
BRAFV600E Mutant Allele Frequency (MAF) Influences Melanoma Clinicopathologic Characteristics

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
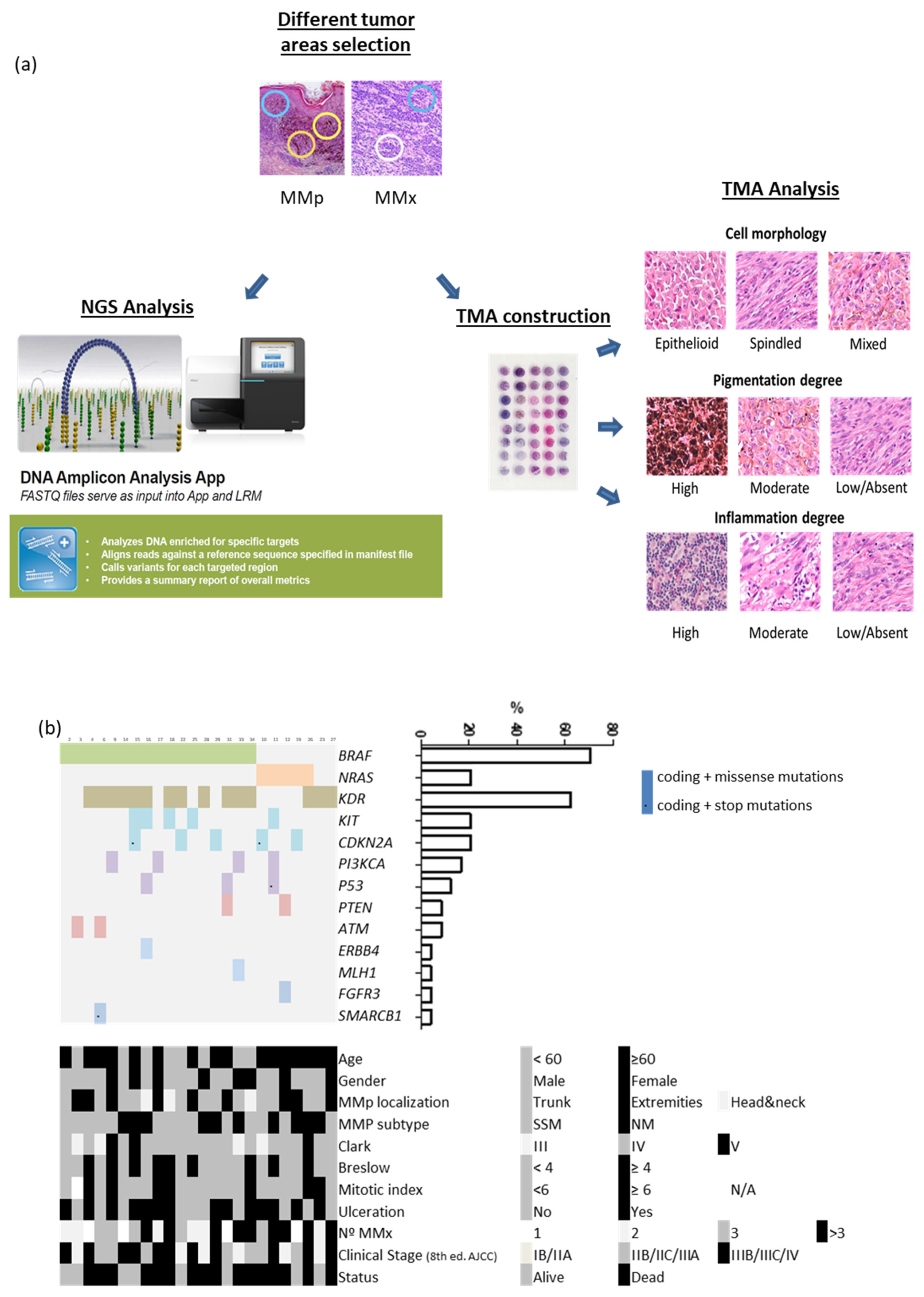
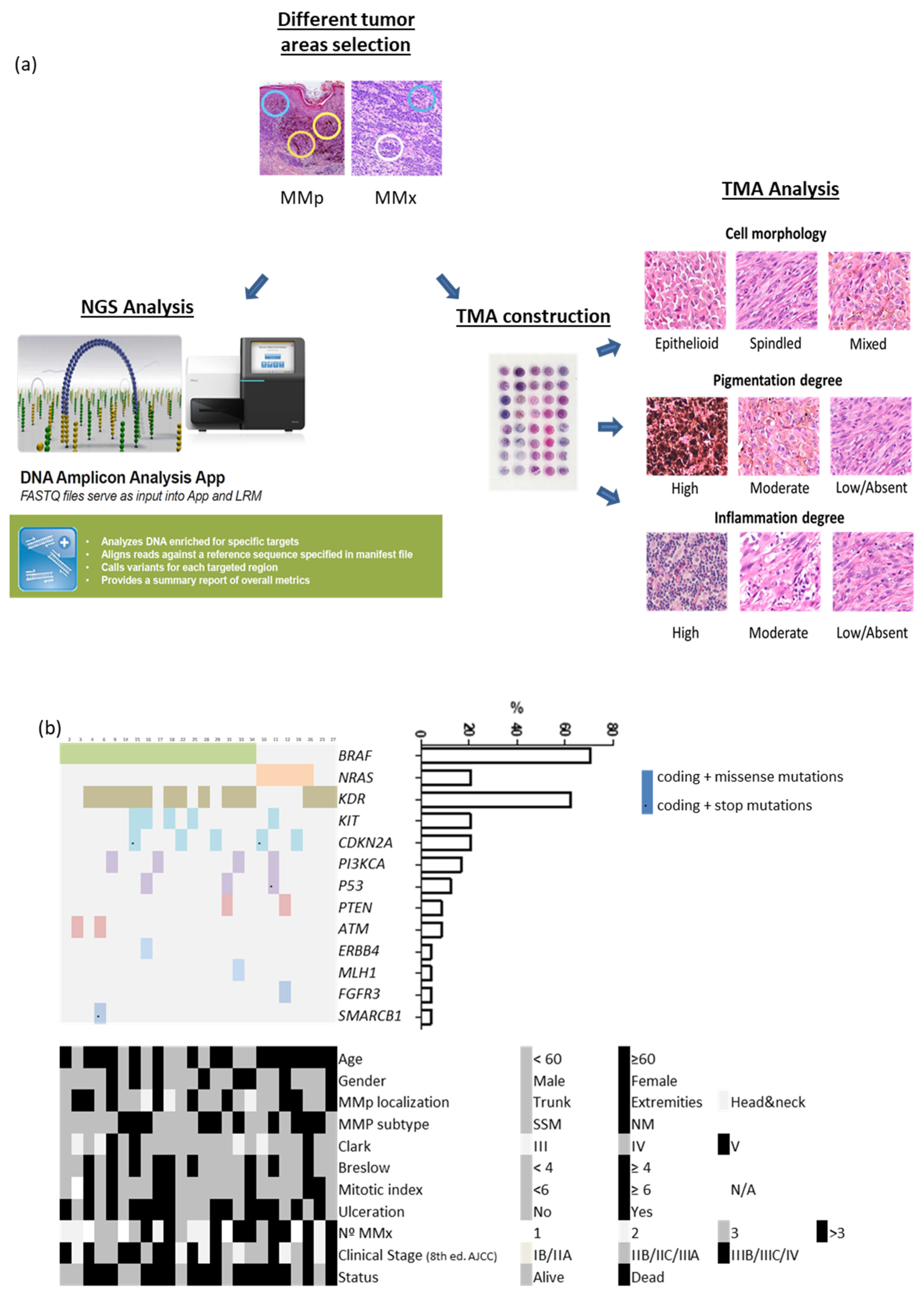
2. Materials and Methods
2.1. Patient Selection and Data Collection
2.2. Diagnostic Criteria of Histological Features
2.3. DNA Extraction and NGS Analysis
2.4. TMA Elaboration and Analysis
Immunohistochemical Analysis of BRAFV600E Specific Target Protein
2.5. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics
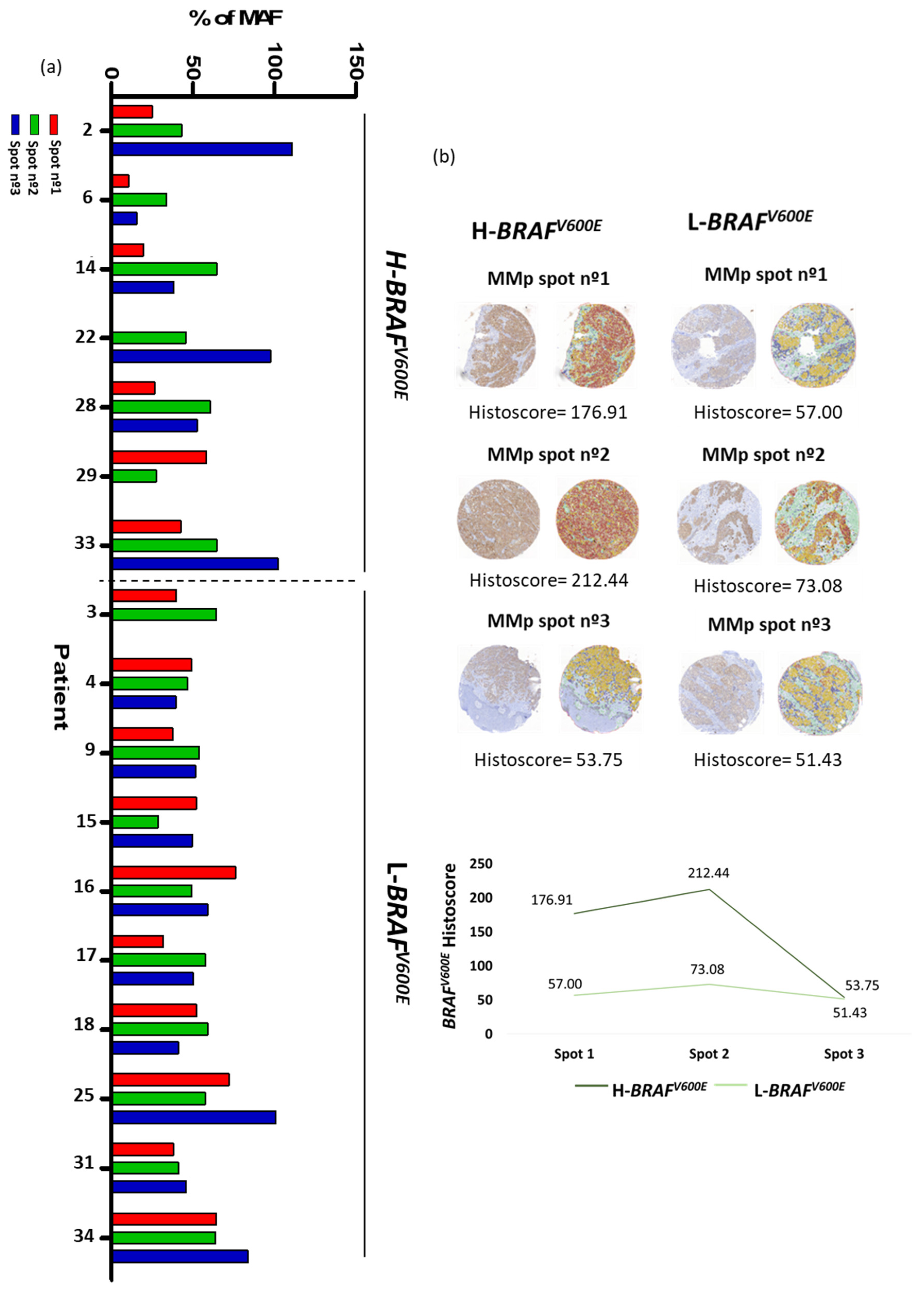
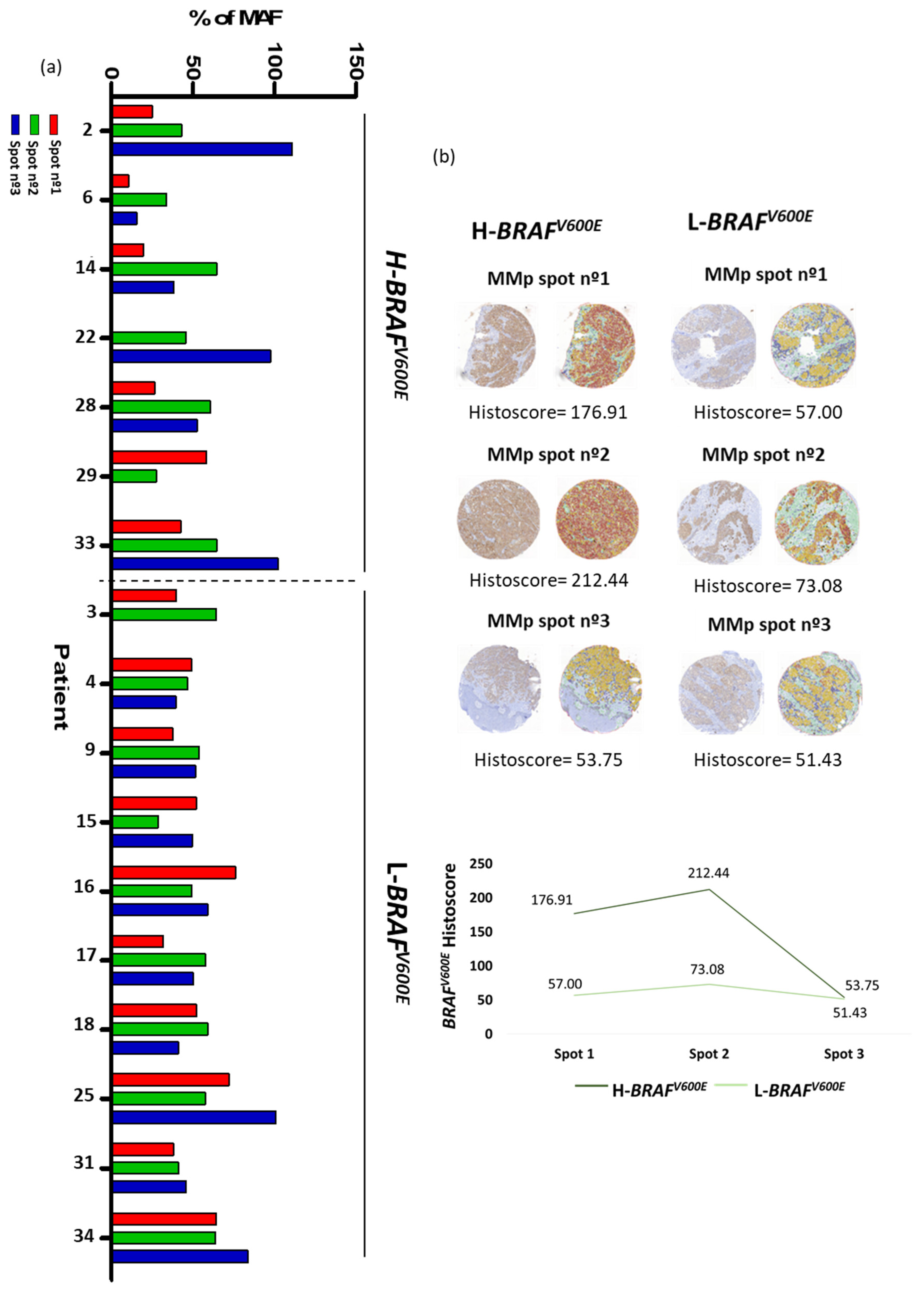
3.2. Genetic Analysis: There Is Variation in BRAFV600E Mutant Allele Frequency in Primary Melanomas
3.3. Immunohistochemical Analysis: There Is Variation in BRAFV600E Immunoexpression in Primary Melanomas
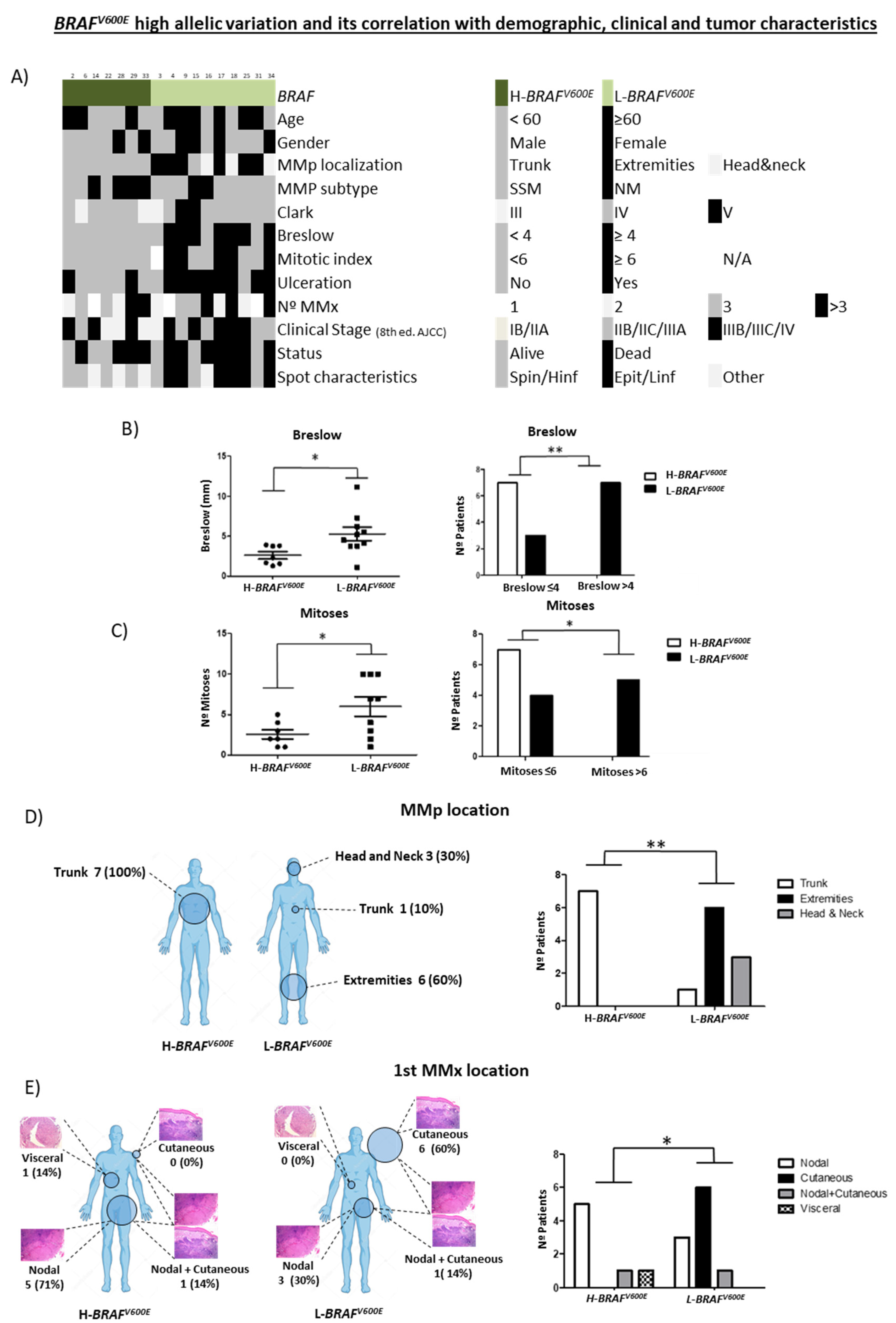
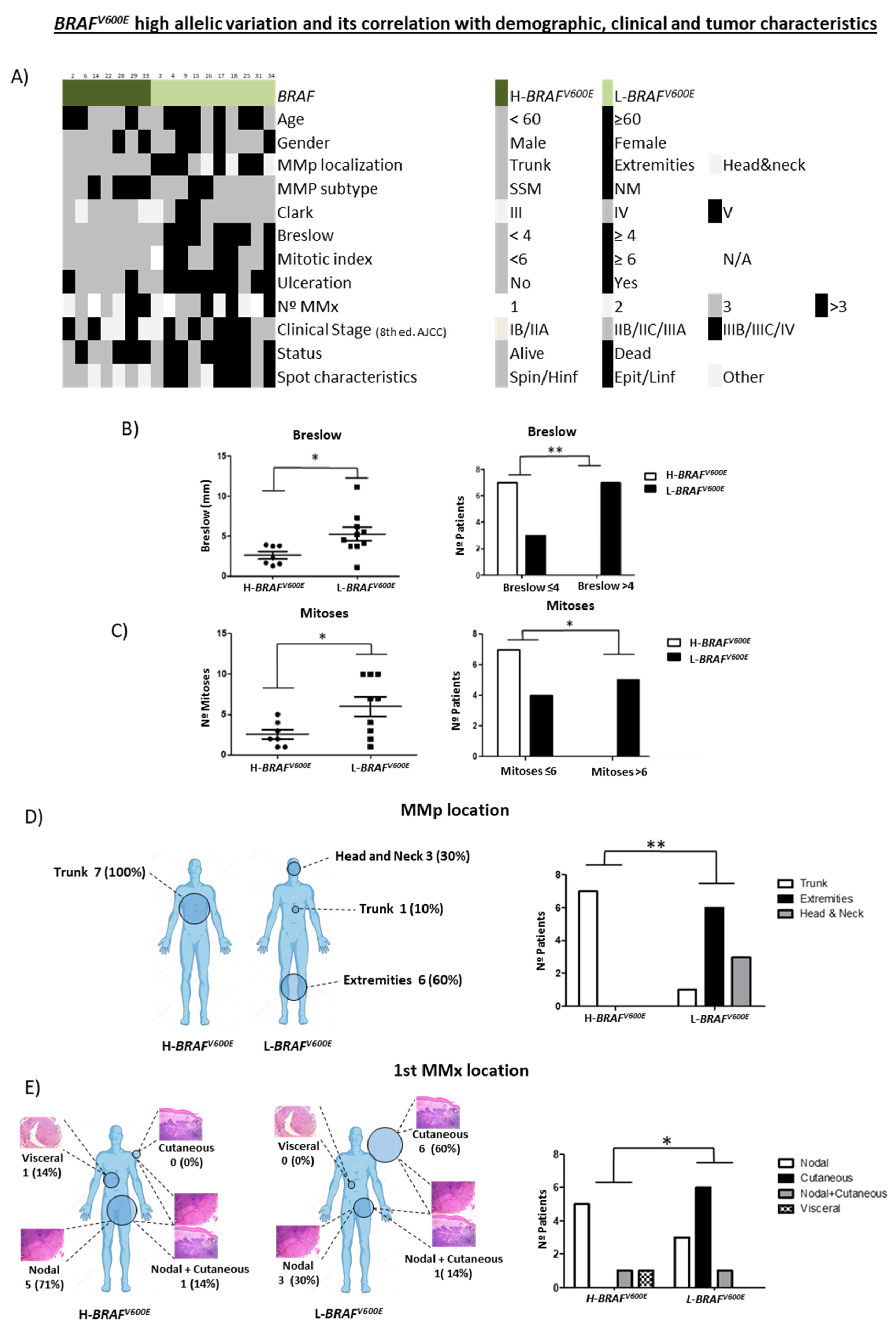
3.4. Correlation between BRAFV600E Allelic Frequency Variation and Histomorphological Features
3.4.1. H-BRAFV600E Correlation with Demographic, Clinical and Tumor Characteristics
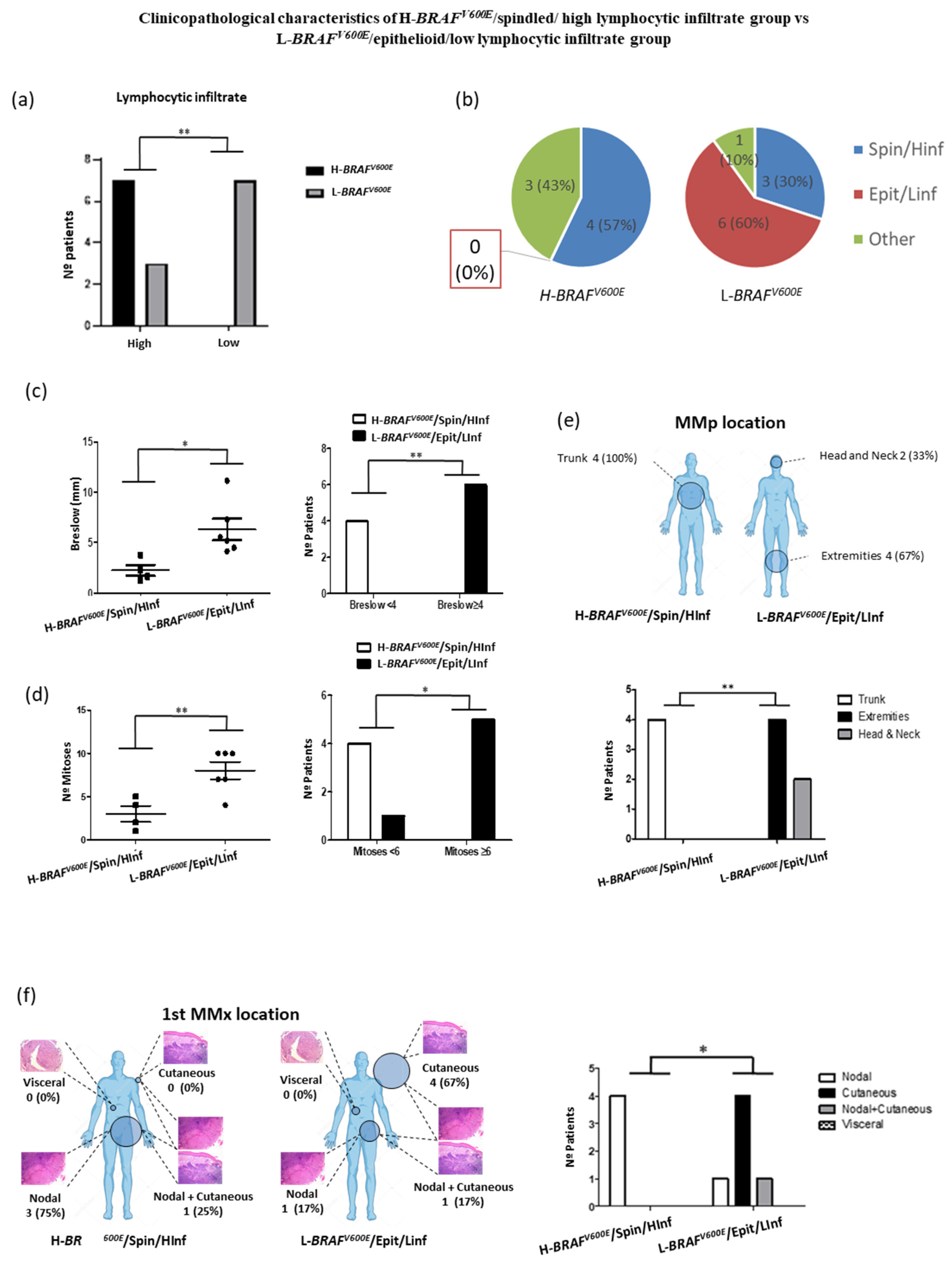
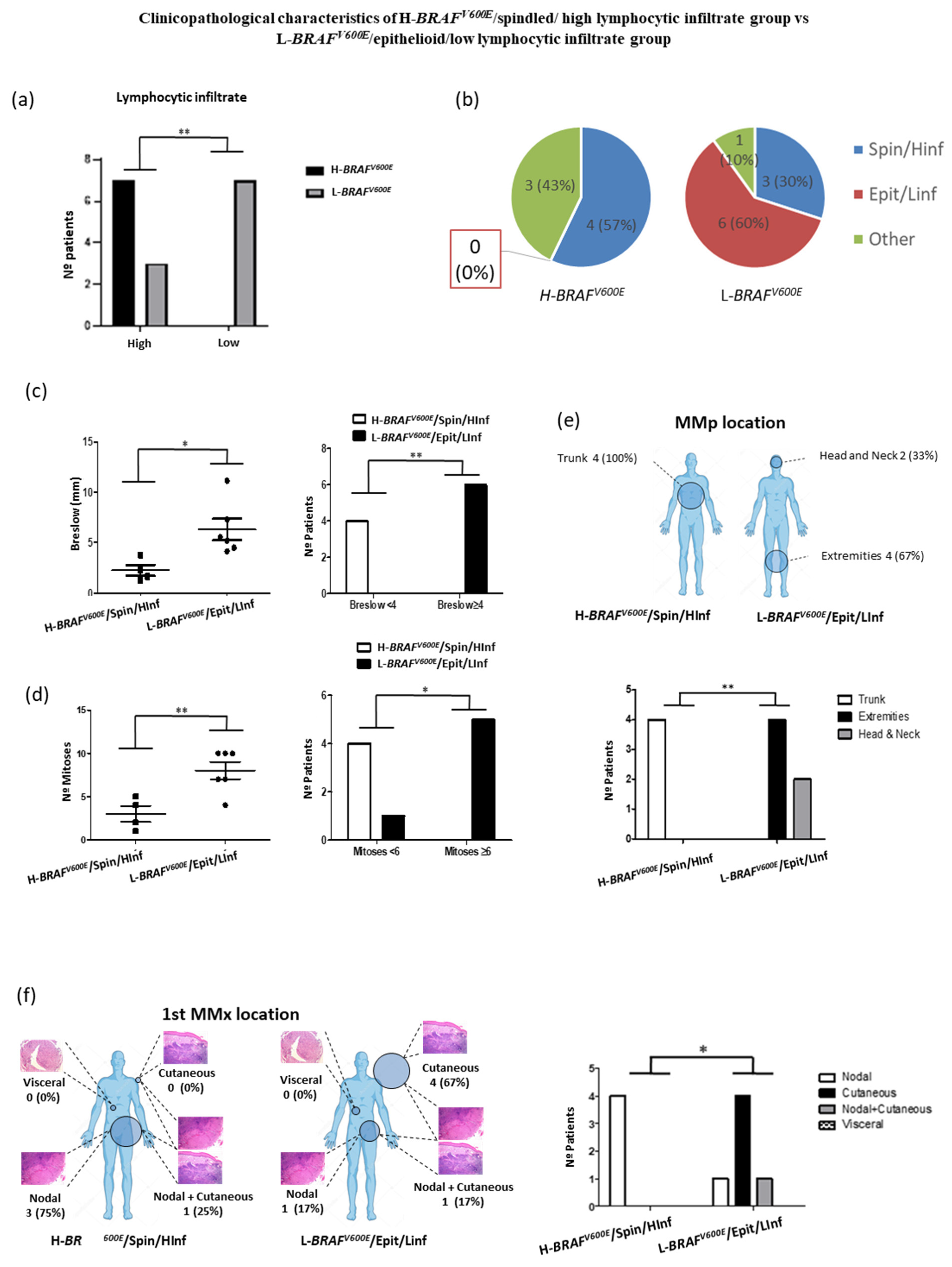
3.4.2. Demographic, Clinical and Tumor Characteristics of H-BRAFV600E/Spindled/ High Lymphocytic Infiltrate Group vs. L-BRAFV600E/Epithelioid/Low Lymphocytic Infiltrate Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma Staging: Evidence-Based Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaherty, K.T.; Hodi, F.S.; Fisher, D.E. From Genes to Drugs: Targeted Strategies for Melanoma. Nat. Rev. Cancer 2012, 12, 349–361. [Google Scholar] [CrossRef]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF Gene in Human Cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Akbani, R.; Akdemir, K.C.; Aksoy, B.A.; Albert, M.; Ally, A.; Amin, S.B.; Arachchi, H.; Arora, A.; Auman, J.T.; Ayala, B.; et al. Genomic Classification of Cutaneous Melanoma. Cell 2015, 161, 1681–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menzies, A.M.; Haydu, L.E.; Visintin, L.; Carlino, M.S.; Howle, J.R.; Thompson, J.F.; Kefford, R.F.; Scolyer, R.A.; Long, G.V. Distinguishing Clinicopathologic Features of Patients with V600E and V600K BRAF -Mutant Metastatic Melanoma. Clin. Cancer Res. 2012, 18, 3242–3249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siroy, A.E.; Boland, G.M.; Milton, D.R.; Roszik, J.; Frankian, S.; Malke, J.; Haydu, L.; Prieto, V.G.; Tetzlaff, M.; Ivan, D.; et al. Beyond BRAF V600: Clinical Mutation Panel Testing by Next-Generation Sequencing in Advanced Melanoma. J. Investig. Dermatol. 2015, 135, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Kuo, H.; Li, W.-Q.; Canales, A.L.; Han, J.; Qureshi, A.A. Association between BRAF V600E and NRAS Q61R Mutations and Clinicopathologic Characteristics, Risk Factors and Clinical Outcome of Primary Invasive Cutaneous Melanoma. Cancer Causes Control 2014, 25, 1379–1386. [Google Scholar] [CrossRef] [Green Version]
- Elder, D.E.; Bastian, B.C.; Cree, I.A.; Massi, D.; Scolyer, R.A. The 2018 World Health Organization Classification of Cutaneous, Mucosal, and Uveal Melanoma: Detailed Analysis of 9 Distinct Subtypes Defined by Their Evolutionary Pathway. Arch. Pathol. Lab. Med. 2020, 144, 500–522. [Google Scholar] [CrossRef] [Green Version]
- Chiappetta, C.; Proietti, I.; Soccodato, V.; Puggioni, C.; Zaralli, R.; Pacini, L.; Porta, N.; Skroza, N.; Petrozza, V.; Potenza, C.; et al. BRAF and NRAS Mutations Are Heterogeneous and Not Mutually Exclusive in Nodular Melanoma. Appl. Immunohistochem. Mol. Morphol. 2015, 23, 172–177. [Google Scholar] [CrossRef] [Green Version]
- Shtivelman, E.; Davies, M.A.; Hwu, P.; Yang, J.; Lotem, M.; Oren, M.; Flaherty, K.T.; Fisher, D.E. Pathways and Therapeutic Targets in Melanoma. Oncotarget 2014, 5, 1701–1752. [Google Scholar] [CrossRef] [Green Version]
- Savoia, P.; Fava, P.; Casoni, F.; Cremona, O. Targeting the ERK Signaling Pathway in Melanoma. Int. J. Mol. Sci. 2019, 20, 1483. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Liu, W.-Z.; Liu, T.; Feng, X.; Yang, N.; Zhou, H.-F. Signaling Pathway of MAPK/ERK in Cell Proliferation, Differentiation, Migration, Senescence and Apoptosis. J. Recept. Signal Transduct. Res. 2015, 35, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Tétu, P.; Baroudjian, B.; Lebbe, C. Targeting BRAF and MEK Inhibitors in Melanoma in the Metastatic, Neoadjuvant and Adjuvant Setting. Curr. Opin. Oncol. 2020, 32, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Czarnecka, A.M.; Bartnik, E.; Fiedorowicz, M.; Rutkowski, P. Targeted Therapy in Melanoma and Mechanisms of Resistance. Int. J. Mol. Sci. 2020, 21, 4576. [Google Scholar] [CrossRef]
- Sevilla, A.; Morales, M.C.; Ezkurra, P.A.; Rasero, J.; Velasco, V.; Cancho-Galan, G.; Sánchez-Diez, A.; Mujika, K.; Penas, C.; Smith, I.; et al. BRAF V600E Mutational Load as a Prognosis Biomarker in Malignant Melanoma. PLoS ONE 2020, 15, e0230136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breslow, A. Thickness, Cross-Sectional Areas and Depth of Invasion in the Prognosis of Cutaneous Melanoma. Ann. Surg. 1970, 172, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Gimotty, P.A.; Elder, D.E.; Fraker, D.L.; Botbyl, J.; Sellers, K.; Elenitsas, R.; Ming, M.E.; Schuchter, L.; Spitz, F.R.; Czerniecki, B.J.; et al. Identification of High-Risk Patients Among Those Diagnosed With Thin Cutaneous Melanomas. JCO 2007, 25, 1129–1134. [Google Scholar] [CrossRef]
- Balch, C.M.; Murad, T.M.; Soong, S.J.; Ingalls, A.L.; Halpern, N.B.; Maddox, W.A. A Multifactorial Analysis of Melanoma: Prognostic histopathological features comparing Clark’s and Breslow’s staging methods. Ann. Surg. 1978, 188, 732–742. [Google Scholar] [CrossRef]
- Green, A.C.; Baade, P.; Coory, M.; Aitken, J.F.; Smithers, M. Population-Based 20-Year Survival Among People Diagnosed With Thin Melanomas in Queensland, Australia. JCO 2012, 30, 1462–1467. [Google Scholar] [CrossRef] [Green Version]
- Piñero-Madrona, A.; Ruiz-Merino, G.; Cerezuela Fuentes, P.; Martínez-Barba, E.; Rodríguez-López, J.N.; Cabezas-Herrera, J. Mitotic Rate as an Important Prognostic Factor in Cutaneous Malignant Melanoma. Clin. Transl. Oncol. 2019, 21, 1348–1356. [Google Scholar] [CrossRef]
- Mandalà, M.; Galli, F.; Cattaneo, L.; Merelli, B.; Rulli, E.; Ribero, S.; Quaglino, P.; De Giorgi, V.; Pigozzo, J.; Sileni, V.C.; et al. Mitotic Rate Correlates with Sentinel Lymph Node Status and Outcome in Cutaneous Melanoma Greater than 1 Millimeter in Thickness: A Multi-Institutional Study of 1524 Cases. J. Am. Acad. Dermatol. 2017, 76, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.L.; Vidri, R.J.; MacGillivray, D.C.; Fitzgerald, T.L. Tumor Mitotic Rate Is an Independent Predictor of Survival for Nonmetastatic Melanoma. Surgery 2018, 164, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Satzger, I.; Marks, L.; Kerick, M.; Klages, S.; Berking, C.; Herbst, R.; Völker, B.; Schacht, V.; Timmermann, B.; Gutzmer, R. Allele Frequencies of BRAF V600 Mutations in Primary Melanomas and Matched Metastases and Their Relevance for BRAF Inhibitor Therapy in Metastatic Melanoma. Oncotarget 2015, 6, 37895–37905. [Google Scholar] [CrossRef] [Green Version]
- Lebbé, C.; How-Kit, A.; Battistella, M.; Sadoux, A.; Podgorniak, M.-P.; Sidina, I.; Pages, C.; Roux, J.; Porcher, R.; Tost, J.; et al. BRAF V600 Mutation Levels Predict Response to Vemurafenib in Metastatic Melanoma. Melanoma Res. 2014, 24, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Stagni, C.; Zamuner, C.; Elefanti, L.; Zanin, T.; Bianco, P.D.; Sommariva, A.; Fabozzi, A.; Pigozzo, J.; Mocellin, S.; Montesco, M.C.; et al. BRAF Gene Copy Number and Mutant Allele Frequency Correlate with Time to Progression in Metastatic Melanoma Patients Treated with MAPK Inhibitors. Mol. Cancer Ther. 2018, 17, 1332–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berrino, E.; Balsamo, A.; Pisacane, A.; Gallo, S.; Becco, P.; Miglio, U.; Caravelli, D.; Poletto, S.; Paruzzo, L.; Debernardi, C.; et al. High BRAF Variant Allele Frequencies Are Associated with Distinct Pathological Features and Responsiveness to Target Therapy in Melanoma Patients. ESMO Open 2021, 6, 100133. [Google Scholar] [CrossRef] [PubMed]
- Serratì, S.; De Summa, S.; Pilato, B.; Petriella, D.; Lacalamita, R.; Tommasi, S.; Pinto, R. Next-Generation Sequencing: Advances and Applications in Cancer Diagnosis. OTT 2016, 9, 7355–7365. [Google Scholar] [CrossRef] [Green Version]
- Slatko, B.E.; Gardner, A.F.; Ausubel, F.M. Overview of Next-Generation Sequencing Technologies. Curr. Protoc. Mol. Biol. 2018, 122, e59. [Google Scholar] [CrossRef] [PubMed]
- Mejbel, H.A.; Arudra, S.K.C.; Pradhan, D.; Torres-Cabala, C.A.; Nagarajan, P.; Tetzlaff, M.T.; Curry, J.L.; Ivan, D.; Duose, D.Y.; Luthra, R.; et al. Immunohistochemical and Molecular Features of Melanomas Exhibiting Intratumor and Intertumor Histomorphologic Heterogeneity. Cancers 2019, 11, 1714. [Google Scholar] [CrossRef] [Green Version]
- Maiques, O.; Macià, A.; Moreno, S.; Barceló, C.; Santacana, M.; Vea, A.; Herreros, J.; Gatius, S.; Ortega, E.; Valls, J.; et al. Immunohistochemical Analysis of T-Type Calcium Channels in Acquired Melanocytic Naevi and Melanoma. Br. J. Dermatol. 2017, 176, 1247–1258. [Google Scholar] [CrossRef] [Green Version]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open Source Software for Digital Pathology Image Analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [Green Version]
- Grzywa, T.M.; Paskal, W.; Włodarski, P.K. Intratumor and Intertumor Heterogeneity in Melanoma. Transl. Oncol. 2017, 10, 956–975. [Google Scholar] [CrossRef]
- McGranahan, N.; Swanton, C. Clonal Heterogeneity and Tumor Evolution: Past, Present, and the Future. Cell 2017, 168, 613–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksson, H.; Zebary, A.; Vassilaki, I.; Omholt, K.; Ghaderi, M.; Hansson, J. BRAF V600E Protein Expression in Primary Cutaneous Malignant Melanomas and Paired Metastases. JAMA Dermatol. 2015, 151, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verlinden, I.; van den Hurk, K.; Clarijs, R.; Willig, A.P.; Stallinga, C.M.H.A.; Roemen, G.M.J.M.; van den Oord, J.J.; zur Hausen, A.; Speel, E.-J.M.; Winnepenninckx, V.J.L. BRAFV600E Immunopositive Melanomas Show Low Frequency of Heterogeneity and Association With Epithelioid Tumor Cells: A STROBE-Compliant Article. Medicine 2014, 93, e285. [Google Scholar] [CrossRef]
- Tetzlaff, M.T.; Pattanaprichakul, P.; Wargo, J.; Fox, P.S.; Patel, K.P.; Estrella, J.S.; Broaddus, R.R.; Williams, M.D.; Davies, M.A.; Routbort, M.J.; et al. Utility of BRAF V600E Immunohistochemistry Expression Pattern as a Surrogate of BRAF Mutation Status in 154 Patients with Advanced Melanoma. Hum. Pathol. 2015, 46, 1101–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, I.P.; Salhi, A.; Giles, K.M.; Vogelsang, M.; Han, S.W.; Ismaili, N.; Lui, K.P.; Robinson, E.M.; Wilson, M.A.; Shapiro, R.L.; et al. Identification of a Novel Pathogenic Germline KDR Variant in Melanoma. Clin. Cancer Res. 2016, 22, 2377–2385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omholt, K.; Platz, A.; Kanter, L.; Ringborg, U.; Hansson, J. NRAS and BRAF Mutations Arise Early during Melanoma Pathogenesis and Are Preserved throughout Tumor Progression. Clin. Cancer Res. 2003, 9, 6483–6488. [Google Scholar]
- Edlundh-Rose, E.; Egyha, S.; Omholt, K.; Mansson-Brahme, E.; Platz, A.; Hansson, J.; Lundeberg, J. NRAS and BRAF Mutations in Melanoma Tumours in Relation to Clinical Characteristics: A Study Based on Mutation Screening by Pyrosequencing. Melanoma Res. 2006, 16, 471–478. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, S.N.; Hahn, H.J.; Lee, Y.W.; Choe, Y.B.; Ahn, K.J. Metaanalysis of BRAF Mutations and Clinicopathologic Characteristics in Primary Melanoma. J. Am. Acad. Dermatol. 2015, 72, 1036–1046. [Google Scholar] [CrossRef]
- Lopez-Martin, J.A.; Arance Fernández, A.; Ríos-Martín, J.J.; Hernández-Losa, J.; Alós Hernández, L.; Cerezuela Fuentes, P.; Ortiz Reina, S.; Ortega Izquierdo, E.; Martí, R.M.; Soberino García, J.; et al. Frequency and Clinicopathological Profile Associated with Braf Mutations in Patients with Advanced Melanoma in Spain. Transl. Oncol. 2020, 13, 100750. [Google Scholar] [CrossRef]
- Lee, J.-H.; Choi, J.-W.; Kim, Y.-S. Frequencies of BRAF and NRAS Mutations Are Different in Histological Types and Sites of Origin of Cutaneous Melanoma: A Meta-Analysis: BRAF and NRAS Mutations in Melanoma. Br. J. Dermatol. 2011, 164, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Saldanha, G.; Potter, L.; DaForno, P.; Pringle, J.H. Cutaneous Melanoma Subtypes Show Different BRAF and NRAS Mutation Frequencies. Clin. Cancer Res. 2006, 12, 4499–4505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Castañeda, L.D.; Nova, J.A.; Tovar-Parra, J.D. Frequency of Mutations in BRAF, NRAS, and KIT in Different Populations and Histological Subtypes of Melanoma: A Systemic Review. Melanoma Res. 2020, 30, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.-L.; Zhou, L.; Sadri, N. Comparison of Targeted next Generation Sequencing (NGS) versus Isolated BRAF V600E Analysis in Patients with Metastatic Melanoma. Virchows Arch. 2018, 473, 371–377. [Google Scholar] [CrossRef]
- Menzies, A.M.; Lum, T.; Wilmott, J.S.; Hyman, J.; Kefford, R.F.; Thompson, J.F.; O’Toole, S.; Long, G.V.; Scolyer, R.A. Intrapatient Homogeneity of BRAFV600E Expression in Melanoma. Am. J. Surg. Pathol. 2014, 38, 377–382. [Google Scholar] [CrossRef]
- Bann, D.V.; Chaikhoutdinov, I.; Zhu, J.; Andrews, G. Satellite and In-Transit Metastatic Disease in Melanoma Skin Cancer: A Retrospective Review of Disease Presentation, Treatment, and Outcomes. Dermatol. Surg. 2019, 45, 371–380. [Google Scholar] [CrossRef]
- Testori, A.; Ribero, S.; Bataille, V. Diagnosis and Treatment of In-Transit Melanoma Metastases. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 544–560. [Google Scholar] [CrossRef]
- Azimi, F.; Scolyer, R.A.; Rumcheva, P.; Moncrieff, M.; Murali, R.; McCarthy, S.W.; Saw, R.P.; Thompson, J.F. Tumor-Infiltrating Lymphocyte Grade Is an Independent Predictor of Sentinel Lymph Node Status and Survival in Patients With Cutaneous Melanoma. JCO 2012, 30, 2678–2683. [Google Scholar] [CrossRef]
- Thomas, N.E.; Busam, K.J.; From, L.; Kricker, A.; Armstrong, B.K.; Anton-Culver, H.; Gruber, S.B.; Gallagher, R.P.; Zanetti, R.; Rosso, S.; et al. Tumor-Infiltrating Lymphocyte Grade in Primary Melanomas Is Independently Associated With Melanoma-Specific Survival in the Population-Based Genes, Environment and Melanoma Study. JCO 2013, 31, 4252–4259. [Google Scholar] [CrossRef] [Green Version]
- Fu, Q.; Chen, N.; Ge, C.; Li, R.; Li, Z.; Zeng, B.; Li, C.; Wang, Y.; Xue, Y.; Song, X.; et al. Prognostic Value of Tumor-Infiltrating Lymphocytes in Melanoma: A Systematic Review and Meta-Analysis. OncoImmunology 2019, 8, e1593806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Hernandez, I.; Maiques, O.; Kohlhammer, L.; Cantelli, G.; Perdrix-Rosell, A.; Monger, J.; Fanshawe, B.; Bridgeman, V.L.; Karagiannis, S.N.; Penin, R.M.; et al. WNT11-FZD7-DAAM1 Signalling Supports Tumour Initiating Abilities and Melanoma Amoeboid Invasion. Nat. Commun. 2020, 11, 5315. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Number (Percentage/Range) |
|---|---|
| Male | 16 (67%) |
| Female | 8 (33%) |
| Median age | 63yo (24–87) |
| MM subtype | |
| SSM | 14 (58%) |
| NM | 10 (42%) |
| MMp location | |
| Trunk | 11 (50%) |
| Lower extremities | 6 (25%) |
| Upper extremities | 3 (12.5%) |
| Head and neck | 3 (12.5%) |
| Mean Breslow | 4.22 mm (1.04–13.50) |
| Mean Clark | 4 (3–5) |
| Ulceration | |
| Yes | 14 (58%) |
| No | 10 (42%) |
| Mean mitotic index | 5 mitoses/cm2 (1–11) |
| MMx location | |
| Cutaneous | 27 (51.92%) |
| Nodal | 13 (25%) |
| CNS | 3 (5.77%) |
| Lung | 2 (3.85%) |
| Suprarenal | 2 (3.85%) |
| Muscular | 2 (3.85%) |
| Parotid | 1 (1.92%) |
| Live status | |
| Alive | 8 (33.3%) |
| Dead | 16 (66.7) |
| Mean survival | 69 months (median 40.5 (9–177)) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soria, X.; Vilardell, F.; Maiques, Ó.; Barceló, C.; Sisó, P.; de la Rosa, I.; Velasco, A.; Cuevas, D.; Santacana, M.; Gatius, S.; et al. BRAFV600E Mutant Allele Frequency (MAF) Influences Melanoma Clinicopathologic Characteristics. Cancers 2021, 13, 5073. https://doi.org/10.3390/cancers13205073
Soria X, Vilardell F, Maiques Ó, Barceló C, Sisó P, de la Rosa I, Velasco A, Cuevas D, Santacana M, Gatius S, et al. BRAFV600E Mutant Allele Frequency (MAF) Influences Melanoma Clinicopathologic Characteristics. Cancers. 2021; 13(20):5073. https://doi.org/10.3390/cancers13205073
Chicago/Turabian StyleSoria, Xavier, Felip Vilardell, Óscar Maiques, Carla Barceló, Pol Sisó, Inés de la Rosa, Ana Velasco, Dolors Cuevas, Maria Santacana, Sònia Gatius, and et al. 2021. "BRAFV600E Mutant Allele Frequency (MAF) Influences Melanoma Clinicopathologic Characteristics" Cancers 13, no. 20: 5073. https://doi.org/10.3390/cancers13205073
APA StyleSoria, X., Vilardell, F., Maiques, Ó., Barceló, C., Sisó, P., de la Rosa, I., Velasco, A., Cuevas, D., Santacana, M., Gatius, S., Matías-Guiu, X., Rodrigo, A., Macià, A., & Martí, R. M. (2021). BRAFV600E Mutant Allele Frequency (MAF) Influences Melanoma Clinicopathologic Characteristics. Cancers, 13(20), 5073. https://doi.org/10.3390/cancers13205073