
Cladribine Combined with Low-Dose Cytarabine as Frontline Treatment for Unfit Elderly Acute Myeloid Leukemia Patients: Results from a Prospective Multicenter Study of Polish Adult Leukemia Group (PALG)

 , , , , , ,
, , , , , ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Human Subjects Considerations
2.2. Treatment Regimen
2.3. Study Procedures
2.4. Endpoints
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Efficacy
3.2.1. Response
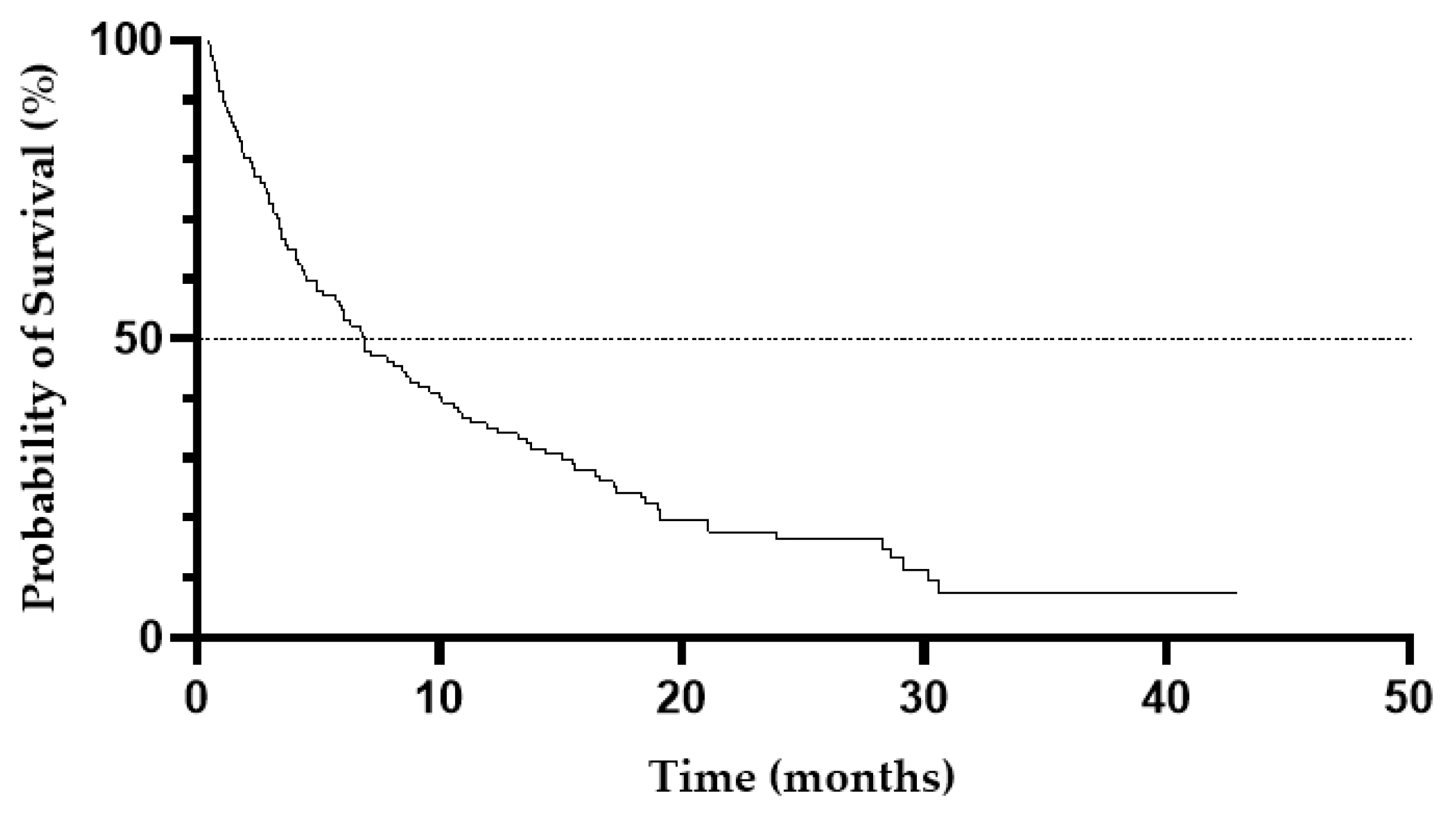
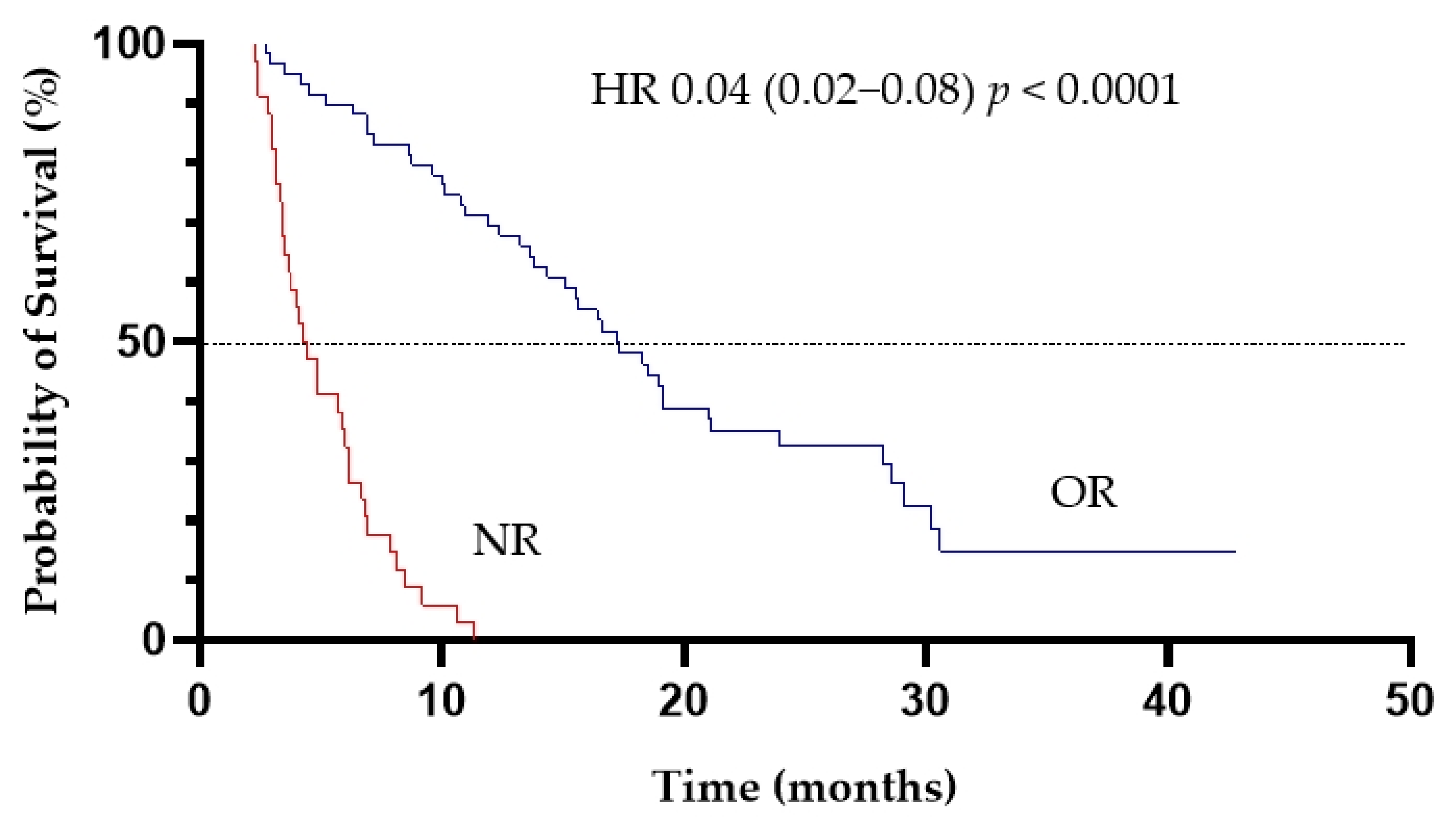
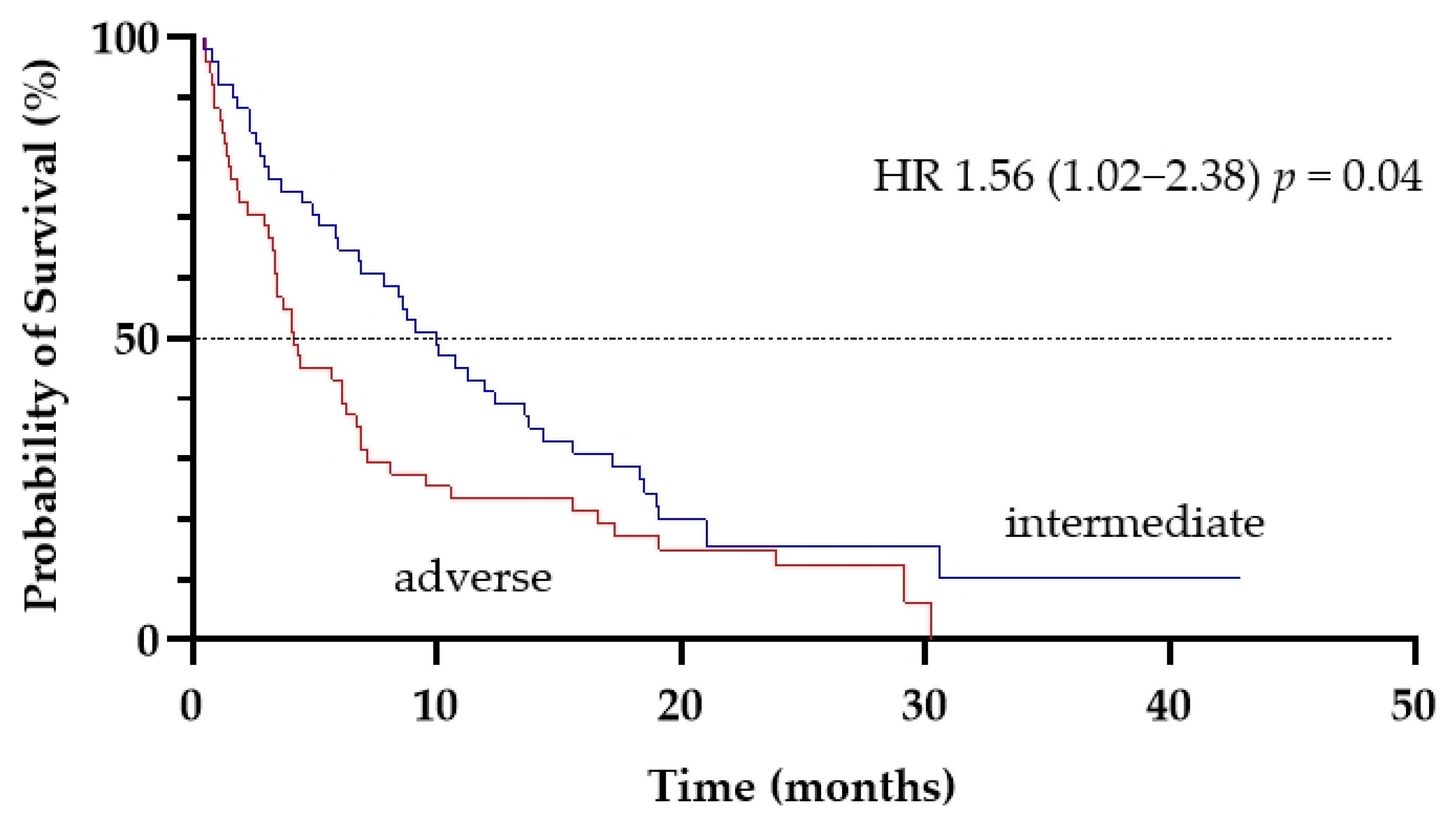
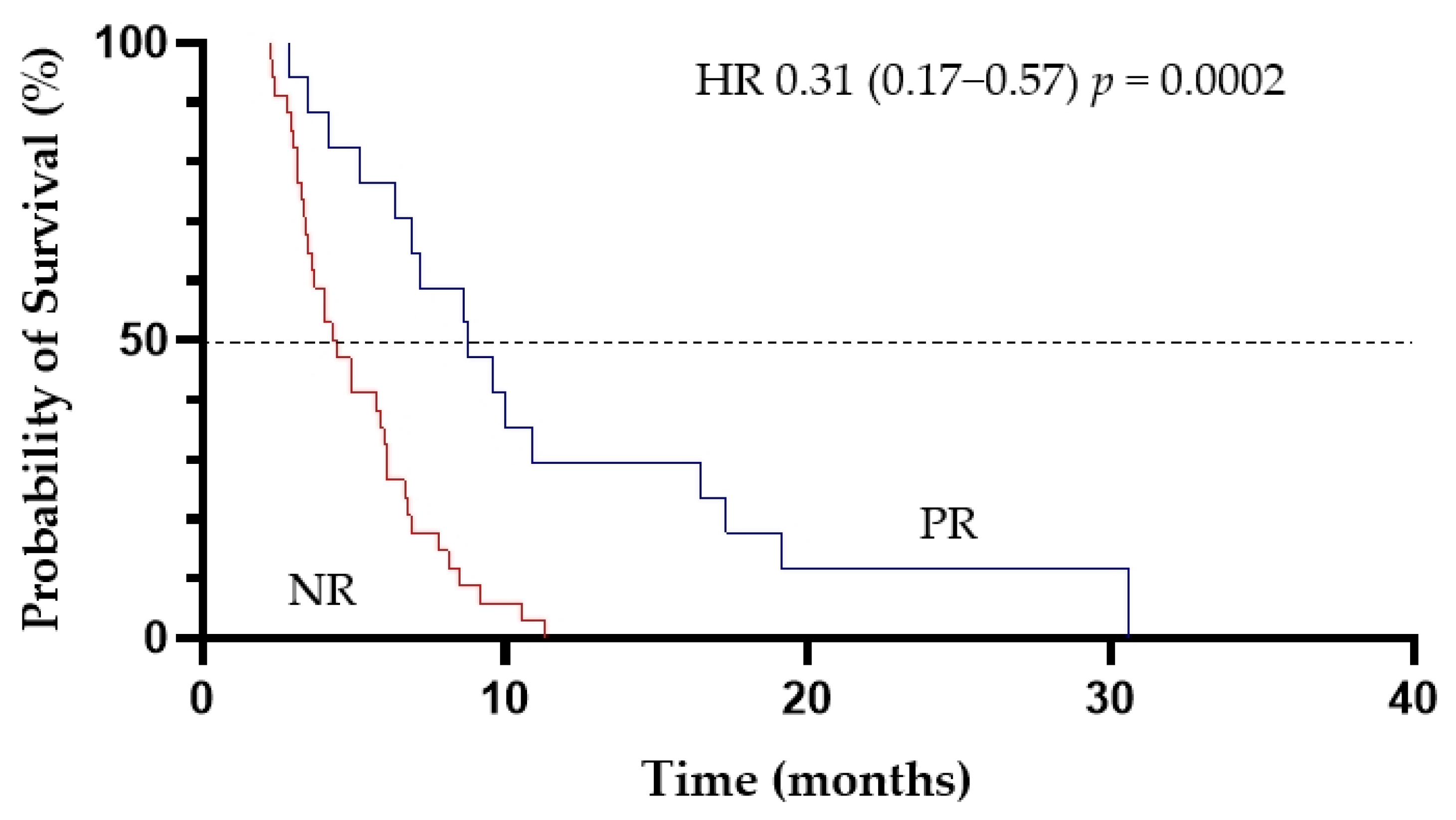
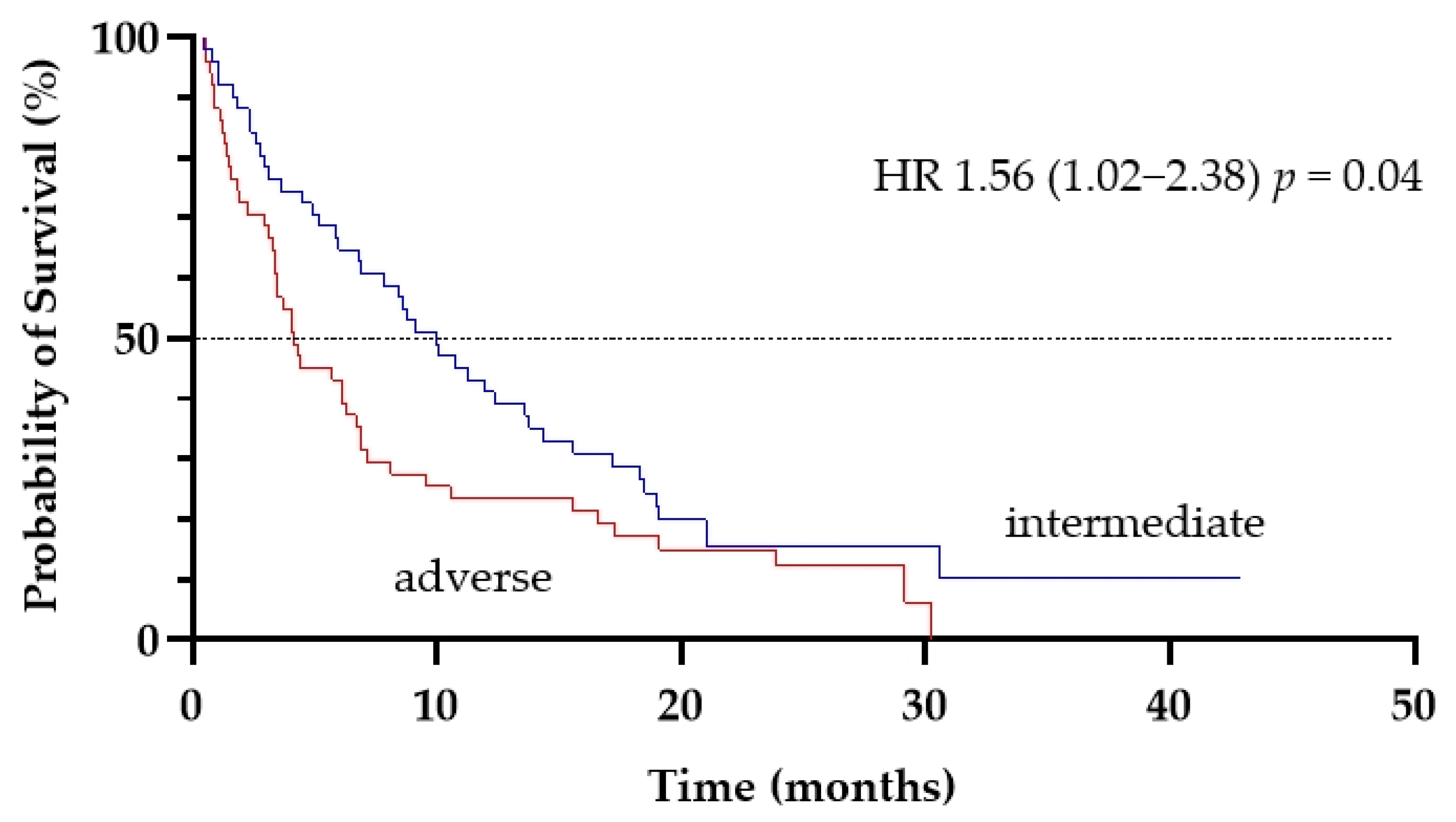
3.2.2. Survival
3.2.3. Safety Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Acute Myeloid Leukemia—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/amyl.html (accessed on 11 April 2021).
- Ross, K.; Gillespie-Twardy, A.L.; Agha, M.; Raptis, A.; Hou, J.Z.; Farah, R.; Redner, R.L.; Im, A.; Duggal, S.; Ding, F.; et al. Intensive Chemotherapy in Patients Aged 70 Years or Older Newly Diagnosed with Acute Myeloid Leukemia. Oncol. Res. 2015, 22, 85–92. [Google Scholar] [CrossRef]
- Appelbaum, F.R.; Gundacker, H.; Head, D.R.; Slovak, M.L.; Willman, C.L.; Godwin, J.E.; Anderson, J.E.; Petersdorf, S.H. Age and Acute Myeloid Leukemia. Blood 2006, 107, 3481–3485. [Google Scholar] [CrossRef] [PubMed]
- Tallman, M.S.; Wang, E.S.; Altman, J.K.; Appelbaum, F.R.; Bhatt, V.R.; Bixby, D.; Coutre, S.E.; De Lima, M.; Fathi, A.T.; Fiorella, M.; et al. Acute Myeloid Leukemia, Version 3.2019. JNCCN J. Natl. Compr. Cancer Netw. 2019, 17, 721–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimwade, D.; Walker, H.; Harrison, G.; Oliver, F.; Chatters, S.; Harrison, C.J.; Wheatley, K.; Burnett, A.K.; Goldstone, A.H. The Predictive Value of Hierarchical Cytogenetic Classification in Older Adults with Acute Myeloid Leukemia (AML): Analysis of 1065 Patients Entered into the United Kingdom Medical Research Council AML11 Trial. Blood 2001, 98, 1312–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, A.V.; Valk, P.J.M.; Metzeler, K.H.; Acharya, C.R.; Tuchman, S.A.; Stevenson, M.M.; Rizzieri, D.A.; Delwel, R.; Buske, C.; Bohlander, S.K.; et al. Age-Specific Differences in Oncogenic Pathway Dysregulation and Anthracycline Sensitivity in Patients with Acute Myeloid Leukemia. J. Clin. Oncol. 2009, 27, 5580–5586. [Google Scholar] [CrossRef] [PubMed]
- Prassek, V.V.; Rothenberg-Thurley, M.; Sauerland, M.C.; Herold, T.; Janke, H.; Ksienzyk, B.; Konstandin, N.P.; Goerlich, D.; Krug, U.; Faldum, A.; et al. Genetics of Acute Myeloid Leukemia in the Elderly: Mutation Spectrum and Clinical Impact in Intensively Treated Patients Aged 75 Years or Older. Haematologica 2018, 103, 1853–1861. [Google Scholar] [CrossRef] [Green Version]
- Oran, B.; Weisdorf, D.J. Survival for Older Patients with Acute Myeloid Leukemia: A Population-Based Study. Haematologica 2012, 97, 1916–1924. [Google Scholar] [CrossRef]
- Lowenberg, B.; Zittoun, R.; Kerkhofs, H.; Jehn, U.; Abels, J.; Debusscher, L.; Cauchie, C.; Peetermans, M.; Solbu, G.; Suciu, S.; et al. On the Value of Intensive Remission-Induction Chemotherapy in Elderly Patients of 65+ Years with Acute Myeloid Leukemia: A Randomized Phase III Study of the European Organization for Research and Treatment of Cancer Leukemia Group. J. Clin. Oncol. 1989, 7, 1268–1274. [Google Scholar] [CrossRef]
- Juliusson, G.; Antunovic, P.; Derolf, Å.; Lehmann, S.; Möllgård, L.; Stockelberg, D.; Tidefelt, U.; Wahlin, A.; Höglund, M. Age and Acute Myeloid Leukemia: Real World Data on Decision to Treat and Outcomes from the Swedish Acute Leukemia Registry. Blood 2009, 113, 4179–4187. [Google Scholar] [CrossRef] [Green Version]
- Klepin, H.D.; Geiger, A.M.; Tooze, J.A.; Kritchevsky, S.B.; Williamson, J.D.; Pardee, T.S.; Ellis, L.R.; Powell, B.L. Geriatric Assessment Predicts Survival for Older Adults Receiving Induction Chemotherapy for Acute Myelogenous Leukemia. Blood 2013, 121, 4287–4294. [Google Scholar] [CrossRef] [PubMed]
- Sherman, A.E.; Motyckova, G.; Fega, K.R.; DeAngelo, D.J.; Abel, G.A.; Steensma, D.; Wadleigh, M.; Stone, R.M.; Driver, J.A. Geriatric Assessment in Older Patients with Acute Myeloid Leukemia: A Retrospective Study of Associated Treatment and Outcomes. Leuk. Res. 2013, 37, 998–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savic, A.; Kvrgic, V.; Rajic, N.; Urosevic, I.; Kovacevic, D.; Percic, I.; Popovic, S. The Hematopoietic Cell Transplantation Comorbidity Index Is a Predictor of Early Death and Survival in Adult Acute Myeloid Leukemia Patients. Leuk. Res. 2012, 36, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Giles, F.J.; Borthakur, G.; Ravandi, F.; Faderl, S.; Verstovsek, S.; Thomas, D.; Wierda, W.; Ferrajoli, A.; Kornblau, S.; Pierce, S.; et al. The Haematopoietic Cell Transplantation Comorbidity Index Score Is Predictive of Early Death and Survival in Patients over 60 Years of Age Receiving Induction Therapy for Acute Myeloid Leukaemia. Br. J. Haematol. 2007, 136, 624–627. [Google Scholar] [CrossRef]
- Sorror, M.L.; Storer, B.E.; Fathi, A.T.; Gerds, A.T.; Medeiros, B.C.; Shami, P.; Brunner, A.M.; Sekeres, M.A.; Mukherjee, S.; Peña, E.; et al. Development and Validation of a Novel Acute Myeloid Leukemia-Composite Model to Estimate Risks of Mortality. JAMA Oncol. 2017, 3, 1675–1682. [Google Scholar] [CrossRef] [PubMed]
- Walter, R.B.; Othus, M.; Borthakur, G.; Ravandi, F.; Cortes, J.E.; Pierce, S.A.; Appelbaum, F.R.; Kantarjian, H.A.; Estey, E.H. Prediction of Early Death after Induction Therapy for Newly Diagnosed Acute Myeloid Leukemia with Pretreatment Risk Scores: A Novel Paradigm for Treatment Assignment. J. Clin. Oncol. 2011, 29, 4417–4423. [Google Scholar] [CrossRef] [PubMed]
- Krug, U.; Röllig, C.; Koschmieder, A.; Heinecke, A.; Sauerland, M.C.; Schaich, M.; Thiede, C.; Kramer, M.; Braess, J.; Spiekermann, K.; et al. Complete Remission and Early Death after Intensive Chemotherapy in Patients Aged 60 Years or Older with Acute Myeloid Leukaemia: A Web-Based Application for Prediction of Outcomes. Lancet 2010, 376, 2000–2008. [Google Scholar] [CrossRef]
- Sekeres, M.A.; Guyatt, G.; Abel, G.; Alibhai, S.; Altman, J.K.; Buckstein, R.; Choe, H.; Desai, P.; Erba, H.; Hourigan, C.S.; et al. American Society of Hematology 2020 Guidelines for Treating Newly Diagnosed Acute Myeloid Leukemia in Older Adults. Blood Adv. 2020, 4, 3528–3549. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, B.C.; Satram-Hoang, S.; Hurst, D.; Hoang, K.Q.; Momin, F.; Reyes, C. Big Data Analysis of Treatment Patterns and Outcomes among Elderly Acute Myeloid Leukemia Patients in the United States. Ann. Hematol. 2015, 94, 1127–1138. [Google Scholar] [CrossRef] [Green Version]
- Dombret, H.; Seymour, J.F.; Butrym, A.; Wierzbowska, A.; Selleslag, D.; Jang, J.H.; Kumar, R.; Cavenagh, J.; Schuh, A.C.; Candoni, A.; et al. International Phase 3 Study of Azacitidine vs. Conventional Care Regimens in Older Patients with Newly Diagnosed AML with >30% Blasts. Blood 2015, 126, 291–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thépot, S.; Itzykson, R.; Seegers, V.; Recher, C.; Raffoux, E.; Quesnel, B.; Delaunay, J.; Cluzeau, T.; Koka, A.M.; Stamatoullas, A.; et al. Azacitidine in Untreated Acute Myeloid Leukemia: A Report on 149 Patients. Am. J. Hematol. 2014, 89, 410–416. [Google Scholar] [CrossRef]
- Maurillo, L.; Venditti, A.; Spagnoli, A.; Gaidano, G.; Ferrero, D.; Oliva, E.; Lunghi, M.; D’Arco, A.M.; Levis, A.; Pastore, D.; et al. Azacitidine for the Treatment of Patients with Acute Myeloid Leukemia: Report of 82 Patients Enrolled in an Italian Compassionate Program. Cancer 2012, 118, 1014–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Ali, H.K.; Jaekel, N.; Junghanss, C.; Maschmeyer, G.; Krahl, R.; Cross, M.; Hoppe, G.; Niederwieser, D. Azacitidine in Patients with Acute Myeloid Leukemia Medically Unfit for or Resistant to Chemotherapy: A Multicenter Phase I/II Study. Leuk. Lymphoma 2012, 53, 110–117. [Google Scholar] [CrossRef]
- Kantarjian, H.M.; Thomas, X.G.; Dmoszynska, A.; Wierzbowska, A.; Mazur, G.; Mayer, J.; Gau, J.P.; Chou, W.C.; Buckstein, R.; Cermak, J.; et al. Multicenter, Randomized, Open-Label, Phase III Trial of Decitabine versus Patient Choice, with Physician Advice, of Either Supportive Care or Low-Dose Cytarabine for the Treatment of Older Patients with Newly Diagnosed Acute Myeloid Leukemia. J. Clin. Oncol. 2012, 30, 2670–2677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lübbert, M.; Rüter, B.H.; Claus, R.; Schmoor, C.; Schmid, M.; Germing, U.; Kuendgen, A.; Rethwisch, V.; Ganser, A.; Platzbecker, U.; et al. A Multicenter Phase II Trial of Decitabine as First-Line Treatment for Older Patients with Acute Myeloid Leukemia Judged Unfit for Induction Chemotherapy. Haematologica 2012, 97, 393–401. [Google Scholar] [CrossRef]
- Cashen, A.F.; Schiller, G.J.; O’Donnell, M.R.; DiPersio, J.F. Multicenter, Phase II Study of Decitabine for the First-Line Treatment of Older Patients with Acute Myeloid Leukemia. J. Clin. Oncol. 2010, 28, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Freyer, C.; Gupta, N.; Wetzler, M.; Wang, E. Revisiting the Role of Cladribine in Acute Myeloid Leukemia: An Improvement on Past Accomplishments or More Old News? Am. J. Hematol. 2015, 90, 62–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molica, M.; Breccia, M.; Capria, S.; Trisolini, S.; Foa, R.; Jabbour, E.; Kadia, T.M. The Role of Cladribine in Acute Myeloid Leukemia: An Old Drug up to New Tricks. Leuk. Lymphoma 2020, 61, 536–545. [Google Scholar] [CrossRef]
- Bertacchini, J.; Frasson, C.; Chiarini, F.; D’Avella, D.; Accordi, B.; Anselmi, L.; Barozzi, P.; Forghieri, F.; Luppi, M.; Martelli, A.; et al. Dual Inhibition of PI3K/MTOR Signaling in Chemoresistant AML Primary Cells. Adv. Biol. Regul. 2018, 68, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Holowiecki, J.; Grosicki, S.; Robak, T.; Kyrcz-Krzemien, S.; Giebel, S.; Hellmann, A.; Skotnicki, A.; Jedrzejczak, W.W.; Konopka, L.; Kuliczkowski, K.; et al. Addition of Cladribine to Daunorubicin and Cytarabine Increases Complete Remission Rate after a Single Course of Induction Treatment in Acute Myeloid Leukemia. Multicenter, Phase III Study. Leukemia 2004, 18, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Holowiecki, J.; Grosicki, S.; Giebel, S.; Robak, T.; Kyrcz-Krzemien, S.; Kuliczkowski, K.; Skotnicki, A.B.; Hellmann, A.; Sulek, K.; Dmoszynska, A.; et al. Cladribine, but Not Fludarabine, Added to Daunorubicin and Cytarabine during Induction Prolongs Survival of Patients with Acute Myeloid Leukemia: A Multicenter, Randomizedphase III Study. J. Clin. Oncol. 2012, 30, 2441–2448. [Google Scholar] [CrossRef]
- Zhou, A.; Han, Q.; Song, H.; Zi, J.; Ma, J.; Ge, Z. Efficacy and Toxicity of Cladribine for the Treatment of Refractory Acute Myeloid Leukemia: A Meta-Analysis. Drug Des. Dev. Ther. 2019, 13, 1867–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wierzbowska, A.; Robak, T.; Pluta, A.; Wawrzyniak, E.; Cebula, B.; Hołowiecki, J.; Kyrcz-Krzemień, S.; Grosicki, S.; Giebel, S.; Skotnicki, A.B.; et al. Cladribine Combined with High Doses of Arabinoside Cytosine, Mitoxantrone, and G-CSF (CLAG-M) Is a Highly Effective Salvage Regimen in Patients with Refractory and Relapsed Acute Myeloid Leukemia of the Poor Risk: A Final Report of the Polish Adult Leukemia Group. Eur. J. Haematol. 2008, 80, 115–126. [Google Scholar] [CrossRef]
- Pluta, A.; Robak, T.; Wrzesien-Kus, A.; Katarzyna Budziszewska, B.; Sulek, K.; Wawrzyniak, E.; Czemerska, M.; Zwolinska, M.; Golos, A.; Holowiecka-Goral, A.; et al. Addition of Cladribine to the Standard Induction Treatment Improves Outcomes in a Subset of Elderly Acute Myeloid Leukemia Patients. Results of a Randomized Polish Adult Leukemia Group (PALG) Phase II Trial. Am. J. Hematol. 2017, 92, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, L.; Li, C.; Wuxiao, Z.; Shao, R.; Wang, H.; Lu, Y. Cladribine with Granulocyte Colony-Stimulating Factor, Cytarabine, and Aclarubicin Regimen in Refractory/Relapsed Acute Myeloid Leukemia: A Phase II Multicenter Study. Oncologist 2020, 25, e1663–e1670. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.M.; Ramos, F. Acute Myeloid Leukemia in the Older Adults. Leuk. Res. Rep. 2016, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 Revision to the World Health Organization Classification of Myeloid Neoplasms and Acute Leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and Management of AML in Adults: 2017 ELN Recommendations from an International Expert Panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Kadia, T.M.; Cortes, J.; Ravandi, F.; Jabbour, E.; Konopleva, M.; Benton, C.B.; Burger, J.; Sasaki, K.; Borthakur, G.; DiNardo, C.D.; et al. Cladribine and Low-Dose Cytarabine Alternating with Decitabine as Front-Line Therapy for Elderly Patients with Acute Myeloid Leukaemia: A Phase 2 Single-Arm Trial. Lancet Haematol. 2018, 5, e411–e421. [Google Scholar] [CrossRef]
- Kadia, T.; Ravandi, F.; Borthakur, G.; Konopleva, M.; DiNardo, C.; Daver, N.; Pemmaraju, N.; Kanagal-Shamanna, R.; Wang, X.; Huang, X.; et al. Long-Term Results of Low-Intensity Chemotherapy with Clofarabine or Cladribine Combined with Low-Dose Cytarabine Alternating with Decitabine in Older Patients with Newly Diagnosed Acute Myeloid Leukemia. Am. J. Hematol. 2021, 96, 914–924. [Google Scholar] [CrossRef]
- Morita, K.; Wang, F.; Jahn, K.; Hu, T.; Tanaka, T.; Sasaki, Y.; Kuipers, J.; Loghavi, S.; Wang, S.A.; Yan, Y.; et al. Clonal Evolution of Acute Myeloid Leukemia Revealed by High-Throughput Single-Cell Genomics. Nat. Commun. 2020, 11, 5327. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, C.D.; Estey, E.; Pleyer, L.; Schuh, A.C.; Stein, E.M.; Tallman, M.S.; Wei, A. Time to Repeal and Replace Response Criteria for Acute Myeloid Leukemia? Blood Rev. 2018, 32, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.K.; Mangal, N.; Menon, R.M.; Freise, K.J.; Salem, A.H. Response Rates as Predictors of Overall Survival: A Meta-Analysis of Acute Myeloid Leukemia Trials. J. Cancer 2017, 8, 1562–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, R.B.; Kantarjian, H.M.; Huang, X.; Pierce, S.A.; Sun, Z.; Gundacker, H.M.; Ravandi, F.; Faderl, S.H.; Tallman, M.S.; Appelbaum, F.R.; et al. Effect of Complete Remission and Responses Less than Complete Remission on Survival in Acute Myeloid Leukemia: A Combined Eastern Cooperative Oncology Group, Southwest Oncology Group, and M. D. Anderson Cancer Center Study. J. Clin. Oncol. 2010, 28, 1766–1771. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.A.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax Combined with Decitabine or Azacitidine in Treatment-Naive, Elderly Patients with Acute Myeloid Leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Wei, A.H.; Montesinos, P.; Ivanov, V.; DiNardo, C.D.; Novak, J.; Laribi, K.; Kim, I.; Stevens, D.A.; Fiedler, W.; Pagoni, M.; et al. Venetoclax plus LDAC for Newly Diagnosed AML Ineligible for Intensive Chemotherapy: A Phase 3 Randomized Placebo-Controlled Trial. Blood 2020, 135, 2137–2145. [Google Scholar] [CrossRef]
- Cortes, J.E.; Heidel, F.H.; Hellmann, A.; Fiedler, W.; Smith, B.D.; Robak, T.; Montesinos, P.; Pollyea, D.A.; DesJardins, P.; Ottmann, O.; et al. Randomized Comparison of Low Dose Cytarabine with or without Glasdegib in Patients with Newly Diagnosed Acute Myeloid Leukemia or High-Risk Myelodysplastic Syndrome. Leukemia 2019, 33, 379–389. [Google Scholar] [CrossRef] [Green Version]
- DiNardo, C.D.; Stein, E.M.; de Botton, S.; Roboz, G.J.; Altman, J.K.; Mims, A.S.; Swords, R.; Collins, R.H.; Mannis, G.N.; Pollyea, D.A.; et al. Durable Remissions with Ivosidenib in IDH1 -Mutated Relapsed or Refractory AML. N. Engl. J. Med. 2018, 378, 2386–2398. [Google Scholar] [CrossRef]
- Pollyea, D.A.; Tallman, M.S.; de Botton, S.; Kantarjian, H.M.; Collins, R.; Stein, A.S.; Frattini, M.G.; Xu, Q.; Tosolini, A.; See, W.L.; et al. Enasidenib, an Inhibitor of Mutant IDH2 Proteins, Induces Durable Remissions in Older Patients with Newly Diagnosed Acute Myeloid Leukemia. Leukemia 2019, 33, 2575–2584. [Google Scholar] [CrossRef] [Green Version]
- Pollyea, D.A.; Bixby, D.; Perl, A.; Bhatt, V.R.; Altman, J.K.; Appelbaum, F.R.; De Lima, M.; Fathi, A.T.; Foran, J.M.; Gojo, I.; et al. Acute Myeloid Leukemia, Version 2.2021 Featured Updates to the NCCN Guidelines. JNCCN J. Natl. Compr. Cancer Netw. 2021, 19, 16–27. [Google Scholar] [CrossRef]
- Paper: Phase II Study of Venetoclax Added to Cladribine + Low Dose AraC (LDAC) Alternating with 5-Azacytidine Demonstrates High Rates of Minimal Residual Disease (MRD) Negative Complete Remissions (CR) and Excellent Tolerability in Older Patients with New. Available online: https://ash.confex.com/ash/2020/webprogram/Paper142092.html (accessed on 21 February 2021).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
| Age (years) | |
| Median (range) | 70 (60–87) |
| >70, n (%) | 67 (57) |
| ≥75, n (%) | 41 (35) |
| ECOG performance status, n (%) | |
| 0 | 11 (9.5) |
| 1 | 36 (31) |
| 2 | 47 (40) |
| 3 | 19 (16) |
| 4 | 4 (3.5) |
| HCT-CI score, n (%) | |
| Median (range) | 3 (0–10) |
| 0–2 | 48 (42) |
| ≥3 | 67 (58) |
| Sex, n (%) | |
| Female | 66 (56) |
| Male | 51 (44) |
| Bone marrow blasts count, n (%) | |
| 20–29% | 15 (13) |
| 30–50% | 41 (35) |
| ≥50% | 61 (52) |
| LDH serum activity >480 IU/L, n (%) | 51 (46) |
| Serum creatinine >1.3 mg/dL, n (%) | 23 (20) |
| Cytogenetic risk, n (%) | |
| Favorable | 8 (7) |
| Intermediate | 51 (43.5) |
| Adverse | 51 (43.5) |
| Lack of metaphases | 7 (6) |
| AML status, n (%) | |
| De novo | 79 (67.5) |
| Secondary | 38 (32.5) |
| Somatic mutation, n (%) | |
| FLT3-ITD or TKD (1) NPM1(2) | 13 (11) 11 (9) |
| Coexistence of somatic mutations, n (%) | |
| FLT3-ITD and TKD (−), NPM1 (−) | 31 (26) |
| FLT3-ITD and TKD (−), NPM1 (+) | 4 (3) |
| FLT3-ITD or TKD (+), NPM1 (−) | 4 (3) |
| FLT3-ITD or TKD (+), NPM1 (+) | 6 (5) |
| Treatment for antecedent hematologic disorders, n (%) | |
| Azacitidine | 7 (6) |
| Hydroxyurea | 3 (3) |
| LD-AC and azacitidine | 1 (1) |
| not specified | 1 (1) |
| Independent Variable | Univariate Analysis | ||
|---|---|---|---|
| CR/CRi | Non-CR | p | |
| n (%) | n (%) | ||
| Age | |||
| 60–74 y | 32 (42%) | 44 (58%) | 0.1 |
| ≥75 y | 11 (26.8%) | 30 (73.2%) | |
| ECOG performance status | |||
| 0–1 | 16 (34%) | 31 (66%) | 0.67 |
| ≥2 | 27 (38.6%) | 43 (61.5%) | |
| HCT-CI score | |||
| 0–2 | 23 (47.9%) | 25 (52.1%) | 0.03 |
| ≥3 | 19 (28.4%) | 48 (71.6%) | |
| Cytogenetic risk | |||
| Intermediate | 26 (51%) | 25 (49%) | 0.009 |
| Adverse | 10 (19.6%) | 41 (80.4%) | |
| Bone marrow blasts count | |||
| 20–30% | 5 (33.3%) | 10 (66.7%) | 0.11 |
| >30% | 38 (37.3%) | 64 (62.7%) | |
| AML status | |||
| De novo | 33 (41.7%) | 46 (58.3%) | 0.15 |
| Secondary | 10 (26.3%) | 28 (73.6%) | |
| Serum LDH activity | |||
| <480 IU/L | 21 (34.4%) | 40 (65.6%) | 0.6 |
| ≥480 IU/L | 20 (39.2%) | 31 (60.8%) | |
| Serum creatinine | |||
| <1.3 mg/dL | 35 (37.2%) | 59 (62.8%) | 0.83 |
| ≥1.3 mg/dL | 8 (34.7%) | 15 (65.3%) | |
| Variable | Multivariate analysis | ||
| Odds ratio for CR/CRi rate (95%CI) | p | ||
| Age ≥75 years | 0.39 (0.14–1.09) | 0.072 | |
| Adverse cytogenetics (vs. intermediate cytogenetics) | 0.28 (0.11–0.71) | 0.007 | |
| Title | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Variable | HR for Death (95%CI) | p | HR for Death (95%CI) | p |
| Age (≥75) | 1.51 (1.01–2.27) | 0.047 | 1.66 (1.05–2.62) | 0.032 |
| HCT-CI score (≥3) | 1.61 (1.07–2.41) | 0.023 | 1.61 (0.98–2.61) | 0.054 |
| Cytogenetic risk (adverse) | 1.55 (1.02–2.36) | 0.042 | 1.67 (1.05–2.67) | 0.031 |
| ECOG PS (>1) | 0.99 (0.67–1.47) | 0.971 | - | - |
| Grade 3 or 4 Infectious Adverse Events | Grade 3 or 4 Non-Infectious Adverse Events | ||
|---|---|---|---|
| Grade 3 or 4 Infectious Adverse Events | n (%) | Grade 3 or 4 Non-Infectious Adverse Events | n (%) |
| Pneumonia | 29 (25%) | Cardiac arrhythmia | 5 (4%) |
| Sepsis | 17 (14.5%) | Cardiac, other (CHF, ACS) | 3 (2.5%) |
| Neutropenic fever | 15 (13%) | Constipation | 6 (5%) |
| Soft tissue infection | 10 (8.5%) | Pruritis | 2 (1.7%) |
| Clostridioides difficile infection | 3 (2.5%) | Thrombosis or pulmonary embolism | 2 (1.7%) |
| Other | 10 (8.5%) | Acute kidney injury | 2 (1.7%) |
| Other | 14 (12%) | ||
| Studied Population | n | Main Inclusion Criteria | Median (Range) Age (Years) of the Study Participants | Selected AML Characteristics | Treatment | Outcomes | References |
|---|---|---|---|---|---|---|---|
| Previously untreated AML or HR-MDS | 118 | Age ≥60 years; ECOG PS ≤2; adequate organ function | 69 (49–85); patients aged ≥70 years, 44% | Cytogenetics: HR, 41%; IR, 21% tAML, 17% | LD-AC+cladribine for 2 cycles alternating with decitabine for 2 cycles, for up to 18 cycles | CR/CRi rate, 68%; median DOR, 14.7 months; median OS, 13.8 months | [39] |
| Previously untreated AML | 35 | Age ≥18 years; adequate renal and hepatic function; the absence of alternative therapeutic options | 77 (46–87); patients aged ≥70 years, 91% | Cytogenetics: HR, 23%; IR, 37% tAML, 3% | Azacitidine | CR/CRi rate, 31%; median DOR, 6 months; median OS, 9 months | [22] |
| Previously untreated AML | 149 | Ineligibility for IC due to age and/or HR AML characteristics, including HR cytogenetics or post-MDS AML or post-MPN AML or tAML (ECOG PS <2 in 71% of participants) | 74 (31–91); patients aged ≥65 years, 83% | Cytogenetics: HR, 40%; IR, 53% tAML, 20% | Azacitidine | CR/CRi rate, 23%; median DOR, not provided; median OS, 9.4 months | [21] |
| Previously untreated AML | 55 | Age ≥60 years and HR or IR cytogenetics; ECOG PS ≤2; adequate renal and hepatic function | 74 (61–87); patients aged ≥70 years, 62% | Cytogenetics: HR, 45%; IR, 53% tAML, 7% | Decitabine | CR/CRi rate, 26%; median DOR, not provided; median OS, 7.7 months | [26] |
| Previously untreated AML | Azacitidine + venetoclax arm: 286 Azacitidine + placebo arm: 145 | Age ≥75 years or the presence of specific clinical conditions precluding IC; ECOG PS 0–2 for patients ≥75 years of age; ECOG PS 0–3 for patients ≥18 to 74 years of age; adequate renal and hepatic function | Azacitidine + venetoclax arm: 76 (49–91); patients aged ≥75 years, 61% Azacitidine + placebo arm: 76 (60–90); patients aged ≥75 years, 60% | Azacitidine + venetoclax arm: HR cytogenetics, 36%; IR cytogenetics, 64% Azacitidine + placebo arm: HR cytogenetics, 39%; IR cytogenetics, 61% | Azacitidine + venetoclax versus azacitidine + placebo | Azacitidine + venetoclax arm: CR/CRi rate, 66.4%; median DOR, 17.5 months; median OS, 14.7 months Azacitidine + placebo arm: CR/CRi rate, 28.3%; median DOR, 13.4 months; median OS, 9.6 months | [42] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budziszewska, B.K.; Salomon-Perzyński, A.; Pruszczyk, K.; Barankiewicz, J.; Pluta, A.; Helbig, G.; Janowska, A.; Kuydowicz, M.; Bołkun, Ł.; Piszcz, J.; et al. Cladribine Combined with Low-Dose Cytarabine as Frontline Treatment for Unfit Elderly Acute Myeloid Leukemia Patients: Results from a Prospective Multicenter Study of Polish Adult Leukemia Group (PALG). Cancers 2021, 13, 4189. https://doi.org/10.3390/cancers13164189
Budziszewska BK, Salomon-Perzyński A, Pruszczyk K, Barankiewicz J, Pluta A, Helbig G, Janowska A, Kuydowicz M, Bołkun Ł, Piszcz J, et al. Cladribine Combined with Low-Dose Cytarabine as Frontline Treatment for Unfit Elderly Acute Myeloid Leukemia Patients: Results from a Prospective Multicenter Study of Polish Adult Leukemia Group (PALG). Cancers. 2021; 13(16):4189. https://doi.org/10.3390/cancers13164189
Chicago/Turabian StyleBudziszewska, Bożena Katarzyna, Aleksander Salomon-Perzyński, Katarzyna Pruszczyk, Joanna Barankiewicz, Agnieszka Pluta, Grzegorz Helbig, Anna Janowska, Marta Kuydowicz, Łukasz Bołkun, Jarosław Piszcz, and et al. 2021. "Cladribine Combined with Low-Dose Cytarabine as Frontline Treatment for Unfit Elderly Acute Myeloid Leukemia Patients: Results from a Prospective Multicenter Study of Polish Adult Leukemia Group (PALG)" Cancers 13, no. 16: 4189. https://doi.org/10.3390/cancers13164189
APA StyleBudziszewska, B. K., Salomon-Perzyński, A., Pruszczyk, K., Barankiewicz, J., Pluta, A., Helbig, G., Janowska, A., Kuydowicz, M., Bołkun, Ł., Piszcz, J., Patkowska, E., Wątek, M., Małecki, P., Kościołek-Zgódka, S., Cichocka, E., Charliński, G., Irga-Staniukiewicz, A., Zaucha, J. M., Piekarska, A., ... Lech-Marańda, E. (2021). Cladribine Combined with Low-Dose Cytarabine as Frontline Treatment for Unfit Elderly Acute Myeloid Leukemia Patients: Results from a Prospective Multicenter Study of Polish Adult Leukemia Group (PALG). Cancers, 13(16), 4189. https://doi.org/10.3390/cancers13164189