
Hypothalamic–Pituitary Autoimmunity in Patients Treated with Anti-PD-1 and Anti-PD-L1 Antibodies

 ,
,  ,
, 
 ,
,
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
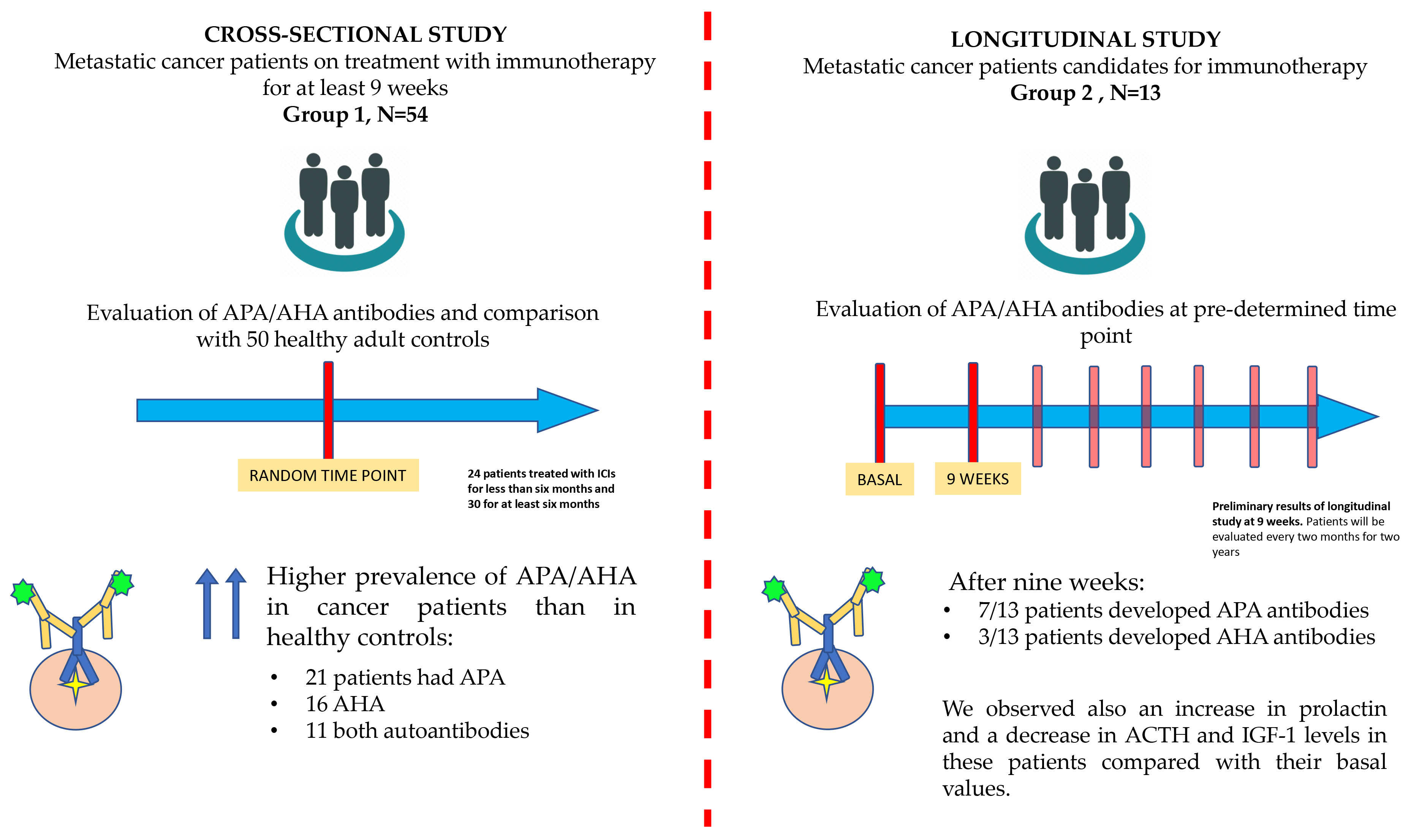
2.1. Cross-Sectional Study Population
2.2. Longitudinal Study Population
2.3. Blood Test Evaluation
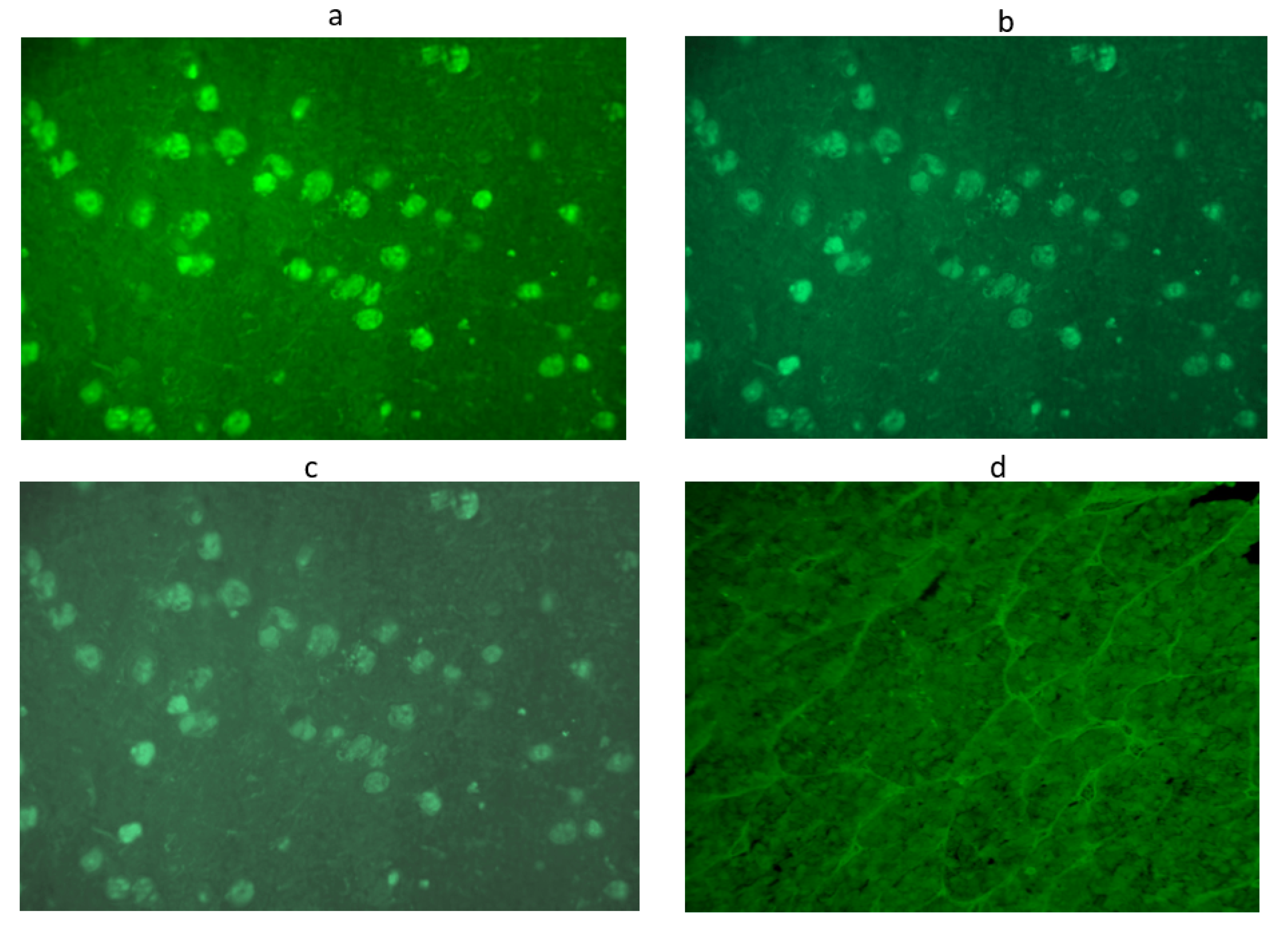
2.4. APA and AHA Evaluation
2.5. Progression-Free Survival
2.6. Statistical Analysis
3. Results
4. Discussion
- -
- The patients were included in the study at different times from the start of immunotherapy and in a highly variable time span, ranging from 4 weeks to 34 months of therapy;
- -
- No dynamic tests were performed to assess the presence of subclinical pituitary dysfunction;
- -
- Lack of characterization by four-layer double immunofluorescence of hypothalamic–pituitary-secreting cells targeted by these antibodies, which has now been planned for the next steps of our longitudinal study.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Presotto, E.M.; Rastrelli, G.; Desideri, I.; Scotti, V.; Gunnella, S.; Pimpinelli, N.; Vaccher, E.; Bearz, A.; Di Costanzo, F.; Bruggia, M.; et al. Endocrine toxicity in cancer patients treated with nivolumab or pembrolizumab: Results of a large multicentre study. J. Endocrinol. Investig. 2019, 43, 337–345. [Google Scholar] [CrossRef]
- Faje, A.T. Immunotherapy and hypophysitis: Clinical presentation, treatment, and biologic insights. Pituitary 2016, 19, 82–92. [Google Scholar] [CrossRef]
- Melmed, S. Pituitary Medicine from Discovery to Patient-Focused Outcomes. J. Clin. Endocrinol. Metab. 2016, 101, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Iwama, S.; De Remigis, A.; Callahan, M.K.; Slovin, S.F.; Wolchok, J.D.; Caturegli, P. Pituitary Expression of CTLA-4 Mediates Hypophysitis Secondary to Administration of CTLA-4 Blocking Antibody. Sci. Transl. Med. 2014, 6, 230ra45. [Google Scholar] [CrossRef]
- Caturegli, P.; Di Dalmazi, G.; Lombardi, M.; Grosso, F.; Larman, H.B.; Larman, T.; Taverna, G.; Cosottini, M.; Lupi, I. Hypophysitis Secondary to Cytotoxic T-Lymphocyte-Associated Protein 4 Blockade: Insights into Pathogenesis from an Autopsy Series. Am. J. Pathol. 2016, 186, 3225–3235. [Google Scholar] [CrossRef]
- Bertrand, A.; Kostine, M.; Barnetche, T.; Truchetet, M.E.; Schaeverbeke, T. Immune related adverse events associated with an-ti-CTLA-4 antibodies: Systematic review and meta-analysis. BMC Med. 2015, 13, 211. [Google Scholar] [CrossRef]
- Michot, J.M.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel-Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur. J. Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Barroso-Sousa, R.; Barry, W.T.; Garrido-Castro, A.C.; Hodi, F.S.; Min, L.; Krop, I.E.; Tolaney, S.M. Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 173–182. [Google Scholar] [CrossRef]
- de Filette, J.; Andreescu, C.E.; Cools, F.; Bravenboer, B.; Velkeniers, B. A Systematic Review and Meta-Analysis of Endocrine-Related Adverse Events Associated with Immune Checkpoint Inhibitors. Horm. Metab. Res. 2019, 51, 145–156. [Google Scholar]
- Di Dalmazi, G.; Ippolito, S.; Lupi, I.; Caturegli, P. Hypophysitis induced by immune checkpoint inhibitors: A 10-year assessment. Expert Rev. Endocrinol. Metab. 2019, 14, 381–398. [Google Scholar] [CrossRef]
- Faje, A.; Reynolds, K.; Zubiri, L.; Lawrence, D.; Cohen, J.V.; Sullivan, R.J.; Nachtigall, L.; Tritos, N. Hypophysitis secondary to nivolumab and pembrolizumab is a clinical entity distinct from ipilimumab-associated hypophysitis. Eur. J. Endocrinol. 2019, 181, 211–219. [Google Scholar] [CrossRef]
- Joshi, M.N.; Whitelaw, B.; Palomar, M.T.P.; Wu, Y.; Carroll, P.V. Immune checkpoint inhibitor-related hypophysitis and endocrine dysfunction: Clinical review. Clin. Endocrinol. 2016, 85, 331–339. [Google Scholar] [CrossRef]
- Byun, D.J.; Wolchok, J.D.; Rosenberg, L.M.; Girotra, M. Cancer immunotherapy—immune checkpoint blockade and associated endocrinopathies. Nat. Rev. Endocrinol. 2017, 13, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Orlov, S.; Salari, F.; Kashat, L.; Walfish, P.G. Induction of Painless Thyroiditis in Patients Receiving Programmed Death 1 Receptor Immunotherapy for Metastatic Malignancies. J. Clin. Endocrinol. Metab. 2015, 100, 1738–1741. [Google Scholar] [CrossRef]
- Badovinac, S.; Korsic, M.; Zarković, K.; Muršić, D.; Roglic, M.; Jakopovic, M.; Samarzija, M. Nivolumab-induced synchronous occurrence of myositis and hypothyroidism in a patient with squamous cell lung cancer. Immunotherapy 2018, 10, 427–431. [Google Scholar] [CrossRef]
- Scott, E.S.; Long, G.; Guminski, A.; Clifton-Bligh, R.; Menzies, A.; Tsang, V.H. The spectrum, incidence, kinetics and management of endocrinopathies with immune checkpoint inhibitors for metastatic melanoma. Eur. J. Endocrinol. 2018, 178, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Castillero, F.; Castillo-Fernández, O.; Jiménez-Jiménez, G.; Fallas-Ramírez, J.; Peralta-Álvarez, M.P.; Arrieta, O. Cancer immunotherapy-associated hypophysitis. Future Oncol. 2019, 15, 3159–3169. [Google Scholar] [CrossRef]
- Lupi, I.; Brancatella, A.; Cosottini, M.; Viola, N.; Lanzolla, G.; Sgrò, D.; Dalmazi, G.D.; Latrofa, F.; Caturegli, P.; Marcocci, C. Clinical heterogeneity of hypophysitis secondary to PD-1/PD-L1 blockade: Insights from four cases. Endocrinol. Diabetes Metab. Case Rep. 2019, 2019, 19–0102. [Google Scholar] [CrossRef]
- de Bellis, A.; Sinisi, A.A.; Pane, E.; DelloIacovo, A.; Bellastella, G.; Di Scala, G.; Falorni, A.; Giavoli, C.; Gasco, V.; Giordano, R.; et al. Involvement of hypothalamus autoimmunity in patients with autoimmune hypopituitarism: Role of antibodies to hypothalamic cells. J. Clin. Endocrinol. Metab. 2012, 97, 3684–3690. [Google Scholar] [CrossRef] [PubMed]
- Bellastella, G.; Maiorino, M.I.; Longo, M.; Cirillo, P.; Scappaticcio, L.; Vietri, M.T.; Bellastella, A.; Esposito, K.; De Bellis, A. Impact of Pituitary Autoimmunity and Genetic Disorders on Growth Hormone Deficiency in Children and Adults. Int. J. Mol. Sci. 2020, 21, 1392. [Google Scholar] [CrossRef]
- De Bellis, A.; Bizzarro, A.; Conte, M.; Perrino, S.; Coronella, C.; Solimeno, S.; Sinisi, A.M.; Stile, L.A.; Pisano, G.; Bellastella, A. Antipituitary antibodies in adults with apparently idiopathic growth hormone deficiency and in adults with autoimmune endocrine diseases. J. Clin. Endocrinol. Metab. 2003, 88, 650–654. [Google Scholar] [CrossRef] [PubMed]
- De Bellis, A.; Bellastella, G.; Maiorino, M.I.; Aitella, E.; Lucci, E.; Cozzolino, D.; Bellastella, A.; Bizzarro, A.; Giugliano, D.; Esposito, K. Italian Autoimmune Hypophysitis Network Group. Longitudinal behavior of autoimmune GH deficiency: From childhood to transition age. Eur. J. Endocrinol. 2016, 174, 381–387. [Google Scholar] [CrossRef]
- Patti, G.; Calandra, E.; De Bellis, A.; Gallizia, A.; Crocco, M.; Napoli, F.; Allegri, A.M.E.; Thiabat, H.F.; Bellastella, G.; Maiorino, M.I.; et al. Antibodies Against Hypothalamus and Pituitary Gland in Childhood-Onset Brain Tumors and Pituitary Dysfunction. Front. Endocrinol. 2020, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- de Bellis, A.; Bellastella, G.; Maiorino, M.I.; Costantino, A.; Cirillo, P.; Longo, M.; Pernice, V.; Bellastella, A.; Esposito, K. The role of autoimmunity in pituitary dysfunction due to traumatic brain injury. Pituitary 2019, 22, 236–248. [Google Scholar] [CrossRef]
- Dillard, T.; Yedinak, C.G.; Alumkal, J.; Fleseriu, M. Anti-CTLA-4 antibody therapy associated autoimmune hypophysitis: Serious immune related adverse events across a spectrum of cancer subtypes. Pituitary 2010, 13, 29–38. [Google Scholar] [CrossRef]
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer-immune set point. Nature 2017, 541, 321–330. [Google Scholar] [CrossRef]
- Sharma, R.; Di Dalmazi, G.; Caturegli, P. Exacerbation of Autoimmune Thyroiditis by CTLA-4 Blockade: A Role for IFNγ-Induced Indoleamine 2, 3-Dioxygenase. Thyroid 2016, 26, 1117–1124. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.C.; Ezzat, S.; Smyth, H.S.; Asa, S.L. The spectrum and significance of primary hypophysitis. J. Clin. Endocrinol. Metab. 2001, 86, 1048–1053. [Google Scholar] [CrossRef]
- Bellastella, G.; Bizzarro, A.; Coronella, C.; Sinisi, A.A.; de Bellis, A. Lymphocytic hypophysitis: A rare or underestimated disease? Eur. J. Endocrinol. 2003, 149, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Caturegli, P.; Newschaffer, C.; Olivi, A.; Pomper, M.G.; Burger, P.C.; Rose, N.R. Autoimmune Hypophysitis. Endocr. Rev. 2005, 26, 599–614. [Google Scholar] [CrossRef] [PubMed]
- Caturegli, P.; Lupi, I.; Landek-Salgado, M.; Kimura, H.; Rose, N.R. Pituitary autoimmunity: 30 years later. Autoimmun. Rev. 2008, 7, 631–637. [Google Scholar] [CrossRef]
- Bellastella, G.; Maiorino, M.I.; Bizzarro, A.; Giugliano, D.; Esposito, K.; Bellastella, A.; de Bellis, A. Revisitation of autoimmune hy-pophysitis: Knowledge and uncertainties on pathophysiological and clinical aspects. Pituitary 2016, 19, 625–642. [Google Scholar] [CrossRef]
- de Bellis, A.; DelloIacovo, A.; Bellastella, G.; Savoia, A.; Cozzolino, D.; Sinisi, A.A.; Bizzarro, A.; Bellastella, A.; Giugliano, D. Charac-terization of pituitary cells targeted by antipituitary antibodies in patients with isolated autoimmune diseases without pituitary insufficiency may help to foresee the kind of future hypopituitarism. Pituitary 2014, 17, 457–463. [Google Scholar] [CrossRef]
- Wei, Q.; Yang, G.; Lue, Z.; Dou, J.; Zang, L.; Li, Y.; Du, J.; Gu, W.; Mu, Y. Clinical aspects of autoimmune hypothalamitis, a variant of autoimmune hypophysitis: Experience from one center. J. Int. Med. Res. 2020, 48, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Tshuma, N.; Glynn, N.; Evanson, J.; Powles, T.; Drake, W. Hypothalamitis and severe hypothalamic dysfunction associated with anti–programmed cell death ligand 1 antibody treatment. Eur. J. Cancer 2018, 104, 247–249. [Google Scholar] [CrossRef]
- Iervasi, E.; Strangio, A.; Saverino, D. Hypothalamic expression of PD-L1: Does it mediate hypothalamitis? Cell. Mol. Immunol. 2019, 16, 625–626. [Google Scholar] [CrossRef]
- Türe, U.; De Bellis, A.; Harput, M.V.; Bellastella, G.; Topcuoglu, M.; Yaltirik, C.K.; Cirillo, P.; Yola, R.N.; Sav, A.; Kelestimur, F. Hypothalamitis: A Novel Autoimmune Endocrine Disease. A Literature Review and Case Report. J. Clin. Endocrinol. Metab. 2021, 106, e415–e429. [Google Scholar] [CrossRef] [PubMed]
- Sznol, M.; Postow, M.A.; Davies, M.J.; Pavlick, A.C.; Plimack, E.R.; Shaheen, M.; Veloski, C.; Robert, C. Endocrine-related adverse events associated with immune checkpoint blockade and expert insights on their management. Cancer Treat. Rev. 2017, 58, 70–76. [Google Scholar] [CrossRef]
- Stamatouli, A.M.; Quandt, Z.; Perdigoto, A.L.; Clark, P.L.; Kluger, H.; Weiss, S.A.; Gettinger, S.; Sznol, M.; Young, A.; Rushakoff, R.; et al. Collateral Damage: Insulin-Dependent Diabetes Induced with Checkpoint Inhibitors. Diabetes 2018, 67, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Min, L.; Ibrahim, N. Ipilimumab-induced autoimmune adrenalitis. Lancet Diabetes Endocrinol. 2013, 1, e15. [Google Scholar] [CrossRef]
- Kotwal, A.; Kottschade, L.; Ryder, M. PD-L1 Inhibitor-Induced Thyroiditis Is Associated with Better Overall Survival in Cancer Patients. Thyroid 2020, 30, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Narita, T.; Oiso, N.; Taketomo, Y.; Okahashi, K.; Yamauchi, K.; Sato, M.; Uchida, S.; Matsuda, H.; Kawada, A. Serological aggravation of autoimmune thyroid disease in two cases receiving nivolumab. J. Dermatol. 2016, 43, 210–214. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients on Treatment with Anti-PD-1, Anti-PD-L1 or Both (Group 1, n = 54) | Control Group (n = 50) | p-Value | |
|---|---|---|---|
| Sex (% of male) | 65 | 59 | 0.76 |
| Age, y | 65 ± 10.7 | 67 ± 8 | 0.28 |
| Systolic Arterial Pressure, mm Hg | 119 ± 15 | 122 ± 12 | 0.26 |
| Diastolic Arterial Pressure, mm Hg | 72 ± 11 | 78 ± 10 | 0.005 |
| Sodium, mmol/L | 139 ± 3 | 142 ± 3 | <0.001 |
| Glycemia, mg/dL | 103 ± 24 | 95 ± 14 | 0.04 |
| ACTH, pg/mL | 21 ± 17 | 22.7 ± 3.6 | 0.49 |
| Cortisol, μg/dL | 13.8 ± 6.8 | 13.4 ± 1.5 | 0.68 |
| TSH, μUI/mL | 1.7 ± 1.6 | 1.5 ± 0.4 | 0.39 |
| FT4, ng/dL | 1.27 ± 0.67 | 1.2 ± 1.8 | 0.79 |
| FT3, pg/mL | 3.4 ± 1.8 | 3.7 ± 0.6 | 0.26 |
| TgAb, UI/mL | 25.4 ± 15.3 | 8.06 ± 3.70 | <0.001 |
| TPOAb, UI/mL | 28.1 ± 39.03 | 6.30 ± 8.18 | <0.001 |
| FSH, UI/L | |||
| Males | 26.3 ± 18.29 | 3.2 ± 1.8 | <0.001 |
| Females | 61.2 ± 39.8 | 81.7 ± 34.5 | 0.006 |
| LH, UI/L | |||
| Males | 7.87 ± 5.38 | 3.8 ± 1.7 | <0.001 |
| Females | 18.4 ± 12.02 | 21.9 ± 9.4 | 0.10 |
| Oestradiol, pg/mL (females) | 16.5 ± 12.1 | 12.7 ± 8.3 | 0.06 |
| Testosterone, ng/dL (males) | 209.2 ± 159.31 | 312.1 ± 172.4 | 0.002 |
| IGF-1, ng/mL | 122.3 ± 45.3 | 134.5 ± 40.2 | 0.15 |
| Prolactin, ng/mL | 14.7 ± 5.59 | 18.6 ± 14.2 | 0.06 |
| Patients positive for APA, n (%) | 21 (39%) | 0 | <0.001 |
| Patients positive for AHA, n (%) | 16 (29%) | 0 | <0.001 |
| Patients positive for APA and AHA, n (%) | 11 (20%) | 0 | 0.002 |
| Patients on Anti-PD-1 Therapy (Group 1a) (n = 37) | Patients on Anti-PD-L1 Therapy (Group 1b) (n = 17) | p-Value | |
|---|---|---|---|
| Time from the start of therapy, month | 8.9 ± 8.8 | 6.8 ± 8.1 | 0.40 |
| Patients with APA positivity, n (%) | 14 (38%) | 7 (41%) | 0.94 |
| Low titer 1:8 | 5 (13.5%) | 0 | 0.16 |
| Middle titer 1:16 | 9 (24.3%) | 7 (41%) | 0.14 |
| High titer 1:32 | 0 | 0 | |
| Patients with AHA positivity, n (%) | 10 (27%) | 6 (35%) | 0.76 |
| Low titer 1:8 | 3 (8%) | 0 | 0.54 |
| Middle titer 1:16 | 7 (19%) | 5 (29%) | 0.48 |
| High titer 1:32 | 1 (2.7%) | 1 (6%) | 0.53 |
| Patients positive for APA/AHA and pituitary deficiency, n (%) | 1 (2.7%) | 0 | 0.99 |
| Patients positive for APA/AHA and other endocrine toxicities, n (%) | 2 (5.4%) | 0 | 0.99 |
| Before Treatment with ICIs | After 9 Weeks on Therapy with ICIs | p-Value | |
|---|---|---|---|
| Systolic arterial pressure, mm Hg | 136 ± 15 | 130 ± 20 | 0.05 |
| Diastolic arterial pressure, mm Hg | 88 ± 12 | 80 ± 16 | 0.16 |
| Glycemia, mg/dL | 90 ± 9 | 98 ± 10 | 0.04 |
| ACTH, pg/mL | 25 ± 7 | 17 ± 9 | 0.01 |
| Cortisol, μg/dL | 10.8 ± 5.39 | 10.1 ± 4.49 | 0.72 |
| TSH, μUI/ mL | 2.5 ± 1.7 | 2.3 ± 1.4 | 0.74 |
| FT4, ng/dL | 1.5 ± 0.8 | 1.1 ± 0.9 | 0.24 |
| FT3, pg/mL | 3.4 ± 0.8 | 2.9 ± 1 | 0.17 |
| TgAb, UI/mL | 24.3 ± 52.05 | 115.7 ± 356.3 | 0.36 |
| TPOAb, UI/mL | 50.06 ± 107.7 | 39.7 ± 85.5 | 0.78 |
| FSH, mUI/mL | |||
| males | 22.1 ± 18.25 | 24.9 ± 19.5 | 0.69 |
| females | 79.1 ± 31.5 | 68.7 ± 53.4 | 0.55 |
| LH, mUI/mL | |||
| males | 10.7 ± 8.48 | 7.64 ± 5.64 | 0.28 |
| females | 21.3 ± 15.7 | 20.8 ± 16.1 | 0.93 |
| Oestradiol, pg/mL (females) | 10.2 ± 1.28 | 14.2 ± 7.6 | 0.07 |
| Testosterone, ng/dl (males) | 162.5 ± 85.5 | 156.8 ± 84.4 | 0.86 |
| IGF-1, ng/mL | 148.3 ± 53.6 | 90.3 ± 35.0 | 0.003 |
| Prolactin, ng/mL | 6.6 ± 3.2 | 16.3 ± 15.8 | 0.04 |
| Patients positive for APA, N (%) | 1 (7.7%) | 7 (53%) | 0.03 |
| Patients positive for AHA, N (%) | 0 | 3 (23%) | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellastella, G.; Carbone, C.; Scappaticcio, L.; Cirillo, P.; Troiani, T.; Morgillo, F.; Vietri, M.T.; Della Corte, C.M.; De Falco, V.; Napolitano, S.; et al. Hypothalamic–Pituitary Autoimmunity in Patients Treated with Anti-PD-1 and Anti-PD-L1 Antibodies. Cancers 2021, 13, 4036. https://doi.org/10.3390/cancers13164036
Bellastella G, Carbone C, Scappaticcio L, Cirillo P, Troiani T, Morgillo F, Vietri MT, Della Corte CM, De Falco V, Napolitano S, et al. Hypothalamic–Pituitary Autoimmunity in Patients Treated with Anti-PD-1 and Anti-PD-L1 Antibodies. Cancers. 2021; 13(16):4036. https://doi.org/10.3390/cancers13164036
Chicago/Turabian StyleBellastella, Giuseppe, Carla Carbone, Lorenzo Scappaticcio, Paolo Cirillo, Teresa Troiani, Floriana Morgillo, Maria Teresa Vietri, Carminia Maria Della Corte, Vincenzo De Falco, Stefania Napolitano, and et al. 2021. "Hypothalamic–Pituitary Autoimmunity in Patients Treated with Anti-PD-1 and Anti-PD-L1 Antibodies" Cancers 13, no. 16: 4036. https://doi.org/10.3390/cancers13164036
APA StyleBellastella, G., Carbone, C., Scappaticcio, L., Cirillo, P., Troiani, T., Morgillo, F., Vietri, M. T., Della Corte, C. M., De Falco, V., Napolitano, S., Maiorino, M. I., De Bellis, A., & Esposito, K. (2021). Hypothalamic–Pituitary Autoimmunity in Patients Treated with Anti-PD-1 and Anti-PD-L1 Antibodies. Cancers, 13(16), 4036. https://doi.org/10.3390/cancers13164036