
Systemic Anti-Cancer Therapy and Metastatic Cancer Are Independent Mortality Risk Factors during Two UK Waves of the COVID-19 Pandemic at University College London Hospital


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Data Collection
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Demographics of Patients with Cancer and Patients without Cancer in Both Waves of COVID-19
3.2. Risk Factors of SARS-CoV-2 Mortality in Both Waves
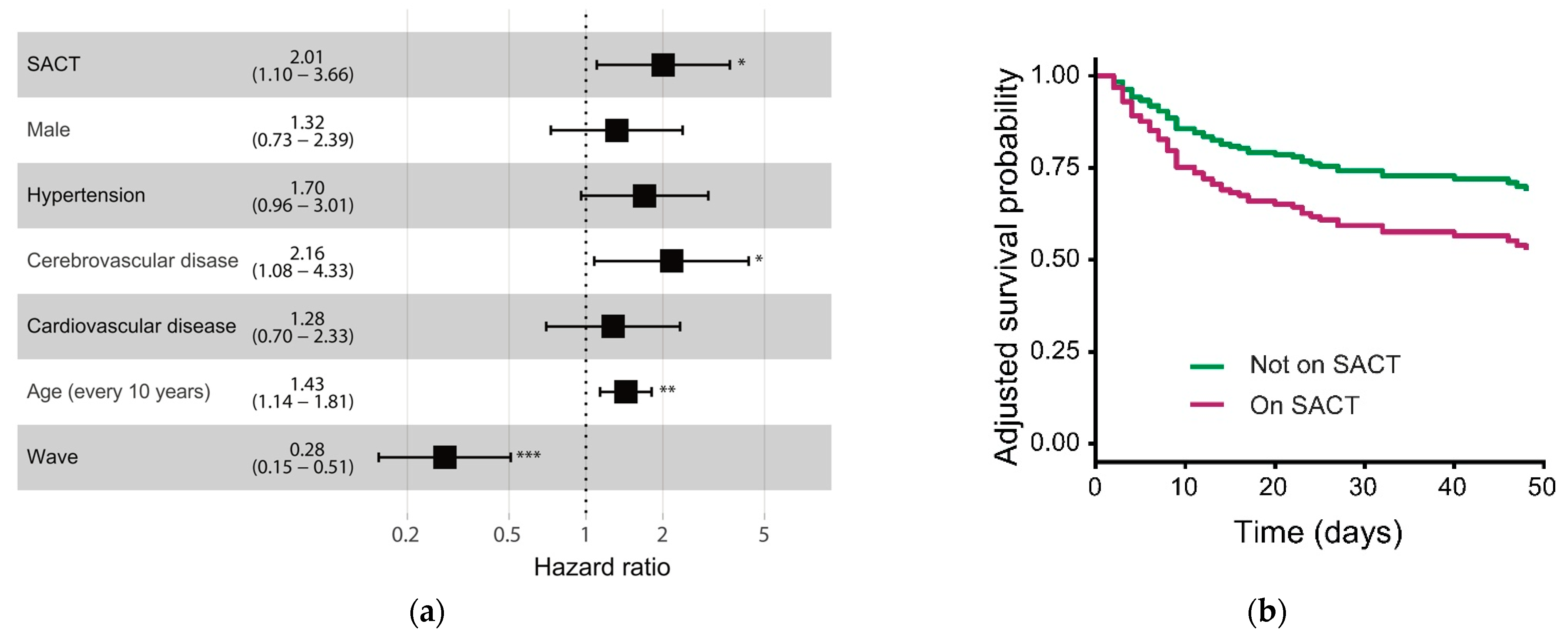
3.3. Determinants of Mortality among Patients with Cancer from Both Waves
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, A.J.X.; Purshouse, K. COVID-19 and cancer registries: Learning from the first peak of the SARS-CoV-2 pandemic. Br. J. Cancer 2021, 124, 1777–1784. [Google Scholar] [CrossRef]
- Sng, C.C.T.; Wong, Y.N.S.; Wu, A.; Ottaviani, D.; Chopra, N.; Galazi, M.; Benafif, S.; Soosaipillai, G.; Roylance, R.; Lee, A.J.X.; et al. Cancer History and Systemic Anti-Cancer Therapy Independently Predict COVID-19 Mortality: A UK Tertiary Hospital Experience. Front. Oncol. 2020, 10, 595804. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multi-center study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Yuan, X.; Xiao, J.; Zhong, Q.; Yang, C.; Liu, B.; Cai, Y.; Lu, Z.; Wang, J.; Wang, Y.; et al. Clinical characteristics and risk factors associated with COVID-19 disease severity in patients with cancer in Wuhan, China: A multicentre, retrospective, cohort study. Lancet Oncol. 2020, 21, 893–903. [Google Scholar] [CrossRef]
- de Azambuja, E.; Brandão, M.; Wildiers, H.; Laenen, A.; Aspeslagh, S.; Fontaine, C.; Collignon, J.; Lybaert, W.; Verheezen, J.; Rutten, A.; et al. Impact of solid cancer on in-hospital mortality overall and among different subgroups of patients with COVID-19: A nationwide, population-based analysis. ESMO Open 2020, 5, e000947. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Yekedüz, E.; Utkan, G.; Ürün, Y. A systematic review and meta-analysis: The effect of active cancer treatment on severity of COVID-19. Eur. J. Cancer 2020, 141, 92–104. [Google Scholar] [CrossRef] [PubMed]
- Kirby, T. New variant of SARS-CoV-2 in UK causes surge of COVID-19. Lancet Respir. Med. 2021, 9, e20–e21. [Google Scholar] [CrossRef]
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.B.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef]
- Public Health England. Guidance on Shielding and Protecting People WHO Are Clinically Extremely Vulnerable from COVID-19. Available online: https://www.gov.uk/government/publications/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19 (accessed on 11 November 2021).
- Oran, D.P.; Topol, E. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Petersen, I.; Phillips, A. Three Quarters of People with SARS-CoV-2 Infection are Asymptomatic: Analysis of English Household Survey Data. Clin. Epidemiol. 2020, 12, 1039–1043. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—preliminary report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group Dexamethasone in Hospitalized Patients with COVID-19—Preliminary Report. N. Engl. J. Med. 2021, 384, 693–704. [CrossRef]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Mariniello, A.; Bironzo, P.; Pisano, C.; De Filippis, M.; Persano, I.; Olmetto, E.; Caramello, V.; Boccuzzi, A.; Capelletto, E.; Passiglia, F.; et al. Descriptive Comparative Analysis of Patients with Cancer Referring to the Emergency Department of an Italian University Hospital Across the Severe Acute Respiratory Syndrome Coronavirus 2 Waves. JCO Oncol. Pract. 2021, OP2100098. [Google Scholar] [CrossRef] [PubMed]
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernández-Flix, S.; de Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Andreychuk, N.; et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PLoS ONE 2021, 16, e0248029. [Google Scholar] [CrossRef]
- Public Health England. PHE: Investigaton of Novel SARS-CoV-2 Variants of Concern (England)—Technical Briefing 9. 22 April 2021. Available online: https://www.gov.uk/government/publications/phe-investigaton-of-novel-sars-cov-2-variants-of-concern-england-technical-briefing-9-22-april-2021 (accessed on 11 November 2021).
- Ben-Aharon, I.; Waldhorn, I.; Holland, R.; Peer, A.; Halberthal, M.; Goshen-Lago, T.G. 1559O Efficacy and toxicity of BNT162b2 vaccine in cancer patients. Ann. Oncol. 2021, 32, S1130. [Google Scholar] [CrossRef]
- Oosting, S.; Van der Veldt, A.; GeurtsvanKessel, C.; Fehrmann, R.; van Binnendijk, R.; Dingemans, A.-M.; Smit, E.; Hiltermann, T.; Hartog, G.D.; Jalving, M.; et al. LBA8 Vaccination against SARS-CoV-2 in patients receiving chemotherapy, immunotherapy, or chemo-immunotherapy for solid tumors. Ann. Oncol. 2021, 32, S1337. [Google Scholar] [CrossRef]
- Joint Committee on Vaccination and Immunisation (JCVI). Joint Committee on Vaccination and Immunisation: Advice on Priority Groups for COVID-19 Vaccination. 30 December 2020. Available online: https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-30-december-2020/joint-committee-on-vaccination-and-immunisation-advice-on-priority-groups-for-covid-19-vaccination-30-december-2020 (accessed on 11 November 2021).
- Ribas, A.; Sengupta, R.; Locke, T.; Zaidi, S.K.; Campbell, K.M.; Carethers, J.M.; Jaffee, E.M.; Wherry, E.J.; Soria, J.-C.; D’Souza, G. Priority COVID-19 Vaccination for Patients with Cancer while Vaccine Supply Is Limited. Cancer Discov. 2021, 11, 233–236. [Google Scholar] [CrossRef]
- Pinato, D.J.; Scotti, L.; Gennari, A.; Colomba-Blameble, E.; Dolly, S.; Loizidou, A.; Chester, J.; Mukherjee, U.; Zambelli, A.; Aguilar-Company, J.; et al. Determinants of enhanced vulnerability to COVID-19 in UK cancer patients: A European Study. Eur. J. Cancer 2021, 150, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.H.; Michlmayr, D.; Gubbels, S.M.; Mølbak, K.; Ethelberg, S. Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: A population-level observational study. Lancet 2021, 397, 1204–1212. [Google Scholar] [CrossRef]
- Nadkarni, A.R.; Vijayakumaran, S.C.; Gupta, S.; Divatia, J.V. Mortality in Cancer Patients With COVID-19 Who Are Admitted to an ICU or Who Have Severe COVID-19: A Systematic Review and Meta-Analysis. JCO Glob. Oncol. 2021, 7, 1286–1305. [Google Scholar] [CrossRef] [PubMed]
- Tashkandi, E.; Al-Abdulwahab, A.; Basulaiman, B.; Alsharm, A.; Al-Hajeili, M.; Alshadadi, F.; Halawani, L.; Al-Mansour, M.; Alquzi, B.; Barnawi, S.; et al. Mortality and morbidity of curative and palliative anticancer treatments during the COVID-19 pandemic: A multicenter population-based retrospective study. Mol. Clin. Oncol. 2021, 14, 1–11. [Google Scholar] [CrossRef]
- Grivas, P.; Khaki, A.; Wise-Draper, T.; French, B.; Hennessy, C.; Hsu, C.-Y.; Shyr, Y.; Li, X.; Choueiri, T.; Painter, C.; et al. Association of clinical factors and recent anticancer therapy with COVID-19 severity among patients with cancer: A report from the COVID-19 and Cancer Consortium. Ann. Oncol. 2021, 32, 787–800. [Google Scholar] [CrossRef]
- Pinato, D.J.; Lee, A.J.X.; Biello, F.; Seguí, E.; Aguilar-Company, J.; Carbó, A.; Bruna, R.; Bower, M.; Rizzo, G.; Benafif, S.; et al. Presenting Features and Early Mortality from SARS-CoV-2 Infection in Cancer Patients during the Initial Stage of the COVID-19 Pandemic in Europe. Cancers 2020, 12, 1841. [Google Scholar] [CrossRef]
- Pinato, D.J.; Zambelli, A.; Aguilar-Company, J.; Bower, M.; Sng, C.; Salazar, R.; Bertuzzi, A.; Brunet, J.; Mesia, R.; Segui, E.; et al. Clinical portrait of the SARS-CoV-2 epidemic in European cancer patients. Cancer Discov. 2020, 10, 1465–1474. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.W.; Cazier, J.-B.; Angelis, V.; Arnold, R.; Bisht, V.; A Campton, N.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.T.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Lee, L.Y.W.; Cazier, J.-B.; Starkey, T.; Briggs, S.E.W.; Arnold, R.; Bisht, V.; Booth, S.; Campton, N.A.; Cheng, V.W.T.; Collins, G.; et al. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: A prospective cohort study. Lancet Oncol. 2020, 21, 1309–1316. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Overview|COVID-19 Rapid Guideline: Delivery of Systemic ANTICANCER Treatments. 2020. Available online: https://www.nice.org.uk/guidance/ng161 (accessed on 11 November 2021).
- Wang, B.; Huang, Y. Immunotherapy or other anti-cancer treatments and risk of exacerbation and mortality in cancer patients with COVID-19: A systematic review and meta-analysis. OncoImmunology 2020, 9, 1824646. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.-C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Vivarelli, S.; Falzone, L.; Grillo, C.M.; Scandurra, G.; Torino, F.; Libra, M. Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers 2020, 12, 2237. [Google Scholar] [CrossRef] [PubMed]
- Vivarelli, S.; Falzone, L.; Torino, F.; Scandurra, G.; Russo, G.; Bordonaro, R.; Pappalardo, F.; Spandidos, D.A.; Raciti, G.; Libra, M. Immune-checkpoint inhibitors from cancer to COVID-19: A promising avenue for the treatment of patients with COVID-19. Int. J. Oncol. 2020, 58, 145–157. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wave 1 Control (n = 226) | Wave 1 Cancer (n = 94) | Wave 2 Control (n = 226) | Wave 2 Cancer (n = 113) | p-Value | |
|---|---|---|---|---|---|
| Male | 152 (67.3%) | 62 (66.0%) | 122 (54.0%) | 61 (54.0%) | *** |
| Median age(years) | 70.50 (60.00–80.00) | 71.00 (62.00–80.00) | 71.00 (58.00–79.00) | 71.00 (58.00–79.00) | |
| BMI | 26.59 (23.45–30.47) | 25.05 (21.72–30.48) | 26.71 (23.34–32.12) | 26.20 (22.37–30.48) | |
| South Asian | 28 (12.4%) | 8 (8.5%) | 42 (18.6%) | 18 (15.9%) | ** |
| Black | 37 (16.4%) | 6 (6.4%) | 29 (12.8%) | 10 (8.8%) | |
| Other | 19 (8.4%) | 9 (9.6%) | 17 (7.5%) | 13 (11.5%) | |
| White | 115 (50.9%) | 64 (68.1%) | 78 (34.5%) | 54 (47.8%) | ** |
| Ex or active smoker | 71 (31.4%) | 49 (52.1%) | 64 (28.3%) | 47 (41.6%) | |
| Cardiovascular disease | 59 (26.1%) | 18 (19.1%) | 57 (25.2%) | 19 (16.8%) | |
| Dementia | 35 (15.5%) | 7 (7.4%) | 17 (7.5%) | 7 (6.2%) | ** |
| Diabetes | 73 (32.3%) | 24 (25.5%) | 77 (34.1%) | 25 (22.1%) | |
| Congestive cardiac failure | 16 (7.1%) | 9 (9.6%) | 11 (4.9%) | 4 (3.5%) | |
| Liver disease | 4 (1.8%) | 3 (3.2%) | 5 (2.2%) | 0 (0.0%) | |
| Hypertension | 123 (54.4%) | 37 (39.4%) | 106 (46.9%) | 48 (42.5%) | |
| Peripheral vascular disease | 13 (5.8%) | 2 (2.1%) | 1 (0.4%) | 4 (3.5%) | * |
| Cerebrovascular disease | 37 (16.4%) | 12 (12.8%) | 12 (5.3%) | 14 (12.4%) | ** |
| Chronic lung disease | 47 (20.8%) | 14 (14.9%) | 51 (22.6%) | 16 (14.2%) | |
| Chronic kidney disease | 26 (11.5%) | 12 (12.8%) | 23 (10.2%) | 13 (11.5%) | |
| Ongoing corticosteroids | 13 (5.8%) | 4 (4.3%) | 2 (0.9%) | 3 (2.7%) | ** |
| Composite co-morbidity score † | 2.57 (1.71) | 2.79 (1.44) | 2.04 (1.33) | 2.81 (1.42) | * |
| COVID-19-specific therapy | 13 (5.8%) | 1(1.1%) | 134 (59.3%) | 37 (32.7%) | **** |
| Hospitalization | 223 (98.7%) | 86 (91.5%) | 179 (79.2%) | 82 (72.6%) | *** |
| Intensive care admission | 76 (33.6%) | 22 (23.4%) | 68 (30.1%) | 24 (21.2%) | |
| Death | 77 (34.1%) | 41 (43.6%) | 43 (19.0%) | 18 (15.9%) | *** |
| HR (95% CI) | p-Value | |
|---|---|---|
| Malignancy status | ||
| Metastatic | 2.1 (1.02–4.34) | 0.04 |
| Active anti-cancer treatment | 1.75 (0.97–3.18) | 0.06 |
| SACT | 2.01 (1.10–3.66) | 0.02 |
| Cytotoxic chemotherapy | 1.93 (0.93–4.00) | 0.08 |
| Endocrine therapy | 1.66 (0.69–3.96) | 0.25 |
| Targeted therapy | 0.84 (0.11–6.28) | 0.86 |
| Immunotherapy | 1.73 (0.4–7.41) | 0.46 |
| Radiotherapy | 2.04 (0.62–6.74) | 0.24 |
| Surgery | 0.67 (0.09–4.98) | 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, Y.N.S.; Sng, C.C.T.; Ottaviani, D.; Patel, G.; Chowdhury, A.; Earnshaw, I.; Sinclair, A.; Merry, E.; Wu, A.; Galazi, M.; et al. Systemic Anti-Cancer Therapy and Metastatic Cancer Are Independent Mortality Risk Factors during Two UK Waves of the COVID-19 Pandemic at University College London Hospital. Cancers 2021, 13, 6085. https://doi.org/10.3390/cancers13236085
Wong YNS, Sng CCT, Ottaviani D, Patel G, Chowdhury A, Earnshaw I, Sinclair A, Merry E, Wu A, Galazi M, et al. Systemic Anti-Cancer Therapy and Metastatic Cancer Are Independent Mortality Risk Factors during Two UK Waves of the COVID-19 Pandemic at University College London Hospital. Cancers. 2021; 13(23):6085. https://doi.org/10.3390/cancers13236085
Chicago/Turabian StyleWong, Yien Ning Sophia, Christopher C. T. Sng, Diego Ottaviani, Grisma Patel, Amani Chowdhury, Irina Earnshaw, Alasdair Sinclair, Eve Merry, Anjui Wu, Myria Galazi, and et al. 2021. "Systemic Anti-Cancer Therapy and Metastatic Cancer Are Independent Mortality Risk Factors during Two UK Waves of the COVID-19 Pandemic at University College London Hospital" Cancers 13, no. 23: 6085. https://doi.org/10.3390/cancers13236085
APA StyleWong, Y. N. S., Sng, C. C. T., Ottaviani, D., Patel, G., Chowdhury, A., Earnshaw, I., Sinclair, A., Merry, E., Wu, A., Galazi, M., Benafif, S., Soosaipillai, G., Chopra, N., Roylance, R., Shaw, H., & Lee, A. J. X. (2021). Systemic Anti-Cancer Therapy and Metastatic Cancer Are Independent Mortality Risk Factors during Two UK Waves of the COVID-19 Pandemic at University College London Hospital. Cancers, 13(23), 6085. https://doi.org/10.3390/cancers13236085