
Robotic Radiosurgery for Persistent Postoperative Acromegaly in Patients with Cavernous Sinus-Invading Pituitary Adenomas—A Multicenter Experience

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics and Treatment Parameters
2.2. Endocrinological Baseline
2.3. Treatment Outcome
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Endocrinological Analysis
4.3. Treatment Procedure and Outcome
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lavrentaki, A.; Paluzzi, A.; Wass, J.A.; Karavitaki, N. Epidemiology of acromegaly: Review of population studies. Pituitary 2017, 20, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Molitch, M.E. Diagnosis and Treatment of Pituitary Adenomas: A Review. Jama 2017, 317, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Nomikos, P.; Buchfelder, M.; Fahlbusch, R. The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur. J. Endocrinol. 2005, 152, 379–387. [Google Scholar] [CrossRef]
- Meij, B.P.; Lopes, M.B.; Ellegala, D.B.; Alden, T.D.; Laws, E.R., Jr. The long-term significance of microscopic dural invasion in 354 patients with pituitary adenomas treated with transsphenoidal surgery. J. Neurosurg. 2002, 96, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Mehta, G.U.; Lonser, R.R. Management of hormone-secreting pituitary adenomas. Neuro-oncology 2017, 19, 762–773. [Google Scholar] [CrossRef]
- Starke, R.M.; Raper, D.M.; Payne, S.C.; Vance, M.L.; Oldfield, E.H.; Jane, J.A., Jr. Endoscopic vs microsurgical transsphenoidal surgery for acromegaly: Outcomes in a concurrent series of patients using modern criteria for remission. J. Clin. Endocrinol Metab 2013, 98, 3190–3198. [Google Scholar] [CrossRef]
- Juraschka, K.; Khan, O.H.; Godoy, B.L.; Monsalves, E.; Kilian, A.; Krischek, B.; Ghare, A.; Vescan, A.; Gentili, F.; Zadeh, G. Endoscopic endonasal transsphenoidal approach to large and giant pituitary adenomas: Institutional experience and predictors of extent of resection. J. Neurosurg. 2014, 121, 75–83. [Google Scholar] [CrossRef]
- Ding, D.; Starke, R.M.; Sheehan, J.P. Treatment paradigms for pituitary adenomas: Defining the roles of radiosurgery and radiation therapy. J. Neurooncol. 2014, 117, 445–457. [Google Scholar] [CrossRef]
- Tritos, N.A.; Biller, B.M.K. Pegvisomant: A growth hormone receptor antagonist used in the treatment of acromegaly. Pituitary 2017, 20, 129–135. [Google Scholar] [CrossRef]
- Ding, D.; Mehta, G.U.; Patibandla, M.R.; Lee, C.C.; Liscak, R.; Kano, H.; Pai, F.Y.; Kosak, M.; Sisterson, N.D.; Martinez-Alvarez, R.; et al. Stereotactic Radiosurgery for Acromegaly: An International Multicenter Retrospective Cohort Study. Neurosurgery 2019, 84, 717–725. [Google Scholar] [CrossRef]
- Graffeo, C.S.; Donegan, D.; Erickson, D.; Brown, P.D.; Perry, A.; Link, M.J.; Young, W.F.; Pollock, B.E. The Impact of Insulin-Like Growth Factor Index and Biologically Effective Dose on Outcomes After Stereotactic Radiosurgery for Acromegaly: Cohort Study. Neurosurgery 2020. [Google Scholar] [CrossRef] [PubMed]
- Iwata, H.; Sato, K.; Nomura, R.; Tabei, Y.; Suzuki, I.; Yokota, N.; Inoue, M.; Ohta, S.; Yamada, S.; Shibamoto, Y. Long-term results of hypofractionated stereotactic radiotherapy with CyberKnife for growth hormone-secreting pituitary adenoma: Evaluation by the Cortina consensus. J. Neurooncol. 2016, 128, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Sala, E.; Moore, J.M.; Amorin, A.; Martinez, H., Jr.; Bhowmik, A.C.; Lamsam, L.; Chang, S.; Soltys, S.G.; Katznelson, L.; Harsh, G.R. CyberKnife robotic radiosurgery in the multimodal management of acromegaly patients with invasive macroadenoma: A single center’s experience. J. Neurooncol. 2018, 138, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Rhome, R.; Germano, I.M.; Sheu, R.D.; Green, S. Long-term outcomes of acromegaly treated with fractionated stereotactic radiation: Case series and literature review. Neurooncol. Pract. 2017, 4, 255–262. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kim, E.H.; Oh, M.C.; Chang, J.H.; Moon, J.H.; Ku, C.R.; Chang, W.S.; Lee, E.J.; Kim, S.H. Postoperative gamma knife radiosurgery for cavernous sinus-invading growth hormone-secreting pituitary adenomas. World Neurosurg. 2018, 110, 534–545. [Google Scholar] [CrossRef]
- Roberts, B.K.; Ouyang, D.L.; Lad, S.P.; Chang, S.D.; Harsh, G.R.t.; Adler, J.R., Jr.; Soltys, S.G.; Gibbs, I.C.; Remedios, L.; Katznelson, L. Efficacy and safety of CyberKnife radiosurgery for acromegaly. Pituitary 2007, 10, 19–25. [Google Scholar] [CrossRef]
- Cho, C.B.; Park, H.K.; Joo, W.I.; Chough, C.K.; Lee, K.J.; Rha, H.K. Stereotactic Radiosurgery with the CyberKnife for Pituitary Adenomas. J. Korean Neurosurg. Soc. 2009, 45, 157–163. [Google Scholar] [CrossRef]
- Leach, P.; Abou-Zeid, A.H.; Kearney, T.; Davis, J.; Trainer, P.J.; Gnanalingham, K.K. Endoscopic transsphenoidal pituitary surgery: Evidence of an operative learning curve. Neurosurgery 2010, 67, 1205–1212. [Google Scholar] [CrossRef]
- Dusek, T.; Kastelan, D.; Melada, A.; Baretic, M.; Skoric Polovina, T.; Perkovic, Z.; Giljevic, Z.; Jelcic, J.; Paladino, J.; Aganovic, I.; et al. Clinical features and therapeutic outcomes of patients with acromegaly: Single-center experience. J. Endocrinol. Investig. 2011, 34, e382–e385. [Google Scholar] [CrossRef]
- Rieger, A.; Rainov, N.G.; Ebel, H.; Sanchin, L.; Shibib, K.; Helfrich, C.; Hoffmann, O.; Burkert, W. Factors predicting pituitary adenoma invasiveness in acromegalic patients. Neurosurg. Rev. 1997, 20, 182–187. [Google Scholar] [CrossRef]
- Wang, M.; Mou, C.; Jiang, M.; Han, L.; Fan, S.; Huan, C.; Qu, X.; Han, T.; Qu, Y.; Xu, G. The characteristics of acromegalic patients with hyperprolactinemia and the differences in patients with merely GH-secreting adenomas: Clinical analysis of 279 cases. Eur. J. Endocrinol. 2012, 166, 797–802. [Google Scholar] [CrossRef]
- Landolt, A.M.; Haller, D.; Lomax, N.; Scheib, S.; Schubiger, O.; Siegfried, J.; Wellis, G. Stereotactic radiosurgery for recurrent surgically treated acromegaly: Comparison with fractionated radiotherapy. J. Neurosurg. 1998, 88, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Landolt, A.M.; Haller, D.; Lomax, N.; Scheib, S.; Schubiger, O.; Siegfried, J.; Wellis, G. Octreotide may act as a radioprotective agent in acromegaly. J. Clin. Endocrinol Metab 2000, 85, 1287–1289. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, J.P.; Pouratian, N.; Steiner, L.; Laws, E.R.; Vance, M.L. Gamma Knife surgery for pituitary adenomas: Factors related to radiological and endocrine outcomes. J. Neurosurg 2011, 114, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Pollock, B.E.; Jacob, J.T.; Brown, P.D.; Nippoldt, T.B. Radiosurgery of growth hormone-producing pituitary adenomas: Factors associated with biochemical remission. J. Neurosurg. 2007, 106, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Katznelson, L.; Laws, E.R., Jr.; Melmed, S.; Molitch, M.E.; Murad, M.H.; Utz, A.; Wass, J.A.H. Acromegaly: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2014, 99, 3933–3951. [Google Scholar] [CrossRef] [PubMed]
- Holdaway, I.M.; Bolland, M.J.; Gamble, G.D. A meta-analysis of the effect of lowering serum levels of GH and IGF-I on mortality in acromegaly. Eur. J. Endocrinol. 2008, 159, 89–95. [Google Scholar] [CrossRef]
- Gutt, B.; Wowra, B.; Alexandrov, R.; Uhl, E.; Schaaf, L.; Stalla, G.K.; Schopohl, J. Gamma-knife surgery is effective in normalising plasma insulin-like growth factor I in patients with acromegaly. Exp. Clin. Endocrinol. Diabetes 2005, 113, 219–224. [Google Scholar] [CrossRef]
- Kong, D.S.; Kim, Y.H.; Kim, Y.H.; Hur, K.Y.; Kim, J.H.; Kim, M.S.; Paek, S.H.; Kwon, D.H.; Kim, D.K.; Lee, J.I. Long-Term Efficacy and Tolerability of Gamma Knife Radiosurgery for Growth Hormone-Secreting Adenoma: A Retrospective Multicenter Study (MERGE-001). World Neurosurg 2019, 122, e1291–e1299. [Google Scholar] [CrossRef]
- Liu, X.; Kano, H.; Kondziolka, D.; Park, K.J.; Iyer, A.; Niranjan, A.; Flickinger, J.C.; Lunsford, L.D. Gamma knife radiosurgery for clinically persistent acromegaly. J. Neurooncol. 2012, 109, 71–79. [Google Scholar] [CrossRef]
- Losa, M.; Gioia, L.; Picozzi, P.; Franzin, A.; Valle, M.; Giovanelli, M.; Mortini, P. The role of stereotactic radiotherapy in patients with growth hormone-secreting pituitary adenoma. J. Clin. Endocrinol. Metab. 2008, 93, 2546–2552. [Google Scholar] [CrossRef]
- Melmed, S.; Bronstein, M.D.; Chanson, P.; Klibanski, A.; Casanueva, F.F.; Wass, J.A.H.; Strasburger, C.J.; Luger, A.; Clemmons, D.R.; Giustina, A. A Consensus Statement on acromegaly therapeutic outcomes. Nat. Rev. Endocrinol. 2018, 14, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.; Yuen, K.; Biller, B.; Kemp, S.; Vance, M. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for Growth Hormone Use in Growth Hormone-Deficient Adults and Transition Patients-2009 Update: Executive Summary of Recommendations. Endocr. Pract. 2009, 15, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Subbarayan, S.K.; Fleseriu, M.; Gordon, M.B.; Brzana, J.A.; Kennedy, L.; Faiman, C.; Hatipoglu, B.A.; Prayson, R.A.; Delashaw, J.B.; Weil, R.J.; et al. Serum IGF-1 in the diagnosis of acromegaly and the profile of patients with elevated IGF-1 but normal glucose-suppressed growth hormone. Endocr. Pract. 2012, 18, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Brabant, G. Insulin-like growth factor-I: Marker for diagnosis of acromegaly and monitoring the efficacy of treatment. Eur. J. Endocrinol. 2003, 148, S15–S20. [Google Scholar] [CrossRef][Green Version]
- ElmLinger, M.W.; Kuhnel, W.; Weber, M.M.; Ranke, M.B. Reference ranges for two automated chemiluminescent assays for serum insulin-like growth factor I (IGF-I) and IGF-binding protein 3 (IGFBP-3). Clin. Chem. Lab. Med. 2004, 42, 654–664. [Google Scholar] [CrossRef]
- Fowler, J.F. The linear-quadratic formula and progress in fractionated radiotherapy. Br. J. Radiol. 1989, 62, 679–694. [Google Scholar] [CrossRef]
- Fowler, J.F. 21 years of biologically effective dose. Br. J. Radiol. 2010, 83, 554–568. [Google Scholar] [CrossRef]


{kind=link}
| Total Number of Patients | 50 | ||
|---|---|---|---|
| Sex (Male/Female, %) | 28 (56) | 22 (44) | |
| Mean (±SD) | Median | Range | |
| Age (years) | 46.7 (10.3) | 47.6 | 26.8–70.7 |
| Pretreatment Karnofsky Performance Status (%) | 93.3 (8.5) | 90 | 60–100 |
| Follow-up (months) | 57.3 (42.4) | 57.7 | 6.1–171.9 |
| IGF-1 level before RRS (ng/mL) | 439 (238) | 381 | 98–1161 |
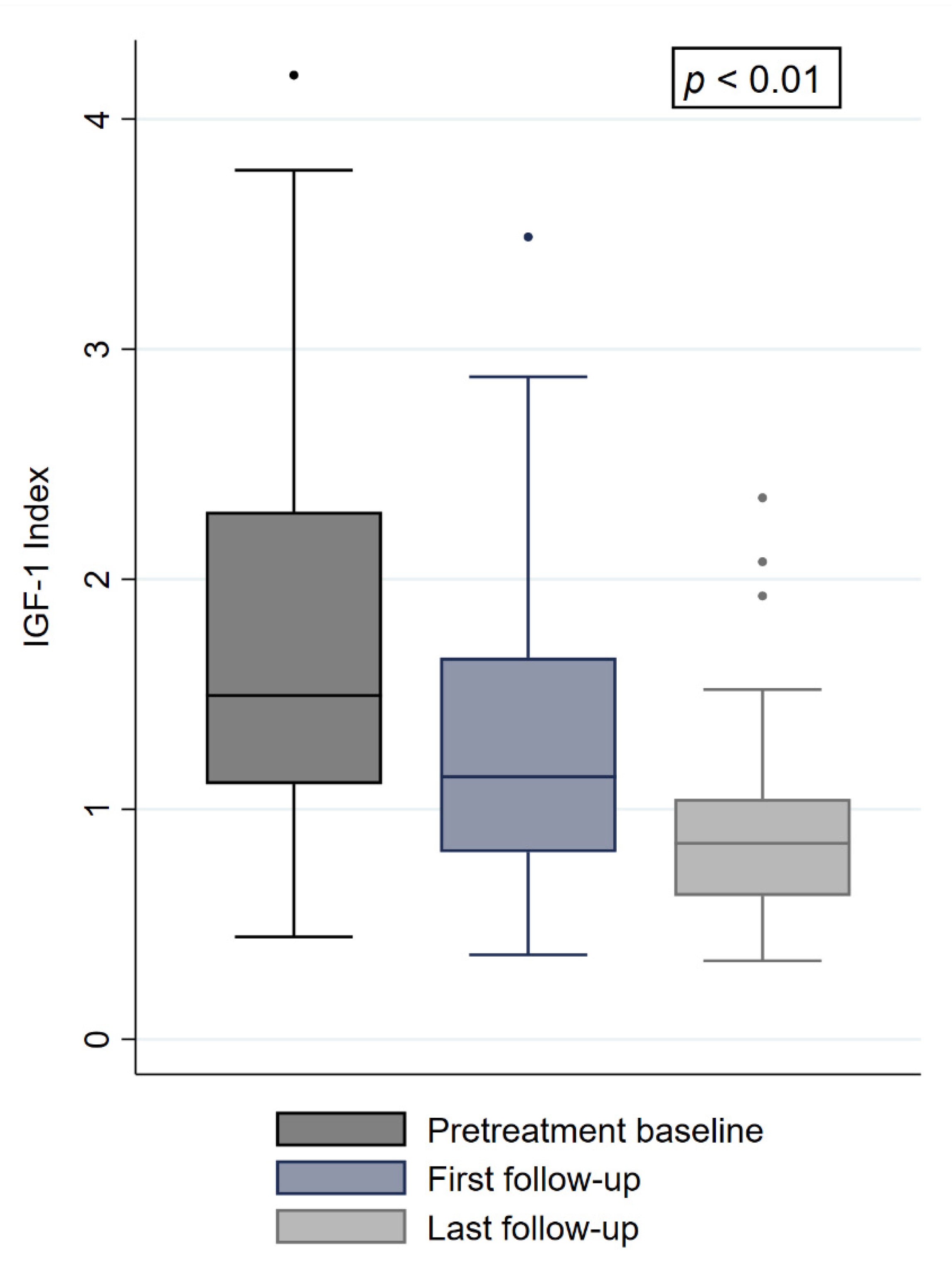
| IGF-1i before RRS | 1.73 (0.90) | 1.49 | 0.44–4.19 |
| IGF-1 level at 6-month follow-up (ng/mL) | 322 (166) | 277 | 109–858 |
| IGF-1i at 6-month follow-up | 1.27 (0.64) | 1.14 | 0.36–3.48 |
| IGF-1 level at last follow-up (ng/mL) | 226 (99) | 196 | 89–575 |
| IGF-1i at last follow-up | 0.89 (0.40) | 0.83 | 0.34–2.35 |
| Patients with an IGF-1i larger 2.25 before RRS (%) | 13 (26) | ||
| Patients with medication before RRS (%) | 46 (92) | ||
| Patients with medication during RRS (%) | 46 (92) | ||
| Patients with medication at last follow-up (%) | 38 (76) | ||
| Pretreatment visual changes (%) | 6 (12) | ||
| Post-treatment visual changes (%) | 4 (8) | ||
| Pretreatment hypopituitarism (%) | 16 (32) | ||
| Post-treatment hypopituitarism (%) | 19 (38) | ||
| Patients with biochemically controlled disease before RRS | 9 (18) | ||
| Patients with biochemically controlled disease at last follow-up (%) | 24 (48) | ||
| Patients with biochemical remission at last follow-up (%) | 9 (18) | ||
| Variable | Median | Mean | Range |
|---|---|---|---|
| Irradiated/tumor volume (cc) | 1.38 | 2.07 | 0.13–12.00 |
| Prescription dose (Gy) | 18 | 18.4 | 14–24 |
| Prescription isodose (%) | 70 | 69.7 | 52–80 |
| Max tumor dose (Gy) | 25.7 | 26.8 | 21.4–43.6 |
| Min tumor dose (Gy) | 15.3 | 15.3 | 7.0–24.1 |
| Mean tumor dose (Gy) | 21.6 | 22.1 | 17.1–31.2 |
| Conformity index | 1.3 | 1.3 | 1.0–2.2 |
| Homogeneity index | 1.4 | 1.4 | 1.2–1.9 |
| Coverage (%) | 98.4 | 96.2 | 83.0–100.0 |
| Max optic nerve dose (Gy) | 5.8 | 6.0 | 1.1–15.5 |
| Max chiasm dose (Gy) | 5.7 | 5.7 | 1.1–15.5 |
| Max brainstem dose (Gy) | 5.1 | 5.7 | 0.0–17.6 |
| BED (Gy) | 99.0 | 104.5 | 63.0–168.0 |
| EQD2 (Gy) | 66.0 | 69.6 | 42.0–112.0 |
| Variable | Biochemical Remission (±SD) | Without Biochemical Remission (±SD) | p-Value |
|---|---|---|---|
| Age | 47.6 (12.5) | 46.5 (9.9) | 0.77 |
| IGF-1 levels before treatment (ng/mL) | 290.2 (138.3) | 472.6 (243.8) | 0.03 |
| IGF-1i before treatment | 1.11 (0.4) | 1.86 (0.9) | 0.02 |
| Irradiated/tumor volume (cc) | 1.2 (0.6) | 2.2 (2.5) | 0.24 |
| Prescription dose (Gy) | 18.7 (3.1) | 18.3 (1.5) | 0.58 |
| Prescription isodose (%) | 70.5 (7.6) | 69.5 (6.8) | 0.70 |
| Max dose in tumor (Gy) | 26.9 (6.9) | 26.8 (4.0) | 0.95 |
| Min dose in tumor (Gy) | 14.8 (4.6) | 15.4 (3.5) | 0.65 |
| Mean dose in tumor (Gy) | 22.3 (4.3) | 22.0 (2.6) | 0.90 |
| Coverage (%) | 94.7 (5.5) | 96.5 (4.1) | 0.26 |
| BED (Gy) | 109.0 (33.5) | 103.5 (16.7) | 0.46 |
| Biochemical Remission (Univariable Analysis) | |||
|---|---|---|---|
| Factor | Odds Ratio | p-Value | 95% Confidence Interval |
| Age | 1.01 | 0.76 | 0.94–1.08 |
| Sex | 0.16 | 0.03 | 0.03–0.89 |
| Irradiated/tumor volume (cc) | 0.64 | 0.26 | 0.29–1.39 |
| Dose (Gy) | 1.10 | 0.57 | 0.76–1.59 |
| Max dose in tumor (Gy) | 1.00 | 0.95 | 0.86–1.17 |
| Mean dose in tumor (Gy) | 1.03 | 0.75 | 0.81–1.31 |
| Min dose in tumor (Gy) | 0.95 | 0.64 | 0.78–1.16 |
| BED (Gy) | 1.01 | 0.46 | 0.97–1.04 |
| Pretreatment IGF Index | 0.15 | 0.03 | 0.02–0.91 |
| Pretreatment IGF level (ng/mL) | 0.99 | 0.05 | 0.98–1.00 |
| IGF-1i at 1. follow-up | 0.17 | 0.06 | 0.02–1.10 |
| IGF-1 level at 1. follow-up (ng/mL) | 0.99 | 0.08 | 0.98–1.00 |
| Complete tumor regression | 2.91 | 0.19 | 0.56–14.94 |
| Biochemical Remission (Multivariable Analysis) | |||
| Age | 0.84 | 0.13 | 0.67–1.05 |
| Sex | 0.01 | 0.05 | 0.01–1.23 |
| Irradiated/tumor volume (cc) | 0.07 | 0.11 | 0.01–1.91 |
| Dose (Gy) | 2.35 | 0.45 | 0.25–21.80 |
| Max dose in tumor (Gy) | 1.11 | 0.75 | 0.25–2.06 |
| Mean dose in tumor (Gy) | (co-linear with dose) | ||
| Min dose in tumor (Gy) | 0.64 | 0.22 | 0.32–1.30 |
| BED (Gy) | (co-linear with dose) | ||
| Pretreatment IGF-1i | 0.04 | 0.04 | 0.01–0.93 |
| Pretreatment IGF-1 level (ng/mL) | (co-linear with pretreatment IGF Index) | ||
| IGF-1i at 1. follow-up | (co-linear with pretreatment IGF Index) | ||
| IGF-1 level at 1. follow-up (ng/mL) | (co-linear with pretreatment IGF Index) | ||
| Complete tumor regression | 8.06 | 0.27 | 0.19–39.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ehret, F.; Kufeld, M.; Fürweger, C.; Haidenberger, A.; Windisch, P.; Fichte, S.; Lehrke, R.; Senger, C.; Kaul, D.; Rueß, D.; et al. Robotic Radiosurgery for Persistent Postoperative Acromegaly in Patients with Cavernous Sinus-Invading Pituitary Adenomas—A Multicenter Experience. Cancers 2021, 13, 537. https://doi.org/10.3390/cancers13030537
Ehret F, Kufeld M, Fürweger C, Haidenberger A, Windisch P, Fichte S, Lehrke R, Senger C, Kaul D, Rueß D, et al. Robotic Radiosurgery for Persistent Postoperative Acromegaly in Patients with Cavernous Sinus-Invading Pituitary Adenomas—A Multicenter Experience. Cancers. 2021; 13(3):537. https://doi.org/10.3390/cancers13030537
Chicago/Turabian StyleEhret, Felix, Markus Kufeld, Christoph Fürweger, Alfred Haidenberger, Paul Windisch, Susanne Fichte, Ralph Lehrke, Carolin Senger, David Kaul, Daniel Rueß, and et al. 2021. "Robotic Radiosurgery for Persistent Postoperative Acromegaly in Patients with Cavernous Sinus-Invading Pituitary Adenomas—A Multicenter Experience" Cancers 13, no. 3: 537. https://doi.org/10.3390/cancers13030537
APA StyleEhret, F., Kufeld, M., Fürweger, C., Haidenberger, A., Windisch, P., Fichte, S., Lehrke, R., Senger, C., Kaul, D., Rueß, D., Ruge, M., Schichor, C., Tonn, J.-C., Stalla, G., & Muacevic, A. (2021). Robotic Radiosurgery for Persistent Postoperative Acromegaly in Patients with Cavernous Sinus-Invading Pituitary Adenomas—A Multicenter Experience. Cancers, 13(3), 537. https://doi.org/10.3390/cancers13030537