
Analysis of Post-Transplant Lymphoproliferative Disorder (PTLD) Outcomes with Epstein–Barr Virus (EBV) Assessments—A Single Tertiary Referral Center Experience and Review of Literature

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Characteristics of Total Cohort
3.2. PTLD Histologic Subtype Profile
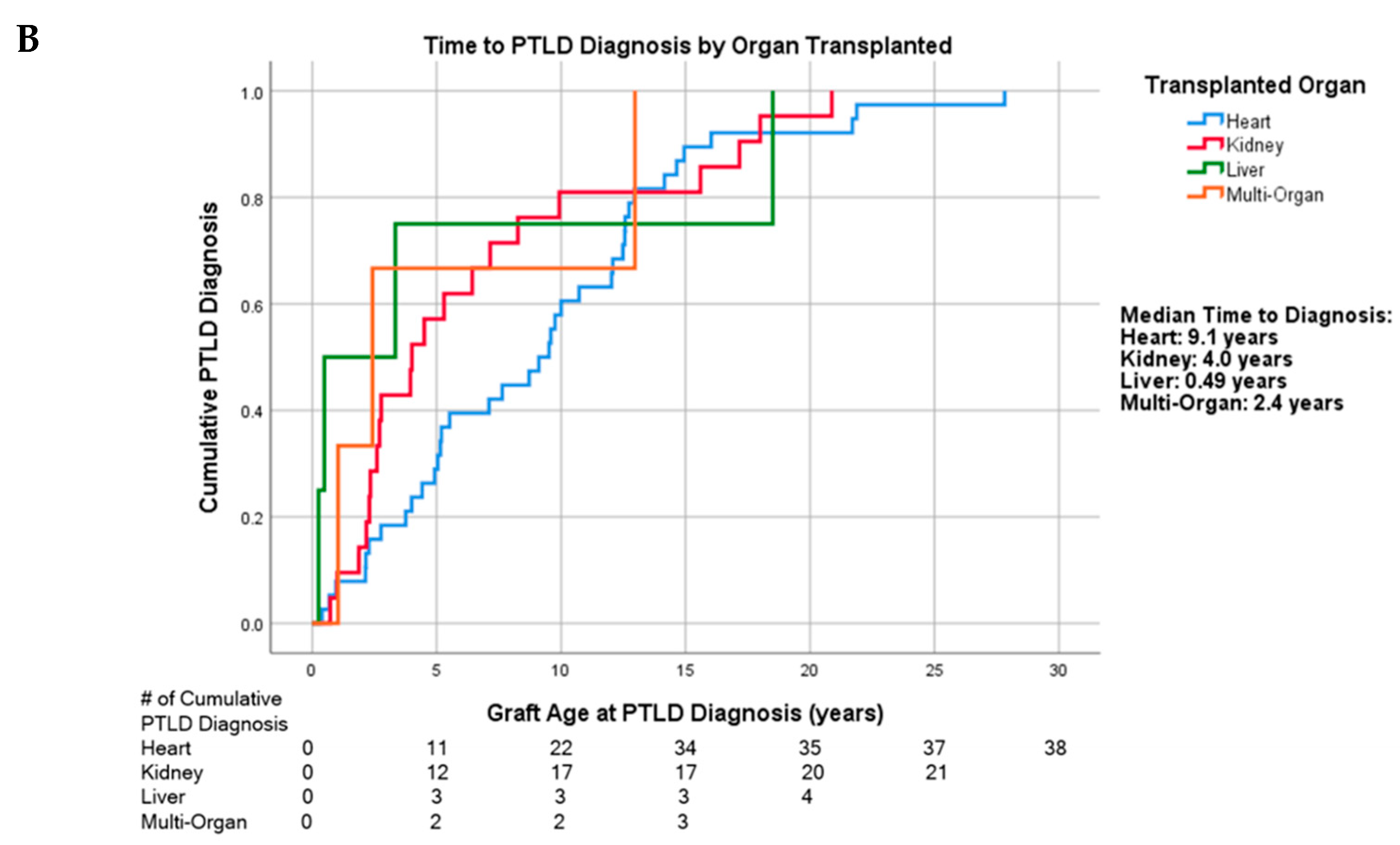
3.3. Time to PTLD Diagnosis by Age and Organ Transplanted
3.4. First-Line Treatment Regimen and Treatment Response
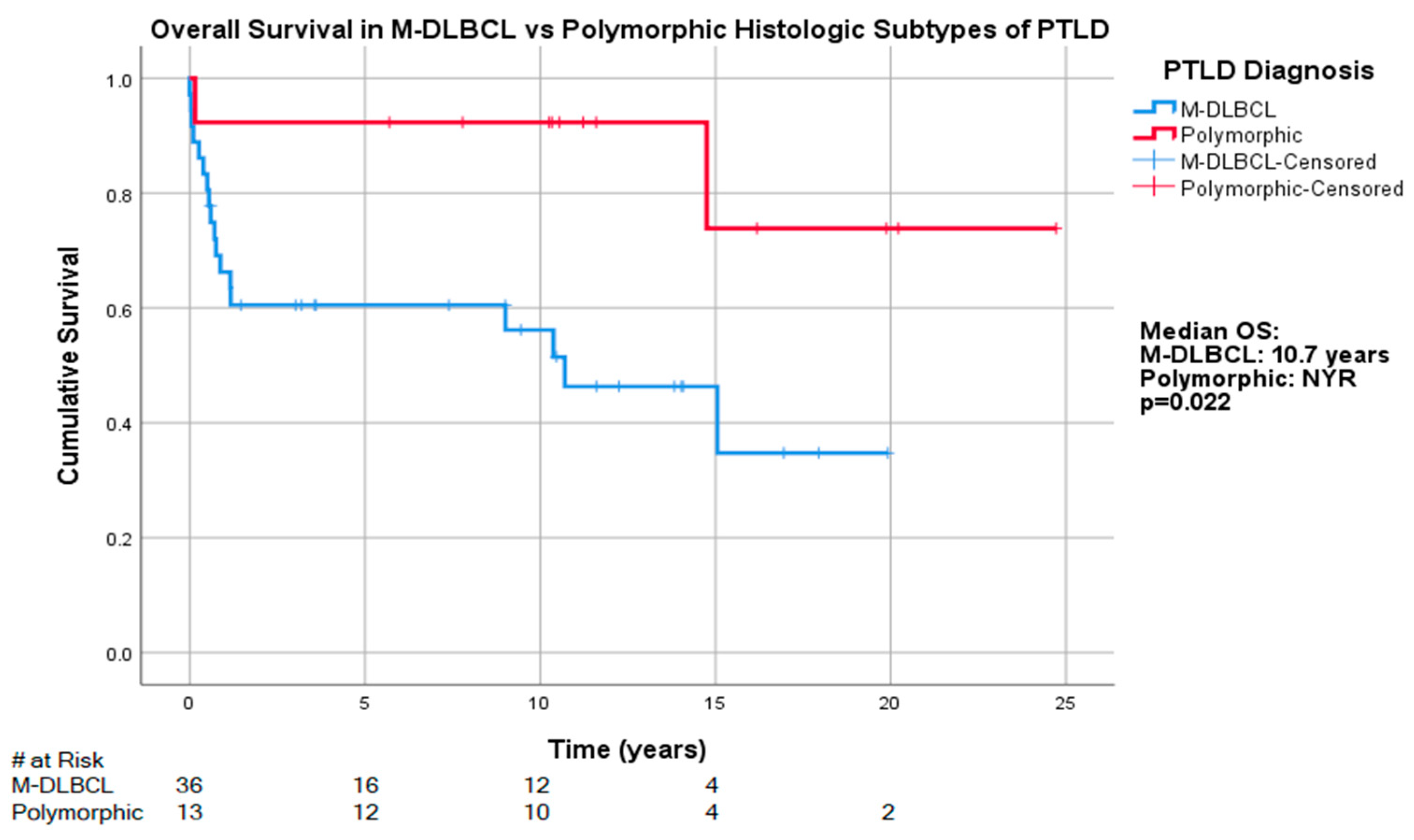
3.5. Overall Survival by Age at PTLD Diagnosis and R-IPI
3.6. Qualitative EBER and EBV DNA Status
3.7. Quantitative EBV Viral Load
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dierickx, D.; Habermann, T.M. Post-Transplantation Lymphoproliferative Disorders in Adults. N. Engl. J. Med. 2018, 378, 13. [Google Scholar] [CrossRef] [PubMed]
- OPTN/SRTR 2017 Annual Data Report: Introduction. Am. J. Transplant. 2019, 19, 7.
- Organ Donation again Sets Record in 2019. Available online: https://unos.org/news/organ-donation-sets-record-in-2019/ (accessed on 3 November 2020).
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J. Spectrum of cancer risk among US solid organ transplant recipients. JAMA 2011, 306, 10. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Webber, S.A.; Chadburm, A.; Ferry, J.A. Post-transplant lymphoproliferative disorders. In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed.; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Pileri, S.A., Stein, H., Thiele, J., Eds.; IARC Press: Lyon, France, 2017; pp. 453–462. [Google Scholar]
- Wang, J. Post-transplant lymphoproliferative disorders (Chapter 10). In Practical Lymph Node and Bone Marrow Pathology, 1st ed.; Wang, E., Lagoo, A.S., Eds.; Springer Nature: New York, NY, USA, 2020; pp. 209–224. [Google Scholar]
- Bishnoi, R.; Bajwa, R.; Franke, A.J. Post-transplant lymphoproliferative disorder (PTLD): Single institutional experience of 141 patients. Exp. Hematol. Oncol. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Dierickx, D.; Tousseyn, T.; Sagaert, X.; Fieuws, S.; Wlodarska, I.; Morscio, J.; Brepoels, L.; Kuypers, D.; Vanhaecke, J.; Nevens, F.; et al. Single-center analysis of biopsy-confirmed posttransplant lymphoproliferative disorder: Incidence, clinicopathological characteristics and prognostic factors. Leuk. Lymphoma 2013, 54, 2433–2440. [Google Scholar] [CrossRef]
- Caillard, S.; Porcher, R.; Provot, F.; Dantal, J.; Choquet, S.; Durrbach, A.; Morelon, E.; Moal, V.; Janbon, B.; Alamartine, E.; et al. Post-transplantation lymphoproliferative disorder after kidney transplantation: Report of a nationwide French registry and the development of a new prognostic score. J. Clin. Oncol. 2013, 31, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Evens, A.M.; David, K.A.; Helenowski, I. Multicenter analysis of 80 solid organ transplantation recipients with post-transplantation lymphoproliferative disease: Outcomes and prognostic factors in the modern era. J. Clin. Oncol. 2010, 28, 8. [Google Scholar] [CrossRef]
- Landgren, O.; Gilbert, E.S.; Rizzo, J.D.; Socié, G.; Banks, P.M.; Sobocinski, K.A.; Horowitz, M.M.; Jaffe, E.S.; Kingma, D.W.; Travis, L.B.; et al. Risk factors for lymphoproliferative disorders after allogeneic hematopoietic cell transplantation. Blood 2009, 113, 4992–5001. [Google Scholar] [CrossRef] [PubMed]
- Dierickx, D.; Tousseyn, T.; Gheysens, O. How I treat posttransplant lymphoproliferative disorders. Blood 2015, 126, 9. [Google Scholar] [CrossRef]
- Gross, T.G.; Orjuela, M.A.; Perkins, S.L.; Park, J.R.; Lynch, J.C.; Cairo, M.S.; Smith, L.M.; Hayashi, R.J. Low-dose chemotherapy and rituximab for posttransplant lymphoproliferative disease (PTLD): A Children’s Oncology Group Report. Am. J. Transplant. 2012, 12, 3069–3075. [Google Scholar] [CrossRef]
- Cockfield, S.M.; Preiksaitis, J.K.; Jewell, L.D.; Parfrey, N.A. Post-transplant lymphoproliferative disorder in renal allograft recipients. Clinical experience and risk factor analysis in a single center. Transplantation 1993, 56, 8. [Google Scholar] [CrossRef]
- Colvin, M.; Smith, J.M.; Hadley, N.; Skeans, M.A.; Uccellini, K.; Lehman, R. OPTN/SRTR 2017 Annual Data Report: Heart. Am. J. Transplant. 2019, 19, 80. [Google Scholar] [CrossRef]
- Reshef, R.; Vardhanabhuti, S.; Luskin, M.R. Reduction of immunosuppression as initial therapy for posttransplantation lymphoproliferative disorder. Am. J. Transplant. 2011, 11, 11. [Google Scholar] [CrossRef]
- Swinnen, L.J.; LeBlanc, M.; Grogan, T.M.; Gordon, L.I.; Stiff, P.J.; Miller, A.M.; Kasamon, Y.; Miller, T.P.; Fisher, R.I. Prospective study of sequential reduction in immunosuppression, interferon alpha-2B, and chemotherapy for posttransplantation lymphoproliferative disorder. Transplantation 2008, 86, 215–222. [Google Scholar] [CrossRef]
- Trappe, R.U.; Dierickx, D.; Zimmermann, H.; Morschhauser, F.; Mollee, P.; Zaucha, J.M. Response to Rituximab Induction Is a Predictive Marker in B-Cell Post-Transplant Lymphoproliferative Disorder and Allows Successful Stratification Into Rituximab or R-CHOP Consolidation in an International, Prospective, Multicenter Phase II Trial. J. Clin. Oncol. 2017, 35, 7. [Google Scholar] [CrossRef]
- Trappe, R.; Oertel, S.; Leblond, V.; Mollee, P.; Sender, M.; Reinke, P.; Neuhaus, R.; Lehmkuhl, H.; Horst, H.A.; Salles, G.; et al. Sequential treatment with rituximab followed by CHOP chemotherapy in adult B-cell post-transplant lymphoproliferative disorder (PTLD): The prospective international multicentre phase 2 PTLD-1 trial. Lancet Oncol. 2012, 13, 10. [Google Scholar] [CrossRef]
- Negrin, R.S. Treatment and prevention of post-transplant lymphoproliferative disorders. In Up To Date; Chao, N.J., Rosmarin, A.G., Eds.; UpToDate: Waltham, MA, USA, 2021. [Google Scholar]
- Singavi, A.K.; Harrington, A.M.; Fenske, T.S. Post-transplant lymphoproliferative disorders. Cancer Treat. Res. 2015, 165, 22. [Google Scholar]
- Swinnen, L.J.; Mullen, G.M.; Carr, T.J.; Costanzo, M.R.; Fisher, R.I. Aggressive treatment for postcardiac transplant lymphoproliferation. Blood 1995, 86, 7. [Google Scholar] [CrossRef]
- Luskin, M.R.; Heil, D.S.; Tan, K.S. The Impact of EBV Status on Characteristics and Outcomes of Posttransplantation Lymphoproliferative Disorder. Am. J. Transplant. 2015, 15, 8. [Google Scholar] [CrossRef]
- Kimura, H.; Kwong, Y.-L. EBV Viral Loads in Diagnosis, Monitoring, and Response Assessment. Front. Oncol. 2019, 9, 62. [Google Scholar] [CrossRef]
- Gulley ML, T.W. Using Epstein-Barr viral load assays to diagnose, monitor, and prevent posttransplant lymphoproliferative disorder. Clin. Microbiol. Rev. 2010, 23, 16. [Google Scholar] [CrossRef]
- Wagner, H.-J.; Wessel, M.; Jabs, W.; Smets, F.; Fischer, L.; Offner, G.; Bucsky, P. Patients at risk for development of posttransplant lymphoproliferative disorder: Plasma versus peripheral blood mononuclear cells as material for quantification of epstein-barr viral load by using real-time quantitative polymerase chain reaction1,2. Transplantation 2001, 72, 1012. [Google Scholar] [CrossRef] [PubMed]
- Kanakry, J.A.; Hegde, A.M.; Durand, C.M.; Massie, A.B.; Greer, A.E.; Ambinder, R.F.; Valsamakis, A. The clinical significance of EBV DNA in the plasma and peripheral blood mononuclear cells of patients with or without EBV diseases. Blood 2016, 127, 2007–2017. [Google Scholar] [CrossRef]
- Tsai, D.E.; Luskin, M.R.; Kremer, B.E.; Chung, A.K.; Arnoldi, S.; Paralkar, V.R.; Nasta, S.D.; Stadtmauer, E.A.; Schuster, S.J.; Xavier, M. A pilot trial of quantitative Epstein-Barr virus polymerase chain reaction in patients undergoing treatment for their malignancy: Potential use of Epstein-Barr virus polymerase chain reaction in multiple cancer types. Leuk. Lymphoma 2015, 56, 1530–1532. [Google Scholar] [CrossRef] [PubMed]
- Schober, T.; Framke, T.; Kreipe, H. Characteristics of early and late PTLD development in pediatric solid organ transplant recipients. Transplantation 2013, 95, 6. [Google Scholar] [CrossRef] [PubMed]
- Mynarek, M.; Schober, T.; Behrends, U.; Maecker-Kolhoff, B. Posttransplant lymphoproliferative disease after pediatric solid organ transplantation. Clin. Dev. Immunol. 2013. [Google Scholar] [CrossRef]
- Caillard, S.; Lamy, F.X.; Quelen, C. Epidemiology of posttransplant lymphoproliferative disorders in adult kidney and kidney pancreas recipients: Report of the French registry and analysis of subgroups of lymphomas. Am. J. Transplant. 2012, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Mucha, K.; Foroncewicz, B.; Ziarkiewicz-Wróblewska, B.; Krawczyk, M.; Lerut, J.; Paczek, L. Post-transplant lymphoproliferative disorder in view of the new WHO classification: A more rational approach to a protean disease? Nephrol. Dial. Transplant. 2010, 25, 9. [Google Scholar] [CrossRef]
- Chinnock, R.; Webber, S.A.; Dipchand, A.I.; Brown, R.N.; George, J.F. Pediatric Heart Transplant Study A 16-year multi-institutional study of the role of age and EBV status on PTLD incidence among pediatric heart transplant recipients. Am. J. Transplant. 2012, 12, 3061–3068. [Google Scholar] [CrossRef]
- Niewiesk, S. Maternal antibodies: Clinical significance, mechanism of interference with immune responses, and possible vaccination strategies. Front. Immunol. 2014, 5, 446. [Google Scholar] [CrossRef]
- Chinnock, R.E.; Bailey, L.L. Heart transplantation for congenital heart disease in the first year of life. Curr. Cardiol. Rev. 2011, 7, 72–84. [Google Scholar] [CrossRef]
- Bailey, L.L. Origins of neonatal heart transplantation: An historical perspective. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2011, 14, 98–100. [Google Scholar] [CrossRef]
- Pitman, S.D.; Huang, Q.; Zuppan, C.W.; Rowsell, E.H.; Cao, J.D.; Berdeja, J.G.; Weiss, L.M.; Wang, J. Hodgkin lymphoma-like posttransplant lymphoproliferative disorder (HL-like PTLD) simulates monomorphic B-cell PTLD both clinically and pathologically. Am. J. Surg. Pathol. 2006, 30, 470–476. [Google Scholar] [CrossRef]
- John, M.; Bailey, L.L. Neonatal heart transplantation. Ann. Cardiothorac. Surg. 2018, 7, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Balfour, H.H., Jr.; Sifakis, F.; Sliman, J.A.; Knight, J.A.; Schmeling, D.O.; Thomas, W. Age-specific prevalence of Epstein-Barr virus infection among individuals aged 6-19 years in the United States and factors affecting its acquisition. J. Infect. Dis. 2013, 208, 1286–1293. [Google Scholar] [CrossRef]
- Opelz, G.; Döhler, B. Lymphomas after solid organ transplantation: A collborative transplant study report. Am. J. Transplant. 2004, 4, 8. [Google Scholar] [CrossRef] [PubMed]
- Tsai, D.E.; Hardy, C.L.; Tomaszewski, J.E. Reduction in immunosuppression as initial therapy for posttransplant lymphoproliferative disorder: Analysis of prognostic variables and long-term follow-up of 42 adult patients. Transplantation 2001, 71, 12. [Google Scholar] [CrossRef]
- Webber, S.A.; Naftel, D.C.; Fricker, F.J.; Olesnevich, P.; Blume, E.D.; Addonizio, L.; Kirklin, J.K.; Canter, C.E. Pediatric Heart Transplant Study Lymphoproliferative disorders after paediatric heart transplantation: A multi-institutional study. Lancet 2006, 367, 233–239. [Google Scholar] [CrossRef]
- NCCN B-Cell Lymphoma. Available online: https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf (accessed on 2 February 2021).
- Trappe, R.U.; Choquet, S.; Dierickx, D.; Mollee, P.; Zaucha, J.M.; Dreyling, M.H.; Dührsen, U.; Tarella, C.; Shpilberg, O.; Sender, M.; et al. International prognostic index, type of transplant and response to rituximab are key parameters to tailor treatment in adults with CD20-positive B cell PTLD: Clues from the PTLD-1 trial. Am. J. Transplant. 2015, 15, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Ferla, V.; Rossi, F.G.; Goldaniga, M.C.; Baldini, L. Biological Difference between Epstein-Barr Virus Positive and Negative Post-transplant Lymphoproliferative Disorders and Their Clinical Impact. Front. Oncol. 2020, 10, 506. [Google Scholar] [CrossRef] [PubMed]
- Tsai, D.E.; Nearey, M.; Hardy, C.L. Use of EBV PCR for the diagnosis and monitoring of post-transplant lymphoproliferative disorder in adult solid organ transplant patients. Am. J. Transplant. 2002, 2, 8. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Sub-Types | Sample Size (n) | Percentage (%) |
|---|---|---|---|
| Total | - | 66 | 100 |
| Sex | Male | 41 | 62.1 |
| Female | 25 | 37.9 | |
| Race | White | 34 | 51.5 |
| Black or African American | 4 | 6.1 | |
| Hispanic | 23 | 34.8 | |
| Asian | 4 | 6.1 | |
| Other | 1 | 1.5 | |
| Transplant Age | Infant (<1 year old) | 23 | 34.8 |
| Pediatric/Adolescent (1–18 years old) | 22 | 33.3 | |
| Adult (At least 18 years old) | 21 | 31.8 | |
| Transplanted Organ | Heart | 38 | 57.6 |
| Kidney | 21 | 31.8 | |
| Liver | 4 | 6.1 | |
| Multi-Organ | 3 | 4.5 | |
| Time to PTLD Diagnosis | Early | 6 | 9.1 |
| Late | 38 | 57.6 | |
| Very Late | 22 | 33.3 | |
| ECOG Status | 0–2 | 50 | 75.8 |
| 3–4 | 16 | 24.2 | |
| CD20 Status | Positive | 51 | 77.3 |
| Negative | 10 | 15.1 | |
| Unknown | 5 | 7.6 | |
| Tumor EBER Status | Positive | 49 | 74.2 |
| Negative | 14 | 21.2 | |
| Unknown | 3 | 4.5 | |
| R-IPI Score | Low (0–2) | 45 | 68.2 |
| High (3–4) | 19 | 28.8 | |
| Unknown | 2 | 3.0 |
| Category | All-Comers | ND-PTLD | P-PTLD | M-BL-PTLD | M-DLBCL-PTLD | M-PCN-PTLD | M-T/NK-PTLD | HL-PTLD |
|---|---|---|---|---|---|---|---|---|
| All | 66 | 4 | 13 | 4 | 36 | 3 | 3 | 3 |
| Transplant Age | ||||||||
| Infant | 23 | 2 | 9 | 0 | 7 | 2 | 2 | 1 |
| Pediatric/Adolescent | 22 | 2 | 3 | 4 | 11 | 0 | 1 | 1 |
| Adult | 21 | 0 | 1 | 0 | 18 | 1 | 0 | 1 |
| Transplanted Organ | ||||||||
| Heart | 38 | 3 | 8 | 1 | 19 | 2 | 3 | 2 |
| Kidney | 21 | 1 | 3 | 3 | 13 | 0 | 0 | 1 |
| Liver | 4 | 0 | 1 | 0 | 3 | 0 | 0 | 0 |
| Multi-Organ | 3 | 0 | 1 | 0 | 1 | 1 | 0 | 0 |
| Time to PTLD Diagnosis | ||||||||
| Early | 6 | 0 | 1 | 0 | 4 | 1 | 0 | 0 |
| Late | 38 | 3 | 6 | 4 | 23 | 0 | 0 | 2 |
| Very Late | 22 | 1 | 6 | 0 | 9 | 2 | 3 | 1 |
| First-Line Treatment | ||||||||
| Observation and RIS ± AV | 18 | 2 | 5 | 1 | 5 | 1 | 2 | 2 |
| Rituximab | 10 | 2 | 2 | 0 | 5 | 1 | 0 | 0 |
| R + CTX | 30 | 0 | 4 | 2 | 24 | 0 | 0 | 0 |
| CTX | 8 | 0 | 2 | 1 | 2 | 1 | 1 | 1 |
| ECOG Status | ||||||||
| 0–2 | 50 | 4 | 9 | 4 | 27 | 3 | 1 | 2 |
| 3–4 | 16 | 0 | 4 | 0 | 9 | 0 | 2 | 1 |
| Tumor EBER Status | ||||||||
| Positive | 49 | 4 | 12 | 3 | 24 | 1 | 3 | 2 |
| Negative | 14 | 0 | 0 | 1 | 11 | 2 | 0 | 0 |
| Unknown | 3 | 0 | 1 | 0 | 1 | 0 | 0 | 1 |
| EBV PCR Status | ||||||||
| Positive | 50 | 3 | 11 | 3 | 27 | 1 | 3 | 2 |
| Negative | 6 | 0 | 1 | 0 | 4 | 1 | 0 | 0 |
| Unknown | 10 | 1 | 1 | 1 | 5 | 1 | 0 | 1 |
| CD20 Status | ||||||||
| Positive | 51 | 4 | 10 | 4 | 32 | 0 | 0 | 1 |
| Negative | 10 | 0 | 1 | 0 | 2 | 3 | 3 | 1 |
| Unknown | 5 | 0 | 2 | 0 | 2 | 0 | 0 | 1 |
| R-IPI Score | ||||||||
| Low (0–2) | 45 | 4 | 12 | 3 | 22 | 1 | 2 | 1 |
| High (3–4) | 19 | 0 | 1 | 1 | 13 | 1 | 1 | 2 |
| Unknown | 2 | 0 | 0 | 0 | 1 | 1 | 0 | 0 |
| First-Line Therapy for M-DLBCL-PTLD | N | Progressive Disease | Partial Response | Complete Response |
| Observation or RIS ± AV | 5 | 5 | 0 | 0 |
| Rituximab | 5 | 1 | 1 | 3 |
| R + CTX | 24 | 3 | 1 | 20 |
| CTX | 2 | 1 | 0 | 1 |
| Total | 36 | 10 | 2 | 24 |
| First-Line Therapy for P-PTLD | N | Progressive Disease | Partial Response | Complete Response |
| RIS ± AV | 5 | 0 | 0 | 5 |
| Rituximab | 2 | 0 | 0 | 2 |
| R + CTX | 4 | 1 | 0 | 3 |
| CTX | 2 | 0 | 0 | 2 |
| Total | 13 | 1 | 0 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, E.; Moyers, J.T.; Wang, B.C.; Jeong, I.S.D.; Lee, J.; Liu, L.; Kim, M.; Villicana, R.; Kim, B.; Mitchell, J.; et al. Analysis of Post-Transplant Lymphoproliferative Disorder (PTLD) Outcomes with Epstein–Barr Virus (EBV) Assessments—A Single Tertiary Referral Center Experience and Review of Literature. Cancers 2021, 13, 899. https://doi.org/10.3390/cancers13040899
Lau E, Moyers JT, Wang BC, Jeong ISD, Lee J, Liu L, Kim M, Villicana R, Kim B, Mitchell J, et al. Analysis of Post-Transplant Lymphoproliferative Disorder (PTLD) Outcomes with Epstein–Barr Virus (EBV) Assessments—A Single Tertiary Referral Center Experience and Review of Literature. Cancers. 2021; 13(4):899. https://doi.org/10.3390/cancers13040899
Chicago/Turabian StyleLau, Eric, Justin Tyler Moyers, Billy Chen Wang, Il Seok Daniel Jeong, Joanne Lee, Lawrence Liu, Matthew Kim, Rafael Villicana, Bobae Kim, Jasmine Mitchell, and et al. 2021. "Analysis of Post-Transplant Lymphoproliferative Disorder (PTLD) Outcomes with Epstein–Barr Virus (EBV) Assessments—A Single Tertiary Referral Center Experience and Review of Literature" Cancers 13, no. 4: 899. https://doi.org/10.3390/cancers13040899
APA StyleLau, E., Moyers, J. T., Wang, B. C., Jeong, I. S. D., Lee, J., Liu, L., Kim, M., Villicana, R., Kim, B., Mitchell, J., Kamal, M. O., Chen, C.-S., Liu, Y., Wang, J., Chinnock, R., & Cao, H. (2021). Analysis of Post-Transplant Lymphoproliferative Disorder (PTLD) Outcomes with Epstein–Barr Virus (EBV) Assessments—A Single Tertiary Referral Center Experience and Review of Literature. Cancers, 13(4), 899. https://doi.org/10.3390/cancers13040899