
Adjuvant Hysterectomy for Cervical Cancer Patients Treated with Chemoradiation Therapy: A Systematic Review on the Pathology-Proven Residual Disease Rate


 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Literature Search
2.3. Eligibility Criteria
2.4. Data Collection
2.5. Assessment of Risk of Bias
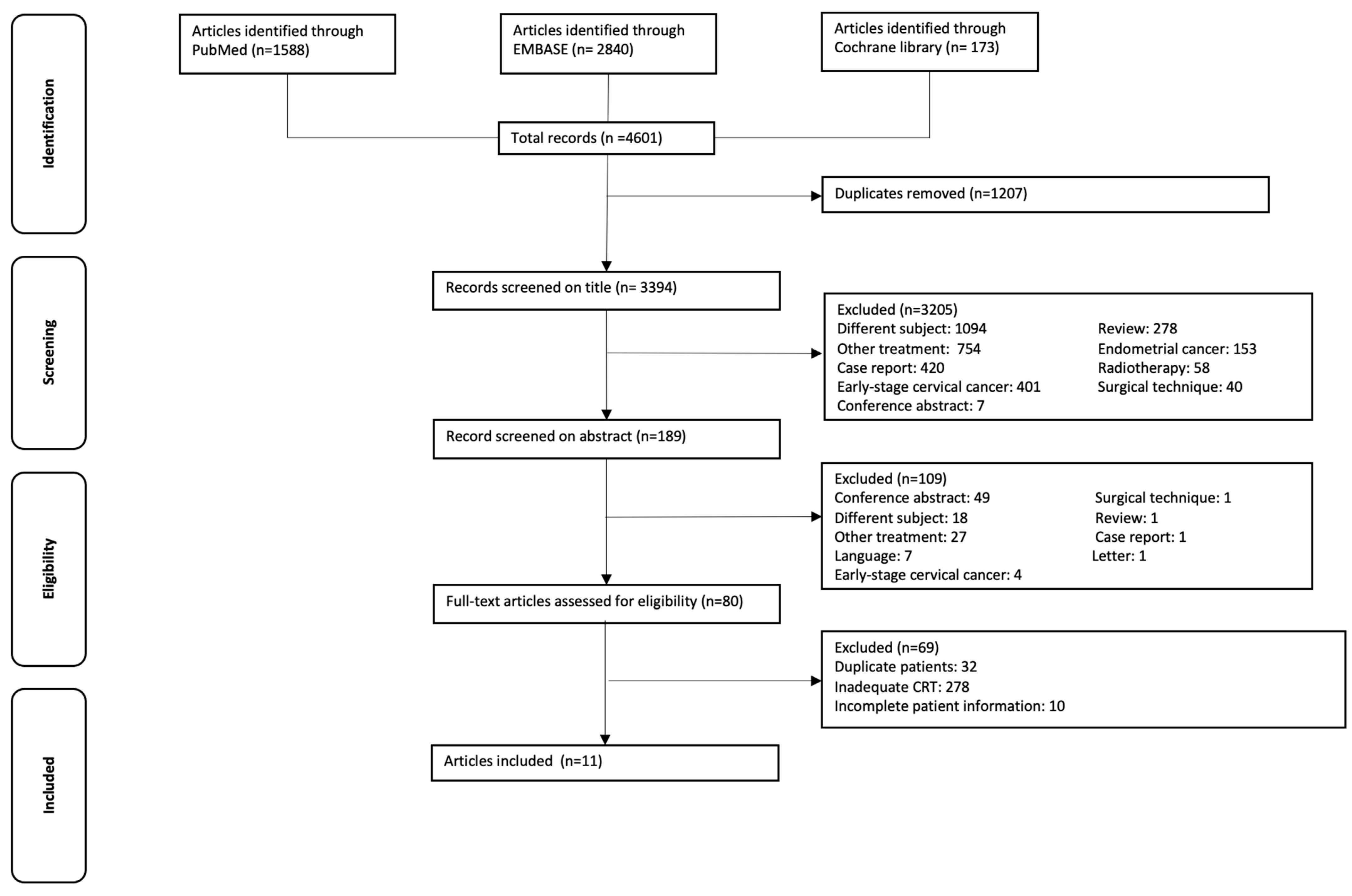
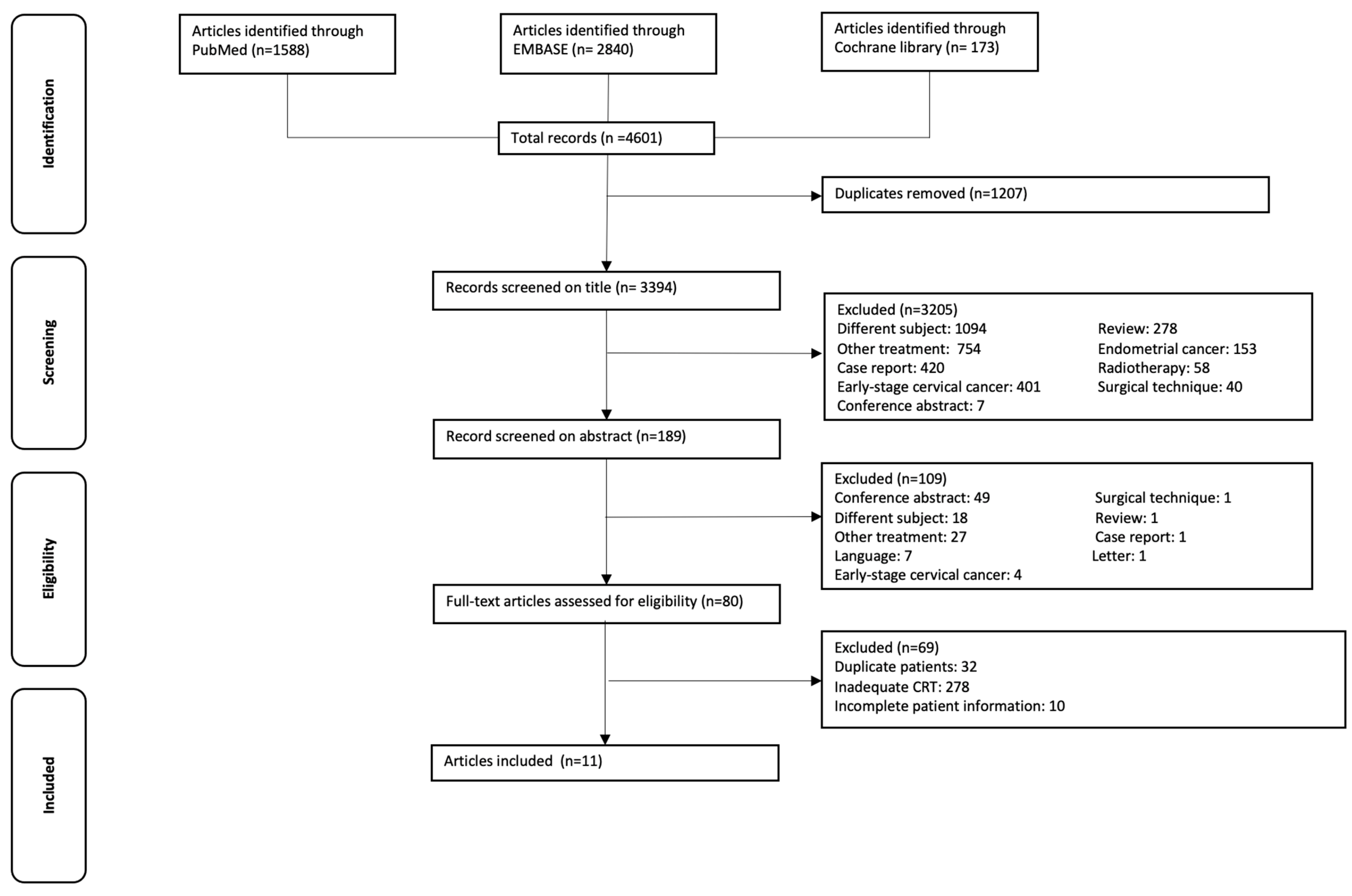
3. Results
3.1. Characteristics of Included Studies
3.2. Newcastle-Ottawa Scale
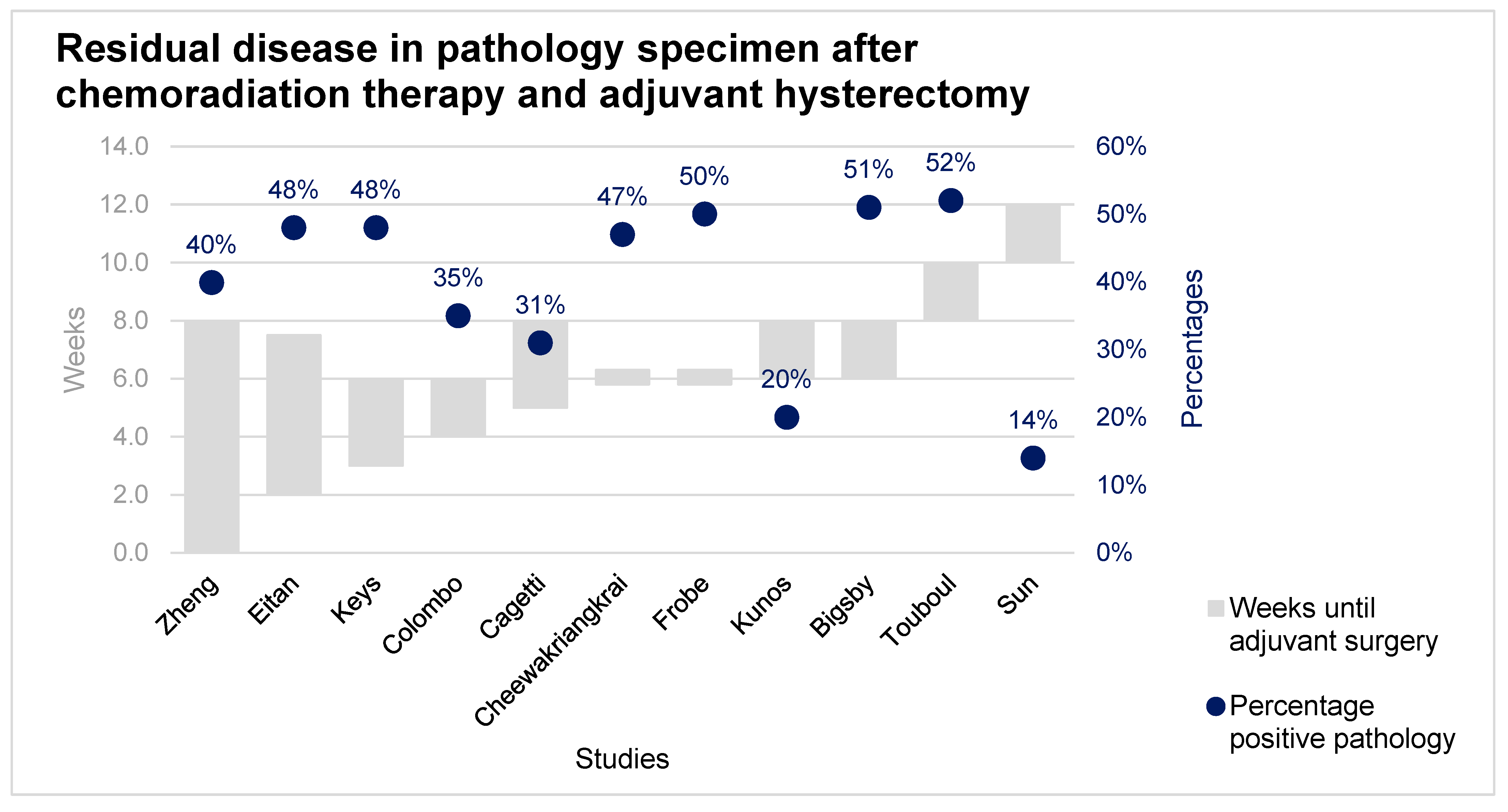
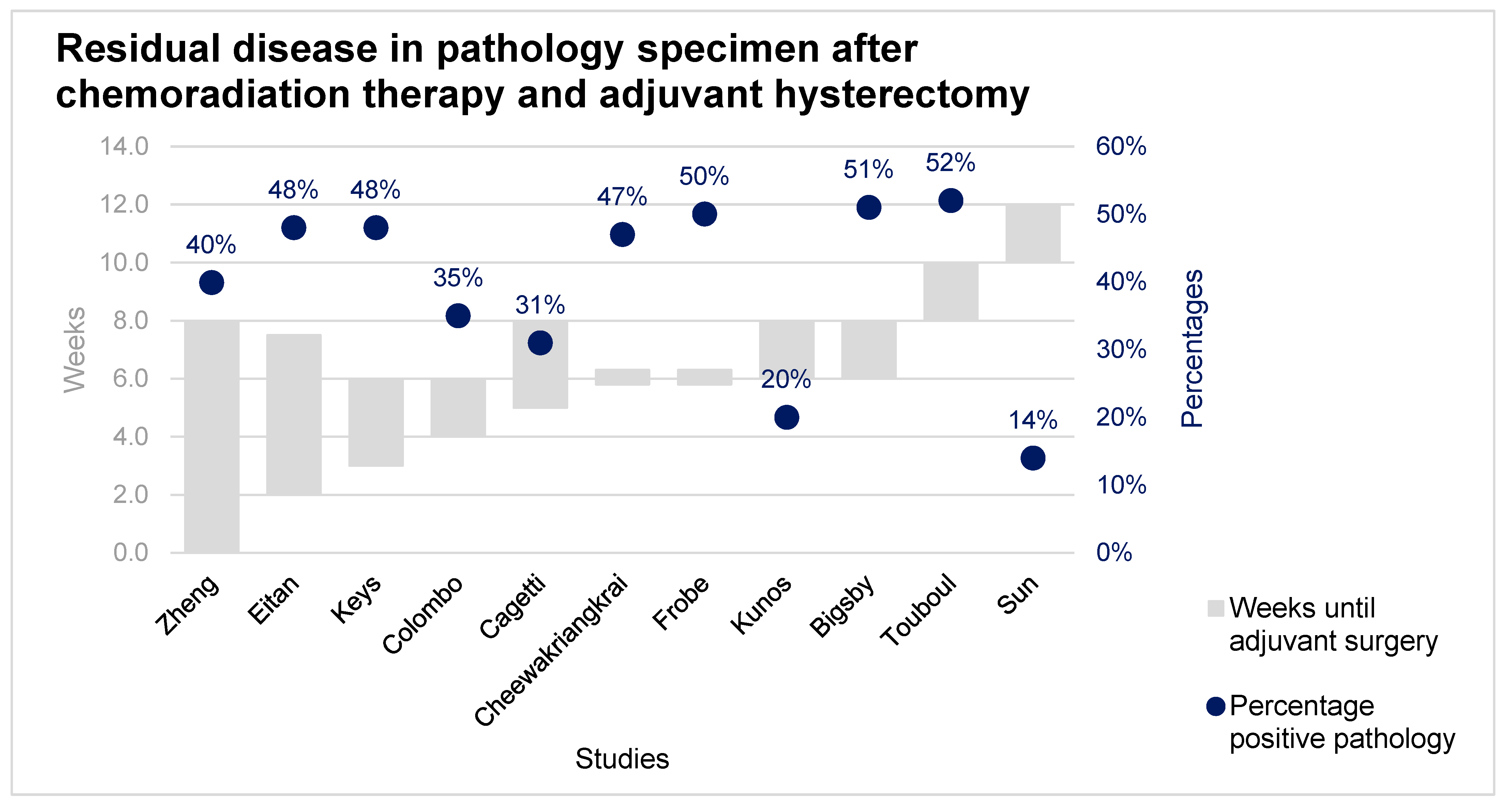
3.3. Analysis
4. Discussion
4.1. Comparison with Existing Literature
4.2. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Cervical Cancer 2019. Available online: https://www.who.int/cancer/prevention/diagnosis-screening/cervical-cancer/en/ (accessed on 2 December 2020).
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri. Int. J. Gynecol. Obstet. 2018, 143, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK. Cancer Statistics for the UK. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics-for-the-uk (accessed on 14 January 2020).
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Haie Meder, C.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int. J. Gynecol. Cancer 2018, 472, 641–655. [Google Scholar] [CrossRef] [PubMed]
- Eifel, P.J.; Winter, K.; Morris, M.; Levenback, C.; Grigsby, P.W.; Cooper, J.; Rotman, M.; Gershenson, D.; Mutch, D.G. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: An update of Radiation Therapy Oncology Group Trial (RTOG) 90-01. J. Clin. Oncol. 2004, 22, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Pötter, R.; Dimopoulos, J.; Georg, P.; Lang, S.; Waldhäusl, C.; Wachter-Gerstner, N.; Weitmann, H.; Reinthaller, A.; Knocke, T.H.; Wachter, S.K.C. Clinical impact of MRI assisted dose volume adaptation and dose escalation in brachytherapy of locally advanced cervix cancer. Radiother. Oncol. 2007, 83, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Sturdza, A.; Pötter, R.; Fokdal, L.U.; Haie-Meder, C.; Tan, L.T.; Mazeron, R.; Petric, P.; Šegedin, B.; Jurgenliemk-Schulz, I.M.; Nomden, C.; et al. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother. Oncol. 2016, 120, 428–433. [Google Scholar] [CrossRef]
- Shi, D.; Liang, Z.; Zhang, C.; Zhang, H.L.X. The effect of surgery on the survival status of patients with locally advanced cervical cancer after radiotherapy/chemoradiotherapy: A meta-analysis. BMC Cancer 2018, 8, 308. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.H.; Kim, S.N.; Chae, S.H.; Kim, J.E.L.S. Impact of adjuvant hysterectomy on prognosis in patients with locally advanced cervical cancer treated with concurrent chemoradiotherapy: A meta-analysis. J. Gynecol. Oncol. 2018, 29, e25. [Google Scholar] [CrossRef] [Green Version]
- Baskar, R.; Lee, K.A.; Yeo, R.; Yeoh, K.W. Cancer and radiation therapy: Current advances and future directions. Int. J. Med. Sci. 2012, 9, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Kol, K.G.G.; Ebisch, R.M.F.; Piek, J.M.J.; Zusterzeel, P.L.M.; Vergeldt, T.F.M.; Bekkers, R.L.M. Salvage surgery for patients with residual disease after chemoradiation therapy for locally advanced cervical cancer: A systematic review on indication, complications, and survival. Acta Obs. Gynecol. Scand. 2021, 100, 1176–1185. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, A.N.; Lee, L.J.; Eswara, J.R.; Horowitz, N.S.; Konstantinopoulos, P.A.; Mirabeau-Beale, K.L.; Rose, B.S.; Von Keudell, A.G.; Wo, J.Y. Complications of pelvic radiation in patients treated for gynecologic malignancies. Cancer 2014, 120, 3870–3883. [Google Scholar] [CrossRef]
- Keys, H.M.; Bundy, B.N.; Stehman, F.B.; Muderspach, L.I.; Chafe, W.E.; Suggs, C.L.; Walker, J.L.; Gersell, D.; Mackey, D. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N. Engl. J. Med. 1999, 340, 1154–1161. [Google Scholar] [CrossRef]
- Eitan, R.; Levavi, H.; Peled, Y.; Brenner, R.; Sabah, G.; Ben-Arie, A.; Dgani, R.; Fishman, A.; Sulkes, A.; Fenig, E.; et al. Should simple hysterectomy be added after chemo-radiation for stage IB2 and bulky IIA cervical carcinoma? Aust. N. Z. J. Obs. Gynaecol. 2010, 50, 289–293. [Google Scholar] [CrossRef]
- Colombo, P.E.; Bertrand, M.M.; Gutowski, M.; Mourregot, A.; Fabbro, M.; Saint-Aubert, B.; Quenet, F.; Gourgou, S.; Kerr, C.; Rouanet, P. Total laparoscopic radical hysterectomy for locally advanced cervical carcinoma (stages IIB, IIA and bulky stages IB) after concurrent chemoradiation therapy: Surgical morbidity and oncological results. Gynecol. Oncol. 2009, 114, 404–409. [Google Scholar] [CrossRef]
- Fröbe, A.; Jones, G.; Bokulić, T.; Mrčela, I.; Budanec, M.; Murgić, J.; Jakšić, B.; Prpić, M.; Bolanča, A.; Kusić, Z. High-dose-rate brachytherapy and concurrent chemoradiotherapy followed by surgery for stage Ib-IIb cervical cancer: Single institution experience. Anticancer Res. 2014, 34, 3861–3866. [Google Scholar] [PubMed]
- Cheewakriangkrai, C.; Srisomboon, J.; Chitapanarux, I.; Suprasert, P.; Phongnarisorn, C.; Sitthicha Siriaree, K.C. Concurrent cisplatin-based chemoradiation and adjuvant hysterectomy for bulky stage IB-IIA cervical cancer. J. Med. Assoc. Thai. 2005, 88, 1331–1337. [Google Scholar]
- Cagetti, L.; Zemmour, C.; Minsat, M.; Lambaudie, E.; Houvenaeghel, G.; Provansal, M.; Cappiello, M.A.; Rua, S.; Jauffret, C.; Ferré, M.; et al. Lessons from radiochemotherapy and modern image-guided adaptive brachytherapy followed by hysterectomy. Gynecol. Oncol. 2020, 156, 328–334. [Google Scholar] [CrossRef]
- Bigsby, G.E.; Robert, W.; Holloway Ahmad, S.; Michael, D.; Sombeck, G.E. Chemoradiation with adjuvant hysterectomy for stage IB-2 cervical cancer: A 10-year experience. Gynecol. Surg. 2012, 9, 327–333. [Google Scholar] [CrossRef] [Green Version]
- Kunos, C.; Ali, S.; Abdul-Karim, F.W.; Stehman, F.B.; Waggoner, S. Posttherapy residual disease associates with long-term survival after chemoradiation for bulky stage 1B cervical carcinoma: A Gynecologic Oncology Group study. Am. J. Obs. Gynecol. 2010, 203, 351.e1–351.e8. [Google Scholar] [CrossRef] [Green Version]
- Zheng, D.; Mou, H.P.; Diao, P.; Li, X.M.; Zhang, C.L.; Jiang, J.; Chen, J.L.; Wang, L.S.; Wang, Q.; Zhou, G.Y.; et al. Chemoradiotherapy in combination with radical surgery is associated with better outcome in cervical cancer patients. Oncotarget 2018, 9, 2866–2875. [Google Scholar] [CrossRef] [Green Version]
- Touboul, C.; Uzan, C.; Mauguen, A.; Gouy, S.; Rey, A.; Pautier, P.; Lhommé, C.; Duvillard, P.; Haie-Meder, C.; Morice, P. Prognostic Factors and Morbidities After Completion Surgery in Patients Undergoing Initial Chemoradiation Therapy for Locally Advanced Cervical Cancer. Oncologist 2010, 15, 405–415. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Sheng, X.; Jiang, J.; Li, X.; Liu, N.; Liu, Y.; Zhang, T.; Li, D.; Zhang, X.; Wei, P. Surgical morbidity and oncologic results after concurrent chemoradiation therapy for advanced cervical cancer. Int. J. Gynecol. Obstet. 2014, 125, 111–115. [Google Scholar] [CrossRef]
- Boers, A.; Arts, H.J.G.; Klip, H.; Nijhuis, E.R.; Pras, E.; Hollema, H.; Wisman, G.B.A.; Nijman, H.W.; Mourits, M.J.E.; Reyners, A.K.L.; et al. Radical surgery in patients with residual disease after (chemo)radiation for cervical cancer. Int. J. Gynecol. Cancer 2014, 24, 1276–1285. [Google Scholar] [CrossRef]
- Hoeijmakers, Y.M.; Snyers, A.; van Ham, M.A.P.C.; Zusterzeel, P.L.M.; Bekkers, R.L.M. Cervical biopsy after chemoradiation for locally advanced cervical cancer to identify residual disease: A retrospective cohort study. J. Surg. Oncol. 2019, 2, 2–6. [Google Scholar]
- Morice, P.; Rouanet, P.; Rey, A.; Romestaing, P.; Houvenaeghel, G.; Boulanger, J.C.; Leveque, J.; Cowen, D.; Mathevet, P.; Malhaire, J.P.; et al. NoResults of the GYNECO 02 study, an FNCLCC phase III trial comparing hysterectomy with no hysterectomy in patients with a (clinical and radiological) complete response after chemoradiation therapy for stage IB2 or II cervical cancer. Oncologist 2012, 17, 64–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetina, L.; Garcia-Arias, A.; Candelaria, M.; Cantú, D.; Rivera, L.; Coronel, J.; Bazan-Perkins, B.; Flores, V.; Gonzalez, A.D.G.A. Brachytherapy versus radical hysterectomy after external beam chemoradiation: A non-randomized matched comparison in IB2-IIB cervical cancer patients. World J. Surg. Oncol. 2009, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Wydra, D.; Emerich, J.; Sawicki, S.; Ciach, K.; Marciniak, A. Major complications following exenteration in cases of pelvic malignancy: A 10-year experience. World J. Gastroenterol. 2006, 12, 1115–1119. [Google Scholar] [CrossRef]
- Magrina, J.F.; Goodrich, M.A.; Weaver, A.L.; Podratz, K.C. Modified radical hysterectomy: Morbidity and mortality. Gynecol. Oncol. 1995, 59, 277–282. [Google Scholar] [CrossRef]
- Narayanan, P.; Nobbenhuis, M.; Reynolds, K.M.; Sahdev, A.; Reznek, R.H.; Rockall, A.G. Fistulas in malignant gynecologic disease: Etiology, imaging, and management. Radiographics 2009, 29, 1073–1083. [Google Scholar] [CrossRef]
- Hilton, P.; Cromwell, D.A. The risk of vesicovaginal and urethrovaginal fistula after hysterectomy performed in the English National Health Service-a retrospective cohort study examining patterns of care between 2000 and 2008. BJOG An. Int. J. Obs. Gynaecol. 2012, 119, 1447–1454. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Author (Year) | Inclusion Period (Years) | Total Number of Patients (Treated with Chemoradiation Therapy and Adjuvant Hysterectomy) | Age Median/Mean (Range) | FIGO Stage *1 | Histology | Chemoradiation Therapy regimen | Brachytherapy Dosage | Type of Adjuvant Hysterectomy | Time Until Adjuvant Hysterectomy | Positive Pathology Results After Surgery n (%) | Follow-up Period Median/Mean (Range) | Recurrence n (%) | Survival n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Keys (1999) [13] | 1992–1997 | 374 (183) | Unknown | IB = 183 | SCC = 147, AC = 9, ASC = 17, Other = 10 | 45 Gy EBRT with concomitant cisplatin (40 mg/m2) *2 | 30 Gy | Extrafascial hysterectomy *3 | 3–6 weeks | 88 (48%) | Median 26 months | 38 (21%) | 27 died (15%) |
| Eitan (2010) [14] | 2003–2006 | 23 | Median 50 year (range, 30–67 year) | IB2 = 20, IIA = 3 | SCC = 22, AC = 1 | 45 Gy EBRT with concomitant cisplatin (35 mg/m2) *4 | 14 Gy (2 × 7 Gy) | Simple extra-fascial total abdominal hysterectomy and bilateral salpingo-oophorectomy (and in 16 patients PLND). | Median 5 weeks, range 14–52 days. | 11 (48%) | Median 20 months (range, 10–50 months) | 4 (17.4%) | 2 (8.7%) |
| Colombo (2009) [15] | 2000–2008 | 102 | Mean 44 year (range, 24–74 year) | IB = 28, IIA = 13, IIB = 61 | SCC = 91 AC = 10 other = 1 | 45 Gy EBRT with concomitant cisplatin (40 mg/m2. | 15 Gy *5 | 56 abdominal radical hysterectomy and 46 total laparoscopic radical hysterectomy | 4–6 weeks | 36 (35%) | Mean 31.2 months | 32 (31.4%): 18 (17.6%) local and 14 (13.7%) distant | 3-year OS 82%, 19 died (18.6%) |
| Fröbe (2014) [16] | 2002–2008 | 24 | Median 50 year (range, 39–71 year) | IB = 8, IIA = 3, IIB = 13 | SCC = 19 AC = 5 | 40 Gy EBRT with concomitant cisplatin (30 mg/m2) *6 | 28 Gy (4 × 7 Gy) | Radical hysterectomy and bilateral salphingo-oophorectomy without lymph node dissection | 6 weeks | 12 (50%) | Median 67 months (range 4–107 months) | three distant metastases (12.5%) | Six died (25%) three without evidence of disease |
| Cheewakriangkrai (2005) [17] | 1999–2001 | 34 | Mean 44 year (range, 30–66 year) | IB1 = 4, IB2 = 25, IIA = 5 | SCC = 22 AC = 11 ASC = 1 | 46–50 Gy ERBT with weekly concomitant cisplatin (40 mg/m2). | 30 Gy (4 × 7.5 Gy) | Extra-fascial hysterectomy | 6 weeks | 16 (47%) | Median 42 months (range 7–58 months) | Six (18.2%):one distant, three local and two combined | five deaths (14.7%) |
| Cagetti (2020) [18] | 2012–2017 | 145 (90) | Median 54 year (range, 24–90 year) | IB = 33, IIA = 9, IIB = 40, III-IV = 8 | SCC = 66, AC = 19, other = 5 | 45 Gy EBRT with concomitant cisplatin (40 mg/m2) *7 | 27.5 Gy (5 × 5.5 Gy) | Radical hysterectomy | 5–8 weeks median: 61 ± 26 days | 28 (31%) | Median 30.8 months (range, 26.0–30.0 months) | 11 local (12.2%) | 3-year OS 50–90% depending on pathology results |
| Bigsby (2011) [19] | 1999–2009 | 69 | Mean 47 year (range, 27–82 year) | IB2 = 69 | SCC = 55 AC = 11 ASC = 3 | 45–50.4 Gy EBRT with concomitant cisplatin (25–40 mg/ m2) *8 | 15–18 Gy (3 × 5–6 Gy) | Extra-fascial total abdominal hysterectomy with common and para-aortic lymphadenectomy | 6–8 weeks | 35 (51%) | Mean 61.7 months (range 10.9–122.5 months) | 16 (23.2%) 2 local, 14 distant | 16 deaths (23.2%) three were of unrelated causes. |
| Kunos (2010) [20] | Unknown | 464 (175) | Median 40 year (range, 21–81 year) | IB = 175 | SCC = 140, AC = 9, ACS = 16, Other = 10 | 45 Gy EBRT with concomitant cisplatin (40 mg/m2) | 30 Gy | Total extrafascial. hysterectomy | 6–8 weeks | 35 (20%) *9 | Median 128 months | 39 (22.3%): 16 (9%) local, 23 (13%) distant | 30 cancer related deaths, 15 death of unrelated cause. |
| Zheng (2017) [21] | 2008–2013 | 314 (163) | Median 51 (range, 26–73 year) | IB2 = 35, IIA = 71, IIB = 57 | SCC = 136, AC = 27 | 46–50 Gy EBRT with concomitant cisplatin (40 mg/m2) *10 | 25–30 Gy | Radical hysterectomy and PLND | Within 8 weeks | 65 (39.9%) | Unknown | 48 (29.4%) 12 local, 29 metastases, seven local and distant | 3-year OS 87.1% 21 deaths (12.9%) |
| Touboul (2009) [22] | 1998–2007 | 150 | Median 47 year (range, 19–77 year) | IB2 = 48, II = 91, III = 10, IV = 1 | SCC = 108 AC = 26 other = 16 | 45 Gy EBRT with concomitant cisplatin (40 mg/m2) *11 | 15 Gy | Radical hysterectomy (n = 44) or simple extra fascial hysterectomy (n = 106) with or without para-aortic and/or PLND | 8–10 weeks | 78 (52%) | Median 43.2 months (range, 2.4–127.2 months) | 41 (27%) | 37 deaths (24.7%) |
| Sun (2013) [23] | 1992–2012 | 378 (192) | Median 48 year (range, 20–75 year) | IIB = 90, III = 101, IVA = 1 | SCC = 149 AC= 30 other= 13 | 44–55 Gy EBRT with concurrent cisplatin (40 mg/m2) and 5-FU (500 mg/m2) | 45–55 Gy | 99 Extra-fascial hysterectomy and 81 Extended hysterectomy 12 other | 10–12 weeks | 27 (14%) | Median 190 months (range 60–245) | 32 (16.7%) | 60 deaths (31.1%) |
| Total | 2077(1205) | Range, 19–90 years | IB = 427, IB1 = 4, IB2 = 197, II = 91, IIA = 104, IIB = 261, III = 111, IV = 1 IVA = 1 III-IVA = 8 | SCC = 955, AC = 158, ASC = 37, Other = 55 | 411(34%) | Range 2.4–245 months | 270 local/distant | 223 died based on 10 studies of which 21 died of unrelated causes to cervical cancer. |
| Article | Selection | Comparability | Outcome | Quality | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort * | Selection Cohorts’ Same Source | Ascertainment of Exposure ** | Outcome of Interest was not Present at Start of Study | Comparability of Cohorts | Assessment of Outcome *** | Follow-Up **** | Adequacy of Follow-Up | ||
| Keys (1999) [13] |  | NA | | | NA | | Median 36 months | No statement about lost to follow-up | Fair |
| Etian (2010) [14] | | NA | | | NA | | Median 20 months (range 10–50 months) | No statement about lost to follow-up | Fair |
| Colombo (2009) [15] | | NA | Not reported | | NA | Not reported | Median 31 months | No statement about lost to follow-up | Poor |
| Fröbe (2014) [16] | | NA | Not reported | | NA | Not reported | Median 5.59 years (range 0.32–8.9 year) | No patient lost to follow-up | Fair |
| Chweewakriangkrai (2005) [17] | | NA | Not reported | | NA | Not reported | Median 42 months (range 7–58 months) | 1 patient was lost to follow-up | Fair |
| Cagetti (2020) [18] | | NA | | | NA | | Median 30.8 months (range, 26.0- 30.0 months) | No statement about lost to follow-up | Fair |
| Bigsby (2010) [19] | | NA | | | NA | | Mean 71.7 months (range 10.9–122.5 months) | No patients lost to follow-up | Good |
| Kunos (2010) [20] | | NA | | | NA | | Median 118 months | Three patients lost to follow-up | Fair |
| Zheng (2017) [21] | | NA | | | NA | | No follow-up period reported | No statement about lost to follow-up | Fair |
| Touboul (2014) [22] | | NA | | | NA | | Median 3.6 years (range 0.2–10.6 year) | Four patients lost to follow up | Good |
| Sun (2013) [23] | | NA | | | NA | | Median 190 months (range 60–245 months) | No statement about lost to follow-up | Fair |
: fulfilled the criteria of the Newcastle Ottawa Scale for this item.| Auteur (Year) | Patients Treated with Adjuvant Hysterectomy | Fistula | Urinary Tract | Female Genital Tract | Gastrointestinal | Infection | Other | Total |
|---|---|---|---|---|---|---|---|---|
| Eitan (2010) [14] | 23 | One recto-vaginal fistula | 10 cystitis | 11 diarrheas | Seven anemia, two lymphedema | 31 | ||
| Colombo (2009) [15] | 144 | Seven urinary fistulas, two digestive fistulas | 15 vesical dysfunction, 12 cystitis, three bladder injury, two ureteral injury | Two digestive injury | Two pelvic infections | Six intraoperative hemorrhages, five other, two symptomatic lymphocysts, one pulmonary embolism, one postoperative hemorrhage | 64 | |
| Bigsby (2011) [19] | 69 | One enterocutaneous fistula, one rectovaginal fistula | One ureteral stenosis requiring stent, one cystotomy with repair | Two vaginal stenosis, one vaginal fault necrosis/grade four proctitis, one vaginal vault necrosis, | one complete small bowel obstruction | One deep venous thrombosis | 10 | |
| Touboul (2009) [22] | 150 | Five ureteral fistula, five bowel fistulas, one bladder fistula | Two ureteral stenosis, two bladder retention, one urinary incontinence | One vaginal vault dehiscence with abscess | Two bowel obstruction, one epigastralgia | Five abscesses, three peritonitis | Nine lymphedemas, eight lymphocysts, three chylous ascites, three phlebitis, two deaths related to postoperative morbidity, two rupture of iliac vessels, two wound dehiscence | 57 |
| Sun (2013) [23] | 192 | Two ureteral fistula, one bowel fistula, one bladder fistula | Two ureteral stenosis, one bladder retention, one urinary incontinence | One vaginal vault dehiscence with abscess | One bowel obstruction | Two abscesses, one peritonitis | 15 lymphocysts, three lymphedemas, two death related to postoperative morbidity, two chylous ascites, two ruptures of iliac vessels, two wound dehiscence, one phlebitis | 40 |
| Total | 578 | 27 | 53 | 6 | 18 | 13 | 81 | 202 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Kol, K.; Ebisch, R.; Piek, J.; Beugeling, M.; Vergeldt, T.; Bekkers, R. Adjuvant Hysterectomy for Cervical Cancer Patients Treated with Chemoradiation Therapy: A Systematic Review on the Pathology-Proven Residual Disease Rate. Cancers 2021, 13, 6190. https://doi.org/10.3390/cancers13246190
van Kol K, Ebisch R, Piek J, Beugeling M, Vergeldt T, Bekkers R. Adjuvant Hysterectomy for Cervical Cancer Patients Treated with Chemoradiation Therapy: A Systematic Review on the Pathology-Proven Residual Disease Rate. Cancers. 2021; 13(24):6190. https://doi.org/10.3390/cancers13246190
Chicago/Turabian Stylevan Kol, Kim, Renée Ebisch, Jurgen Piek, Maaike Beugeling, Tineke Vergeldt, and Ruud Bekkers. 2021. "Adjuvant Hysterectomy for Cervical Cancer Patients Treated with Chemoradiation Therapy: A Systematic Review on the Pathology-Proven Residual Disease Rate" Cancers 13, no. 24: 6190. https://doi.org/10.3390/cancers13246190
APA Stylevan Kol, K., Ebisch, R., Piek, J., Beugeling, M., Vergeldt, T., & Bekkers, R. (2021). Adjuvant Hysterectomy for Cervical Cancer Patients Treated with Chemoradiation Therapy: A Systematic Review on the Pathology-Proven Residual Disease Rate. Cancers, 13(24), 6190. https://doi.org/10.3390/cancers13246190