
From Focused Ultrasound Tumor Ablation to Brain Blood Barrier Opening for High Grade Glioma: A Systematic Review

 , ,
, ,  ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
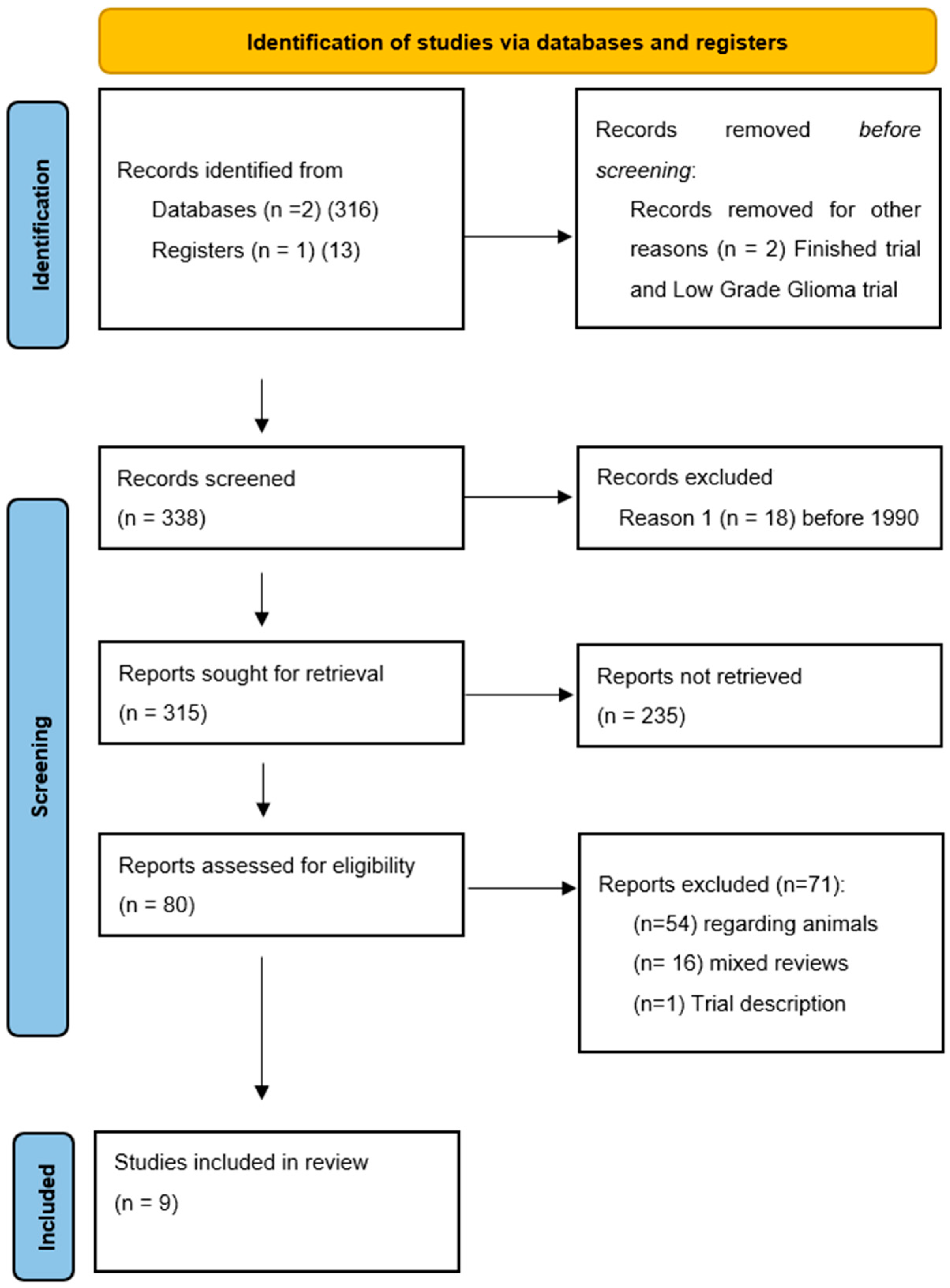
2. Materials and Methods
Search Strategy, Inclusion Criteria, and Study Selection
3. Results
3.1. Patient Characteristics
3.2. FUS Devices for Direct Tumor Ablation
3.3. FUS Devices for BBB Opening
3.4. FUS for Tumor Ablation
3.5. FUS-Mediated BBB Opening
3.6. Ongoing Clinical Trials
4. Discussion
4.1. FUS Direct Tumor Ablation
4.2. FUS-Mediated BBB Opening
4.3. Ongoing Trials and Future Perspectives
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| HGG | High-grade glioma |
| FUS | Focused Ultrasound |
| BBB | Blood-Brain Barrier |
| US | Ultrasound |
| 5-ALA | 5-Aminolevulinic Acid |
| MRI | Magnetic Resonance Imaging |
| TMZ | Temozolomide |
| KPS | Karnofsky Performance Status |
| CT | Computed Tomography |
| RT | Radiotherapy |
| H | Hematoma |
| TND | Transient Neurological Deficit |
| NL | New Lesion |
| NA | Not Assessed |
| IV | Intravenous |
| GBM | Glioblastoma |
| AA | Anaplastic Astrocytoma |
| PFS | Progression-Free Survival |
| OS | Overall Survival |
| DLT | Dose Limiting Toxicity |
| RT | Radiotherapy |
References
- Briquard, P. Paul langevin. Ultrasonics 1972, 10, 213–214. [Google Scholar] [CrossRef] [PubMed]
- Van Tiggelen, R.; Pouders, E. Ultrasound and computed tomography: Spin-offs of the world wars. JBR-BTR 2003, 86, 235–241. [Google Scholar] [PubMed]
- Gersten, J.W.; Kawashima, E. Recent advances in fundamental aspects of ultrasound and muscle. Br. J. Phys. Med. 1955, 18, 106–109. [Google Scholar] [PubMed]
- Gersten, J.W. Relation of ultrasound effects to the orientation of tendon in the ultrasound field. Arch. Phys. Med. Rehabil. 1956, 37, 201–209. [Google Scholar]
- Lynn, J.G.; Zwemer, R.L.; Chick, A.J.; Miller, A.E. A new method for the generation and use of focused ultrasound in experimental biology. J. Gen. Physiol. 1942, 26, 179–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fry, W.J.; Meyers, R. Ultrasonic method of modifying brain structures. Stereotact. Funct. Neurosurg. 1962, 22, 315–327. [Google Scholar] [CrossRef]
- Fry, W.J.; Mosberg, W.H.; Barnard, J.W.; Fry, F.J. Production of focal destructive lesions in the central nervous system with ultrasound. J. Neurosurg. 1954, 11, 471–478. [Google Scholar] [CrossRef]
- Vallancien, G.; Harouni, M.; Veillon, B.; Mombet, A.; Prapotnich, D.; Brisset, J.M.; Bougaran, J. Focused extracorporeal pyrotherapy: Feasibility study in man. J. Endourol. 1992, 6, 173–181. [Google Scholar] [CrossRef]
- Visioli, A.; Rivens, I.; ter Haar, G.; Horwich, A.; Huddart, R.; Moskovic, E.; Padhani, A.; Glees, J. Preliminary results of a phase I dose escalation clinical trial using focused ultrasound in the treatment of localised tumours. Eur. J. Ultrasound 1999, 9, 11–18. [Google Scholar] [CrossRef]
- Moiraghi, A.; Pallud, J. Intraoperative ultrasound techniques for cerebral gliomas resection: Usefulness and pitfalls. Ann. Transl. Med. 2020, 8, 523. [Google Scholar] [CrossRef]
- Moiraghi, A.; Prada, F.; Delaidelli, A.; Guatta, R.; May, A.; Bartoli, A.; Saini, M.; Perin, A.; Walchli, T.; Momjian, S.; et al. Navigated intraoperative 2-dimensional ultrasound in high-grade glioma surgery: Impact on extent of resection and patient outcome. Oper. Neurosurg. 2020, 18, 363–373. [Google Scholar] [CrossRef] [Green Version]
- Prada, F.; Del Bene, M.; Moiraghi, A.; DiMeco, F. Echographic brain semeiology and topographic anatomy according to surgical approaches. In Intraoperative Ultrasound (IOUS) in Neurosurgery; Springer: Berlin, Germany, 2016; ISBN 9783319252681. [Google Scholar]
- Prada, F.; Vitale, V.; Del Bene, M.; Boffano, C.; Sconfienza, L.M.; Pinzi, V.; Mauri, G.; Solbiati, L.; Sakas, G.; Kolev, V.; et al. Contrast-enhanced MR Imaging versus Contrast-enhanced US: A comparison in glioblastoma surgery by using intraoperative fusion imaging. Radiology 2017, 285, 242–249. [Google Scholar] [CrossRef] [Green Version]
- Unsgaard, G.; Gronningsaeter, A.; Ommedal, S.; Hernes, T.A.N. Brain operations guided by real-time two-result of improved image quality. Neurosurgery 2002, 51, 402–412. [Google Scholar] [CrossRef] [PubMed]
- Incekara, F.; Smits, M.; Dirven, L.; Bos, E.M.; Balvers, R.K.; Haitsma, I.K.; Schouten, J.W.; Vincent, A.J.P.E. Intraoperative B-mode ultrasound guided surgery and the extent of glioblastoma resection: A randomized controlled trial. Front. Oncol. 2021, 11, 649797. [Google Scholar] [CrossRef] [PubMed]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.J. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Senft, C.; Bink, A.; Franz, K.; Vatter, H.; Gasser, T.; Seifert, V. Intraoperative MRI guidance and extent of resection in glioma surgery: A randomised, controlled trial. Lancet Oncol. 2011, 12, 997–1003. [Google Scholar] [CrossRef]
- Moiraghi, A.; Roux, A.; Peeters, S.; Pelletier, J.B.; Baroud, M.; Trancart, B.; Oppenheim, C.; Lechapt, E.; Benevello, C.; Parraga, E.; et al. Feasibility, safety and impact on overall survival of awake resection for newly diagnosed supratentorial IDH-wildtype glioblastomas in adults. Cancers 2021, 13, 2911. [Google Scholar] [CrossRef]
- Pallud, J.; Zanello, M.; Moiraghi, A.; Peeters, S.; Trancart, B.; Edjlali, M.; Oppenheim, C.; Varlet, P.; Chrétien, F.; Dhermain, F.; et al. Surgery of insular diffuse gliomas-part 1: Transcortical awake resection is safe and independently improves overall survival. Neurosurgery 2021, 89, 565–578. [Google Scholar] [CrossRef]
- Pallud, J.; Roux, A.; Trancart, B.; Peeters, S.; Moiraghi, A.; Edjlali, M.; Oppenheim, C.; Varlet, P.; Chrétien, F.; Dhermain, F.; et al. Surgery of insular diffuse gliomas-part 2: Probabilistic cortico-subcortical atlas of critical eloquent brain structures and probabilistic resection map during transcortical awake resection. Neurosurgery 2021, 89, 579–590. [Google Scholar] [CrossRef]
- Raabe, A.; Beck, J.; Schucht, P.; Seidel, K. Continuous dynamic mapping of the corticospinal tract during surgery of motor eloquent brain tumors: Evaluation of a new method: Clinical article. J. Neurosurg. 2014, 120, 1015–1024. [Google Scholar] [CrossRef]
- Boex, C.; Haemmerli, J.; Momjian, S.; Schaller, K. Prognostic values of motor evoked potentials in insular, precental, or postcentral resections. J. Clin. Neurophysiol. 2016, 33, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Boëx, C.; Goga, C.; Bérard, N.; Al Awadhi, A.; Bartoli, A.; Meling, T.; Bijlenga, P.; Schaller, K. Intraoperative subcortico-cortical evoked potentials of the visual pathway under general anesthesia. Clin. Neurophysiol. 2021, 132, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Bond, A.E.; Dallapiazza, R.; Huss, D.; Warren, A.L.; Sperling, S.; Gwinn, R.; Shah, B.B.; Elias, W.J. A randomized, sham-controlled trial of transcranial magnetic resonance-guided focused ultrasound thalamotomy trial for the treatment of tremor-dominant, idiopathic Parkinson disease. Neurosurgery 2016, 63, 154. [Google Scholar] [CrossRef]
- Elias, W.J.; Lipsman, N.; Ondo, W.G.; Ghanouni, P.; Kim, Y.G.; Lee, W.; Schwartz, M.; Hynynen, K.; Lozano, A.M.; Shah, B.B.; et al. A randomized trial of focused ultrasound thalamotomy for essential tremor. N. Engl. J. Med. 2016, 375, 730–739. [Google Scholar] [CrossRef]
- Meng, Y.; Suppiah, S.; Mithani, K.; Solomon, B.; Schwartz, M.L.; Lipsman, N. Current and emerging brain applications of MR-guided focused ultrasound. J. Ther. Ultrasound 2017, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.R.; Dallapiazza, R.; Jeff Elias, W. Neurological applications of transcranial high intensity focused ultrasound. Int. J. Hyperth. 2015, 31, 285–291. [Google Scholar] [CrossRef]
- Tufail, Y.; Matyushov, A.; Baldwin, N.; Tauchmann, M.L.; Georges, J.; Yoshihiro, A.; Tillery, S.I.H.; Tyler, W.J. Transcranial pulsed ultrasound stimulates intact brain circuits. Neuron 2010, 66, 681–694. [Google Scholar] [CrossRef] [Green Version]
- Chang, W.S.; Jung, H.H.; Zadicario, E.; Rachmilevitch, I.; Tlusty, T.; Vitek, S.; Chang, J.W. Factors associated with successful magnetic resonance-guided focused ultrasound treatment: Efficiency of acoustic energy delivery through the skull. J. Neurosurg. 2016, 124, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Hynynen, K.; McDannold, N.; Clement, G.; Jolesz, F.A.; Zadicario, E.; Killiany, R.; Moore, T.; Rosen, D. Pre-clinical testing of a phased array ultrasound system for MRI-guided noninvasive surgery of the brain--a primate study. Eur. J. Radiol. 2006, 59, 149–156. [Google Scholar] [CrossRef]
- Coluccia, D.; Fandino, J.; Schwyzer, L.; O’Gorman, R.; Remonda, L.; Anon, J.; Martin, E.; Werner, B. First noninvasive thermal ablation of a brain tumor with MR-guided focused ultrasound. J. Ther. Ultrasound 2014, 2, 17. [Google Scholar] [CrossRef] [Green Version]
- Ram, Z.; Cohen, Z.R.; Harnof, S.; Tal, S.; Faibel, M.; Nass, D.; Maier, S.E.; Hadani, M.; Mardor, Y. Magnetic resonance imaging-guided, high-intensity focused ultrasound for brain tumor therapy. Neurosurgery 2006, 59, 949–955. [Google Scholar] [CrossRef]
- McDannold, N.; Clement, G.T.; Black, P.; Jolesz, F.; Hynynen, K. Transcranial magnetic resonance imaging—Guided focused ultrasound surgery of brain tumors. Neurosurgery 2010, 66, 323–332. [Google Scholar] [CrossRef] [Green Version]
- Arvanitis, C.D.; Livingstone, M.S.; McDannold, N. Combined ultrasound and MR imaging to guide focused ultrasound therapies in the brain. Phys. Med. Biol. 2013, 58, 4749–4761. [Google Scholar] [CrossRef] [Green Version]
- Aryal, M.; Vykhodtseva, N.; Zhang, Y.-Z.; Park, J.; McDannold, N. Multiple treatments with liposomal doxorubicin and ultrasound-induced disruption of blood-tumor and blood-brain barriers improve outcomes in a rat glioma model. J. Control. Release 2013, 169, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Bijgaart, R.J.E.; Eikelenboom, D.C.; Hoogenboom, M.; Fütterer, J.J.; den Brok, M.H.; Adema, G.J. Thermal and mechanical high-intensity focused ultrasound: Perspectives on tumor ablation, immune effects and combination strategies. Cancer Immunol. Immunother. 2017, 66, 247–258. [Google Scholar] [CrossRef] [Green Version]
- Zünkeler, B.; Carson, R.E.; Olson, J.; Blasberg, R.G.; DeVroom, H.; Lutz, R.J.; Saris, S.C.; Wright, D.C.; Kammerer, W.; Patronas, N.J.; et al. Quantification and pharmacokinetics of blood-brain barrier disruption in humans. J. Neurosurg. 1996, 85, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Ostergaard, L.; Hochberg, F.H.; Rabinov, J.D.; Sorensen, A.G.; Lev, M.; Kim, L.; Weisskoff, R.M.; Gonzalez, R.G.; Gyldensted, C.; Rosen, B.R. Early changes measured by magnetic resonance imaging in cerebral blood flow, blood volume, and blood-brain barrier permeability following dexamethasone treatment in patients with brain tumors. J. Neurosurg. 1999, 90, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, A.; McDannold, N.J.; Golby, A.J. Focused ultrasound strategies for brain tumor therapy. Oper. Neurosurg. 2020, 19, 9–18. [Google Scholar] [CrossRef]
- Kinoshita, M.; McDannold, N.; Jolesz, F.A.; Hynynen, K. Noninvasive localized delivery of Herceptin to the mouse brain by MRI-guided focused ultrasound-induced blood-brain barrier disruption. Proc. Natl. Acad. Sci. USA 2006, 103, 11719–11723. [Google Scholar] [CrossRef] [Green Version]
- McDannold, N.; Vykhodtseva, N.; Raymond, S.; Jolesz, F.A.; Hynynen, K. MRI-guided targeted blood-brain barrier disruption with focused ultrasound: Histological findings in rabbits. Ultrasound Med. Biol. 2005, 31, 1527–1537. [Google Scholar] [CrossRef]
- McDannold, N.J.; Vykhodtseva, N.I.; Hynynen, K. Microbubble contrast agent with focused ultrasound to create brain lesions at low power levels: MR imaging and histologic study in rabbits. Radiology 2006, 241, 95–106. [Google Scholar] [CrossRef]
- Salameh, J.-P.; Bossuyt, P.M.; McGrath, T.A.; Thombs, B.D.; Hyde, C.J.; Macaskill, P.; Deeks, J.J.; Leeflang, M.; Korevaar, D.A.; Whiting, P.; et al. Preferred reporting items for systematic review and meta-analysis of diagnostic test accuracy studies (PRISMA-DTA): Explanation, elaboration, and checklist. BMJ 2020, 370, m2632. [Google Scholar] [CrossRef] [PubMed]
- Guthkelch, A.N.; Carter, L.P.; Cassady, J.R.; Hynynen, K.H.; Iacono, R.P.; Johnson, P.C.; Obbens, E.A.M.T.; Roemer, R.B.; Seeger, J.F.; Shimm, D.S.; et al. Treatment of malignant brain tumors with focused ultrasound hyperthermia and radiation: Results of a phase I trial. J. Neurooncol. 1991, 10, 271–284. [Google Scholar] [CrossRef] [PubMed]
- Tobias, J.; Hynynen, K.; Roemer, R.; Guthkelch, A.N.; Fleischer, A.S.; Shively, J. An ultrasound window to perform scanned, focused ultrasound hyperthermia treatments of brain tumors. Med. Phys. 1987, 14, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Hynynen, K.; Roemer, R.; Anhalt, D.; Johnson, C.; Xu, Z.X.; Swindell, W.; Cetas, T. A scanned, focused, multiple transducer ultrasonic system for localized hyperthermia treatments. Int. J. Hyperth. 1987, 3, 21–35. [Google Scholar] [CrossRef]
- Park, J.W.; Jung, S.; Jung, T.Y.; Lee, M.C. Focused ultrasound surgery for the treatment of recurrent anaplastic astrocytoma: A preliminary report. AIP Conf. Proc. 2006, 829, 238. [Google Scholar]
- Carpentier, A.; Canney, M.; Vignot, A.; Reina, V.; Beccaria, K.; Horodyckid, C.; Karachi, C.; Leclercq, D.; Lafon, C.; Chapelon, J.-Y.; et al. Clinical trial of blood-brain barrier disruption by pulsed ultrasound. Sci. Transl. Med. 2016, 8, 343re2. [Google Scholar] [CrossRef]
- Mainprize, T.; Lipsman, N.; Huang, Y.; Meng, Y.; Bethune, A.; Ironside, S.; Heyn, C.; Alkins, R.; Trudeau, M.; Sahgal, A.; et al. Blood-brain barrier opening in primary brain tumors with non-invasive MR-guided focused ultrasound: A clinical safety and feasibility study. Sci. Rep. 2019, 9, 321. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.-T.; Chai, W.-Y.; Lin, Y.-J.; Lin, C.-J.; Chen, P.-Y.; Tsai, H.-C.; Huang, C.-Y.; Kuo, J.S.; Liu, H.-L.; Wei, K.-C. Neuronavigation-guided focused ultrasound for transcranial blood-brain barrier opening and immunostimulation in brain tumors. Sci. Adv. 2021, 7, eabd0772. [Google Scholar] [CrossRef]
- Idbaih, A.; Canney, M.; Belin, L.; Desseaux, C.; Vignot, A.; Bouchoux, G.; Asquier, N.; Law-Ye, B.; Leclercq, D.; Bissery, A.; et al. Safety and feasibility of repeated and transient blood–brain barrier disruption by pulsed ultrasound in patients with recurrent glioblastoma. Clin. Cancer Res. 2019, 25, 3793–3801. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.-T.; Lin, Y.-J.; Chai, W.-Y.; Lin, C.-J.; Chen, P.-Y.; Huang, C.-Y.; Kuo, J.S.; Liu, H.-L.; Wei, K.-C. Neuronavigation-guided focused ultrasound (NaviFUS) for transcranial blood-brain barrier opening in recurrent glioblastoma patients: Clinical trial protocol. Ann. Transl. Med. 2020, 8, 673. [Google Scholar] [CrossRef] [PubMed]
- Raspagliesi, L.; D’Ammando, A.; Gionso, M.; Sheybani, N.D.; Lopes, M.-B.; Moore, D.; Allen, S.; Gatesman, J.; Porto, E.; Timbie, K.; et al. Intracranial sonodynamic therapy with 5-aminolevulinic acid and sodium fluorescein: Safety study in a porcine model. Front. Oncol. 2021, 11, 679989. [Google Scholar] [CrossRef]
- D’Ammando, A.; Raspagliesi, L.; Gionso, M.; Franzini, A.; Porto, E.; Di Meco, F.; Durando, G.; Pellegatta, S.; Prada, F. Sonodynamic therapy for the treatment of intracranial gliomas. J. Clin. Med. 2021, 10, 1101. [Google Scholar] [CrossRef]
- Prada, F.; Franzini, A.; Moosa, S.; Padilla, F.; Moore, D.; Solbiati, L.; DiMeco, F.; Legon, W. In vitro and in vivo characterization of a cranial window prosthesis for diagnostic and therapeutic cerebral ultrasound. J. Neurosurg. 2020, 134, 646–658. [Google Scholar] [CrossRef] [PubMed]
- Burgess, M.T.; Apostolakis, I.; Konofagou, E.E. Power cavitation-guided blood-brain barrier opening with focused ultrasound and microbubbles. Phys. Med. Biol. 2018, 63, 65009. [Google Scholar] [CrossRef] [PubMed]
- Pouliopoulos, A.N.; Jimenez, D.A.; Frank, A.; Robertson, A.; Zhang, L.; Kline-Schoder, A.R.; Bhaskar, V.; Harpale, M.; Caso, E.; Papapanou, N.; et al. Temporal stability of lipid-shelled microbubbles during acoustically-mediated blood-brain barrier opening. Front. Phys. 2020, 8, 137. [Google Scholar] [CrossRef]
- Konofagou, E.E.; Tunga, Y.-S.; Choia, J.; Deffieuxa, T.; Baseria, B.; Vlachosa, F. Ultrasound-induced blood-brain barrier opening. Curr. Pharm. Biotechnol. 2012, 13, 1332–1345. [Google Scholar] [CrossRef]
- Konofagou, E.E. Optimization of the ultrasound-induced blood-brain barrier opening. Theranostics 2012, 2, 1223–1237. [Google Scholar] [CrossRef]
- Prada, F.; Gennari, A.G.; Linville, I.M.; Mutersbaugh, M.E.; Chen, Z.; Sheybani, N.; DiMeco, F.; Padilla, F.; Hossack, J.A. Quantitative analysis of in-vivo microbubble distribution in the human brain. Sci. Rep. 2021, 11, 11797. [Google Scholar] [CrossRef]
- Zhu, L.; Cheng, G.; Ye, D.; Nazeri, A.; Yue, Y.; Liu, W.; Wang, X.; Dunn, G.P.; Petti, A.A.; Leuthardt, E.C.; et al. Focused ultrasound-enabled brain tumor liquid biopsy. Sci. Rep. 2018, 8, 6553. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, Y.; Huang, Z.; Wang, X.; Jin, Z.; Li, J.; Limsakul, P.; Zhu, L.; Allen, M.; Pan, Y.; et al. Control of the activity of CAR-T cells within tumours via focused ultrasound. Nat. Biomed. Eng. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jermakowicz, W.J.; Mahavadi, A.K.; Cajigas, I.; Dan, L.; Guerra, S.; Farooq, G.; Shah, A.H.; D’Haese, P.F.; Ivan, M.E.; Jagid, J.R.; et al. Predictive modeling of brain tumor laser ablation dynamics. J. Neurooncol. 2019, 144, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, O.; Arzumanov, G.; Luther, E.; McMahon, J.T.; Malcolm, J.G.; Mansour, S.; Lee, I.Y.; Willie, J.T.; Komotar, R.J.; Danish, S.F. Magnetic resonance-guided laser interstitial thermal therapy for posterior fossa neoplasms. J. Neurooncol. 2020, 149, 533–542. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patient (N) | 68 |
|---|---|
| Age (years) | 50.5 ± 15.3 |
| Sex (M/F) | 46/22 |
| Pre-FUS surgery (N) | 11 |
| Pre-FUS radiotherapy (N) | 52 |
| Patient (N) | 23 |
|---|---|
| Age (years) | 45.6 ± 19.4 |
| Sex (M/F) | 17/6 |
| Pre-FUS KPS (N) * | >40 |
| Pre-FUS surgery (N) | 11 |
| Pre-FUS RT (N) | 18 |
| Mean Sonications 1 (N) | 30.3 ± 6.8 |
| Post-FUS complication (%) | 26.1 |
| Follow-up 2 (months) | 19.7 ± 14.6 |
| References | Patient (N) | Pre-FUS Treatment (Y/N, N) | Pre-FUS Debulking (N) | Pre-FUS RT (N) | Localisation | Diagnosis | Age (yy) | Sex (M/F) | Pre-FUS KPS (N) | Recurrence (Y/N, N) | HIFU Machine | Sonications (N) | Post-FUS Follow-up (Months) | Major Complications (N) | Minor Adverse Events (N) | Stopped Procedures (N) | Post-FUS KPS (N) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Guthkelch et al. 1991 [44] | 15 | 10/5 | 6 | 10 | Supratentorial | 11 GBM 4 AA | 61 | 11/4 | >40 | 5/10 | Octoson, (Ausonics Inc., Sydney, Australia) | NA | 29.6 | 4 H (1 subcortical and 3 intracerebral) 1 TND | 0 | 4 | NA |
| Ram et al. 2006 [32] | 3 | 3/0 | 3 | 3 | Supratentorial | 3 GBM | 52 | 2/1 | NA | 3/0 | ExAblate 2000 System (InSightec, Haifa, Israel) | 38 | 26.6 | 1 NL | 0 | 0 | 60–70 |
| Park et al. 2006 [47] | 1 | 1 | 1 | 1 | Supratentorial | 1 AA | 17 | 0/1 | NA | 0/1 | Mode-JC HIFU system, (Chongqing HAIFU Medical Technology Co., LTD, Chongqing, China) | NA | NA | NA | NA | 0 | NA |
| McDannold et al. 2010 [33] | 3 | 3/0 | 0 | 3 | NA | 3 GBM | 35 | 3/0 | NA | 3/0 | ExAblate 3000 TcMRgFUS system (InSightec Ltd., Haifa, Israel) | 28 | NA | 1 H | 0 | 0 | NA |
| Coluccia et al. 2014 [31] | 1 | 1 | 1 | 1 | Supratentorial | 1 GBM | 63 | 1/0 | NA | 1/0 | ExAblate Neuro® system (InSightec Ltd., Haifa, Israel) | 25 | 3 | 0 | 0 | 0 | NA |
| Patient (N) | 45 |
|---|---|
| Age (years) | 56.6 ± 5.3 |
| Sex (M/F) | 29/16 |
| Pre-FUS KPS (N) * | 88 |
| Pre-FUS surgery 1 (N) | NA |
| Pre-FUS RT 2 (N) | 17 |
| Mean Sonications 3 (N) | 53 ± 17 |
| Post-FUS complication (%) | 0 |
| Follow-up (months) | 13.7 ± 16.1 |
| References | Patient (N) | Pre-FUS Treatment (Y/N, N) | Pre-FUS Debulking (N) | Pre-FUS RT (N) | Localisation | Diagnosis | Age (yy) | Sex (M/F) | Pre-FUS KPS (N) | Recurrence (Y/N, N) | HIFU Machine | Sonication (N) | Post-FUS Follow-up (months) | Major Complication (N) | Minor Adverse Events (N) | Stopped Procedure (N) | Post-FUS KPS (N) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Carpentier et al. 2016 [48] | 15 | 15/0 | NA | 15 | NA | 15 de novo GBM | 62 | 9/6 | NA | 11/4 | SonoCloud-9 (CarThera, Paris, France) | 41 | 2.8 | 0 | 3 (1 Local pain 1 vagal episode 1 cerebral edema) | 0 | NA |
| Mainprize et al. 2019 [49] | 5 | 5/0 | 0 | No | Supratentorial | 3 GBM 2 AA | 56 | 4/1 | 70–100 | NA | ExAblate Neuro system (InSightec Tirat Carmel, Israel) | NA | 3 | 0 | 3 (1 back pain 2 Minor headache) | 0 | NA |
| Idbaih et al. 2019 [51] | 19 | 19/0 | NA | 19 | NA | 19 GBM | 59 | 13/6 | 90 | 19 GBM | SonoCloud-9 (CarThera, Paris, France) | 65 | 12 | 0 | 8 (2 cerebral edema 2 vagal episode 3 facial palsy 1 sensorimotor deficit) | 0 | NA |
| Chen et al. 2021 [52] | 6 | 6/0 | NA | NA | Supratentorial | 6 GBM | 49.5 | 3/3 | 90 | 6 | NaviFUS (NaviFUS Inc., Taiwan) | NA | 37 | 0 | 0 | 0 | NA |
| Study | ClinicalTrials.gov Identifier | Aim | Study Location(s) | Intervention | Condition | Status |
|---|---|---|---|---|---|---|
| Non-Invasive Focused Ultrasound (FUS) With Oral Panobinostat in Children With Progressive Diffuse Midline Glioma (DMG) | NCT04804709 | BBB Opening | Columbia University Irving Medical Center New York, NY, USA |
|
| Recruiting |
| Study of Sonodynamic Therapy in Participants With Recurrent High-Grade Glioma | NCT04559685 | Tumor Ablation | St. Joseph’s Hospital and Medical Center, Phoenix, AZ, USA | Combination Product: SONALA-001(ALA) and MR-Guided Focused Ultrasound device (MRgFUS) | High Grade Glioma | Recruiting |
| ExAblate (Magnetic Resonance-guided Focused Ultrasound Surgery) Treatment of Brain Tumors | NCT01473485 | Tumor Ablation | Sunnybrook Health Sciences Centre Toronto, ON, Canada | ExAblate Transcranial System |
| Active, not recruiting |
| Assessment of Safety and Feasibility of ExAblate Blood-Brain Barrier (BBB) Disruption | NCT03551249 | BBB Opening |
| Focused ultrasound |
| Recruiting |
| Assessment of Safety and Feasibility of ExAblate Blood-Brain Barrier (BBB) Disruption for Treatment of Glioma | NCT03616860 | BBB Opening | Sunnybrook Health Sciences Centre Toronto, ON, Canada | Focused Ultrasound BBB Disruption | Glioblastoma | Recruiting |
| Efficacy and Safety of NaviFUS System add-on Bevacizumab (BEV) in Recurrent GBM Patients | NCT04446416 | BBB Opening | Linkou Chang Gung Memorial Hospital Taoyuan City, Taiwan |
|
| Recruiting |
| Sonodynamic Therapy With ExAblate System in Glioblastoma Patients | NCT04845919 | BBB Opening and Immunologic Effect | Fondazione I.R.C.C.S. Istituto Neurologico Carlo Besta, Milan, Italy | 5-Aminolevulinic Acid | Glioblastoma Multiforme | Not yet recruiting |
| Exablate Blood-Brain Barrier Disruption With Carboplatin for the Treatment of rGBM | NCT04440358 | BBB Opening |
|
| Recurrent Glioblastoma | Recruiting |
| Exablate Blood-Brain Barrier Disruption for the Treatment of rGBM in Subjects Undergoing Carboplatin Monotherapy | NCT04417088 | BBB Opening |
|
| Recurrent Glioblastoma | Recruiting |
| ExAblate Blood-Brain Barrier Disruption for Glioblastoma in Patients Undergoing Standard Chemotherapy | NCT03712293 | BBB Opening | Severance Hospital, Yonsei University Health System Seoul, Seodaemun-gu, Korea | BBB Disruption with Chemotherapy Arm | Glioblastoma Multiforme | Recruiting |
| Ultrasound-based Blood-brain Barrier Opening and Albumin-bound Paclitaxel for Recurrent Glioblastoma (SC9-ABX) | NCT04528680 | BBB Opening | Northwestern Memorial Hospital Chicago, IL, USA | Paclitaxel administration | Recurrent Glioblastoma | Recruiting |
| Innovative SonoCloud-9 Device for Blood Brain Barrier Opening in First Line Temozolomide Glioblastoma Patients. (SonoFIRST) | NCT04614493 | BBB Opening |
| Temozolomide administration and increasing drug delivery | Newly diagnosed Glioblastoma | Not yet recruiting |
| Safety and Efficacy of Transient Opening of the Blood-brain Barrier (BBB) With the SonoCloud-9 (SC9-GBM-01) | NCT03744026 | BBB Opening |
| Dose limiting toxicity (DLT) of number of activated ultrasound beams for carboplatin chemotherapy | Recurrent Glioblastoma | Active, not recruiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paun, L.; Moiraghi, A.; Jannelli, G.; Nouri, A.; DiMeco, F.; Pallud, J.; Meling, T.R.; Momjian, S.; Schaller, K.; Prada, F.; et al. From Focused Ultrasound Tumor Ablation to Brain Blood Barrier Opening for High Grade Glioma: A Systematic Review. Cancers 2021, 13, 5614. https://doi.org/10.3390/cancers13225614
Paun L, Moiraghi A, Jannelli G, Nouri A, DiMeco F, Pallud J, Meling TR, Momjian S, Schaller K, Prada F, et al. From Focused Ultrasound Tumor Ablation to Brain Blood Barrier Opening for High Grade Glioma: A Systematic Review. Cancers. 2021; 13(22):5614. https://doi.org/10.3390/cancers13225614
Chicago/Turabian StylePaun, Luca, Alessandro Moiraghi, Gianpaolo Jannelli, Aria Nouri, Francesco DiMeco, Johan Pallud, Torstein R. Meling, Shahan Momjian, Karl Schaller, Francesco Prada, and et al. 2021. "From Focused Ultrasound Tumor Ablation to Brain Blood Barrier Opening for High Grade Glioma: A Systematic Review" Cancers 13, no. 22: 5614. https://doi.org/10.3390/cancers13225614
APA StylePaun, L., Moiraghi, A., Jannelli, G., Nouri, A., DiMeco, F., Pallud, J., Meling, T. R., Momjian, S., Schaller, K., Prada, F., & Migliorini, D. (2021). From Focused Ultrasound Tumor Ablation to Brain Blood Barrier Opening for High Grade Glioma: A Systematic Review. Cancers, 13(22), 5614. https://doi.org/10.3390/cancers13225614