
Frequency of CDH1 Germline Mutations in Non-Gastric Cancers


 , ,
, ,  and
and
Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
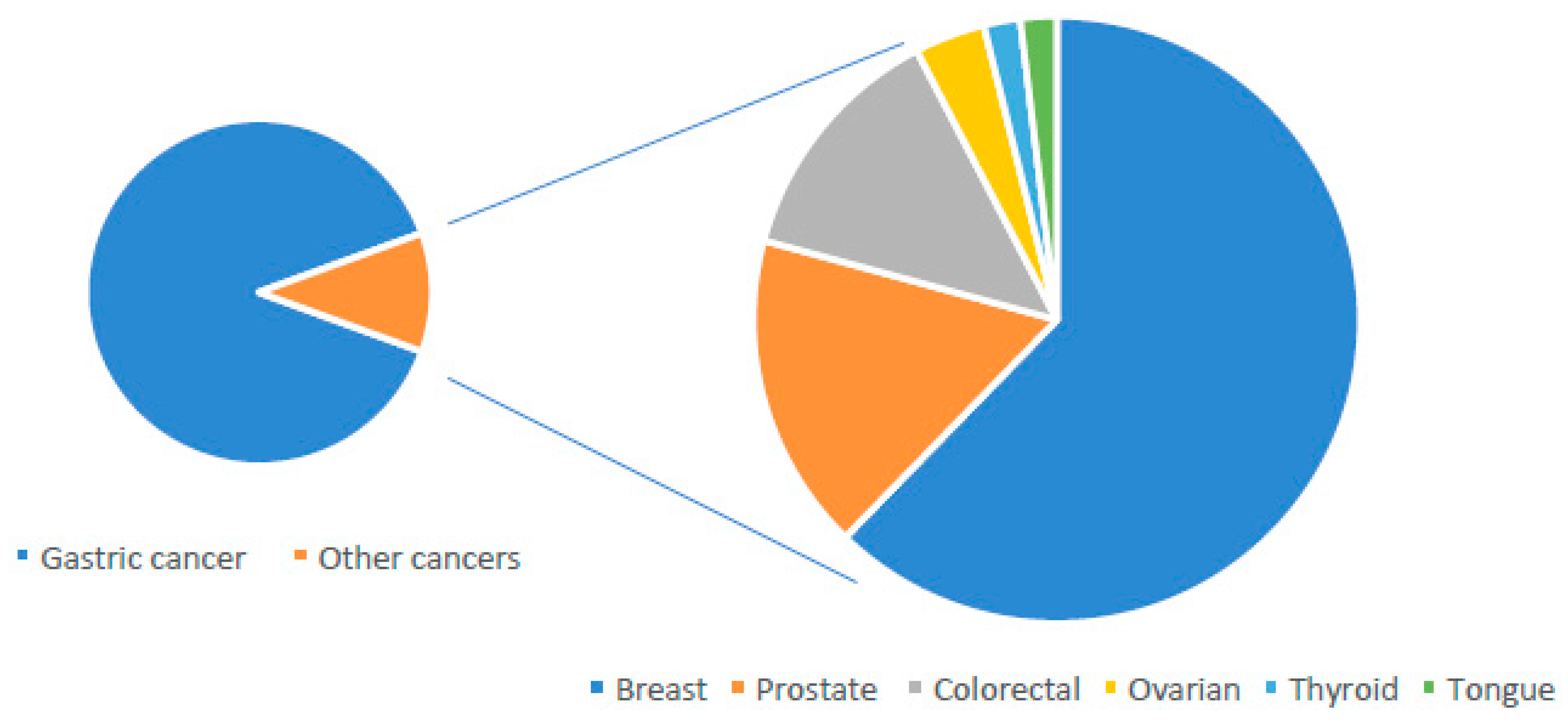
3.1. Other Types of Cancer
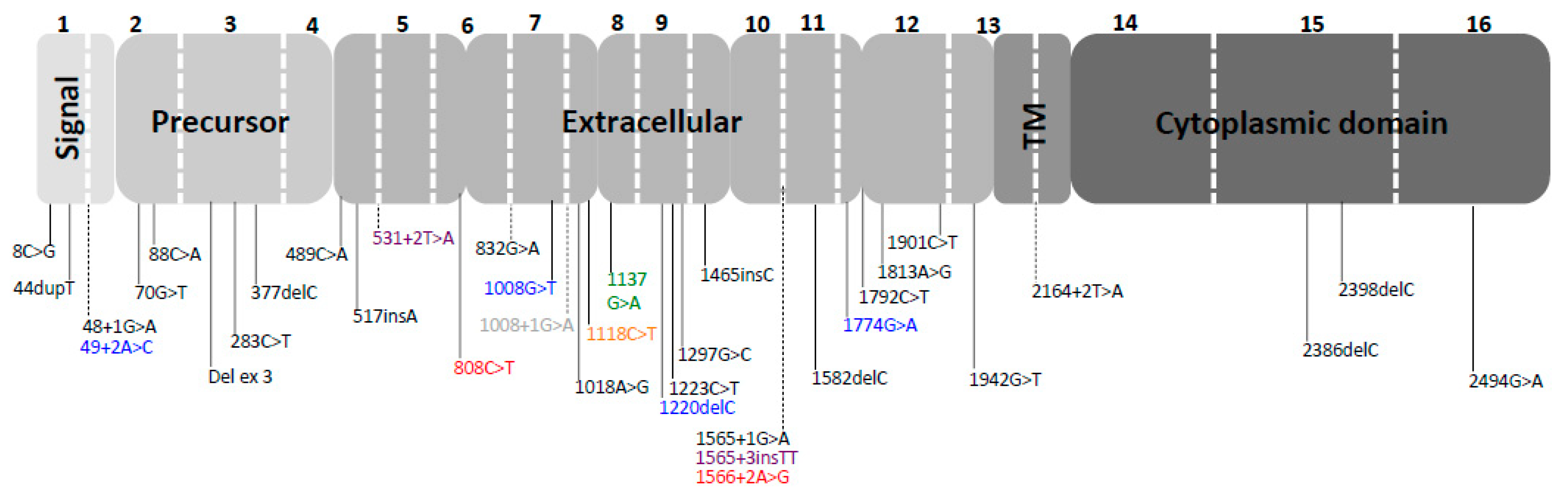
3.2. Type of Mutations
4. Discussion
4.1. First Point
4.2. Second Point
4.3. Third Point
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Corso, G.; Montagna, G.; Figueiredo, J.; La Vecchia, C.; Fumagalli Romario, U.; Fernandes, M.S.; Seixas, S.; Roviello, F.; Trovato, C.; Guerini-Rocco, E.; et al. Hereditary Gastric and Breast Cancer Syndromes Related to CDH1 Germline Mutation: A Multidisciplinary Clinical Review. Cancers 2020, 12, 1598. [Google Scholar] [CrossRef]
- Blair, V.R.; McLeod, M.; Carneiro, F.; Coit, D.G.; D’Addario, J.L.; van Dieren, J.M.; Harris, K.L.; Hoogerbrugge, N.; Oliveira, C.; van der Post, R.S.; et al. Hereditary diffuse gastric cancer: Updated clinical practice guidelines. Lancet Oncol. 2020, 21, 386–397. [Google Scholar] [CrossRef]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric Cancer Syndrome: CDH1 Mutations and Beyond. JAMA Oncol. 2015, 1, 23–32. [Google Scholar] [CrossRef]
- Caldas, C.; Carneiro, F.; Lynch, H.T.; Yokota, J.; Wiesner, G.L.; Powell, S.M.; Lewis, F.R.; Huntsman, D.G.; Pharoah, P.D.; Jankowski, J.A.; et al. Familial gastric cancer: Overview and guidelines for management. J. Med. Genet. 1999, 36, 873–880. [Google Scholar]
- Corso, G.; Figueiredo, J.; La Vecchia, C.; Veronesi, P.; Pravettoni, G.; Macis, D.; Karam, R.; Lo Gullo, R.; Provenzano, E.; Toesca, A.; et al. Hereditary lobular breast cancer with an emphasis on E-cadherin genetic defect. J. Med. Genet. 2018, 55, 431–441. [Google Scholar] [CrossRef]
- Frebourg, T.; Oliveira, C.; Hochain, P.; Karam, R.; Manouvrier, S.; Graziadio, C.; Vekemans, M.; Hartmann, A.; Baert-Desurmont, S.; Alexandre, C.; et al. Cleft lip/palate and CDH1/E-cadherin mutations in families with hereditary diffuse gastric cancer. J. Med. Genet. 2006, 43, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Corso, G.; Corso, F.; Bellerba, F.; Carneiro, P.; Seixas, F.; Cioffi, A.; La Vecchia, C.; Magnoni, F.; Bonanni, B.; Veronesi, P.; et al. Geographical Distribution of E-cadherin Germline Mutations in the Context of Diffuse Gastric Cancer: A Systematic Review. Cancers 2021, 13, 1269. [Google Scholar] [CrossRef] [PubMed]
- Ikonen, T.; Matikainen, M.; Mononen, N.; Hyytinen, E.; Helin, H.; Tommola, S.; Tammela, T.; Pukkala, E.; Schleutker, J.; Kallioniemi, O.; et al. Association of E-cadherin germ-line alterations with prostate cancer. Clin. Cancer Res. 2001, 7, 3465–3471. [Google Scholar]
- Oliveira, C.; Bordin, M.C.; Grehan, N.; Huntsman, D.; Suriano, G.; Machado, J.C.; Kiviluoto, T.; Aaltonen, L.; Jackson, C.E.; Seruca, R.; et al. Screening E-cadherin in gastric cancer families reveals germline mutations only in hereditary diffuse gastric cancer kindred. Hum. Mutat. 2002, 19, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Lynch, H.T.; Kaurah, P.; Wirtzfeld, D.; Rubinstein, W.S.; Weissman, S.; Lynch, J.F.; Grady, W.; Wiyrick, S.; Senz, J.; Huntsman, D.G. Hereditary diffuse gastric cancer: Diagnosis, genetic counseling, and prophylactic total gastrectomy. Cancer 2008, 112, 2655–2663. [Google Scholar] [CrossRef]
- Chen, Q.H.; Deng, W.; Li, X.W.; Liu, X.F.; Wang, J.M.; Wang, L.F.; Xiao, N.; He, Q.; Wang, Y.P.; Fan, Y.M. Novel CDH1 germline mutations identified in Chinese gastric cancer patients. World J. Gastroenterol. 2013, 19, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Salahshor, S.; Haixin, L.; Huo, H.; Kristensen, V.; Loman, N.; Sjöberg-Margolin, S.; Borg, Å.; Børresen-Dale, A.; Vorechovsky, I.; Lindblom, A. Low frequency of E-cadherin alterations in familial breast cancer. Breast Cancer Res. 2001, 3, 199–207. [Google Scholar] [CrossRef]
- Katona, B.W.; Clark, D.F.; Domchek, S. CDH1 on Multigene Panel Testing: Look Before You Leap. J. Natl. Cancer Inst. 2020, 112, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Gullo, I.; Devezas, V.; Baptista, M.; Garrido, L.; Castedo, S.; Morais, R.; Wen, X.; Rios, E.; Pinheiro, J.; Pinto-Ribeiro, I.; et al. Phenotypic heterogeneity of hereditary diffuse gastric cancer: Report of a family with early-onset disease. Gastrointest. Endosc. 2018, 87, 1566–1575. [Google Scholar] [CrossRef]
- López, M.; Cervera-Acedo, C.; Santibáñez, P.; Salazar, R.; Sola, J.J.; Domínguez-Garrido, E. A novel mutation in the CDH1 gene in a Spanish family with hereditary diffuse gastric cancer. Springerplus 2016, 5, 1181. [Google Scholar] [CrossRef] [PubMed]
- Bardram, L.; Hansen, T.V.; Gerdes, A.M.; Timshel, S.; Friis-Hansen, L.; Federspiel, B. Prophylactic total gastrectomy in hereditary diffuse gastric cancer: Identification of two novel CDH1 gene mutations-a clinical observational study. Fam. Cancer 2014, 13, 231–242. [Google Scholar] [CrossRef] [PubMed]
- More, H.; Humar, B.; Weber, W.; Ward, R.; Christian, A.; Lintott, C.; Graziano, F.; Ruzzo, A.M.; Acosta, E.; Boman, B.; et al. Identification of seven novel germline mutations in the human E-cadherin (CDH1) gene. Hum. Mutat. 2007, 28, 203. [Google Scholar] [CrossRef]
- Kluijt, I.; Siemerink, E.J.; Ausems, M.G.; van Os, T.A.; de Jong, D.; Simões-Correia, J.; van Krieken, J.H.; Ligtenberg, M.J.; Figueiredo, J.; van Riel, E.; et al. CDH1-related hereditary diffuse gastric cancer syndrome: Clinical variations and implications for counseling. Int. J. Cancer 2012, 131, 367–376. [Google Scholar] [CrossRef]
- Guilford, P.; Humar, B.; Blair, V. Hereditary diffuse gastric cancer: Translation of CDH1 germline mutations into clinical practice. Gastric Cancer 2010, 13, 1–10. [Google Scholar] [CrossRef]
- Keller, G.; Vogelsang, H.; Becker, I.; Plaschke, S.; Ott, K.; Suriano, G.; Mateus, A.R.; Seruca, R.; Biedermann, K.; Huntsman, D.; et al. Germline mutations of the E-cadherin (CDH1) and TP53 genes, rather than of RUNX3 and HPP1, contribute to genetic predisposition in German gastric cancer patients. J. Med. Genet. 2004, 41, e89. [Google Scholar] [CrossRef]
- Masciari, S.; Larsson, N.; Senz, J.; Boyd, N.; Kaurah, P.; Kandel, M.; Harris, L.; Pinheiro, H.; Troussard, A.; Miron, P.; et al. Germline E-cadherin mutations in familial lobular breast cancer. J. Med. Genet. 2007, 44, 726–731. [Google Scholar] [CrossRef]
- Schrader, K.; Masciari, S.; Boyd, N.; Salamanca, C.; Senz, J.; Saunders, D.; Yorida, E.; Maines-Bandiera, S.; Kaurah, P.; Tung, N.; et al. Germline mutations in CDH1 are infrequent in women with early-onset or familial lobular breast cancers. J. Med. Genet. 2011, 48, 64–68. [Google Scholar] [CrossRef]
- Takeichi, M. Cadherins in cancer: Im- plications for invasion and metastasis. Curr. Opin. Cell Biol. 1993, 5, 806–811. [Google Scholar] [CrossRef]
- Takeichi, M. Cadherin cell adhesion receptors as a morphogenetic regulator. Science 1991, 251, 1451–1455. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Li, L.; Laquet, C.; Penault-Llorca, F.; Uhrhammer, N.; Xie, X.M.; Bignon, Y.J. Germline mutations of the E-cadherin gene in families with inherited invasive lobular breast carcinoma but no diffuse gastric cancer. Cancer 2011, 117, 3112–3117. [Google Scholar] [CrossRef]
- Manchana, T.; Phowthongkum, P.; Teerapakpinyo, C. Germline mutations in Thai patients with nonmucinous epithelial ovarian cancer. World J. Clin. Oncol. 2019, 10, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.; Torre, L.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Lyons, K.; Le, L.C.; Pham, Y.T.; Borron, C.; Park, J.Y.; Tran, C.T.D.; Tran, T.V.; Tran, H.T.; Vu, K.T.; Do, C.D.; et al. Gastric cancer: Epidemiology, biology, and prevention: A mini review. Eur. J. Cancer Prev. 2019, 28, 397–412. [Google Scholar] [CrossRef]
- Corso, G.; Carvalho, J.; Marrelli, D.; Vindigni, C.; Carvalho, B.; Seruca, R.; Roviello, F.; Oliveira, C. Somatic mutations and deletions of the E-cadherin gene predict poor survival of patients with gastric cancer. J. Clin. Oncol. 2013, 31, 868–875. [Google Scholar] [CrossRef]
- Yaghoobi, M.; McNabb-Baltar, J.; Bijarchi, R.; Hunt, R. What is the quantitative risk of gastric cancer in the first-degree relatives of patients? A meta-analysis. World J. Gastroenterol. 2017, 23, 2435–2442. [Google Scholar] [CrossRef]
- Gorini, A.; Miglioretti, M.; Pravettoni, G. A new perspective on blame culture: An experimental study. J. Eval. Clin. Pract. 2012, 18, 671–675. [Google Scholar] [CrossRef]
- Oliveri, S.; Ferrari, F.; Manfrinati, A.; Pravettoni, G. A systematic review of the psychological implications of genetic testing: A comparative analysis among cardiovascular, neurodegenerative and cancer diseases. Front. Genet. 2018, 9, 624. [Google Scholar] [CrossRef] [PubMed]
- Masiero, M.; Riva, S.; Fioretti, C.; Pravettoni, G. Pediatric blood cancer survivors and tobacco use across adolescence and emerging adulthood: A narrative review. Front. Psychol. 2016, 7, 392. [Google Scholar] [CrossRef]
- Berx, G.; Cleton-Jansen, A.M.; Nollet, F.; de Leeuw, W.J.; Van de Vijver, M.; Cornelisse, C. E-cadherin is a tumour/inva- sion suppressor gene mutated in human lobular breast cancers. EMBO J. 1995, 14, 6107–6115. [Google Scholar] [CrossRef] [PubMed]
- Christofori, G.; Semb, H. The role of the cell-adhesion molecule E-cadherin as a tumour-suppressor gene. Trends Biochem. Sci. 1999, 24, 73–76. [Google Scholar] [CrossRef]
- Guilford, P.; Hopkins, J.; Harraway, J.; McLeod, M.; McLeod, N.; Harawira, P.; Taite, H.; Scoular, R.; Miller, A.; Reeve, A.E. E-cadherin germline mutations in familial gastric cancer. Nature 1998, 392, 402–405. [Google Scholar] [CrossRef]
- Benusiglio, P.R.; Malka, D.; Rouleau, E.; De Pauw, A.; Buecher, B.; Noguès, C.; Fourme, E.; Colas, C.; Coulet, F.; Warcoin, M.; et al. CDH1 germline mutations and the hereditary diffuse gastric and lobular breast cancer syndrome: A multicentre study. J. Med. Genet. 2013, 50, 486–489. [Google Scholar] [CrossRef]
- Petridis, C.; Shinomiya, I.; Kohut, K.; Gorman, P.; Caneppele, M.; Shah, V.; Troy, M.; Pinder, S.E.; Hanby, A.; Tomlinson, I.; et al. Germline CDH1 mutations in bilateral lobular carcinoma in situ. Br. J. Cancer 2014, 110, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Gamble, C.; Havrilesky, L.; Myers, E.; Chino, J.; Hollenbeck, S.; Plichta, J.; Marcom, P.; Hwang, E.; Kauff, N.; Greenup, R. Cost Effectiveness of Risk-Reducing Mastectomy versus Surveillance in BRCA Mutation Carriers with a History of Ovarian Cancer. Ann. Surg. Oncol. 2017, 24, 3116–3123. [Google Scholar] [CrossRef]
- Carneiro, F.; Huntsman, D.G.; Smyrk, T.; Owen, D.; Seruca, R.; Pharoah, P.; Caldas, C.; Sobrinho-Simões, M. Model of the early development of diffuse gastric cancer in E-cadherin mutation carriers and its implications for patient screening. J. Pathol. 2004, 203, 681–687. [Google Scholar] [CrossRef]
- Melo, S.; Figueiredo, J.; Fernandes, M.; Gonçalves, M.; Morais-de-Sá, E.; Sanches, J.; Seruca, R. Predicting the Functional Impact of CDH1 Missense Mutations in Hereditary Diffuse Gastric Cancer. Int. J. Mol. Sci. 2017, 18, 2687. [Google Scholar] [CrossRef] [PubMed]
- Corso, G. Mutual exclusion of CDH1 and BRCA germline mutations in the pathway of hereditary breast cancer. Arch. Gynecol. Obstet. 2018, 297, 1067–1068. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author | Country | Type | HGVS | Localization | Protein | CDH1_DGC | CDH1_OC | OCs |
|---|---|---|---|---|---|---|---|---|
| Ikonen 2001 [8] | Finland | Missense | 808T>G | Ex_6 | S270A | - | 8 | PC |
| Oliveira 2002 [9] | Europe | Insertion | 44dupT | Ex_1 | - | 1 | 3 | CRC(2), LBC(1) |
| Lynch 2008 [10] | USA | Non sense | 70G>T | Ex_2 | - | 5 | 3 | BC |
| Xie 2011 29] | France | Non sense | 283C>T | Ex_3 | - | - | 3 | LBC |
| Chen 2013 [11] | China | Missense | 1018A>G | Ex_8 | T340A | - | 3 | LBC |
| Salahshor 2001 [12] | Sweden | Missense | 1774G>A | Ex_12 | A592T | - | 2 | CRC |
| Katona 2020 [13] | USA | Splice site | 1566+2A>G | In_10 | - | 1 | 1 | PC |
| Gullo 2018 [14] | Portugal | Missense | 1901C>T | Ex_12 | A634V | 7 | 1 | LBC |
| López 2016 [15] | Spain | Deletion | 1220delC | Ex_9 | - | 2 | 1 | CRC |
| Bardram 2014 [16] | Denmark | Insertion | 1565+3insTT | In_10 | - | 5 | 1 | Ca |
| More 2007 [17] | Caucasian | Splice site | 49+2A>C | In_1 | - | 3 | 1 | CRC |
| Caucasian | Splice site | 1137G>A | Ex_8 | - | 2 | 1 | ToC | |
| Kluijt 2012 [18] | Unknown | Non sense | 489C>A | Ex_4 | - | 2 | 1 | LBC |
| Guilford 2010 [19] | Europe | Non sense | 70G>T | Ex_2 | - | 3 | 1 | BC |
| Keller 2004 [20] | Germany | Deletion | 377delC | Ex_3 | - | 2 | 1 | LBC |
| Frebourg 2006 [6] | Caucasian | Splice site | 531+2T>A | In_4 | - | 3 | 1 | Ca |
| Guilford 2010 [20] | Maori | Splice site | 1008G>T | Ex_7 | - | 9 | 1 | CRC |
| Oliveira 2002 [9] | Pakistan | Splice site | 832G>A | Ex_6 | - | 3 | 1 | LBC |
| Lynch 2008 [10] | USA | Non sense | 1792C>T | Ex_12 | - | 1 | 1 | BC |
| Masciari 2007 [21] | USA | Insertion | 517insA | Ex_4 | - | - | 1 | LBC |
| Schrader 2011 [22] | USA | Splice site | 1565+1G>A | In_10 | - | - | 1 | BC |
| Canada | Missense | 8C>G | Ex_1 | P3R | - | 1 | BC | |
| Canada | Missense | 88C>A | Ex_2 | P30T | - | 1 | BC | |
| Canada | Missense | 88C>A | Ex_2 | P30T | - | 1 | BC | |
| Canada | Missense | 1223C>T | Ex_9 | A408V | - | 1 | BC | |
| Canada | Missense | 1297G>C | Ex_9 | D433N | - | 1 | BC | |
| Canada | Missense | 1813A>G | Ex_12 | R605G | - | 1 | BC | |
| Canada | Missense | 2494G>A | Ex_16 | V832M | - | 1 | BC | |
| Petridis 2014 [23] | UK | Splice site | 48+1G>A | Ex_1 | - | - | 1 | LBC |
| UK | Insertion | 1465insC | Ex_10 | - | - | 1 | LBC | |
| UK | Missense | 1942G>T | Ex_13 | E648X | - | 1 | LBC | |
| UK | Deletion | 2398delC | Ex_15 | - | - | 1 | LBC | |
| Benusiglio 2013 [24] | France | Splice site | 2164+2T>A | In_13 | - | - | 1 | LBC |
| France | Deletion | del_ex_3 | Ex_3 | - | - | 1 | LBC | |
| France | Splice site | 1008+1G>A | In_7 | - | - | 1 | ThC | |
| France | Deletion | 2386delC | Ex_15 | - | - | 1 | LBC | |
| Xie 2011 [25] | France | Deletion | 1582delC | Ex_11 | - | - | 1 | LBC |
| Manchana 2019 [26] | Thailandia | Missense | 1118C>T | Ex_8 | P373L | - | 1 | OC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massari, G.; Magnoni, F.; Favia, G.; Peradze, N.; Veronesi, P.; La Vecchia, C.; Corso, G. Frequency of CDH1 Germline Mutations in Non-Gastric Cancers. Cancers 2021, 13, 2321. https://doi.org/10.3390/cancers13102321
Massari G, Magnoni F, Favia G, Peradze N, Veronesi P, La Vecchia C, Corso G. Frequency of CDH1 Germline Mutations in Non-Gastric Cancers. Cancers. 2021; 13(10):2321. https://doi.org/10.3390/cancers13102321
Chicago/Turabian StyleMassari, Giulia, Francesca Magnoni, Giorgio Favia, Nickolas Peradze, Paolo Veronesi, Carlo La Vecchia, and Giovanni Corso. 2021. "Frequency of CDH1 Germline Mutations in Non-Gastric Cancers" Cancers 13, no. 10: 2321. https://doi.org/10.3390/cancers13102321
APA StyleMassari, G., Magnoni, F., Favia, G., Peradze, N., Veronesi, P., La Vecchia, C., & Corso, G. (2021). Frequency of CDH1 Germline Mutations in Non-Gastric Cancers. Cancers, 13(10), 2321. https://doi.org/10.3390/cancers13102321