
Salvage Radioligand Therapy with Repeated Cycles of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer with Diffuse Bone Marrow Involvement

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiolabeling and Administration
2.3. Toxicity Assessment
2.4. Response Assessment
2.5. Whole-Body Dosimetry
2.6. Statistical Analysis
3. Results
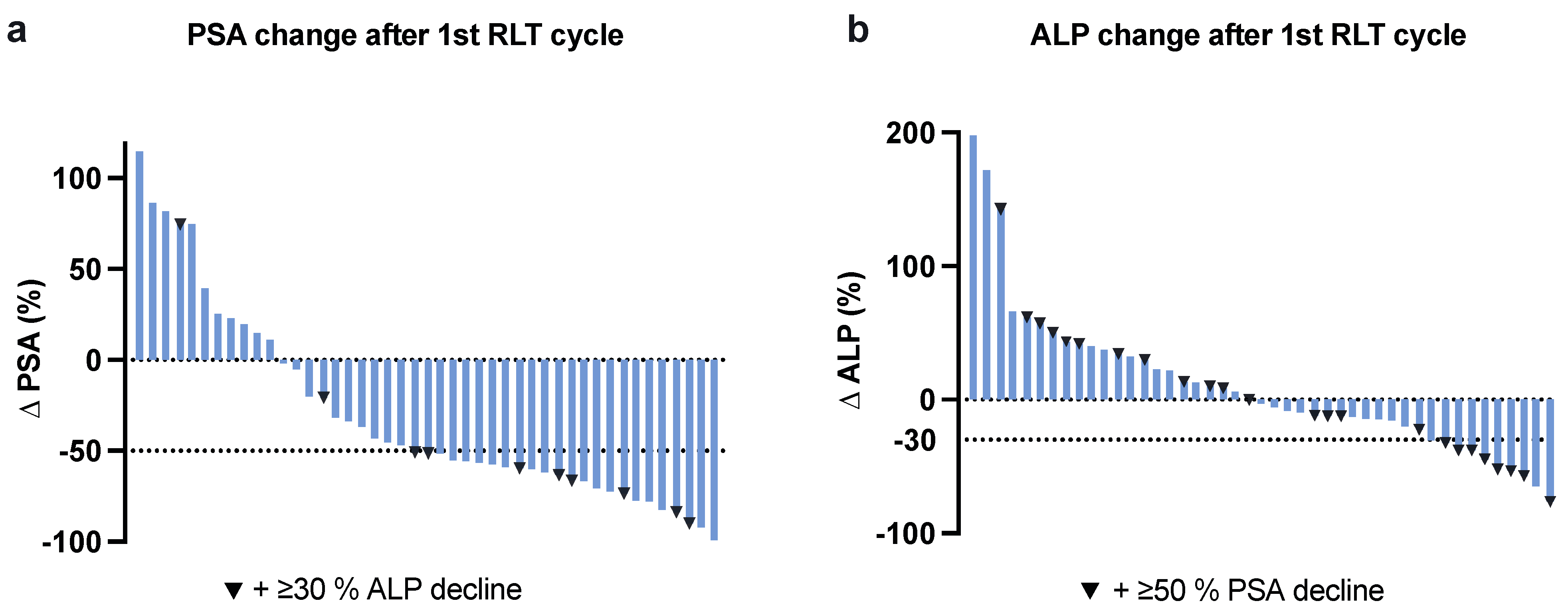
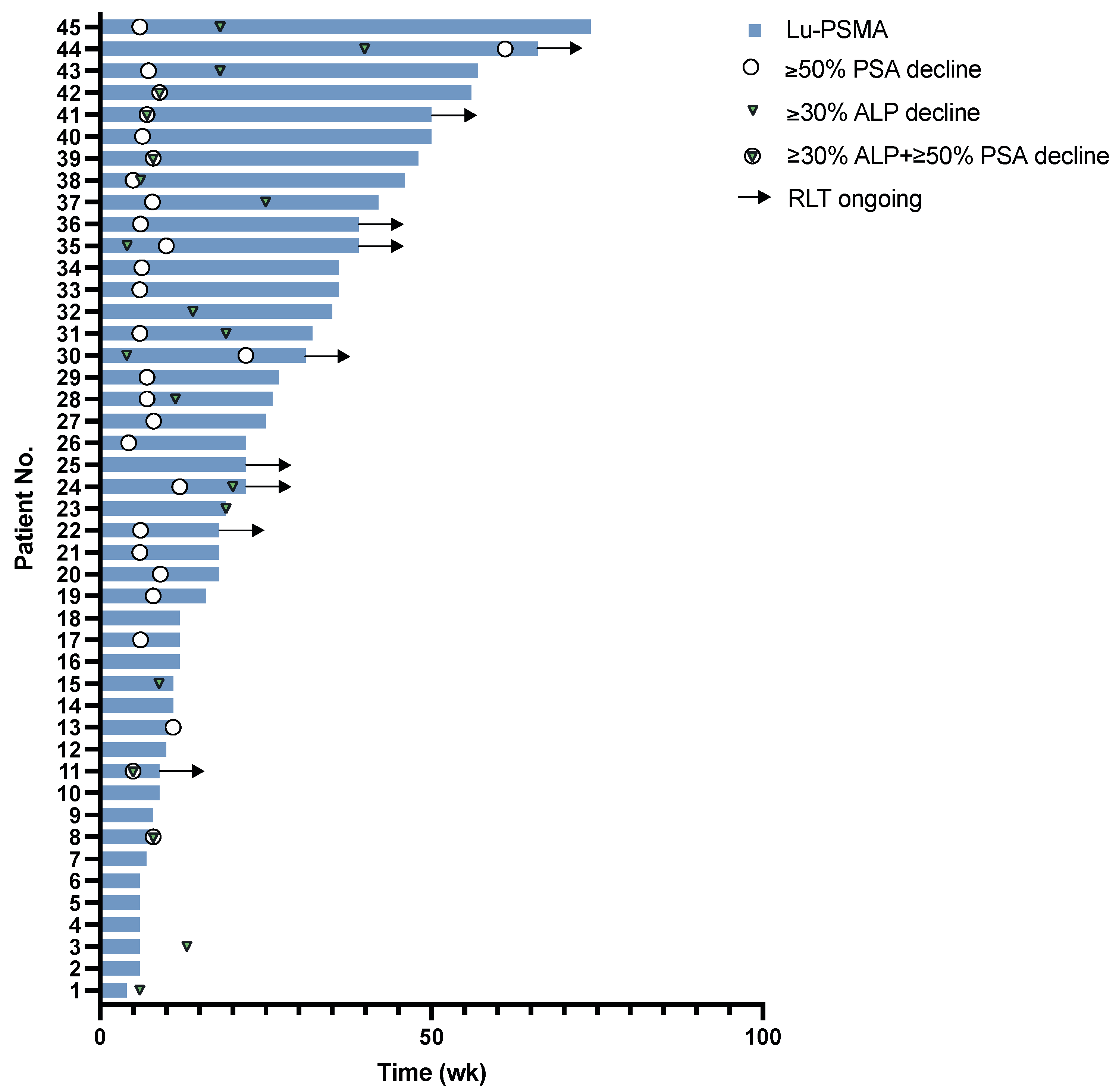
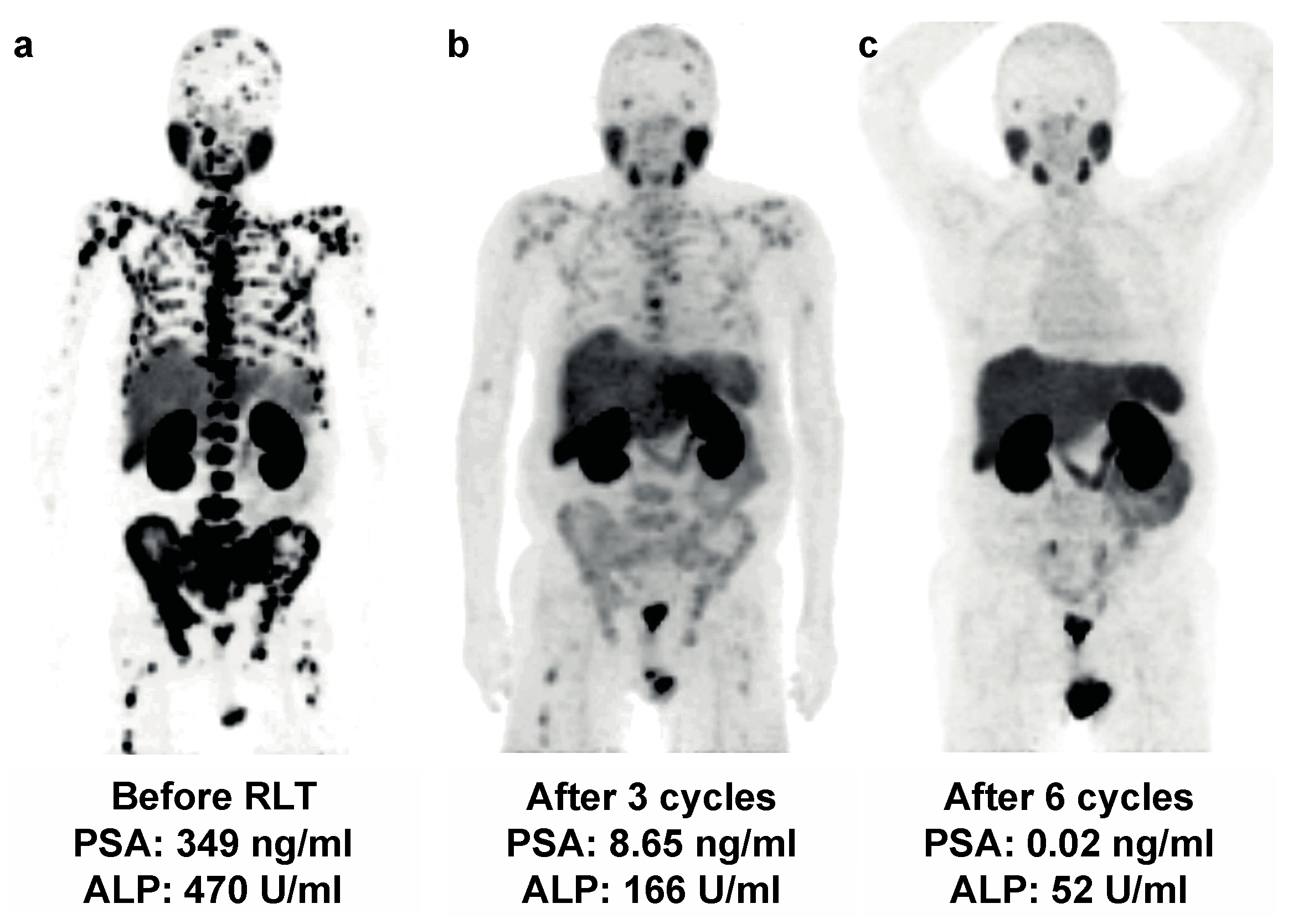
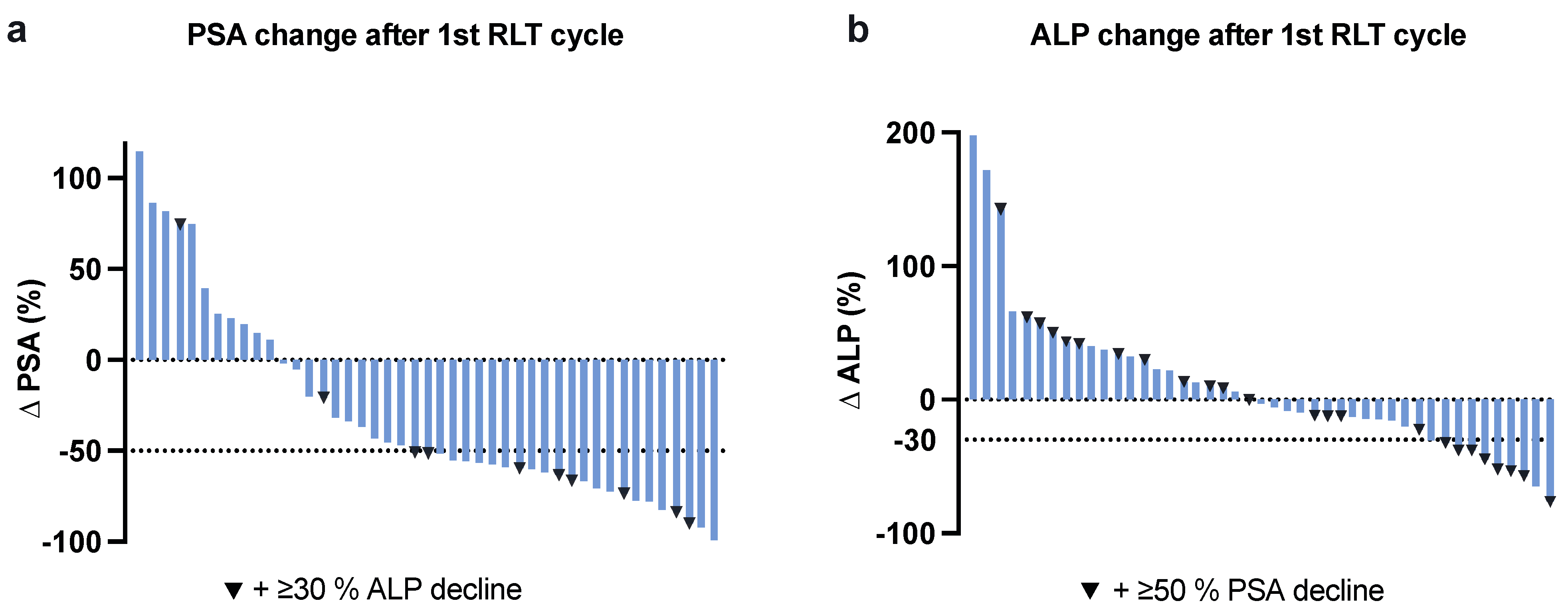
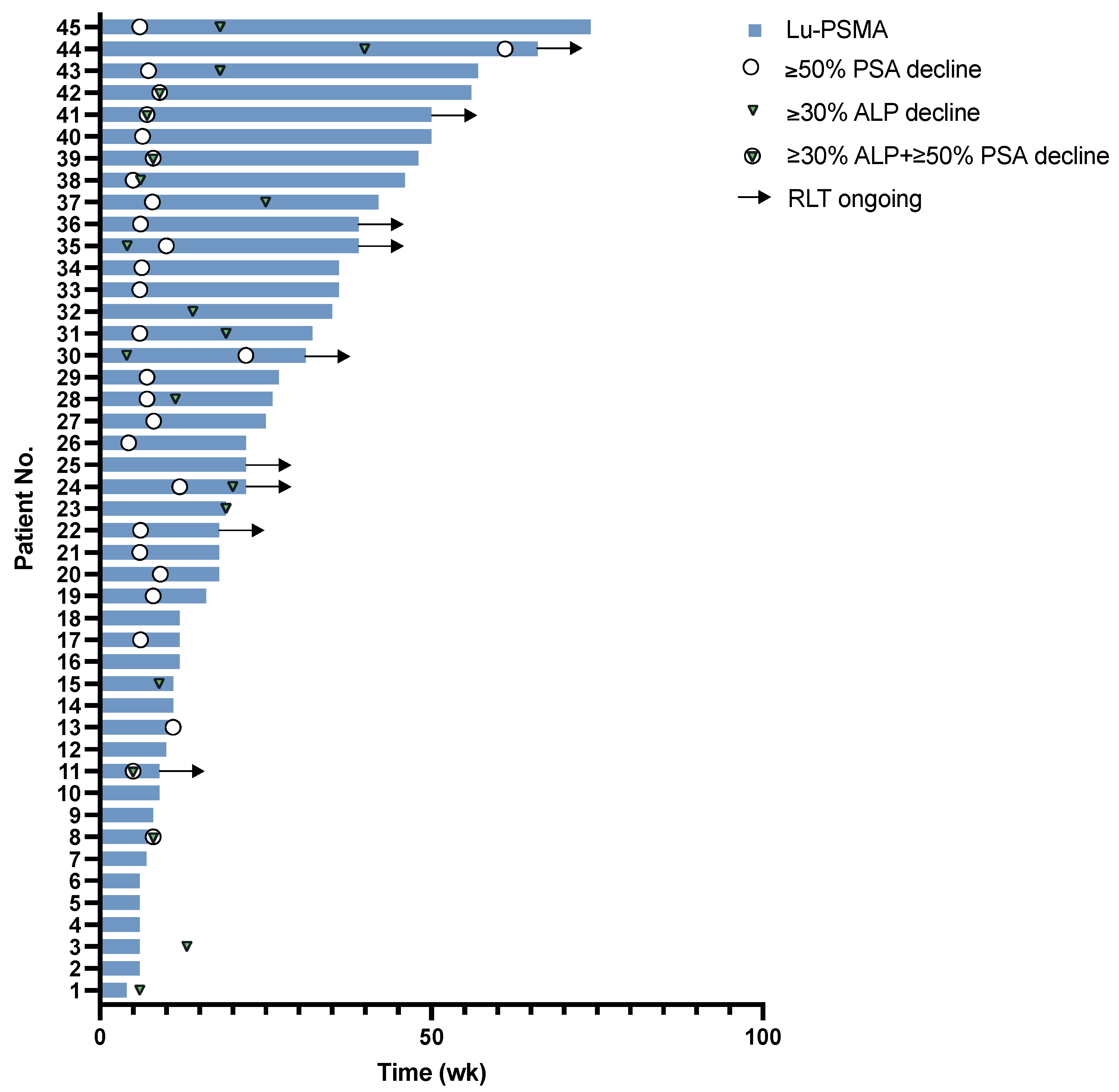
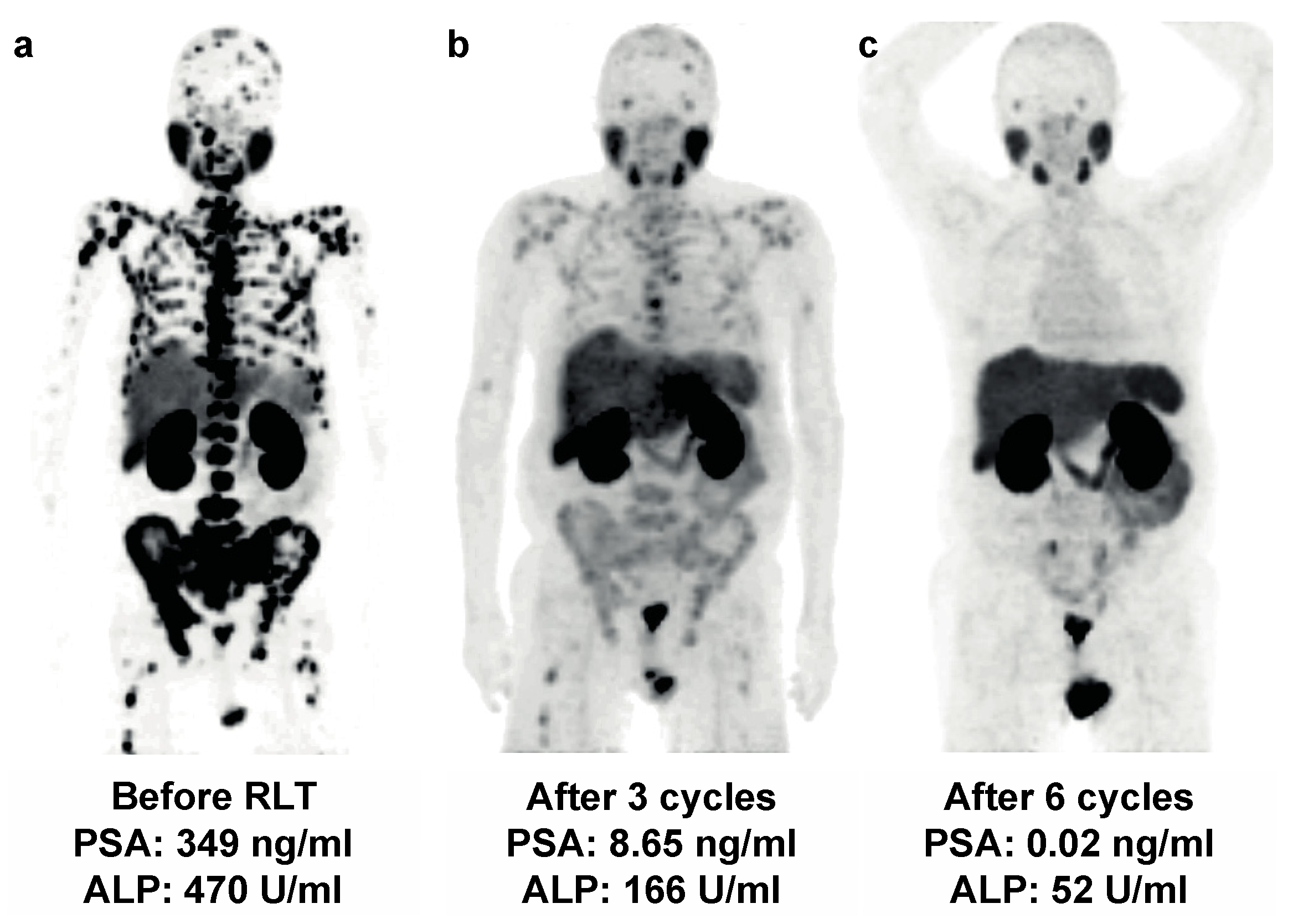
3.1. Response
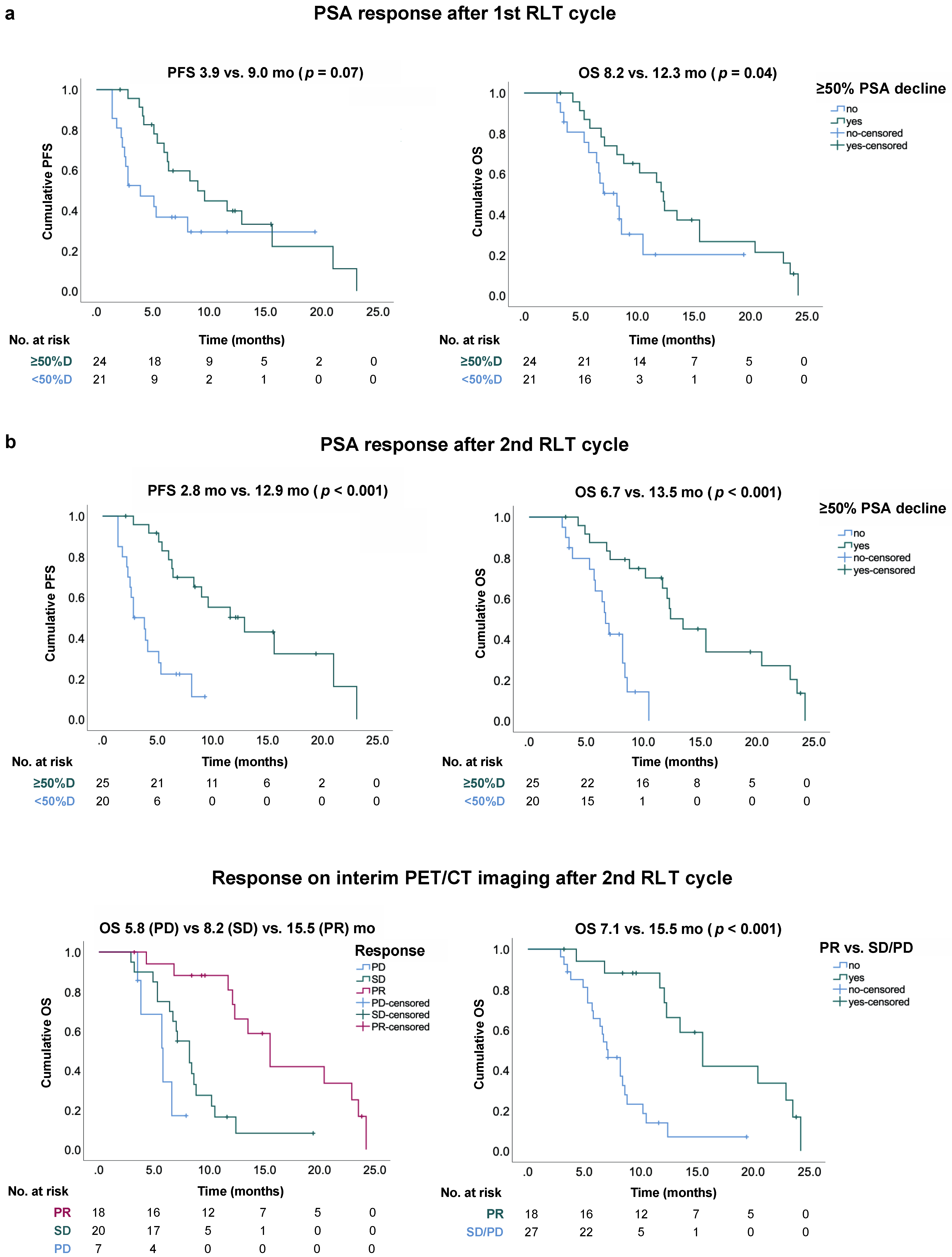
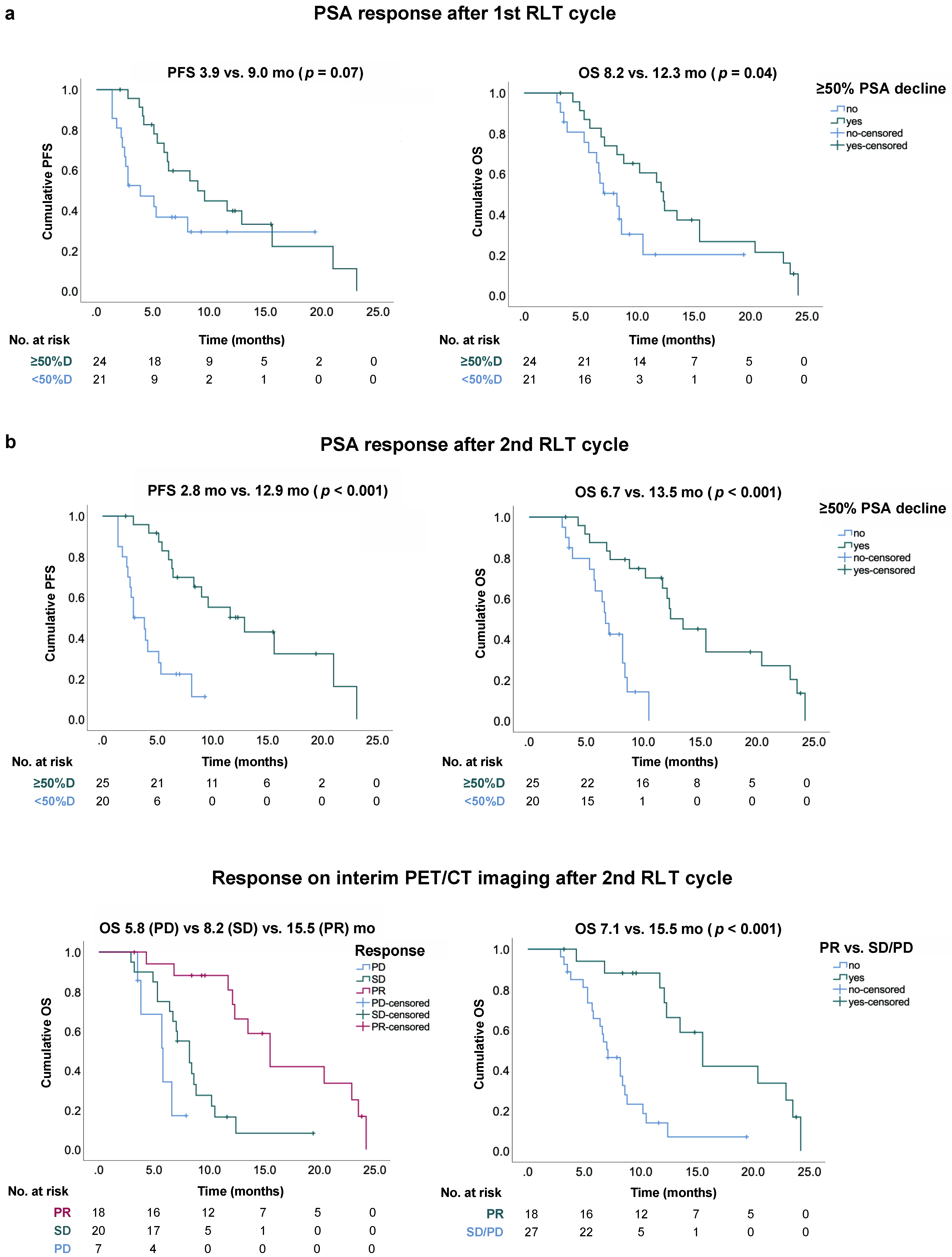
3.2. Survival
3.3. Safety
3.4. Patients with Significant Toxicity
3.5. Whole-Body Dosimetry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2018, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirby, M.; Hirst, C.; Crawford, E.D. Characterising the castration-resistant prostate cancer population: A systematic review. Int. J. Clin. Pract. 2011, 65, 1180–1192. [Google Scholar] [CrossRef] [PubMed]
- Ottewell, P.D.; Wang, N.; Meek, J.; Fowles, C.A.; Croucher, P.I.; Eaton, C.L.; Holen, I. Castration-induced bone loss triggers growth of disseminated prostate cancer cells in bone. Endocr. Relat. Cancer 2014, 21, 769–781. [Google Scholar] [CrossRef]
- Saad, F. Impact of bone metastases on patient’s quality of life and importance of treatment. Eur. Urol. Suppl. 2006, 5, 547–550. [Google Scholar] [CrossRef]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [Green Version]
- de Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.-P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus Cabazitaxel or Mitoxantrone for Metastatic Castration-Resistant Prostate Cancer Progressing after Docetaxel Treatment: A Randomised Open-Label Trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- de Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B.; Saad, F.; et al. Abiraterone and increased survival in metastatic prostate cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef] [PubMed]
- Cabot, R.C.; Harris, N.L.; Rosenberg, E.S.; Shepard, J.-A.O.; Cort, A.M.; Ebeling, S.H.; McDonald, E.K.; Scher, H.I.; Fizazi, K.; Saad, F.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [Green Version]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Murphy, D.G.; et al. [177Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): A single-centre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef]
- Heck, M.M.; Tauber, R.; Schwaiger, S.; Retz, M.; D’Alessandria, C.; Maurer, T.; Gafita, A.; Wester, H.-J.; Gschwend, J.E.; Weber, W.A.; et al. Treatment outcome, toxicity, and predictive factors for radioligand therapy with 177Lu-PSMA-I&T in metastatic castration-resistant prostate cancer. Eur. Urol. 2018, 75, 920–926. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu] Lu-PSMA-617 versus Cabazitaxel in Patients with Metastatic Castration-Resistant Prostate Cancer (TheraP): A Randomised, Open-Label, Phase 2 Trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schäfers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German multicenter study investigating 177Lu-PSMA-617 radioligand therapy in advanced prostate cancer patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Violet, J.; Zhang, A.Y.; Lawrence, N.J.; Stockler, M.; Francis, R.J.; Iravani, A.; Williams, S.; Azad, A.; et al. TheraP: A randomized phase 2 trial of 177Lu-PSMA-617 theranostic treatment vs cabazitaxel in progressive metastatic castration-resistant prostate cancer (Clinical Trial Protocol ANZUP 1603). BJU Int. 2019, 124, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gafita, A.; Fendler, W.P.; Hui, W.; Sandhu, S.; Weber, M.; Esfandiari, R.; Calais, J.; Rauscher, I.; Rathke, H.; Tauber, R.; et al. Efficacy and safety of 177Lu-labeled prostate-specific membrane antigen radionuclide treatment in patients with diffuse bone marrow involvement: A multicenter retrospective study. Eur. Urol. 2020, 78, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Matern, R.; Baum, R.P.; Seifert, R.; Kessel, K.; Bögemann, M.; Kratochwil, C.; Rathke, H.; Ilhan, H.; Svirydenka, H.; et al. The impact of the extent of the bone involvement on overall survival and toxicity in MCRPC patients receiving [177Lu] Lu-PSMA-617: A WARMTH multicentre study. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–10. [Google Scholar] [CrossRef]
- Gafita, A.; Rauscher, I.; Retz, M.; Knorr, K.; Heck, M.; Wester, H.-J.; D’Alessandria, C.; Weber, W.A.; Eiber, M.; Tauber, R. Early experience of rechallenge 177Lu-PSMA radioligand therapy after an initial good response in patients with advanced prostate cancer. J. Nucl. Med. 2018, 60, 644–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rescigno, P.; Lorente, D.; Bianchini, D.; Ferraldeschi, R.; Kolinsky, M.P.; Sideris, S.; Zafeiriou, Z.; Sumanasuriya, S.; Smith, A.D.; Mehra, N.; et al. Prostate-specific antigen decline after 4 weeks of treatment with abiraterone acetate and overall survival in patients with metastatic castration-resistant prostate cancer. Eur. Urol. 2016, 70, 724–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartor, O.; Coleman, R.E.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Vogelzang, N.J.; Bruland, Ø.; Kobina, S.; Wilhelm, S.; et al. An exploratory analysis of alkaline phosphatase, lactate dehydrogenase, and prostate-specific antigen dynamics in the phase 3 ALSYMPCA trial with radium-223. Ann. Oncol. 2017, 28, 1090–1097. [Google Scholar] [CrossRef] [PubMed]
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate cancer molecular imaging standardized evaluation (PROMISE): Proposed MiTNM classification for the interpretation of PSMA-ligand PET/CT. J. Nucl. Med. 2017, 59, 469–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadzadehfar, H.; Rahbar, K.; Kürpig, S.; Bögemann, M.; Claesener, M.; Eppard, E.; Gärtner, F.; Rogenhofer, S.; Schäfers, M.; Essler, M. Early side effects and first results of radioligand therapy with 177Lu-DKFZ-617 PSMA of castrate-resistant metastatic prostate cancer: A two-centre study. EJNMMI Res. 2015, 5, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratochwil, C.; Giesel, F.L.; Stefanova, M.; Benešová, M.; Bronzel, M.; Afshar-Oromieh, A.; Mier, W.; Eder, M.; Kopka, K.; Haberkorn, U. PSMA-targeted radionuclide therapy of metastatic castration-resistant prostate cancer with 177Lu-labeled PSMA-617. J. Nucl. Med. 2016, 57, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- Derlin, T.; Sohns, J.M.S.; Schmuck, S.; Henkenberens, C.; Klot, C.A.J.; Ross, T.L.; Bengel, F.M. Influence of short-term dexamethasone on the efficacy of 177Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Prostate 2020, 80, 619–631. [Google Scholar] [CrossRef] [Green Version]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial design and objectives for castration-resistant prostate cancer: Updated recommendations from the prostate cancer clinical trials working group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [Green Version]
- Fanti, S.; Goffin, K.; Hadaschik, B.A.; Herrmann, K.; Maurer, T.; MacLennan, S.; Oprea-Lager, D.E.; Oyen, W.J.; Rouvière, O.; Mottet, N.; et al. Consensus statements on PSMA PET/CT response assessment criteria in prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Eckerman, K.F.; Endo, A. MIRD: Radionuclide Data and Decay Schemes; SNMMI: Reston, VA, USA, 2007. [Google Scholar]
- Violet, J.; Sandhu, S.; Iravani, A.; Ferdinandus, J.; Thang, S.-P.; Kong, G.; Kumar, A.R.; Akhurst, T.; Pattison, D.; Beaulieu, A.; et al. Long-term follow-up and outcomes of retreatment in an expanded 50-patient single-center phase II prospective trial of 177Lu-PSMA-617 theranostics in metastatic castration-resistant prostate cancer. J. Nucl. Med. 2019, 61, 857–865. [Google Scholar] [CrossRef]
- Morris, M.J.; Bono, J.S.D.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Phase III study of Lutetium-177-PSMA-617 in patients with metastatic castration-resistant prostate cancer (VISION). J. Clin. Oncol. 2021, 39, LBA4. [Google Scholar] [CrossRef]
- Khreish, F.; Kochems, N.; Rosar, F.; Sabet, A.; Ries, M.; Maus, S.; Saar, M.; Bartholomä, M.; Ezziddin, S. Response and outcome of liver metastases in patients with metastatic castration-resistant prostate cancer (MCRPC) undergoing 177Lu-PSMA-617 radioligand therapy. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 103–112. [Google Scholar] [CrossRef]
- Rasul, S.; Hacker, M.; Kretschmer-Chott, E.; Leisser, A.; Grubmüller, B.; Kramer, G.; Shariat, S.; Wadsak, W.; Mitterhauser, M.; Hartenbach, M.; et al. Clinical outcome of standardized 177Lu-PSMA-617 therapy in metastatic prostate cancer patients receiving 7400 MBq every 4 weeks. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Manafi-Farid, R.; Harsini, S.; Saidi, B.; Ahmadzadehfar, H.; Herrmann, K.; Briganti, A.; Walz, J.; Beheshti, M. Factors predicting biochemical response and survival benefits following radioligand therapy with [177Lu] Lu-PSMA in metastatic castrate-resistant prostate cancer: A review. Eur. J. Nucl. Med. Mol. Imaging 2021, 1–14. [Google Scholar] [CrossRef]
- Rao, S.R.; Snaith, A.E.; Marino, D.; Cheng, X.; Lwin, S.T.; Orriss, I.R.; Hamdy, F.C.; Edwards, C.M. Tumour-derived alkaline phosphatase regulates tumour growth, epithelial plasticity and disease-free survival in metastatic prostate cancer. Brit. J. Cancer 2017, 116, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Boegemann, M.; Yordanova, A.; Eveslage, M.; Schäfers, M.; Essler, M.; Ahmadzadehfar, H. PSMA targeted radioligandtherapy in metastatic castration resistant prostate cancer after chemotherapy, abiraterone and/or enzalutamide. A retrospective analysis of overall survival. Eur. J. Nucl. Med. Mol. Imaging 2017, 45, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Schlolaut, S.; Fimmers, R.; Yordanova, A.; Hirzebruch, S.; Schlenkhoff, C.; Gaertner, F.C.; Awang, Z.H.; Hauser, S.; Essler, M. Predictors of overall survival in metastatic castration-resistant prostate cancer patients receiving [177Lu] Lu-PSMA-617 radioligand therapy. Oncotarget 2014, 5, 103108–103116. [Google Scholar] [CrossRef] [Green Version]
- Barber, T.W.; Singh, A.; Kulkarni, H.R.; Niepsch, K.; Billah, B.; Baum, R.P. Clinical outcomes of 177Lu-PSMA radioligand therapy in earlier and later phases of metastatic castration-resistant prostate cancer grouped by previous taxane chemotherapy. J. Nucl. Med. 2019, 60, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Ferdinandus, J.; Eppard, E.; Gaertner, F.C.; Kürpig, S.; Fimmers, R.; Yordanova, A.; Hauser, S.; Feldmann, G.; Essler, M.; Ahmadzadehfar, H. Predictors of response to radioligand therapy of metastatic castrate-resistant prostate cancer with 177Lu-PSMA-617. J. Nucl. Med. 2016, 58, 312–319. [Google Scholar] [CrossRef]
- Ferdinandus, J.; Violet, J.; Sandhu, S.; Hicks, R.J.; Kumar, A.S.R.; Iravani, A.; Kong, G.; Akhurst, T.; Thang, S.P.; Murphy, D.G.; et al. Prognostic biomarkers in men with metastatic castration-resistant prostate cancer receiving [177Lu]-PSMA-617. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2322–2327. [Google Scholar] [CrossRef]
- Prasad, V.; Huang, K.; Prasad, S.; Makowski, M.R.; Czech, N.; Brenner, W. In comparison to PSA, Interim Ga-68-PSMA PET/CT response evaluation based on modified RECIST 1.1 after 2nd cycle is better predictor of overall survival of prostate cancer patients treated with 177Lu-PSMA. Front. Oncol. 2021, 11, 291. [Google Scholar] [CrossRef]
- Grubmüller, B.; Senn, D.; Kramer, G.; Baltzer, P.; D’Andrea, D.; Grubmüller, K.H.; Mitterhauser, M.; Eidherr, H.; Haug, A.R.; Wadsak, W.; et al. Response assessment using 68Ga-PSMA ligand PET in patients undergoing 177Lu-PSMA radioligand therapy for metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1063–1072. [Google Scholar] [CrossRef] [Green Version]
- Kesavan, M.; Turner, J.H. Myelotoxicity of peptide receptor radionuclide therapy of neuroendocrine tumors: A decade of experience. Cancer Biother. Radiopharm. 2016, 31, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Sabet, A.; Ezziddin, K.; Pape, U.-F.; Ahmadzadehfar, H.; Mayer, K.; Pöppel, T.; Guhlke, S.; Biersack, H.-J.; Ezziddin, S. Long-term hematotoxicity after peptide receptor radionuclide therapy with 177Lu-octreotate. J. Nucl. Med. 2013, 54, 1857–1861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogelzang, N.J.; Coleman, R.E.; Michalski, J.M.; Nilsson, S.; O’Sullivan, J.M.; Parker, C.; Widmark, A.; Thuresson, M.; Xu, L.; Germino, J.; et al. Hematologic safety of radium-223 dichloride: Baseline prognostic factors associated with myelosuppression in the ALSYMPCA trial. Clin. Genitourin. Cancer 2017, 15, 42–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifert, R.; Kessel, K.; Schlack, K.; Weckesser, M.; Bögemann, M.; Rahbar, K. Radioligand therapy using [177Lu] Lu-PSMA-617 in MCRPC: A pre-VISION single-center analysis. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2106–2112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begum, N.J.; Thieme, A.; Eberhardt, N.; Tauber, R.; D’Alessandria, C.; Beer, A.J.; Glatting, G.; Eiber, M.; Kletting, P. The effect of total tumor volume on the biologically effective dose to tumor and kidneys for 177Lu-labeled PSMA peptides. J. Nucl. Med. 2018, 59, 929–933. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 45) |
|---|---|
| Age | 71 (68–76) |
| PSA (µg/L) | 551 (339–1280) |
| ALP (U/L) | 373 (153–598) |
| LDH (U/L) | 297 (239–440) |
| Hemoglobin (g/L) | 10.4 (8.8–11.3) |
| White blood cells (109/L) | 6.2 (4.9–7.7) |
| Platelets (109/L) | 215 (148–289) |
| eGFR (mL/min/1.73 m2) | 88.2 (70–96.6) |
| Gleason score * | |
| <8 | 12 (32) |
| ≥8 | 25 (68) |
| ECOG performance status | |
| 1 | 20 (44) |
| 2–3 | 25 (56) |
| Pain | |
| No pain/controlled pain | 21 (47) |
| Pain | 24 (53) |
| Sites of metastases | |
| Bone | 45 (100) |
| Lymph nodes | 26 (58) |
| Visceral | 10 (22) |
| - hepatic | 5 (11) |
| - pulmonary | 3 (7) |
| Prior systemic therapies for mCRPC | |
| Abiraterone | 34 (76) |
| Enzalutamide | 32 (71) |
| 223Ra-dichloride | 12 (27) |
| Docetaxel | 36 (80) |
| Cabazitaxel | 20 (44) |
| Other chemotherapies ** | 2 (4) |
| External beam radiotherapy | |
| Primary site | 17 (38) |
| Metastatic site | 22 (49) |
| Risk Factor | Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|---|
| n | (%) | p | HR | 95% CI | p | ||
| Gleason score * | |||||||
| <8 | 12 | 32 | |||||
| ≥8 | 25 | 68 | 0.52 | ||||
| ECOG status at baseline | |||||||
| 1 | 20 | 44 | |||||
| 2–3 | 25 | 56 | 0.47 | ||||
| Visceral metastases at baseline | |||||||
| - any | 10 | 22 | 0.23 | ||||
| - hepatic | 5 | 11 | 0.07 | 1.82 | (0.54–6.17) | 0.34 | |
| Previous mCRPC therapies | |||||||
| - Taxane-based chemotherapy | 36 | 80 | 0.02 | 3.21 | (1.18–8.70) | 0.02 | |
| - 223Ra-dichloride | 12 | 27 | 0.90 | ||||
| - Palliative radiotherapy | 22 | 49 | 0.41 | ||||
| Continuous baseline variables | |||||||
| PSA (per ng/mL) | 0.48 | ||||||
| ALP (per unit) | 0.43 | ||||||
| LDH (per unit) | 0.02 | 1.001 | (1.000–1.001) | 0.04 | |||
| Toxicity | Baseline (%) | Intra-/Posttherapeutic (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | ||
| Anemia | 25 (56) | 16 (36) | 3 (7) | 0 (0) | 10 (22) | 18 (40) | 17 (38) | 0 (0) | |
| Leukopenia | 2 (4) | 4 (9) | 0 (0) | 0 (0) | 17 (38) | 11 (24) | 6 (13) | 0 (0) | |
| Thrombocytopenia | 8 (18) | 1 (2) | 0 (0) | 0 (0) | 18 (40) | 10 (22) | 6 (13) | 2 (4) | |
| Chronic kidney disease (eGFR) | 19 (42) | 7 (16) | 0 (0) | 0 (0) | 21 (47) | 13 (29) | 0 (0) | 0 (0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groener, D.; Baumgarten, J.; Haefele, S.; Happel, C.; Klimek, K.; Mader, N.; Nguyen Ngoc, C.; Tselis, N.; Chun, F.K.H.; Grünwald, F.; et al. Salvage Radioligand Therapy with Repeated Cycles of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer with Diffuse Bone Marrow Involvement. Cancers 2021, 13, 4017. https://doi.org/10.3390/cancers13164017
Groener D, Baumgarten J, Haefele S, Happel C, Klimek K, Mader N, Nguyen Ngoc C, Tselis N, Chun FKH, Grünwald F, et al. Salvage Radioligand Therapy with Repeated Cycles of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer with Diffuse Bone Marrow Involvement. Cancers. 2021; 13(16):4017. https://doi.org/10.3390/cancers13164017
Chicago/Turabian StyleGroener, Daniel, Justus Baumgarten, Sebastian Haefele, Christian Happel, Konrad Klimek, Nicolai Mader, Christina Nguyen Ngoc, Nikolaos Tselis, Felix K. H. Chun, Frank Grünwald, and et al. 2021. "Salvage Radioligand Therapy with Repeated Cycles of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer with Diffuse Bone Marrow Involvement" Cancers 13, no. 16: 4017. https://doi.org/10.3390/cancers13164017
APA StyleGroener, D., Baumgarten, J., Haefele, S., Happel, C., Klimek, K., Mader, N., Nguyen Ngoc, C., Tselis, N., Chun, F. K. H., Grünwald, F., & Sabet, A. (2021). Salvage Radioligand Therapy with Repeated Cycles of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer with Diffuse Bone Marrow Involvement. Cancers, 13(16), 4017. https://doi.org/10.3390/cancers13164017