
New Approaches in Characterization of Lesions Dissemination in DLBCL Patients on Baseline PET/CT



 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PET/CT Scanning
2.3. PET/CT Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
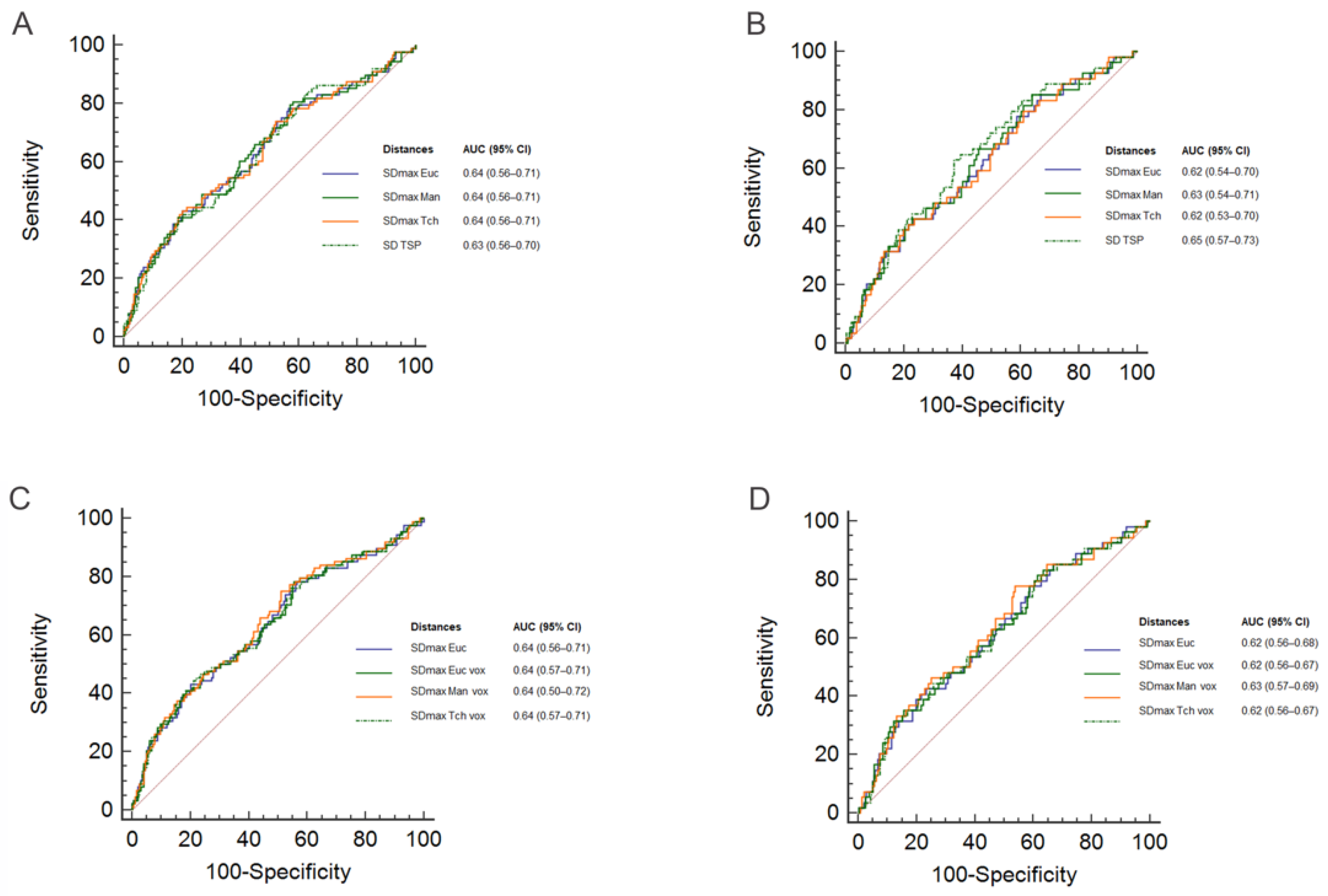
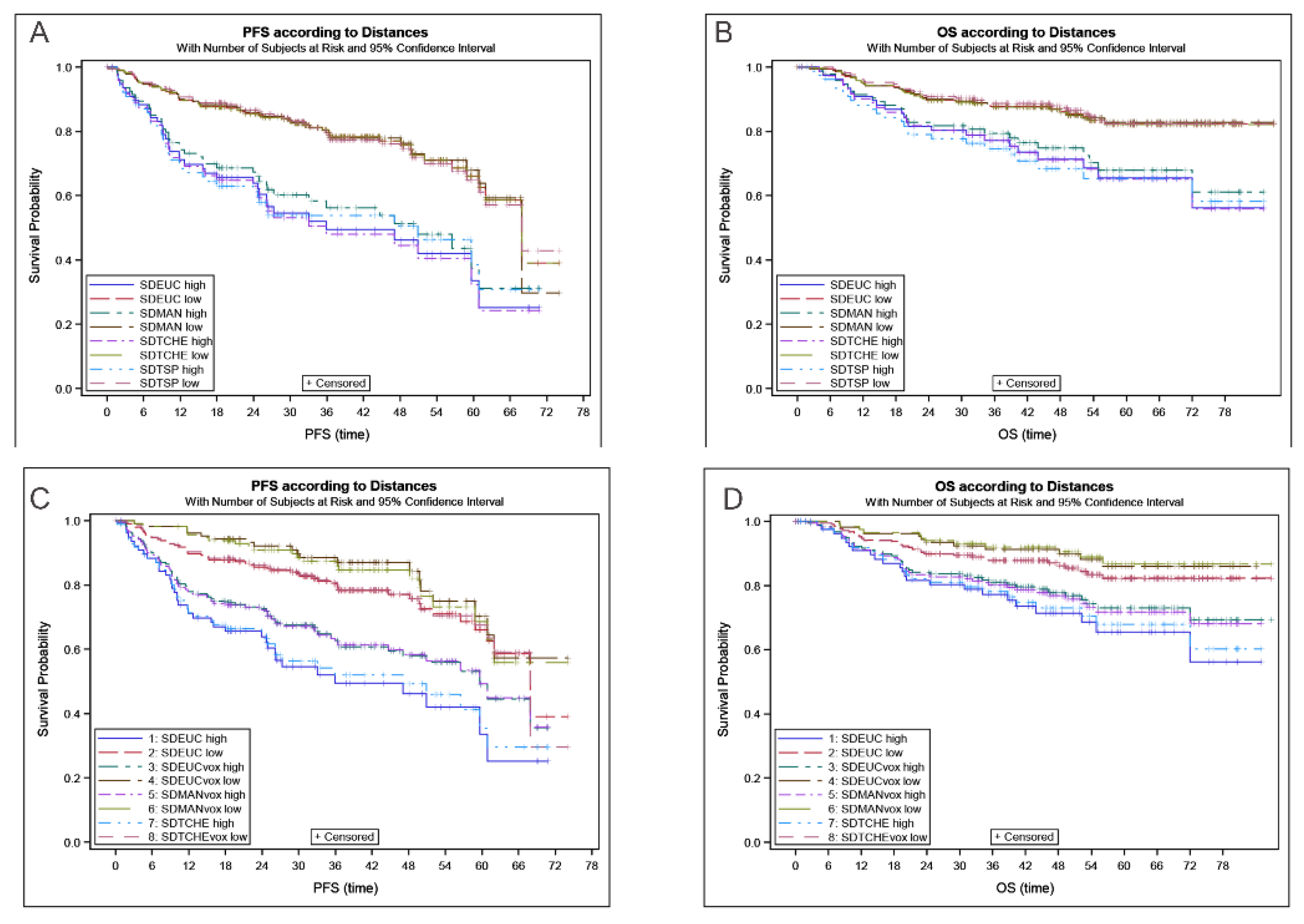
3.2. PET Characteristics
3.3. Comparison with Other Prognosticators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carbone, P.P.; Kaplan, H.S.; Musshoff, K.; Smithers, D.W.; Tubiana, M. Report of the Committee on Hodgkin’s Disease Staging Classification. Cancer Res. 1971, 31, 1860–1861. [Google Scholar]
- Rosenberg, S.A. Validity of the Ann Arbor staging classification for the non-Hodgkin’s lymphomas. Cancer Treat. Rep. 1977, 61, 1023–1027. [Google Scholar]
- Chaganti, S.; Illidge, T.; Barrington, S.; McKay, P.; Linton, K.; Cwynarski, K.; McMillan, A.; Davies, A.; Stern, S.; Peggs, K.; et al. Guidelines for the management of diffuse large B-cell lymphoma. Br. J. Haematol. 2016, 174, 43–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sehn, L.H.; Gascoyne, R.D. Diffuse large B-cell lymphoma: Optimizing outcome in the context of clinical and biologic heterogeneity. Blood 2015, 125, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Thieblemont, C.; Tilly, H.; Gomes da Silva, M.; Casasnovas, R.O.; Fruchart, C.; Morschhauser, F.; Haioun, C.; Lazarovici, J.; Grosicka, A.; Perrot, A.; et al. Lenalidomide Maintenance Compared With Placebo in Responding Elderly Patients With Diffuse Large B-Cell Lymphoma Treated With First-Line Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone. J. Clin. Oncol. 2017, 35, 2473–2481. [Google Scholar] [CrossRef] [PubMed]
- Mikhaeel, N.G.; Smith, D.; Dunn, J.T.; Phillips, M.; Moller, H.; Fields, P.A.; Wrench, D.; Barrington, S.F. Combination of baseline metabolic tumour volume and early response on PET/CT improves progression-free survival prediction in DLBCL. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1209–1219. [Google Scholar] [CrossRef] [Green Version]
- Cottereau, A.S.; Lanic, H.; Mareschal, S.; Meignan, M.; Vera, P.; Tilly, H.; Jardin, F.; Becker, S. Molecular Profile and FDG-PET/CT Total Metabolic Tumor Volume Improve Risk Classification at Diagnosis for Patients with Diffuse Large B-Cell Lymphoma. Clin. Cancer Res. 2016, 22, 3801–3809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostakoglu, L.; Martelli, M.; Sehn, L.H.; Belada, D.; Carella, A.M.; Chua, N.; Gonzalez-Barca, E.; Hong, X.; Pinto, A.; Shi, Y.; et al. Baseline PET-Derived Metabolic Tumor Volume Metrics Predict Progression-Free and Overall Survival in DLBCL after First-Line Treatment: Results from the Phase 3 GOYA Study. Blood 2017, 130, 824. [Google Scholar] [CrossRef]
- Schmitz, C.; Huttmann, A.; Muller, S.P.; Hanoun, M.; Boellaard, R.; Brinkmann, M.; Jockel, K.H.; Duhrsen, U.; Rekowski, J. Dynamic risk assessment based on positron emission tomography scanning in diffuse large B-cell lymphoma: Post-hoc analysis from the PETAL trial. Eur. J. Cancer 2020, 124, 25–36. [Google Scholar] [CrossRef] [Green Version]
- Cottereau, A.S.; Nioche, C.; Dirand, A.S.; Clerc, J.; Morschhauser, F.; Casasnovas, O.; Meignan, M.; Buvat, I. (18)F-FDG PET Dissemination Features in Diffuse Large B-Cell Lymphoma Are Predictive of Outcome. J. Nucl. Med. 2020, 61, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Cottereau, A.S.; Meignan, M.; Nioche, C.; Capobianco, N.; Clerc, J.; Chartier, L.; Vercellino, L.; Casasnovas, O.; Thieblemont, C.; Buvat, I. Risk stratification in diffuse large B cell lymphoma using lesion dissemination and metabolic tumor burden calculated from baseline PET/CT. Ann. Oncol. 2021, 32, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Jemaa, S.; Fredrickson, J.; Carano, R.A.D.; Nielsen, T.; de Crespigny, A.; Bengtsson, T. Tumor Segmentation and Feature Extraction from Whole-Body FDG-PET/CT Using Cascaded 2D and 3D Convolutional Neural Networks. J. Digit. Imaging 2020, 33, 888–894. [Google Scholar] [CrossRef]
- Vercellino, L.; Cottereau, A.S.; Casasnovas, R.O.; Tilly, H.; Feugier, P.; Chartier, L.; Fruchart, C.; Roulin, L.; Oberic, L.; Pica, G.M.; et al. High total metabolic tumor volume at baseline allows discrimination of survival even in patients aged 60 to 80 years responding to R-CHOP. Blood 2020. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef]
- Capobianco, N.; Meignan, M.A.; Cottereau, A.S.; Vercellino, L.; Sibille, L.; Spottiswoode, B.; Zuehlsdorff, S.; Casasnovas, O.; Thieblemont, C.; Buvat, I. Deep learning FDG uptake classification enables total metabolic tumor volume estimation in diffuse large B-cell lymphoma. J. Nucl. Med. 2021, 62, 30–36. [Google Scholar] [CrossRef]
- Grossiord, E.; Talbot, H.; Passat, N.; Meignan, M.; Terv´e, P.; Najman, L. Hierarchies and shape –space for PET image segmentation. In Proceedings of the 2015 IEEE International Symposium on Biomedical Imaging, Brooklyn, NY, USA, 16–19 April 2015; pp. 1118–1121. [Google Scholar]
- Meignan, M.; Sasanelli, M.; Casasnovas, R.O.; Luminari, S.; Fioroni, F.; Coriani, C.; Masset, H.; Itti, E.; Gobbi, P.G.; Merli, F.; et al. Metabolic tumour volumes measured at staging in lymphoma: Methodological evaluation on phantom experiments and patients. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuze, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A Freeware for Radiomic Feature Calculation in Multimodality Imaging to Accelerate Advances in the Characterization of Tumor Heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [Green Version]
- Vercellino, L.; Cottereau, A.S.; Casasnovas, O.; Tilly, H.; Feugier, P.; Chartier, L.; Fruchart, C.; Roulin, L.; Oberic, L.; Pica, G.M.; et al. High total metabolic tumor volume at baseline predicts survival independent of response to therapy. Blood 2020, 135, 1396–1405. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Durand, P.; Jegou, S.; Kanoun, S.; Berriolo-Riedinger, A.; Bodet-Milin, C.; Kraeber-Bodere, F.; Carlier, T.; Le Gouill, S.; Casasnovas, R.O.; Meignan, M.; et al. Fully automatic segmentation of diffuse large B cell lymphoma lesions on 3D FDG-PET/CT for total metabolic tumour volume prediction using a convolutional neural network. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Mueller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of imaging in the staging and response assessment of lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A.; Alliance, A.L.; Lymphoma, G.; Eastern Cooperative Oncology, G.; et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, D.M.; Scherer, F.; Jin, M.C.; Soo, J.; Craig, A.F.M.; Esfahani, M.S.; Chabon, J.J.; Stehr, H.; Liu, C.L.; Tibshirani, R.; et al. Circulating Tumor DNA Measurements As Early Outcome Predictors in Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. 2018, 36, 2845–2853. [Google Scholar] [CrossRef] [PubMed]
- Chapuy, B.; Stewart, C.; Dunford, A.J.; Kim, J.; Kamburov, A.; Redd, R.A.; Lawrence, M.S.; Roemer, M.G.M.; Li, A.J.; Ziepert, M.; et al. Molecular subtypes of diffuse large B cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat. Med. 2018, 24, 679–690. [Google Scholar] [CrossRef]
- Onaindia, A.; Santiago-Quispe, N.; Iglesias-Martinez, E.; Romero-Abrio, C. Molecular Update and Evolving Classification of Large B-Cell Lymphoma. Cancers 2021, 13, 3352. [Google Scholar] [CrossRef]
- Thieblemont, C.; Chartier, L.; Dührsen, U.; Vitolo, U.; Barrington, S.F.; Vercellino, L.; Zaucha, J.; Patrocinio Carvalho, I.; Maria, G.d.S.; Decazes, P.; et al. The Combination of High Total Metabolic Tumor Volume and Poor ECOG Performance Status Defines Ultra-High Risk Diffuse Large B-Cell Lymphoma. Validation across Multiple Cohorts of Large Clinical Trials and in Real World. Blood 2020, 136, 30–31. [Google Scholar] [CrossRef]
- Eertink, J.J.; van de Brug, T.; Wiegers, S.E.; Zwezerijnen, G.J.C.; Pfaehler, E.; Lugtenburg, P.J.; van der Holt, B.; de Vet, H.C.W.; Hoekstra, O.S.; Boellaard, R.; et al. 18f-FDG PET/CT Baseline Rdiomics Features Improve the Prediction of Treatment Outcome in Diffuse Large B-Cell Lymphoma Patients. Blood 2020, 136, 27–28. [Google Scholar] [CrossRef]
- Lugtenburg, P.J.; de Nully Brown, P.; van der Holt, B.; D’Amore, F.A.; Koene, H.R.; de Jongh, E.; Fijnheer, R.; van Esser, J.W.; Bohmer, L.H.; Pruijt, J.F.; et al. Rituximab-CHOP With Early Rituximab Intensification for Diffuse Large B-Cell Lymphoma: A Randomized Phase III Trial of the HOVON and the Nordic Lymphoma Group (HOVON-84). J. Clin. Oncol. 2020, 38, 3377–3387. [Google Scholar] [CrossRef]
- Ceriani, L.M.; Cascione, L.; Gritti, G.; Dalmasso, F.; Esposito, F.; Schär, S.; Bruno, A.; Dirnhofer, S.; Giovanella, L.; Hayoz, S.; et al. Development and validation of a PET radiomics prognostic model for diffuse large B cell lymphoma. Hematol. Oncol. 2021, 39 (Suppl. 2), 51. [Google Scholar] [CrossRef]
- Durmo, R.; Ségolèn Cottereau, A.; Rebaud, L.; Nioche, C.; Ruffini, A.; Fioroni, F.; Meignan, M.; Buvat, I.; Merli, F.; Versari, A.; et al. Prognostic role of lesion dissemination feature (DMAX) calculated on baseline PET/CT in Hodgkin Lymphoma. Hematol. Oncol. 2021, 39 (Suppl. 2), 48–49. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Standardized Distances (m−1) | Mean | Median | SD | Q1–Q3 |
|---|---|---|---|---|
| SDmax_Euc | 0.230 | 0.232 | 0.12 | 0.13–0.33 |
| SDmax_Man | 0.296 | 0.293 | 0.15 | 0.17–0.41 |
| SDmax_Tch | 0.223 | 0.225 | 0.12 | 0.12–0.32 |
| SD_TSP | 0.765 | 0.657 | 0.56 | 0.34–1.03 |
| SDmax_Euc_Vox | 0.248 | 0.249 | 0.12 | 0.14–0.34 |
| SDmax_Man_Vox | 0.326 | 0.317 | 0.15 | 0.21–0.43 |
| SDmax_Tch_Vox | 0.240 | 0.245 | 0.12 | 0.13–0.34 |
| Method | SDmax _Euc | SDmax _Man | SDmax _Tch | SDTSP | SDmax _Euc_Vox | SDmax _Man_Vox | SDmax _Tch_Vox | |
|---|---|---|---|---|---|---|---|---|
| Kappa | SDmax_Euc | NA | 0.84 | 0.92 | 0.64 | 0.87 | 0.85 | 0.82 |
| PFS | HR | 2.90 | 2.70 | 3.11 | 2.95 | 3.58 | 2.84 | 3.66 |
| 95% CI | 1.8–4.7 | 1.7–4.2 | 2.0–4.9 | 1.7–5.1 | 2.2–5.8 | 1.8–4.5 | 2.2–6.1 | |
| p-value | <0.0001 | <0.0001 | <0.0001 | 0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Se | 0.27 | 0.32 | 0.30 | 0.18 | 0.25 | 0.30 | 0.23 | |
| Sp | 0.90 | 0.87 | 0.89 | 0.92 | 0.92 | 0.89 | 0.93 | |
| OS | HR | 2.66 | 2.60 | 2.90 | 3.11 | 3.10 | 2.85 | 2.93 |
| 95% CI | 1.4–4.8 | 1.5–4.6 | 1.6–5.2 | 1.6–6.0 | 1.7–5.7 | 1.6–5.1 | 1.5–5.6 | |
| p-value | 0.0013 | 0.0009 | 0.0003 | 0.0008 | 0.0003 | 0.0004 | 0.0011 | |
| Se | 0.28 | 0.33 | 0.31 | 0.20 | 0.26 | 0.31 | 0.22 | |
| Sp | 0.88 | 0.84 | 0.87 | 0.91 | 0.89 | 0.87 | 0.91 | |
| Factors | Multivariate Analysis of PFS | Multivariate Analysis of OS | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| High SDmax_Euc | 2.4 (1.5–4.0) | 0.0004 | 1.8 (0.98–3.4) | 0.0586 |
| MTV > 220 cm3 | 2.1 (1.3–3.3) | 0.0027 | 3.1 (1.6–6.0) | 0.0012 |
| ECOG 2–3 | 2.3 (1.4–3.8) | 0.0007 | 2.3 (1.3–4.0) | 0.0062 |
| HighSDmax_Man | 2.1 (1.3–3.4) | 0.0022 | 1.7 (0.91–3.0) | 0.0971 |
| MTV > 220 cm3 | 2.0 (1.2–3.2) | 0.0052 | 3.0 (1.5–6.0) | 0.0015 |
| ECOG 2–3 | 2.3 (1.4–3.7) | 0.0011 | 2.2 (1.2–4.0) | 0.0076 |
| High SDmax_Tch | 2.4 (1.5–3.9) | 0.0004 | 1.9 (1.0–3.4) | 0.0433 |
| MTV > 220 cm3 | 2.0 (1.2–3.2) | 0.0064 | 3.0 (1.5–5.8) | 0.0018 |
| ECOG 2–3 | 2.2 (1.4–3.6) | 0.0013 | 2.2 (1.2–4.0) | 0.0076 |
| High SD_TSP | 2.2 (1.2–3.9) | 0.0084 | 1.9 (0.93–3.8) | 0.081 |
| MTV > 220 cm3 | 2.0 (1.2–3.2) | 0.0055 | 3.0 (1.5–5.9) | 0.0018 |
| ECOG 2–3 | 2.4 (1.5–3.9) | 0.0005 | 2.4 (1.3–4.2) | 0.0038 |
| High SDmax_Euc _Vox | 2.7 (1.6–4.6) | 0.0001 | 2.0 (1.0–3.7) | 0.0389 |
| MTV > 220 cm3 | 2.0 (1.2–3.2) | 0.0051 | 3.0 (1.5–5.9) | 0.0014 |
| ECOG 2–3 | 2.3 (1.4–3.7) | 0.001 | 2.2 (1.2–4.0) | 0.0073 |
| High SDmax_Man_Vox | 2.3 (1.4–3.7) | 0.0006 | 1.9 (1.1–3.5) | 0.0306 |
| MTV > 220 cm3 | 2.0 (1.3–3.2) | 0.0038 | 3.0 (1.5–5.9) | 0.0013 |
| ECOG 2–3 | 2.3 (1.4–3.8) | 0.0006 | 2.2 (1.2–4.0) | 0.0068 |
| High SDmax_Tch_Vox | 2.8 (1.6–4.7) | 0.0002 | 1.8 (0.91–3.6) | 0.0911 |
| MTV > 220 cm3 | 2.0 (1.2–3.2) | 0.0048 | 3.1 (1.6–6.0) | 0.0012 |
| ECOG 2–3 | 2.2 (1.4–3.6) | 0.0012 | 2.2 (1.2–4.0) | 0.0075 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cottereau, A.-S.; Meignan, M.; Nioche, C.; Clerc, J.; Chartier, L.; Vercellino, L.; Casasnovas, O.; Thieblemont, C.; Buvat, I. New Approaches in Characterization of Lesions Dissemination in DLBCL Patients on Baseline PET/CT. Cancers 2021, 13, 3998. https://doi.org/10.3390/cancers13163998
Cottereau A-S, Meignan M, Nioche C, Clerc J, Chartier L, Vercellino L, Casasnovas O, Thieblemont C, Buvat I. New Approaches in Characterization of Lesions Dissemination in DLBCL Patients on Baseline PET/CT. Cancers. 2021; 13(16):3998. https://doi.org/10.3390/cancers13163998
Chicago/Turabian StyleCottereau, Anne-Ségolène, Michel Meignan, Christophe Nioche, Jérôme Clerc, Loic Chartier, Laetitia Vercellino, Olivier Casasnovas, Catherine Thieblemont, and Irène Buvat. 2021. "New Approaches in Characterization of Lesions Dissemination in DLBCL Patients on Baseline PET/CT" Cancers 13, no. 16: 3998. https://doi.org/10.3390/cancers13163998
APA StyleCottereau, A.-S., Meignan, M., Nioche, C., Clerc, J., Chartier, L., Vercellino, L., Casasnovas, O., Thieblemont, C., & Buvat, I. (2021). New Approaches in Characterization of Lesions Dissemination in DLBCL Patients on Baseline PET/CT. Cancers, 13(16), 3998. https://doi.org/10.3390/cancers13163998