
The Screen Project: Guided Direct-To-Consumer Genetic Testing for Breast Cancer Susceptibility in Canada




Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Results Disclosure
2.3. Follow-Up
3. Results
3.1. Who Was Tested?
3.2. Who Was Positive?
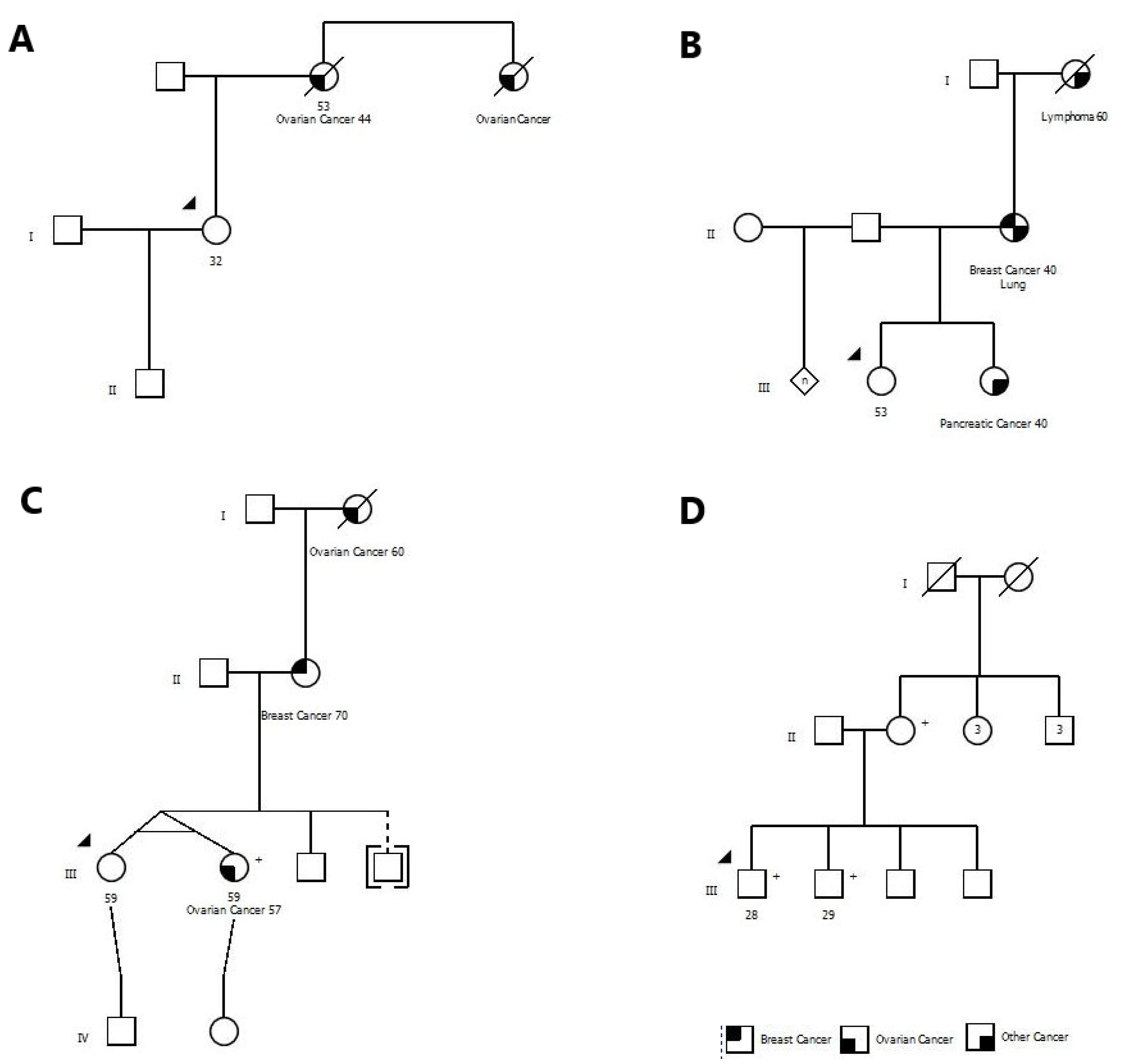
3.3. Pedigree Examples
3.4. Patient Satisfaction
3.5. Preventive Measures Taken by Mutation Carriers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manahan, E.R.; Kuerer, H.M.; Sebastian, M.; Hughes, K.S.; Boughey, J.C.; Euhus, D.M.; Boolbol, S.K.; Taylor, W.A. Consensus Guidelines on Genetic’ Testing for Hereditary Breast Cancer from the American Society of Breast Surgeons. Ann. Surg. Oncol. 2019, 26, 3025–3031. [Google Scholar] [CrossRef]
- Green, M.; Force, U.P.S.T.; Dk, O.; Kw, D.; Ah, K.; Mj, B.; M, C.; Ab, C.; Ca, D.; Jw, E.; et al. Faculty Opinions recommendation of Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: US Preventive Services Task Force Recommendation Statement. Fac. Opin. Post Publ. Peer Rev. Biomed. Lit. 2019, 322, 652–665. [Google Scholar] [CrossRef]
- Nelson, H.D.; Pappas, M.; Cantor, A.; Haney, E.; Holmes, R. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2019, 322, 666–685. [Google Scholar] [CrossRef] [PubMed]
- Domchek, S.; Robson, M. Broadening criteria for BRCA1/2 evaluation: Placing the USPSTF recommendation in context. JAMA 2019, 322, 619–621. [Google Scholar] [CrossRef]
- Rajagopal, P.S.; Nielsen, S.; Olopade, O.I. USPSTF recommendations for BRCA1 and BRCA2 testing in the context of a trans-formative National Cancer Control Plan. JAMA Netw. Open 2019, 2, e1910142. [Google Scholar] [CrossRef]
- Newman, L. US Preventive Services Task Force Breast Cancer Recommendation Statement on Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer. JAMA Surg. 2019, 154, 895. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Guidelines for Genetic/Familial High Risk assessment: Breast and Ovary Version 2 2019. 20 July 2018. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1503 (accessed on 18 August 2020).
- Donenberg, T.; Lunn, J.; Curling, D.; Turnquest, T.; Krill-Jackson, E.; Royer, R.; Narod, S.A.; Hurley, J. A high prevalence of BRCA1 mutations among breast cancer patients from the Bahamas. Breast Cancer Res. Treat. 2010, 125, 591–596. [Google Scholar] [CrossRef]
- Donenberg, T.; Ahmed, H.; Royer, R.; Zhang, S.; Narod, S.A.; George, S.; Akbari, M.R.; Ali, J.; Hurley, J. A Survey of BRCA1, BRCA2, and PALB2 mutations in women with breast cancer in Trinidad and Tobago. Breast Cancer Res. Treat. 2016, 159, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Villarreal-Garza, C.; Weitzel, J.N.; Llacuachaqui, M.; Sifuentes, E.; Magallanes-Hoyos, M.C.; Gallardo, L.; Alvarez-Gómez, R.M.; Herzog, J.; Castillo, D.; Royer, R.; et al. The prevalence of BRCA1 and BRCA2 mutations among young Mexican women with tri-ple-negative breast cancer. Breast Cancer Res. Treat. 2015, 150, 389–394. [Google Scholar] [CrossRef]
- King, M.C.; Levy-Lahad, E.; Lahad, A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA 2014, 312, 1091–1092. [Google Scholar] [CrossRef]
- Hughes, K.S. Genetic Testing: What Problem Are We Trying to Solve? J. Clin. Oncol. 2017, 35, 3789–3791. [Google Scholar] [CrossRef]
- Sie, A.S.; Spruijt, L.; van Zelst-Stams, W.A.; Mensenkamp, A.R.; Ligtenberg, M.J.; Brunner, H.G.; Prins, J.B.; Hoogerbrugge, N. DNA-testing for BRCA1/2 prior to genetic counselling in patients with breast cancer: Design of an intervention study, DNA-direct. BMC Womens Health 2012, 12, 12. [Google Scholar] [CrossRef]
- Beitsch, P.D.; Whitworth, P.W.; Hughes, K.; Patel, R.; Rosen, B.; Compagnoni, G.; Baron, P.; Simmons, R.; Smith, L.A.; Grady, I.; et al. Un-derdiagnosis of hereditary breast cancer: Are genetic testing guidelines a tool or an obstacle? J. Clin. Oncol. 2019, 37, 453–460. [Google Scholar] [CrossRef]
- Ginsburg, O.; Narod, S.A. Clinical Cancer Genetics in a Lower-Middle Income Country: Considerations for Policymaking. J. Glob. Oncol. 2018, 4, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.J.; Reid, J.E.; Wenstrup, R.J. Prevalence of BRCA1 and BRCA2 Mutations in Women with Breast Carcinoma In Situ and Referred for Genetic Testing. Cancer Prev. Res. 2010, 3, 1579–1585. [Google Scholar] [CrossRef]
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Nombela, P.; Lozano, R.; Aytes, A.; Mateo, J.; Olmos, D.; Castro, E. BRCA2 and Other DDR Genes in Prostate Cancer. Cancers 2019, 11, 352. [Google Scholar] [CrossRef] [PubMed]
- Goggins, M.; Overbeek, K.A.; Brand, R.; Syngal, S.; Del Chiaro, M.; Bartsch, D.K.; Bassi, C.; Carrato, A.; Farrell, J.; Fishman, E.K.; et al. Man-agement of patients with increased risk for familial pancreatic cancer: Updated recommendations from the International Cancer of the Pancreas Screening (CAPS) Consortium. Gut 2020, 69, 7–17. [Google Scholar] [CrossRef]
- Giannakeas, V.; Narod, S.A. The expected benefit of preventive mastectomy on breast cancer incidence and mortality in BRCA mutation carriers, by age at mastectomy. Breast Cancer Res. Treat. 2017, 167, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Kotsopoulos, J.; Gronwald, J.; Karlan, B.; Rosen, B.; Huzarski, T.; Moller, P.; Lynch, H.T.; Singer, C.F.; Senter, L.; Neuhausen, S.L.; et al. Age-specific ovarian cancer risks among women with a BRCA1 or BRCA2 mutation. Gynecol. Oncol. 2018, 150, 85–91. [Google Scholar] [CrossRef]
- Knerr, S.; Bowles, E.J.A.; Leppig, K.A.; Buist, D.S.M.; Gao, H.; Wernli, K.J. Trends in BRCA Test Utilization in an Integrated Health System, 2005–2015. J. Natl. Cancer Inst. 2019, 111, 795–802. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Mean (Range) and Frequency (Percent) |
|---|---|
| Mean Age | 47.9 (19–87) |
| Age Group | |
| 18–25 | 18 (1.5) |
| 25–35 | 188 (15.1) |
| 35–50 | 521 (41.9) |
| 50–60 | 320 (25.7) |
| 60+ | 197 (15.8) |
| Missing | 25 |
| Sex | |
| Female | 1157 (93.0) |
| Male | 87 (7.0) |
| Missing | 25 |
| Province | |
| Ontario | 892 (72.2) |
| British Columbia | 117 (9.5) |
| Alberta | 57 (4.6) |
| Saskatchewan | 42 (3.4) |
| Quebec | 40 (3.2) |
| Manitoba | 31 (2.5) |
| Nova Scotia | 28 (2.3) |
| New Brunswick | 14 (1.1) |
| Newfoundland | 8 (0.7) |
| Prince Edward Island | 3 (0.2) |
| Yukon | 2 (0.2) |
| Nunavut | 1 (0.1) |
| Missing | 34 |
| Ethnic group * | |
| Jewish | 89 (7.0) |
| French–Canadian | 118 (9.3) |
| Other white | 1137 (89.6) |
| Asian | 82 (6.5) |
| Aboriginal/indigenous | 25 (2.0) |
| African-American | 12 (0.9) |
| Other | 162 (12.8) |
| Missing | 24 |
| Education | |
| Elementary/other | 14 (1.1) |
| High school | 114 (9.2) |
| Post-secondary | 729 (57.4) |
| Graduate school | 378 (29.8) |
| Missing | 34 |
| Previous cancer | |
| None | 994 (78.5) |
| Breast/DCIS | 196 (15.4) |
| Ovarian | 6 (0.5) |
| Prostate | 10 (0.8) |
| Pancreas | 0 (0.0) |
| Other | 63 (5.0) |
| Source | Number (%) |
|---|---|
| Social media (Facebook, Twitter) | 215 (16.9) |
| Friend | 172 (13.6) |
| Genetic counsellor | 127 (10.0) |
| Internet | 120 (9.5) |
| Family doctor | 120 (9.5) |
| Magazine/newspaper | 107 (8.4) |
| Specialist physician | 59 (4.6) |
| Television | 55 (4.3) |
| Family member | 51 (4.0) |
| Women’s College Hospital | 45 (3.5) |
| Canadian Cancer Society | 4 (0.3) |
| Other | 100 (7.9) |
| Missing | 94 |
| Mutated Gene | Age | Sex | Province | History of Cancer | Number of First or Second Degree Relatives with Cancer | ||
|---|---|---|---|---|---|---|---|
| Breast | Ovary | Other | |||||
| BRCA1 | 44 | M | Ontario | Leukemia | 2 | 0 | 1 |
| BRCA1 | 38 | F | Quebec | 1 | 1 | 0 | |
| BRCA2 | 44 | F | Alberta | 1 | 1 | 0 | |
| BRCA1 | 56 | F | Ontario | Breast | 0 | 0 | 1 |
| BRCA1 | 32 | F | New Brunswick | 0 | 2 | 0 | |
| BRCA2 | 53 | F | Ontario | 1 | 0 | 2 | |
| BRCA2 | 46 | F | British Columbia | Breast | 2 | 0 | 4 |
| BRCA1 | 43 | F | Ontario | 1 | 0 | 1 | |
| BRCA2 | 38 | M | Ontario | 5 | 0 | 2 | |
| BRCA1 | 36 | F | British Columbia | 1 | 0 | 1 | |
| BRCA2 | 38 | F | Ontario | 1 | 0 | 3 | |
| BRCA1 | 40 | M | Ontario | 3 | 0 | 0 | |
| BRCA2 | 32 | M | Ontario | 1 | 0 | 0 | |
| BRCA2 | 40 | F | Nova Scotia | 1 | 0 | 3 | |
| BRCA2 | 35 | M | Ontario | 2 | 0 | 0 | |
| BRCA2 | 59 | F | Alberta | 1 | 2 | 0 | |
| BRCA2 | 45 | M | Quebec | 1 | 0 | 0 | |
| BRCA2 | 51 | F | Ontario | Breast | 1 | 0 | 2 |
| BRCA1 | 28 | M | Ontario | 0 | 0 | 0 | |
| BRCA2 | 42 | F | Ontario | 2 | 0 | 0 | |
| BRCA1 | 29 | M | Ontario | 0 | 0 | 0 | |
| BRCA1 | 52 | F | Ontario | 1 | 0 | 0 | |
| BRCA2 | 30 | F | Newfoundland | Breast | 2 | 0 | 2 |
| BRCA2 | 44 | F | Ontario | 2 | 0 | 1 | |
| BRCA1 | 52 | F | Ontario | Breast | 0 | 0 | 2 |
| BRCA2 | 57 | F | Quebec | Breast | 1 | 1 | 0 |
| BRCA1 | 19 | F | Ontario | 2 | 0 | 0 | |
| BRCA2 | 44 | M | Ontario | 2 | 1 | 2 | |
| BRCA1 | 64 | M | Ontario | 1 | 0 | 0 | |
| BRCA1 | 28 | F | Ontario | 2 | 1 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narod, S.A.; Gojska, N.; Sun, P.; Tryon, A.; Kotsopoulos, J.; Metcalfe, K.; Akbari, M.R. The Screen Project: Guided Direct-To-Consumer Genetic Testing for Breast Cancer Susceptibility in Canada. Cancers 2021, 13, 1894. https://doi.org/10.3390/cancers13081894
Narod SA, Gojska N, Sun P, Tryon A, Kotsopoulos J, Metcalfe K, Akbari MR. The Screen Project: Guided Direct-To-Consumer Genetic Testing for Breast Cancer Susceptibility in Canada. Cancers. 2021; 13(8):1894. https://doi.org/10.3390/cancers13081894
Chicago/Turabian StyleNarod, Steven A., Nicole Gojska, Ping Sun, Angelina Tryon, Joanne Kotsopoulos, Kelly Metcalfe, and Mohammad R. Akbari. 2021. "The Screen Project: Guided Direct-To-Consumer Genetic Testing for Breast Cancer Susceptibility in Canada" Cancers 13, no. 8: 1894. https://doi.org/10.3390/cancers13081894
APA StyleNarod, S. A., Gojska, N., Sun, P., Tryon, A., Kotsopoulos, J., Metcalfe, K., & Akbari, M. R. (2021). The Screen Project: Guided Direct-To-Consumer Genetic Testing for Breast Cancer Susceptibility in Canada. Cancers, 13(8), 1894. https://doi.org/10.3390/cancers13081894