
High Levels of Expression of Cartilage Oligomeric Matrix Protein in Lymph Node Metastases in Breast Cancer Are Associated with Reduced Survival

 ,
, 
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
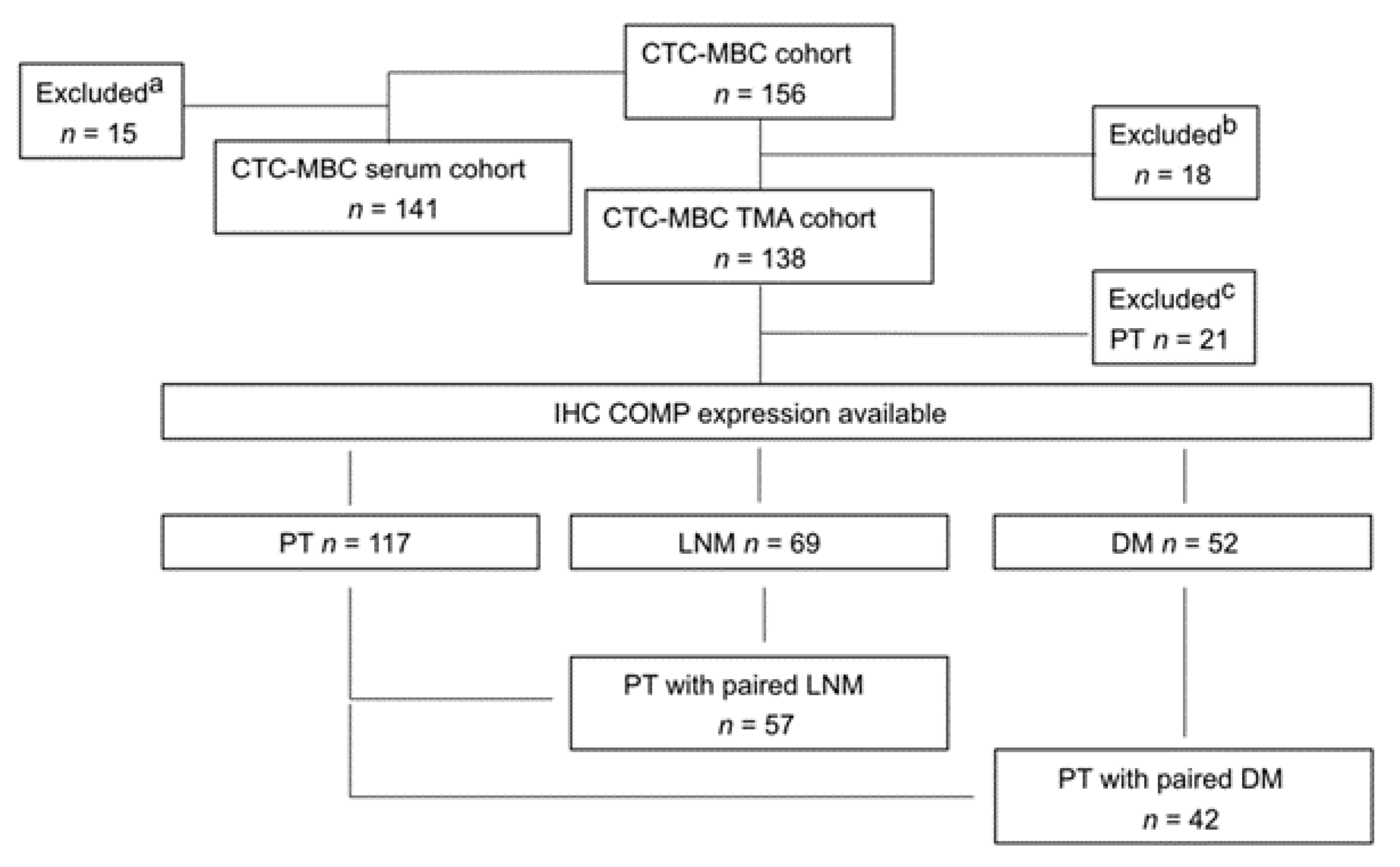
2.1. Cohort Description
2.2. Determination of COMP Levels in Sera (S-COMP)
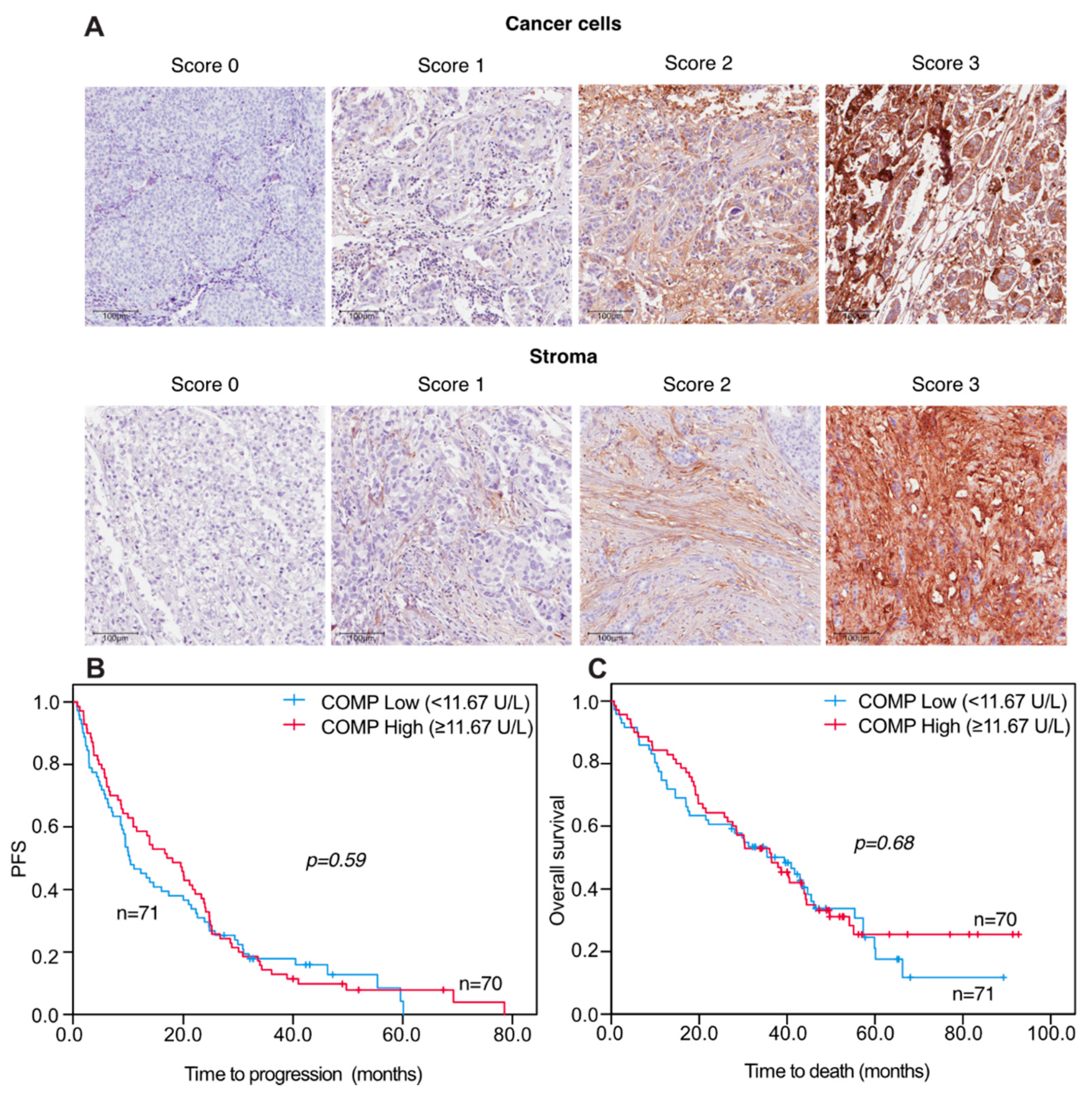
2.3. Immunohistochemical (IHC) Detection of COMP in Tumor Tissues
2.4. Statistical Analyses
3. Results
3.1. Serum COMP Levels in Patients with Metastatic Breast Cancer and Associations to Clinicopathological Variables
3.2. Progression-Free and Overall Survival in Correlation to S-COMP Levels
3.3. Correlations of S-COMP Levels and Comp IHC Expression in Distant Metastases
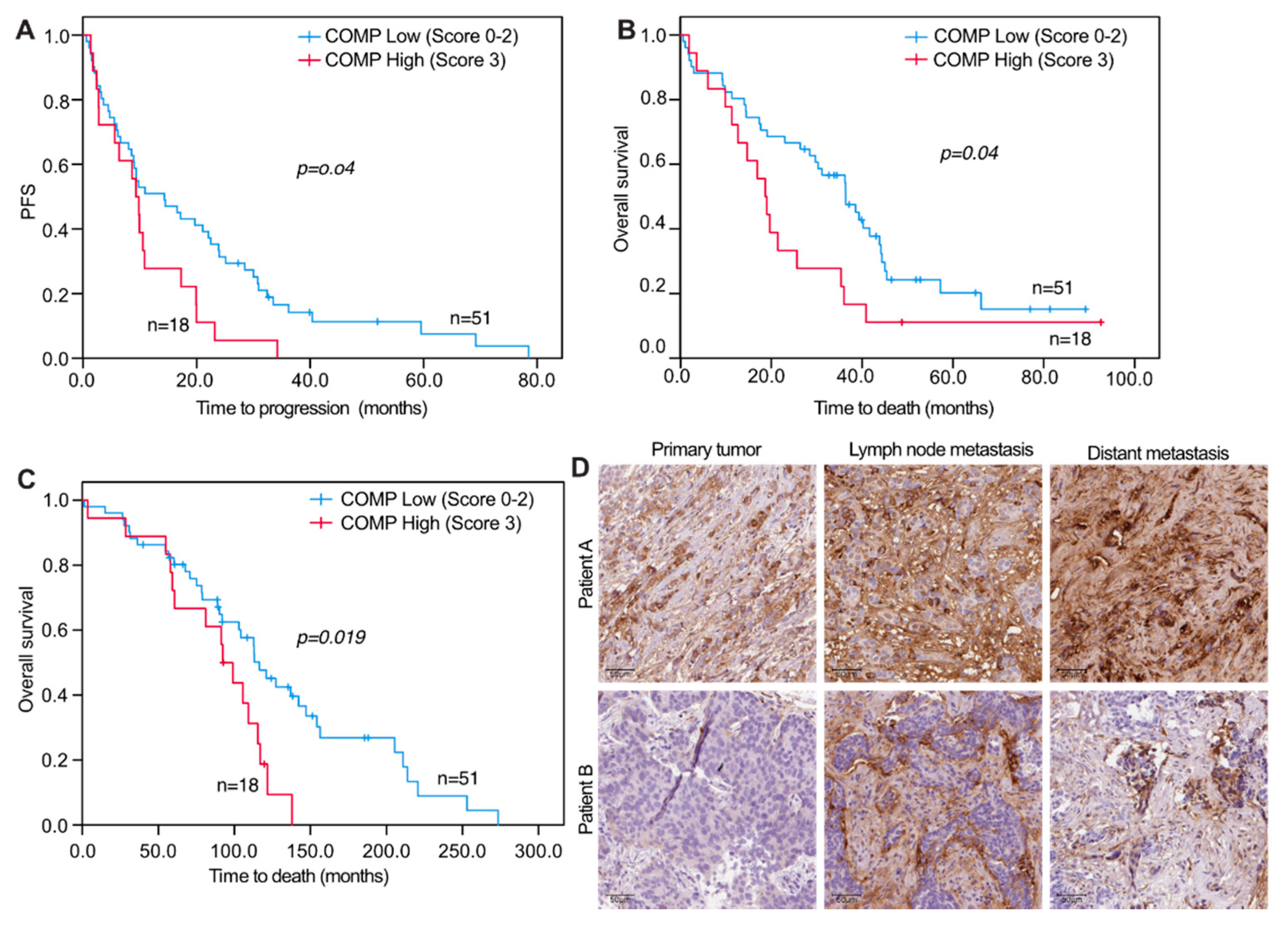
3.4. Concordance and Discordance of IHC COMP Expression in Matched Samples of Primary Tumors, Lymph Node Metastases, and Distant Metastases
3.5. COMP IHC Expression and Correlations to Clinicopathological Variables
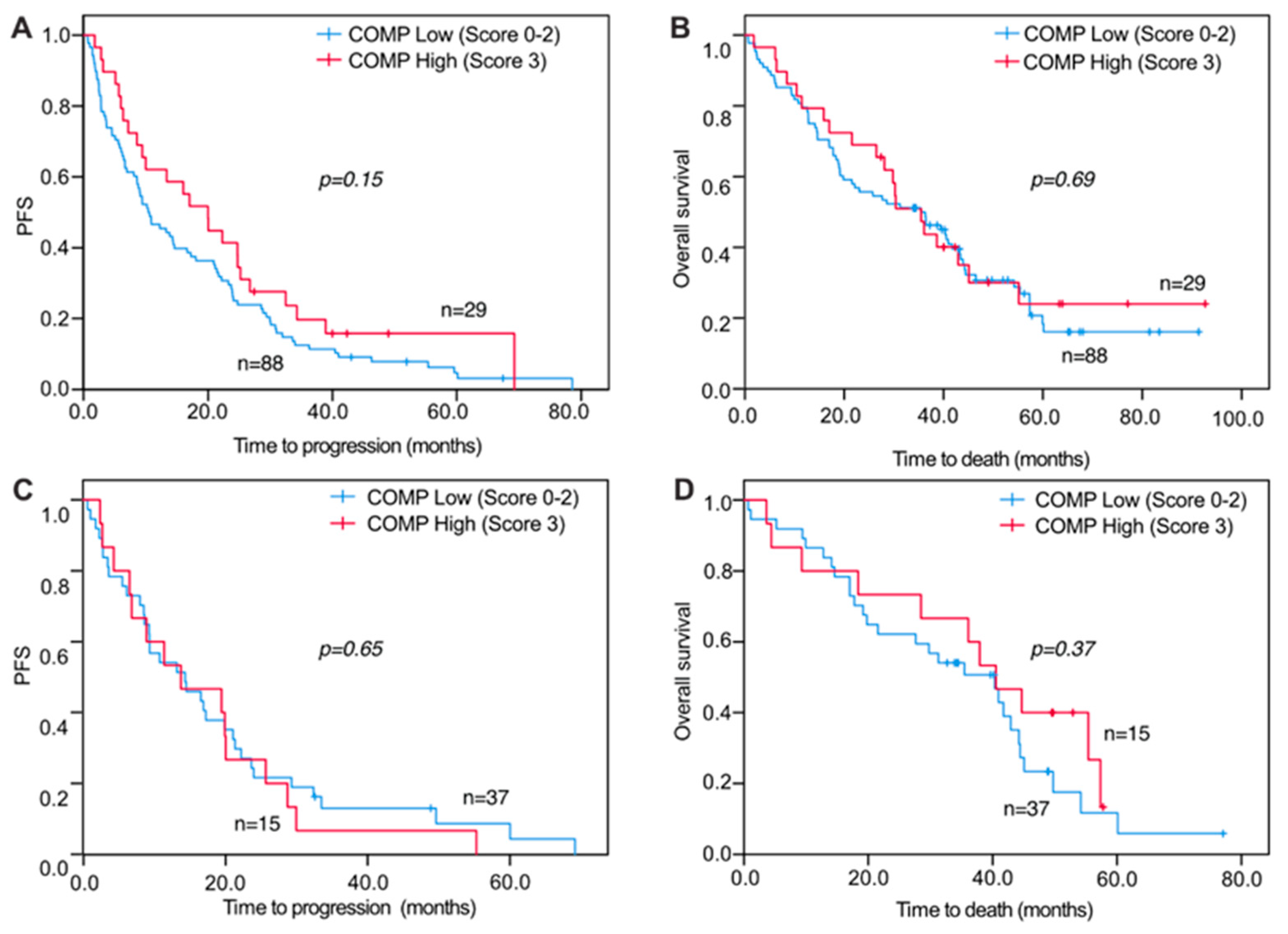
3.6. COMP IHC Expression in Relation to Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heinegård, D. Fell-Muir Lecture: Proteoglycans and more-from molecules to biology. Int. J. Exp. Pathol. 2009, 90, 575–586. [Google Scholar] [CrossRef]
- Agarwal, P.; Schulz, J.-N.; Blumbach, K.; Andreasson, K.; Heinegård, D.; Paulsson, M.; Mauch, C.; Eming, S.A.; Eckes, B.; Krieg, T. Enhanced deposition of cartilage oligomeric matrix protein is a common feature in fibrotic skin pathologies. Matrix Biol. 2013, 32, 325–331. [Google Scholar] [CrossRef]
- Acharya, C.; Yik, J.H.; Kishore, A.; Van Dinh, V.; Di Cesare, P.E.; Haudenschild, D. Cartilage oligomeric matrix protein and its binding partners in the cartilage extracellular matrix: Interaction, regulation and role in chondrogenesis. Matrix Biol. 2014, 37, 102–111. [Google Scholar] [CrossRef]
- Adams, J.C.; Lawler, J. The thrombospondins. Cold Spring Harb. Perspect. Biol. 2011, 3, a009712. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, X.; Kong, W. ADAMTS-7, a novel proteolytic culprit in vascular remodeling. Sheng Li Xue Bao [Acta Physiol. Sin.] 2010, 62, 285–294. [Google Scholar]
- Riessen, R.; Fenchel, M.; Chen, H.; Axel, D.I.; Karsch, K.R.; Lawler, J. Cartilage oligomeric matrix protein (Thrombospondin-5) is expressed by human vascular smooth muscle cells. Arter. Thromb. Vasc. Biol. 2001, 21, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hultman, K.; Edsfeldt, A.; Björkbacka, H.; Dunér, P.; Sundius, L.; Nitulescu, M.; Persson, A.; Boyle, J.J.; Nilsson, J.; Hultgårdh-Nilsson, A.; et al. Cartilage oligomeric matrix protein associates with a vulnerable plaque phenotype in human atherosclerotic plaques. Stroke 2019, 50, 3289–3292. [Google Scholar] [CrossRef]
- Liang, Y.; Fu, Y.; Qi, R.; Wang, M.; Yang, N.; He, L.; Yu, F.; Zhang, J.; Yun, C.-H.; Wang, X.; et al. Cartilage oligomeric matrix protein is a natural inhibitor of thrombin. Blood 2015, 126, 905–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Happonen, K.E.; Saxne, T.; Aspberg, A.; Mörgelin, M.; Heinegård, D.; Blom, A.M. Regulation of complement by cartilage oligomeric matrix protein allows for a novel molecular diagnostic principle in rheumatoid arthritis. Arthritis Rheum. 2010, 62, 3574–3583. [Google Scholar] [CrossRef] [Green Version]
- Happonen, K.E.; Saxne, T.; Geborek, P.; Andersson, M.; A Bengtsson, A.; Hesselstrand, R.; Heinegård, D.; Blom, A.M. Serum COMP-C3b complexes in rheumatic diseases and relation to anti-TNF-α treatment. Arthritis Res. Ther. 2012, 14, R15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Englund, E.; Bartoschek, M.; Reitsma, B.; Jacobsson, L.; Escudero-Esparza, A.; Orimo, A.; Leandersson, K.; Hagerling, C.; Aspberg, A.; Storm, P.; et al. Cartilage oligomeric matrix protein contributes to the development and metastasis of breast cancer. Oncogene 2016, 35, 5585–5596. [Google Scholar] [CrossRef]
- Englund, E.; Canesin, G.; Papadakos, K.S.; Vishnu, N.; Persson, E.; Reitsma, B.; Anand, A.; Jacobsson, L.; Helczynski, L.; Mulder, H.; et al. Cartilage oligomeric matrix protein promotes prostate cancer progression by enhancing invasion and disrupting intracellular calcium homeostasis. Oncotarget 2017, 8, 98298–98311. [Google Scholar] [CrossRef]
- Liu, T.-T.; Liu, X.-S.; Zhang, M.; Liu, X.-N.; Zhu, F.-X.; Zhu, F.-M.; Ouyang, S.-W.; Li, S.-B.; Song, C.-L.; Sun, H.-M.; et al. Cartilage oligomeric matrix protein is a prognostic factor and biomarker of colon cancer and promotes cell proliferation by activating the Akt pathway. J. Cancer Res. Clin. Oncol. 2018, 144, 1049–1063. [Google Scholar] [CrossRef]
- Nfonsam, V.N.; Jecius, H.C.; Janda, J.; Omesiete, P.N.; Elquza, E.; Scott, A.J.; Nfonsam, L.E.; Jandova, J. Cartilage oligomeric matrix protein (COMP) promotes cell proliferation in early-onset colon cancer tumorigenesis. Surg. Endosc. 2019, 34, 3992–3998. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wang, C.; Wang, Y.; Sun, L.; Liu, Z.; Wang, L.; Song, T.; Yao, Y.; Liu, Q.; Tu, K. HSCs-derived COMP drives hepatocellular carcinoma progression by activating MEK/ERK and PI3K/AKT signaling pathways. J. Exp. Clin. Cancer Res. 2018, 37, 231. [Google Scholar] [CrossRef]
- Papadakos, K.; Darlix, A.; Jacot, W.; Blom, A.M. High levels of cartilage oligomeric matrix protein in the serum of breast cancer patients can serve as an independent prognostic marker. Front. Oncol. 2019, 9, 1141. [Google Scholar] [CrossRef]
- Papadakos, K.; Bartoschek, M.; Rodriguez, C.; Gialeli, C.; Jin, S.-B.; Lendahl, U.; Pietras, K.; Blom, A.M. Cartilage oligomeric matrix protein initiates cancer stem cells through activation of Jagged1-Notch3 signaling. Matrix Biol. 2019, 81, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.-M.; Jansson, S.; Bendahl, P.-O.; Jörgensen, C.L.T.; Loman, N.; Graffman, C.; Lundgren, L.; Aaltonen, K.; Rydén, L. Longitudinal enumeration and cluster evaluation of circulating tumor cells improve prognostication for patients with newly diagnosed metastatic breast cancer in a prospective observational trial. Breast Cancer Res. 2018, 20, 48. [Google Scholar] [CrossRef]
- Saxne, T.; Heinegård, D. Cartilage oligomeric matrix protein: A novel marker of cartilage turnover detectable in synovial fluid and blood. Rheumatology 1992, 31, 583–591. [Google Scholar] [CrossRef]
- Forslind, K.; Eberhardt, K.; Jonsson, A.; Saxne, T. Increased serum concentrations of cartilage oligomeric matrix protein. A prognostic marker in early rheumatoid arthritis. Rheumatology 1992, 31, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Mündermann, A.; Dyrby, C.O.; Andriacchi, T.P.; King, K.B. Serum concentration of cartilage oligomeric matrix protein (COMP) is sensitive to physiological cyclic loading in healthy adults. Osteoarthr. Cartil. 2005, 13, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.; André, F.; Barrios, C.; Bergh, J.; Bhattacharyya, G.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H.; et al. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef] [Green Version]
- Zhong, W.; Hou, H.; Liu, T.; Su, S.; Xi, X.; Liao, Y.; Xie, R.; Jin, G.; Liu, X.; Zhu, L.; et al. Cartilage oligomeric matrix protein promotes epithelial-mesenchymal transition by interacting with Transgelin in Colorectal Cancer. Theranostics 2020, 10, 8790–8806. [Google Scholar] [CrossRef] [PubMed]
- Posey, K.L.; Coustry, F.; Hecht, J.T. Cartilage oligomeric matrix protein: COMPopathies and beyond. Matrix Biol. 2018, 71–72, 161–173. [Google Scholar] [CrossRef]
- Rosenberg, K.; Olsson, H.; Mörgelin, M.; Heinegård, D. Cartilage oligomeric matrix protein shows high affinity zinc-dependent interaction with triple helical collagen. J. Biol. Chem. 1998, 273, 20397–20403. [Google Scholar] [CrossRef] [Green Version]
- Dicesare, P.; Hauser, N.; Lehman, D.; Pasumarti, S.; Paulsson, M. Cartilage oligomeric matrix protein (COMP) is an abundant component of tendon. FEBS Lett. 1994, 354, 237–240. [Google Scholar] [CrossRef] [Green Version]
- Rizwan, A.; Bulte, C.; Kalaichelvan, A.; Cheng, M.; Krishnamachary, B.; Bhujwalla, Z.M.; Jiang, L.; Glunde, K. Metastatic breast cancer cells in lymph nodes increase nodal collagen density. Sci. Rep. 2015, 5, 10002. [Google Scholar] [CrossRef] [Green Version]
- Tian, C.; Clauser, K.; Öhlund, D.; Rickelt, S.; Huang, Y.; Gupta, M.; Mani, D.R.; Carr, S.A.; Tuveson, D.A.; Hynes, R.O. Proteomic analyses of ECM during pancreatic ductal adenocarcinoma progression reveal different contributions by tumor and stromal cells. Proc. Natl. Acad. Sci. USA 2019, 116, 19609–19618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, C.; Öhlund, D.; Rickelt, S.; Lidström, T.; Huang, Y.; Hao, L.; Zhao, R.T.; Franklin, O.; Bhatia, S.N.; Tuveson, D.A.; et al. Cancer cell–derived matrisome proteins promote metastasis in pancreatic ductal adenocarcinoma. Cancer Res. 2020, 80, 1461–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients, n = 141 | BL COMP Levels Low (<11.67), n = 71 | BL COMP Levels High (≥11.67), n = 70 | p-Value |
|---|---|---|---|---|
| Age at MBC diagnosis | ||||
| <65 years | 67 | 40 | 27 | 0.04 c |
| ≥65 years | 74 | 31 | 43 | |
| Metastasis-free interval (years) | ||||
| 0 | 29 | 9 | 20 | 0.03 c |
| >0–3 | 26 | 20 | 6 | |
| >3 | 86 | 42 | 44 | |
| BL ECOG | ||||
| 0 | 79 | 46 | 33 | 0.10 b |
| 1 | 36 | 13 | 23 | |
| 2 | 22 | 10 | 12 | |
| Unknown | 4 | 2 | 2 | |
| PT hist subtype | ||||
| Ductal | 104 | 57 | 47 | 0.01 c |
| Lobular | 26 | 7 | 19 | |
| Unknown | 11 | 7 | 4 | |
| PT NHG | ||||
| I | 12 | 9 | 3 | 0.41 b |
| II | 59 | 24 | 35 | |
| III | 42 | 28 | 14 | |
| Unknown | 28 | 10 | 18 | |
| PT T (size) | ||||
| T1 | 50 | 30 | 20 | 0.17 b |
| T2 | 47 | 19 | 28 | |
| T3 | 18 | 13 | 5 | |
| T4 | 17 | 5 | 12 | |
| Unknown | 9 | 4 | 5 | |
| PT node status | ||||
| Neg | 41 | 26 | 15 | 0.13 c |
| Pos | 80 | 39 | 41 | |
| Unknown | 20 | 6 | 14 | |
| Breast cancer subtype a | ||||
| ER+HER2− | 98 | 46 | 52 | 0.04 b |
| HER2+ | 15 | 4 | 11 | |
| ER−HER2− | 25 | 19 | 6 | |
| Unknown | 3 | 1 | 2 | |
| No of metastatic sites | ||||
| <3 | 99 | 49 | 50 | 0.75 c |
| ≥3 | 42 | 22 | 20 | |
| Bone metastasis | ||||
| Yes | 98 | 42 | 56 | 0.007 c |
| No | 43 | 29 | 14 | |
| Liver metastasis | ||||
| Yes | 39 | 19 | 20 | 0.81 c |
| No | 102 | 52 | 50 | |
| Lung metastasis | ||||
| Yes | 46 | 31 | 15 | 0.005 c |
| No | 95 | 40 | 55 | |
| Visceral metastasis d | ||||
| Yes | 83 | 43 | 40 | 0.68 c |
| No | 58 | 28 | 30 | |
| Treatment | ||||
| Chemotherapy | 64 | 30 | 34 | 0.03 c |
| Endocrine therapy | 58 | 38 | 20 | |
| HER2-directed therapy | 13 | 4 | 9 | |
| CTC count | ||||
| <5 | 67 | 44 | 23 | <0.001 c |
| ≥5 | 72 | 26 | 46 | |
| unknown | 2 | |||
| CTC-cluster | ||||
| Yes | 13 | 1 | 12 | 0.001 c |
| No | 126 | 69 | 57 | |
| Unknown | 2 | 1 | 1 | |
| COMP score cancer cells (IHC) | ||||
| 0 | 17 | 9 | 8 | 0.13 b |
| 1 | 14 | 7 | 7 | |
| 2 | 9 | 1 | 8 | |
| 3 | 11 | 3 | 8 | |
| Unknown | 90 | 51 | 39 | |
| COMP score stroma (IHC) | ||||
| 0 | 4 | 4 | 0 | 0.01 b |
| 1 | 17 | 9 | 8 | |
| 2 | 17 | 3 | 14 | |
| 3 | 13 | 4 | 9 | |
| Unknown | 90 | 51 | 39 |
| Location | COMP Expression in Cancer Cells N (%) | p | COMP Expression in Stroma N (%) | p |
|---|---|---|---|---|
| PT+/LNM+ | 27 (47) | 0.08 | 33 (58) | 0.049 |
| PT+/LNM− | 12 (21) | 13 (23) | ||
| PT−/LNM+ | 4 (7) | 4 (7) | ||
| PT−/LNM− | 14 (25) | 7 (12) | ||
| Total | 57 (100) | 57 (100) | ||
| PT+/DM+ | 23 (55) | 0.77 | 32 (76) | 0.51 |
| PT+/DM− | 7 (17) | 3 (7) | ||
| PT−/DM+ | 5 (12) | 6 (14) | ||
| PT−/DM− | 7 (17) | 1 (2) | ||
| Total | 42 (100) | 42 (100) | ||
| LNM+/DM+ | 6 (23) | 0.80 | 18 (69) | 0.13 |
| LNM+/DM− | 7 (27%) | 1 (4) | ||
| LNM−/DM+ | 9 (35) | 6 (23) | ||
| LNM−/DM− | 4 (15) | 1 (4) | ||
| Total | 26 | 26 |
| COMP PT Cancer Cells | COMP PT Stroma | COMP LNM Cancer Cells | COMP LNM Stroma | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | 0 | 1 | 2 | 3 | p | 0 | 1 | 2 | 3 | p | 0 | 1 | 2 | 3 | p | 0 | 1 | 2 | 3 | p |
| Age <65 >65 | 24 | 14 | 14 | 6 | 0.005 | 11 | 15 | 22 | 10 | 0.15 | 13 | 6 | 4 | 5 | 0.39 | 12 | 3 | 11 | 2 | 0.13 |
| 13 | 11 | 21 | 14 | 7 | 14 | 22 | 16 | 16 | 8 | 6 | 11 | 10 | 9 | 13 | 9 | |||||
| ECOG 0 1 2 | 23 | 15 | 22 | 7 | 0.10 | 11 | 17 | 26 | 13 | 0.41 | 20 | 10 | 4 | 10 | 0.09 | 17 | 7 | 14 | 6 | 0.02 |
| 8 | 7 | 9 | 7 | 4 | 9 | 11 | 7 | 6 | 3 | 4 | 3 | 4 | 4 | 5 | 3 | |||||
| 5 | 3 | 4 | 6 | 3 | 3 | 6 | 6 | 1 | 1 | 2 | 3 | 0 | 0 | 5 | 2 | |||||
| MFI 0years 0–3years >3years | 4 | 3 | 9 | 7 | 0.22 | 0 | 2 | 12 | 9 | 0.007 | 1 | 2 | 1 | 2 | 0.75 | 1 | 0 | 3 | 2 | 0.31 |
| 12 | 5 | 4 | 2 | 5 | 7 | 8 | 3 | 6 | 4 | 3 | 1 | 5 | 3 | 4 | 2 | |||||
| 21 | 17 | 22 | 11 | 13 | 20 | 24 | 14 | 22 | 8 | 6 | 13 | 16 | 9 | 17 | 7 | |||||
| Subtype ductal | 25 | 21 | 23 | 16 | 0.78 | 12 | 20 | 31 | 22 | 0.50 | 17 | 11 | 5 | 13 | 0.51 | 12 | 7 | 19 | 8 | 0.28 |
| lobular | 7 | 3 | 7 | 3 | 4 | 6 | 8 | 2 | 10 | 2 | 3 | 2 | 8 | 5 | 3 | 1 | ||||
| other | 4 | 1 | 5 | 1 | 1 | 3 | 5 | 2 | 2 | 0 | 2 | 1 | 2 | 0 | 1 | 2 | ||||
| PT T1 | 13 | 8 | 13 | 4 | 0.84 | 6 | 10 | 14 | 8 | 0.90 | 9 | 2 | 2 | 3 | 0.81 | 6 | 3 | 3 | 4 | 0.37 |
| T2 | 7 | 10 | 13 | 11 | 5 | 10 | 15 | 11 | 9 | 6 | 6 | 8 | 4 | 8 | 12 | 5 | ||||
| T3 | 10 | 3 | 5 | 0 | 6 | 3 | 8 | 1 | 7 | 2 | 1 | 3 | 7 | 1 | 5 | 0 | ||||
| T4 | 5 | 3 | 2 | 5 | 1 | 4 | 5 | 5 | 3 | 2 | 1 | 2 | 4 | 0 | 2 | 2 | ||||
| Node neg Node pos | 10 | 8 | 9 | 4 | 0.87 | 5 | 9 | 10 | 7 | 0.84 | x | x | x | X | X | x | x | x | X | x |
| 24 | 16 | 21 | 11 | 13 | 19 | 26 | 14 | x | x | x | x | x | x | x | x | |||||
| NHG I II III | 5 | 0 | 3 | 0 | 0.44 | 2 | 1 | 3 | 2 | 0.68 | 4 | 0 | 1 | 0 | 0.12 | 2 | 2 | 1 | 0 | 0.31 |
| 14 | 11 | 15 | 7 | 5 | 15 | 19 | 8 | 17 | 5 | 6 | 10 | 11 | 8 | 13 | 6 | |||||
| 13 | 8 | 12 | 6 | 8 | 10 | 13 | 8 | 4 | 7 | 3 | 5 | 6 | 2 | 7 | 4 | |||||
| PT ER- ER+ | 7 | 6 | 4 | 2 | 0.25 | 3 | 6 | 6 | 4 | 0.67 | 3 | 2 | 0 | 2 | 0.84 | 2 | 1 | 2 | 2 | 0.56 |
| 30 | 17 | 31 | 17 | 15 | 21 | 38 | 21 | 24 | 10 | 10 | 16 | 19 | 11 | 19 | 9 | |||||
| PT HER2- HER2+ | 30 | 16 | 26 | 14 | 15 | 22 | 31 | 18 | 18 | 9 | 6 | 12 | 14 | 10 | 14 | 7 | ||||
| 1 | 3 | 4 | 3 | 0 | 1 | 6 | 4 | 1 | 3 | 3 | 1 | 2 | 0 | 5 | 1 | |||||
| Mets <3 >=3 | 24 | 21 | 22 | 10 | 0.21 | 10 | 22 | 32 | 13 | 0.51 | 21 | 9 | 8 | 9 | 0.41 | 16 | 10 | 12 | 9 | 0.58 |
| 13 | 4 | 13 | 10 | 8 | 7 | 12 | 13 | 8 | 5 | 2 | 7 | 6 | 2 | 12 | 2 | |||||
| CTC <5 >=5 | 15 | 14 | 15 | 10 | 0.68 | 8 | 11 | 20 | 15 | 0.26 | 13 | 7 | 3 | 5 | 0.28 | 9 | 4 | 11 | 4 | 0.91 |
| 22 | 11 | 20 | 10 | 10 | 18 | 24 | 11 | 16 | 6 | 7 | 11 | 13 | 8 | 12 | 7 | |||||
| Cluster neg | 29 | 21 | 28 | 18 | 0.40 | 14 | 24 | 36 | 22 | 0.63 | 21 | 12 | 6 | 11 | 0.56 | 15 | 10 | 17 | 8 | 0.79 |
| pos | 8 | 4 | 7 | 2 | 4 | 5 | 8 | 4 | 8 | 1 | 4 | 5 | 7 | 2 | 6 | 3 | ||||
| Visc no | 19 | 11 | 13 | 6 | 0.09 | 9 | 15 | 18 | 7 | 0.07 | 14 | 7 | 1 | 6 | 0.21 | 12 | 8 | 4 | 4 | 0.03 |
| yes | 18 | 14 | 22 | 14 | 9 | 14 | 26 | 19 | 15 | 7 | 9 | 10 | 10 | 4 | 20 | 7 | ||||
| Bone-only no | 27 | 19 | 29 | 15 | 0.58 | 15 | 18 | 35 | 22 | 0.38 | 23 | 10 | 9 | 12 | 0.97 | 18 | 7 | 21 | 8 | 0.95 |
| yes | 10 | 6 | 6 | 5 | 3 | 11 | 9 | 4 | 6 | 4 | 1 | 4 | 4 | 5 | 3 | 3 | ||||
| Lung met no | 26 | 19 | 23 | 12 | 0.37 | 11 | 21 | 33 | 15 | 0.79 | 23 | 10 | 7 | 10 | 0.23 | 19 | 11 | 12 | 8 | 0.04 |
| yes | 11 | 6 | 12 | 8 | 7 | 8 | 11 | 11 | 6 | 4 | 3 | 6 | 3 | 1 | 12 | 3 | ||||
| Liver mets no | 31 | 19 | 23 | 11 | 0.01 | 15 | 26 | 27 | 16 | 0.01 | 23 | 12 | 4 | 10 | 0.07 | 17 | 10 | 17 | 5 | 0.09 |
| yes | 6 | 6 | 12 | 9 | 3 | 3 | 17 | 10 | 6 | 2 | 6 | 6 | 5 | 2 | 7 | 6 | ||||
| Bone mets no | 16 | 8 | 11 | 5 | 0.16 | 9 | 6 | 17 | 8 | 0.60 | 9 | 5 | 6 | 3 | 0.78 | 8 | 3 | 7 | 5 | 0.82 |
| yes | 21 | 17 | 24 | 15 | 9 | 23 | 27 | 18 | 20 | 9 | 4 | 13 | 14 | 9 | 17 | 6 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadakos, K.S.; Hagerling, C.; Rydén, L.; Larsson, A.-M.; Blom, A.M. High Levels of Expression of Cartilage Oligomeric Matrix Protein in Lymph Node Metastases in Breast Cancer Are Associated with Reduced Survival. Cancers 2021, 13, 5876. https://doi.org/10.3390/cancers13235876
Papadakos KS, Hagerling C, Rydén L, Larsson A-M, Blom AM. High Levels of Expression of Cartilage Oligomeric Matrix Protein in Lymph Node Metastases in Breast Cancer Are Associated with Reduced Survival. Cancers. 2021; 13(23):5876. https://doi.org/10.3390/cancers13235876
Chicago/Turabian StylePapadakos, Konstantinos S., Catharina Hagerling, Lisa Rydén, Anna-Maria Larsson, and Anna M. Blom. 2021. "High Levels of Expression of Cartilage Oligomeric Matrix Protein in Lymph Node Metastases in Breast Cancer Are Associated with Reduced Survival" Cancers 13, no. 23: 5876. https://doi.org/10.3390/cancers13235876
APA StylePapadakos, K. S., Hagerling, C., Rydén, L., Larsson, A.-M., & Blom, A. M. (2021). High Levels of Expression of Cartilage Oligomeric Matrix Protein in Lymph Node Metastases in Breast Cancer Are Associated with Reduced Survival. Cancers, 13(23), 5876. https://doi.org/10.3390/cancers13235876