
Dynamics of Serum Thymidine Kinase 1 at the First Cycle of Neoadjuvant Chemotherapy Predicts Outcome of Disease in Estrogen-Receptor-Positive Breast Cancer


Abstract
:Simple Summary
Abstract
1. Introduction
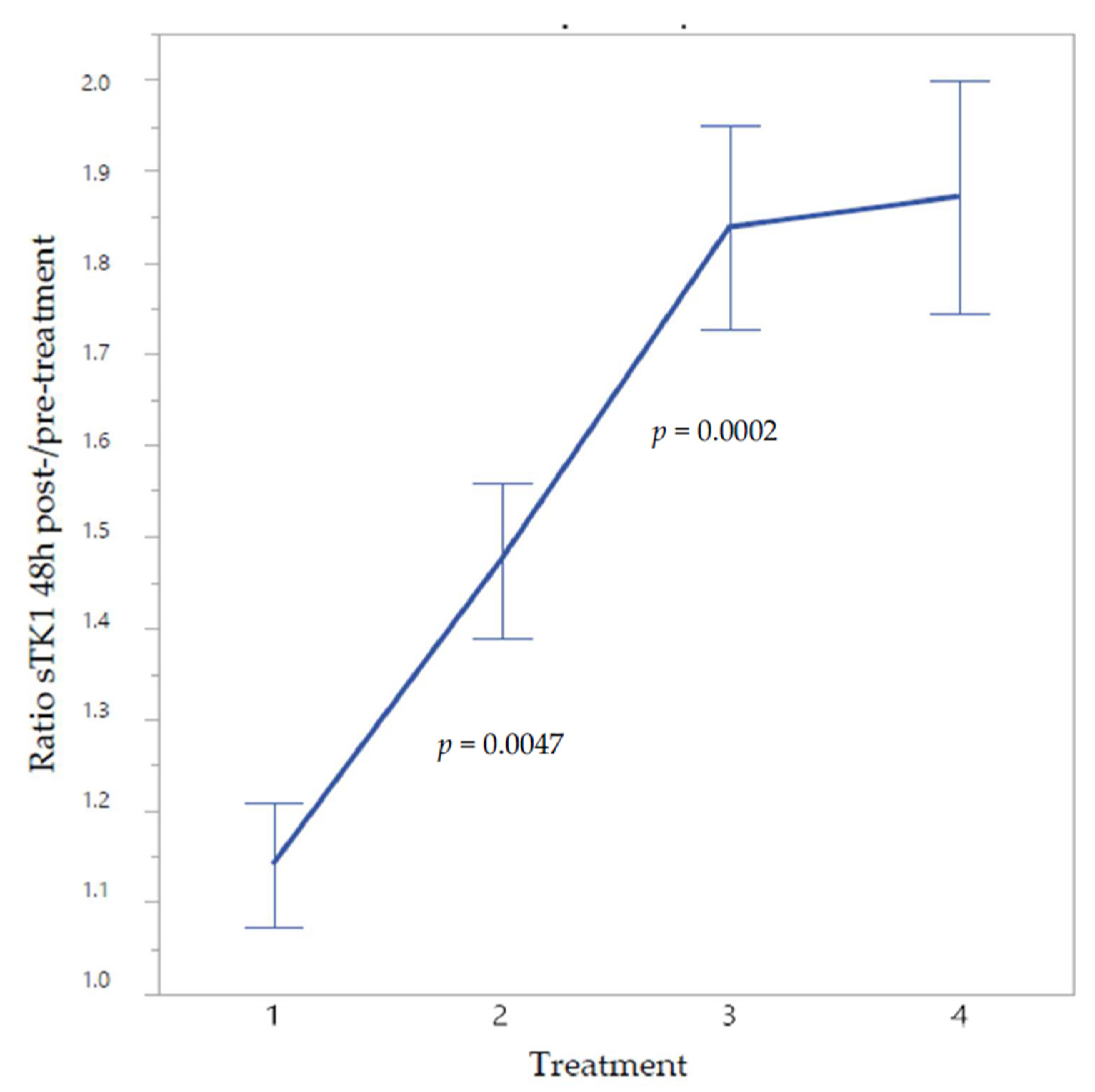
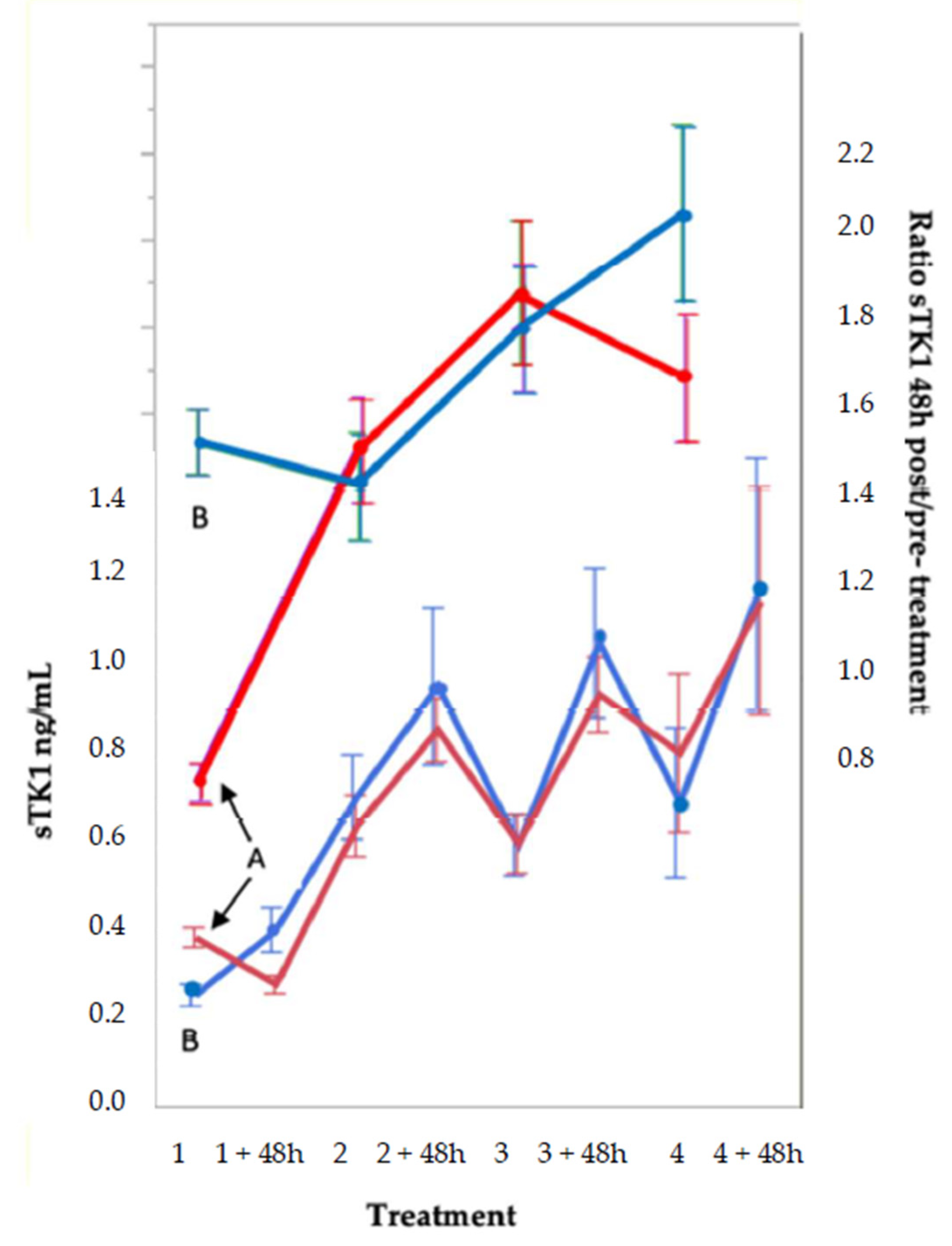
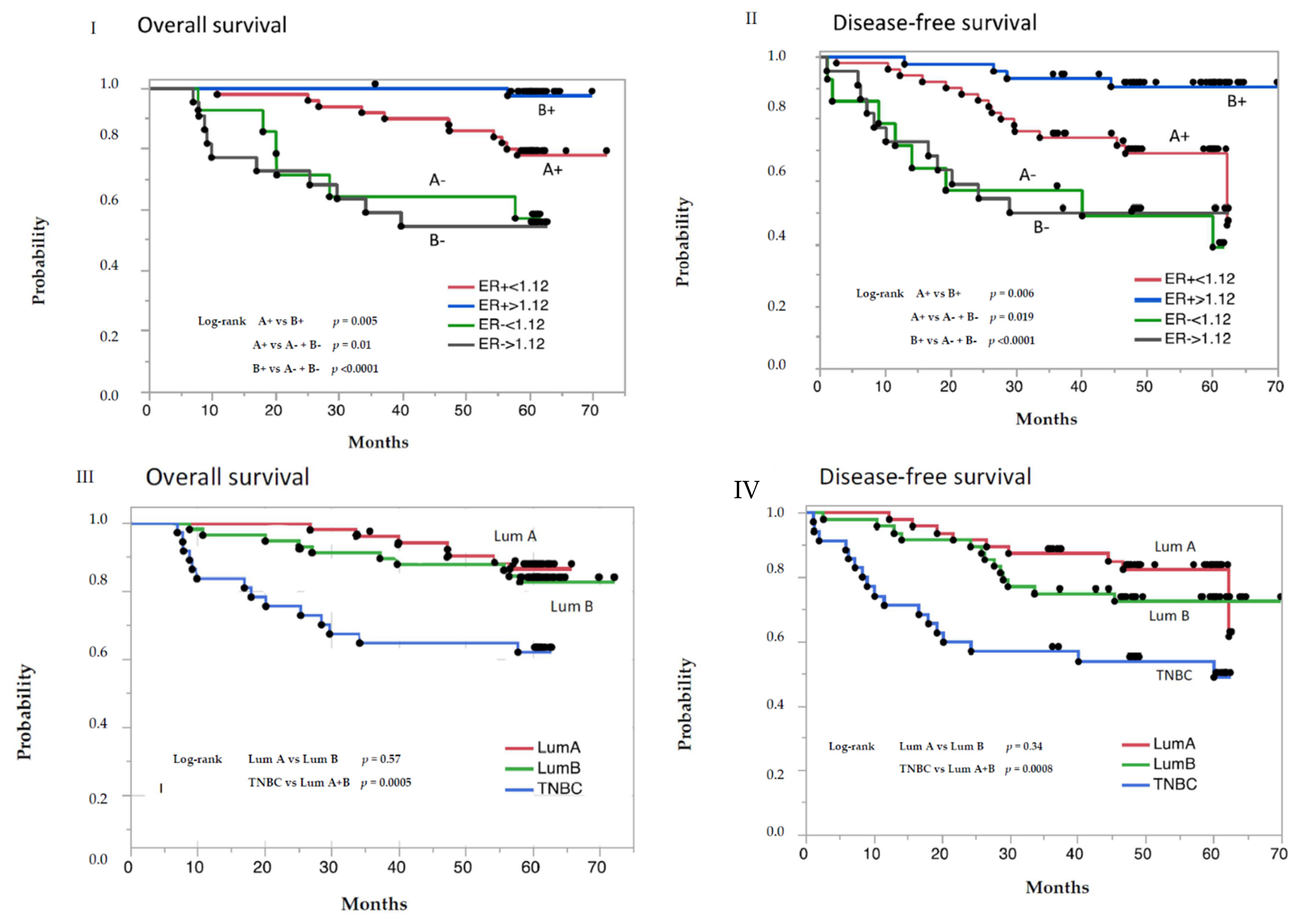
2. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A1 | A2 | A3 | B1 | B2 | B3 | |
|---|---|---|---|---|---|---|
| Before Treatment | 48 h after Treatment | Ratio Post/Pre-Treatment | Before Treatment | 48 h after Treatment | Ratio Post/Pre-Treatment | Statistics |
| Group 1 n = 54 | ||||||
| sTK1, ng/mL | ||||||
| 0.40(0.34–0.45) | 0.27(0.2–0.37) | 0.76(0.6–0.9) | 0.23(0.17–0.30) | 0.30(0.22–0.46) | 1.38(1.18–1.82) | A1 vs. A2 p < 0.0001 |
| (n = 27) | (n = 27) | B1 vs. B2 p < 0.0001 | ||||
| A1 vs. B1 p < 0.0001 | ||||||
| A2 vs. B2 p = 0.139 | ||||||
| Group 2 n = 77 | A3 vs. B3 p < 0.0001 | |||||
| sTK1, ng/mL | ||||||
| 0.35(0.24–0.45) | 0.27(0.17–034) | 0.82(0.59–1.0) | 0.31(0.21–0.44) | 0.56(0.31–0.78) | 1.60(1.32–2.29) | A1 vs. A2 p = 0.0006 |
| (n = 38) | (n = 39) | B1 vs. B2 p = 0.0001 | ||||
| A1 vs. B1 p = 0.495 | ||||||
| A2 vs. B2 p < 0.0001 | ||||||
| Group 1 + 2 n = 131 | A3 vs. B3 p < 0.0001 | |||||
| sTK1, ng/mL | ||||||
| 0.35(0.25–0.44) | 0.27(0.19–0.34) | 0.78(0.60–0.98) | 0.26(0.19–0.42) | 0.45(0.27–0.74) | 1.46(1.29–1.98) | A1 vs. A2 p < 0.0001 |
| (n = 65) | (n = 66) | B1 vs. B2 p < 0.0001 | ||||
| A1 vs. B1 p = 0.007 | ||||||
| A2 vs. B2 p < 0.001 | ||||||
| A3 vs. B3 p < 0.0001 |
3. Discussion
4. Materials and Methods
4.1. Study Design and Treatment
4.2. Data Collection
4.3. Tumor Pathology
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mougalian, S.S.; Soulos, P.R.; Killelea, B.K.; Lannin, D.R.; Abu-Khalaf, M.M.; DiGiovanna, M.P.; Sanft, T.B.; Pusztai, L.; Gross, C.P.; Chagpar, A.B. Use of neoadjuvant chemotherapy for patients with stage I to III breast cancer in the United States. Cancer 2015, 121, 2544–2552. [Google Scholar] [CrossRef]
- Killelea, B.K.; Yang, V.Q.; Mougalian, S.; Horowitz, N.R.; Pusztai, L.; Chagpar, A.B.; Lannin, D. RNeoadjuvant chemotherapy for breast cancer increases the rate of breast conservation: Results from the National Cancer Database. JACS 2015, 220, 1063–1069. [Google Scholar] [CrossRef]
- Houssami, N.; Macaskill, P.; von Minckwitz, G.; Marinovich, M.L.; Mamounas, E. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoadjuvant chemotherapy. Eur. J. Cancer 2012, 48, 3342–3354. [Google Scholar] [CrossRef]
- Thompson, A.M.; Moulder-Thompson, S.L. Neoadjuvant treatment of breast cancer. Ann. Oncol. 2012, 23 (Suppl. S10), x231–x236. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Mankoff, D.; Espié, M.; Hindié, E. ¹⁸F-FDG PET/CT in the early prediction of pathological response in aggressive subtypes of breast cancer: Review of the literature and recommendations for use in clinical trials. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 983–993. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Majdoub, M.; Sanna, A.; de Cremoux, P.; Hindié, E.; Giacchetti, S.; Martineau, A.; de Roquancourt, A.; Merlet, P.; Visvikis, D.; et al. Early Metabolic Response to Neoadjuvant Treatment: FDG PET/CT Criteria according to Breast Cancer Subtype. Radiology 2015, 277, 358–371. [Google Scholar] [CrossRef]
- Moghadas-Dastjerdi, H.; Sha-E-Tallat, H.R.; Sannachi, L.; Sadeghi-Naini, A.; Czarnota, G.J. A priori prediction of tumour response to neoadjuvant chemotherapy in breast cancer patients using quantitative CT and machine learning. Sci. Rep. 2020, 10, 10936. [Google Scholar] [CrossRef] [PubMed]
- Schwarzenbach, H.; Pantel, K. Circulating DNA as biomarker in breast cancer. Breast Cancer Res. 2015, 17, 136. [Google Scholar] [CrossRef] [Green Version]
- Migliaccio, I.; Leo, A.; Galardi, F.; Guarducci, C.; Fusco, G.M.; Benelli, M.; Di Leo, A.; Biganzoli, L.; Malorni, L. Circulating Biomarkers of CDK4/6 Inhibitors Response in Hormone Receptor Positive and HER2 Negative Breast Cancer. Cancers 2021, 13, 2640. [Google Scholar] [CrossRef]
- Jagarlamudi, K.K.; Shaw, M. Thymidine kinase 1 as a tumor biomarker: Technical advances offer new potential to an old biomarker. Biomark. Med. 2018, 12, 1035–1048. [Google Scholar] [CrossRef] [Green Version]
- Bitter, E.E.; Townsend, M.H.; Erickson, R.; Allen, C.; O’Neill, K.L. Thymidine kinase 1 through the ages: A comprehensive review. Cell Biosci. 2020, 10, 138. [Google Scholar] [CrossRef] [PubMed]
- Munch-Petersen, B. Enzymatic regulation of cytosolic thymidine kinase 1 and mitochondrial thymidine kinase 2: A mini review. Nucleosides Nucleotides Nucleic Acids 2010, 29, 363–369. [Google Scholar] [CrossRef]
- Chen, Y.L.; Eriksson, S.; Chang, Z.F. Regulation and functional contribution of thymidine kinase 1 in repair of DNA damage. J. Biol. Chem. 2010, 285, 27327–27335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherley, J.L.; Kelly, T.J. Regulation of human thymidine kinase during the cell cycle. J. Biol. Chem. 1988, 263, 8350–8358. [Google Scholar] [CrossRef]
- Ke, P.Y.; Chang, Z.F. Mitotic degradation of human thymidine kinase 1 is dependent on the anaphase-promoting complex/cyclosome-CDH1-mediated pathway. Mol. Cell. Biol. 2004, 24, 514–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, J.K.; Holmgren, S.; Levedahl, K.H.; Höglund, M.; Venge, P.; Eriksson, S. AroCell TK 210 ELISA for determination of TK1 protein: Age-related reference ranges and comparison with other TK1 assays. BioTechniques 2020, 68, 334–341. [Google Scholar] [CrossRef]
- Tribukait, B. Early prediction of pathologic response to neoadjuvant treatment of breast cancer: Use of a cell-loss metric based on serum thymidine kinase 1 and tumour volume. BMC Cancer 2020, 20, 440. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J.; Panel members. Personalizing the treatment of women with early breast cancer: Highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Malaise, E.P.; Chavaudra, N.; Tubiana, M. The relationship between growth rate, labelling index and histological type of human solid tumours. Eur. J. Cancer 1973, 9, 305–312. [Google Scholar] [CrossRef]
- Patel, A.A.; Zhang, Y.; Fullerton, J.N.; Boelen, L.; Rongvaux, A.; Maini, A.A.; Bigley, V.; Flavell, R.A.; Gilroy, D.W.; Asquith, B.; et al. The fate and lifespan of human monocyte subsets in steady state and systemic inflammation. J. Exp. Med. 2017, 214, 1913–1923. [Google Scholar] [CrossRef]
- Safonov, A.; Jiang, T.; Bianchini, G.; Győrffy, B.; Karn, T.; Hatzis, C.; Pusztai, L. Immune Gene Expression Is Associated with Genomic Aberrations in Breast Cancer. Cancer Res. 2017, 77, 3317–3324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrales, L.; Matson, V.; Flood, B.; Spranger, S.; Gajewski, T.F. Innate immune signaling and regulation in cancer immunotherapy. Cancer Res. 2017, 27, 96–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallioniemi, O.P.; Blanco, G.; Alavaikko, M.; Hietanen, T.; Mattila, J.; Lauslahti, K.; Koivula, T. Tumour DNA ploidy as an independent prognostic factor in breast cancer. Br. J. Cancer 1987, 56, 637–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Q.; Zou, L.; Zhang, P.A.; Lui, J.X.; Skog, S.; Fornander, T. The clinical significance of thymidine kinase 1 measurement in serum of breast cancer patients using anti-TK1 antibody. Int. J. Biol. Markers 2000, 15, 139–146. [Google Scholar] [CrossRef]
- Zou, L.; Zhang, P.G.; Zou, S.; Li, Y.; He, Q. The half-life of thymidine kinase 1 in serum measured by ECL dot blot: A potential marker for monitoring the response to surgery of patients with gastric cancer. Int. J. Biol. Markers 2002, 7, 135–140. [Google Scholar] [CrossRef]
- Lou, X.; Zhou, J.; Ma, H.; Xu, S.; He, E.; Skog, S.; Wang, H. The Half-Life of Serum Thymidine Kinase 1 Concentration Is an Important Tool for Monitoring Surgical Response in Patients with Lung Cancer: A Meta-Analysis. Genet. Test. Mol. Biomark. 2017, 21, 471–478. [Google Scholar] [CrossRef]
- Dodson, A.; Parry, S.; Ibrahim, M.; Bartlett, J.M.; Pinder, S.; Dowsett, M.; Miller, K. Breast cancer biomarkers in clinical testing: Analysis of a UK national external quality assessment scheme for immunocytochemistry and in situ hybridisation database containing results from 199 300 patients. J. Pathol. Clin. Res. 2018, 4, 262–273. [Google Scholar] [CrossRef]
- Johansson, A.; Trewin, C.B.; Fredriksson, I.; Reinertsen, K.V.; Russnes, H.; Ursin, G. In modern times, how important are breast cancer stage, grade and receptor subtype for survival: A population-based cohort study. Breast Cancer Res. 2021, 23, 17. [Google Scholar] [CrossRef]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.; Reynolds, K.L.; Smith, B.L.; Alexander, B.; Moy, B.; Isakoff, S.J.; et al. Pathologic Complete Response after Neoadjuvant Chemotherapy and Impact on Breast Cancer Recurrence and Survival: A Comprehensive Meta-analysis. Clin. Cancer Res. 2020, 26, 2838–2848. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Untch, M.; Blohmer, J.U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. Am. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef] [Green Version]
- Selli, C.; Dixon, J.M.; Sims, A.H. Accurate prediction of response to endocrine therapy in breast cancer patients: Current and future biomarkers. Breast Cancer Res. 2016, 18, 118. [Google Scholar] [CrossRef] [Green Version]
- Dumontet, C.; Jordan, M.A. Microtubule-binding agents: A dynamic field of cancer therapeutics. Nat. Rev. Drug Discov. 2010, 9, 790–803. [Google Scholar] [CrossRef] [Green Version]
- Björnström, L.; Sjöberg, M. Mechanisms of estrogen receptor signaling: Convergence of genomic and nongenomic actions on target genes. Mol. Endocrinol. 2005, 19, 833–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saha, S.; Dey, S.; Nath, S. Steroid Hormone Receptors: Links With Cell Cycle Machinery and Breast Cancer Progression. Front. Oncol. 2021, 11, 620214. [Google Scholar] [CrossRef]
- Bloom, C.R.; North, B.J. Physiological relevance of post-translational regulation of the spindle assembly checkpoint protein BubR1. Cell Biosci. 2021, 11, 76. [Google Scholar] [CrossRef] [PubMed]
- Van de Vijver, M.J.; He, Y.D.; van’t Veer, L.J.; Dai, H.; Hart, A.A.; Voskuil, D.W.; Schreiber, G.J.; Peterse, J.L.; Roberts, C.; Marton, M.J.; et al. A gene-expression signature as a predictor of survival in breast cancer. N. Engl. J. Med. 2002, 347, 1999–2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matikas, A.; Wang, K.; Lagoudaki, E.; Acs, B.; Zerdes, I.; Hartman, J.; Azavedo, E.; Bjöhle, J.; Carlsson, L.; Einbeigi, Z.; et al. Prognostic role of serum thymidine kinase 1 kinetics during neoadjuvant chemotherapy for early breast cancer. ESMO Open 2021, 6, 100076. [Google Scholar] [CrossRef]
- McKenna, P.G.; O’Neill, K.L.; Abram, W.P.; Hannigan, B.M. Thymidine kinase activities in mononuclear leukocytes and serum from breast cancer patients. Br. J. Cancer 1988, 57, 619–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlström, A.R.; Neumüller, M.; Gronowitz, J.S.; Källander, C.F. Molecular forms in human serum of enzymes synthesizing DNA precursors and DNA. Mol. Cell. Biochem. 1990, 92, 23–35. [Google Scholar] [CrossRef]
- Jagarlamudi, K.K.; Hansson, L.O.; Eriksson, S. Breast and prostate cancer patients differ significantly in their serum Thymidine kinase 1 (TK1) specific activities compared with those hematological malignancies and blood donors: Implications of using serum TK1 as a biomarker. BMC Cancer 2015, 15, 66. [Google Scholar] [CrossRef] [Green Version]
- Nisman, B.; Allweis, T.; Kadouri, L.; Mali, B.; Hamburger, T.; Baras, M.; Gronowitz, S.; Peretz, T. Comparison of diagnostic and prognostic performance of two assays measuring thymidine kinase 1 activity in serum of breast cancer patients. Clin. Chem. Lab. Med. 2013, 51, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Tacca, O.; Penault-Llorca, F.; Abrial, C.; Mouret-Reynier, M.A.; Raoelfils, I.; Durando, X.; Achard, J.L.; Gimbergues, P.; Curé, H.; Chollet, P. Changes in and prognostic value of hormone receptor status in a series of operable breast cancer patients treated with neoadjuvant chemotherapy. Oncologist 2007, 12, 636–643. [Google Scholar] [CrossRef]
- Hirata, T.; Shimizu, C.; Yonemori, K.; Hirakawa, A.; Kouno, T.; Tamura, K.; Ando, M.; Katsumata, N.; Fujiwara, Y. Change in the hormone receptor status following administration of neoadjuvant chemotherapy and its impact on the long-term outcome in patients with primary breast cancer. Br. J. Cancer 2009, 101, 1529–1536. [Google Scholar] [CrossRef] [Green Version]
- Magbanua, M.J.; Wolf, D.M.; Yau, C.; Davis, S.E.; Crothers, J.; Au, A.; Haqq, C.M.; Livasy, C.; Rugo, H.S. I-SPY 1 TRIAL Investigators; et al. Serial expression analysis of breast tumors during neoadjuvant chemotherapy reveals changes in cell cycle and immune pathways associated with recurrence and response. Breast Cancer Res. 2015, 17, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimbung, S.; Markholm, I.; Bjöhle, J.; Lekberg, T.; von Wachenfeldt, A.; Azavedo, E.; Saracco, A.; Hellström, M.; Veerla, S.; Paquet, E.; et al. For the PROMIX Trialists Group. Assessment of early response biomarkers in relation to long-term survival in patients with HER2-negative breast cancer receiving neoadjuvant chemotherapy plus bevacizumab: Results from the phase II PROMIX trial. Int. J. Cancer 2018, 142, 618–628. [Google Scholar] [CrossRef] [Green Version]
- Korde, L.A.; Lusa, L.; McShane, L.; Lebowitz, P.F.; Lukes, L.; Camphausen, K.; Parker, J.S.; Swain, S.M.; Hunter, K.; Zujewski, J.A. Gene expression pathway analysis to predict response to neoadjuvant docetaxel and capecitabine for breast cancer. Breast Cancer Res. Treat. 2010, 119, 685–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matikas, A.; Lövrot, J.; Ramberg, A.; Eriksson, M.; Lindsten, T.; Lekberg, T.; Hedenfalk, I.; Loman, N.; Bergh, J.; Hatschek, T.; et al. Dynamic evaluation of the immune infiltrate and immune function genes as predictive markers for neoadjuvant chemotherapy in hormone receptor positive, HER2 negative breast cancer. Oncoimmunology 2018, 7, e1466017. [Google Scholar] [CrossRef] [Green Version]
- SweBCG, Nationella Riktlinjer för Behandling av Bröst Cancer. 2013. Available online: http://www.swebcg.se/wp-content/uploads/2016/10/nationellt-vardprogram-brostcancer_200211.pdf (accessed on 16 January 2018).
| Characteristics | Subgroup 1 (n = 54) | Subgroup 2 (n = 77) | p Value | Total (n = 131) |
|---|---|---|---|---|
| Age, years | ||||
| Median (range) | 49.8 (33.7–70.6) | 49.7 (30.0–69.2) | 0.801 | 49.8 (30.0–70.6) |
| Menopausal status | ||||
| Pre-menopausal | 30 (55.6%) | 48 (61.3%) | 0.187 | 78(59.5%) |
| Post-menopausal | 24 (44.4%) | 29 (37.7%) | 53 (40.5%) | |
| Stage | ||||
| 1 (≤20 mm) | 3 (5.5%) | 1 (1.3%) | 0.333 | 4 (3.1) |
| 2 (>20 ≤50 mm) | 19 (35.2%) | 32 (41.6%) | 51 (38.9%) | |
| 3 (>50 mm) | 31 (57.4%) | 40 (51.9%) | 71 (54.2%) | |
| Tx | 1 (1.9%) | 4 (5.2%) | 5 (3.8%) | |
| Tumor Volume, cm3 | ||||
| Median (range) | 87 (4.2–3052) | 87 (4.2–904) | 0.831 | 87 (4.23052) |
| Missing data | 1 | 5 | 6 | |
| Grade | ||||
| 1 | 4 (5.2%) | 0.073 | 4(3.0%) | |
| 2 | 11 (20.4%) | 29 (37.7%) | 40 (30.5%) | |
| 3 | 14 (25.9%) | 20 (26.9%) | 34 (26.0%) | |
| Missing data | 29 (53.7%) | 24 (31.2%) | 53 (40.5% | |
| Histological type | ||||
| Ductal | 35 (64.8%) | 56 (72.7%) | 0.259 | 91 (69.5%) |
| Lobular | 9 (16.7%) | 11 (14.3%) | 20 (15.3%9) | |
| Other | 8 (14.8%) | 10 (13.0%) | 18 (13.7%) | |
| Missing data | 2 (3.7%) | 2 (1.5%) | ||
| ER status | ||||
| <10% | 16 (29.6%) | 20 (26.0%) | 0.630 | 36 (27.5%) |
| >10% | 37 (68.5%) | 56 (72.7%) | 93 (71.9%) | |
| Missing data | 1 (1.9%) | 1 (1.3%) | 2 (1.5%) | |
| PR status | ||||
| <10% | 20 (37.0%) | 38 (49.4%) | 0.167 | 58 (44.3%) |
| >10% | 33 (61.1%) | 38 (49.4%) | 71 (54.2) | |
| Missing data | 1 (1.9%) | 1 (1.2%) | 2 (1.5%) | |
| HER2 | ||||
| 2+ | 12 (22.2%) | 19 (24.7%) | 0.789 | 31 (23.7%) |
| 0 or 1+ | 41 (75.9%) | 58 (75.3%) | 99 (75.6%) | |
| Missing data | 1 (1.9%) | 1 (0.7%) | ||
| Nodal status | ||||
| Positive | 32 (59.3%) | 43 (55.8%) | 0.697 | 75 (57.3%) |
| Negative | 22 (40.7%) | 34 (44.2%) | 56 (42./%) | |
| Intrinsic subtype | ||||
| Luminal A | 22 (40.8%) | 26 (33.8%) | 0.699 | 48 (36.7%) |
| Luminal B | 18 (33.3%) | 30 (40.0%) | 48 (36.6%) | |
| TNBC | 14 (25.9%) | 21 (27.2%) | 35 (26.7%) | |
| Ki 67/Mib1, % | ||||
| Median (range) | 30% (1–90%) | 30% (3–90%) | 0.282 | 30% (1–90%) |
| Missing data | 3 | 6 | 9 | |
| Serum thymidine kinase 1, | ||||
| ng/mL | ||||
| Median (range) | 0.30 (0.1–0.72) | 0.32 (0.12–1.29) | 0.487 | 0.31 (0.1–1.29) |
| Characteristics | A | B | p-Value |
|---|---|---|---|
| Ratio < 1.12 (n = 65) | Ratio > 1.12 (n = 66) | ||
| Age, years | |||
| Median (range) | 51.2 (30.0–69.2) | 49.2(32.8–70.6) | 0.58 |
| Menopausal status | |||
| Premenopausal | 38 (58.5%) | 40 (60.6%) | 0.80 |
| Postmenopausal | 27 (41.5%) | 26 (39.4%) | |
| Stage | |||
| 1 (≤20 mm) | 4 (6.2%) | 0 | 0.10 |
| 2 (>20 ≤50 mm) | 23 (35.4%) | 28 (42.4%) | |
| 3 (>50 mm) | 35 (53.8%) | 36 (54.6%) | |
| Tx | 3 (4.6%) | 2 (3.0%) | |
| Tumor volume, cm3 | |||
| Median (range) | 87 (4.2–3052) | 87 (8.2–904) | 0.61 |
| Missing data | 4 | 2 | |
| Grade | |||
| 1 | 2 (3.1%) | 2 (3.9%) | 0.55 |
| 2 | 19 (29.2%) | 21 (31,8%) | |
| 3 | 14 (21.5%) | 20 (30.4%) | |
| Missing data | 30 (46.2) | 23 (34.9(%) | |
| Histological type | |||
| Ductal | 45 (69.3%) | 46 (69.7%) | 0.28 |
| Lobular | 13 (20.0%) | 7 (10.6%) | |
| Other | 6 (9.2%) | 12 (18.2%) | |
| Missing data | 1 (1.5%) | 1 (1.5%) | |
| ER status | |||
| <10% | 14 (21.6%) | 22 (33.3%) | 0.13 |
| >10% | 50 (76.9%) | 43 (65.2%) | |
| Missing data | 1 (1.5%) | 1 (1.5%) | |
| PR status | |||
| <10% | 26 (40.0%) | 32 (48.5%) | 0.33 |
| >10% | 38 (58.5%) | 33 (50%) | |
| Missing data | 1 (1.5%) | 1 (1.5%) | |
| HER2 | |||
| 2+ | 14 (21.5%) | 17 (25.8%) | 0.60 |
| 0 or 1+ | 50 (76.9%) | 49 (74.2%) | |
| Missing data | 1 (1.5%) | ||
| Nodal status | |||
| Positive | 36 (55.4%) | 39 (59.1%) | 0.69 |
| Negative | 29 (44.6%) | 27 (40.9/%) | |
| Intrinsic subtype St Gallen | |||
| Luminal A | 27 (41.5%) | 21 (31.8%) | 0.34 |
| Luminal B | 24 (36.9%) | 24 (36.4%) | |
| TNBC | 14 (21.6%) | 21 (31.8%) | |
| Ki 67/Mib1, % | |||
| Median (range) | 30% (1–90%) | 30% (3–90%) | 0.55 |
| Missing data | 6 | 3 | |
| Serum thymidine kinase 1, | |||
| ng/mL | |||
| Median (range) | 0.35 (0.12–1.29) | 0.26 (0.1–0.71) | 0.0068 |
| Stage/Lymph Nodes | Group A (n = 65) | Group B (n = 66) | p-Value |
|---|---|---|---|
| Ratio < 1.12 | Ratio > 1.12 | ||
| pT0 | 18 (27.7%) | 18 (27.3%) | 0.774 |
| pT1 | 24 (36.9%) | 22 (33.3%) | |
| pT2 | 13 (20.0%) | 18 (27.3%) | |
| pT3 | 10 (15.4%) | 8 (12.1%) | |
| pN0 | 26 (40.0%) | 19 (28.8%) | 0.610 |
| pN1 (1–3) | 23 (35.4%) | 25 (37.9%) | |
| pN2 (4–9) | 11 (16.9%) | 13 (19.7%) | |
| PN3 (>9) | 4 (6.2%) | 8 (12.1%) | |
| pNX | 1 (1.5%) | 1 (1.5%) |
| Intrinsic Subtype | Estrogen Receptor Positive | Estrogen Receptor Negative | Total | ||
|---|---|---|---|---|---|
| Group A | Group B | Group A | Group B | ||
| Ratio < 1.12 | Ratio > 1.12 | Ratio < 1.12 | Ratio > 1.12 | ||
| Luminal A | 27 (54.0%) | 20 (46.5%) | 0 | 0 | 47 |
| Luminal B | 22 (44.0%) | 23 (53.5%) | 1 (7.2%) | 1 (4.6%) | 47 |
| TNBC | 1 (2.0%) | 0 | 13 (92.8%) | 21 (95.4%) | 35 |
| Total | 50 | 43 | 14 | 22 | 129 |
| Characteristics | Luminal A | Luminal B | p-Value | Group A | Group B | p-Value |
|---|---|---|---|---|---|---|
| (n = 47) | (n = 45) | (n = 49) | (n = 43) | |||
| Age, years | Ratio < 1.12 | Ratio > 1.12 | ||||
| Median (range) | 49.4 (33.1–66.3) | 53.4 (34.4–69.2) | 0.262 | 52.8 (33.1–69.2) | 49.2 (34.4–68.1) | 0.194 |
| Menopausal status | ||||||
| Premenopausal | 30 (63.8%) | 22 (48.9%) | 0.148 | 28 (57.1%) | 24 (55.8%) | 0.898 |
| Postmenopausal | 17 (36.2%) | 23 (51.1%) | 21 (42.9%) | 19 (44.2%) | ||
| Stage | ||||||
| 1 (≤20 mm) | 3 (6.4%) | 0.030 | 3 (6.1%) | 0.192 | ||
| 2 (>20 ≤50 mm) | 22 (46.8%) | 15 (33.4%) | 17 (34.7%) | 20 (46. 5%) | ||
| 3 (>50 mm) | 22 (46.8%) | 28 (62.2%) | 28 (57.1%) | 22 (51.2%) | ||
| Tx | 2 (4.4%) | 1 (2.1%) | 1 (2.3%) | |||
| Tumor volume, cm3 | ||||||
| Median (range) | 65.4 (4.2–3052) | 96.9 (14.1–1150) | 0.051 | 96.9 (4.2–3052) | 73.6 (8.2–904) | 0.553 |
| Missing data | 1 | 2 | 2 | 1 | ||
| Grade | ||||||
| 1 | 3 (6.1%) | 1 (2.2%) | 0.010 | 2 (41%) | 2 (4.6%) | 0.898 |
| 2 | 21 (42.9%) | 17 (37.8%) | 19 (38.8%) | 19 (44.2%) | ||
| 3 | 2 (4.1%) | 12 (26.7%) | 6 (12.2%) | 8 (18.6%) | ||
| Missing data | 21 (42.9%) | 15 (33.3%) | 22 (44.9%) | 14 (32.6%) | ||
| Histological type | ||||||
| Ductal | 33 (70.3%) | 32 (71.1%) | 0.037 | 33 (67.4%) | 32 (74.4%) | 0.314 |
| Lobular | 12 (25.5%) | 6 (13.3%) | 12 (24.5%) | 6 (14.0%) | ||
| Other | 1 (2.1%) | 7 (15.6%) | 3 (6.1%) | 5 (11.6%) | ||
| Missing data | 1 (2.1%) | 1 (2.0%) | ||||
| PR status | ||||||
| <10% | 5 (10.6%) | 18 (40.0%) | 0.0009 | 12 (24.5%) | 11 (25.6%) | 0.904 |
| >10% | 42 (89.4%) | 27 (60.0%) | 37 (75.5%) | 32 (74.4%) | ||
| HER2 | ||||||
| 2+ | 12 (25.5%) | 14 (31.1%) | 0.507 | 13 (26.5%) | 13 (30.2%) | 0.740 |
| 0 or 1+ | 35 (74.5%) | 30 (66.7%) | 35 (71.5%) | 30 (69.8%) | ||
| Missing data | 1 (2.2%) | 1 (2.0%) | ||||
| Nodal status | ||||||
| Positive | 27 (57.4%) | 24 (53.3%) | 0.691 | 25 (51.0%) | 26 (60.5%) | 0.363 |
| Negative | 20 (42.6%) | 21 (46.7%) | 24 (49.0%) | 17 (39.5%) | ||
| Ki67/Mib 1, % | ||||||
| Median, (range) | 11% (1–30) | 40% (20–90) | <0.0001 | 20% (1–90) | 25% (3–85) | 0.560 |
| Missing data | 2 | 2 | 4 | |||
| Thymidine kinase 1, | ||||||
| ng/mL | ||||||
| Median (range) | 0.32 (0.13–1.29) | 0.31 (0.1–0.93) | 0.512 | 0.38 (0.12–1.29) | 0.25 (0.1–0.68) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tribukait, B. Dynamics of Serum Thymidine Kinase 1 at the First Cycle of Neoadjuvant Chemotherapy Predicts Outcome of Disease in Estrogen-Receptor-Positive Breast Cancer. Cancers 2021, 13, 5442. https://doi.org/10.3390/cancers13215442
Tribukait B. Dynamics of Serum Thymidine Kinase 1 at the First Cycle of Neoadjuvant Chemotherapy Predicts Outcome of Disease in Estrogen-Receptor-Positive Breast Cancer. Cancers. 2021; 13(21):5442. https://doi.org/10.3390/cancers13215442
Chicago/Turabian StyleTribukait, Bernhard. 2021. "Dynamics of Serum Thymidine Kinase 1 at the First Cycle of Neoadjuvant Chemotherapy Predicts Outcome of Disease in Estrogen-Receptor-Positive Breast Cancer" Cancers 13, no. 21: 5442. https://doi.org/10.3390/cancers13215442
APA StyleTribukait, B. (2021). Dynamics of Serum Thymidine Kinase 1 at the First Cycle of Neoadjuvant Chemotherapy Predicts Outcome of Disease in Estrogen-Receptor-Positive Breast Cancer. Cancers, 13(21), 5442. https://doi.org/10.3390/cancers13215442