. https://doi.org/10.3390/cancers13081979