Combining Correlated Outcomes and Surrogate Endpoints in a Network Meta-Analysis of Colorectal Cancer Treatments


Simple Summary
Abstract
1. Background
2. Methods
2.1. Data Sources
2.2. Statistical Analyses
2.2.1. Multivariate Random Effects Model for Surrogate Endpoints
2.2.2. Network Meta-Regression Analysis of Treatment Therapies
3. Results
3.1. Association between Surrogacy Endpoint and Correlated Outcome
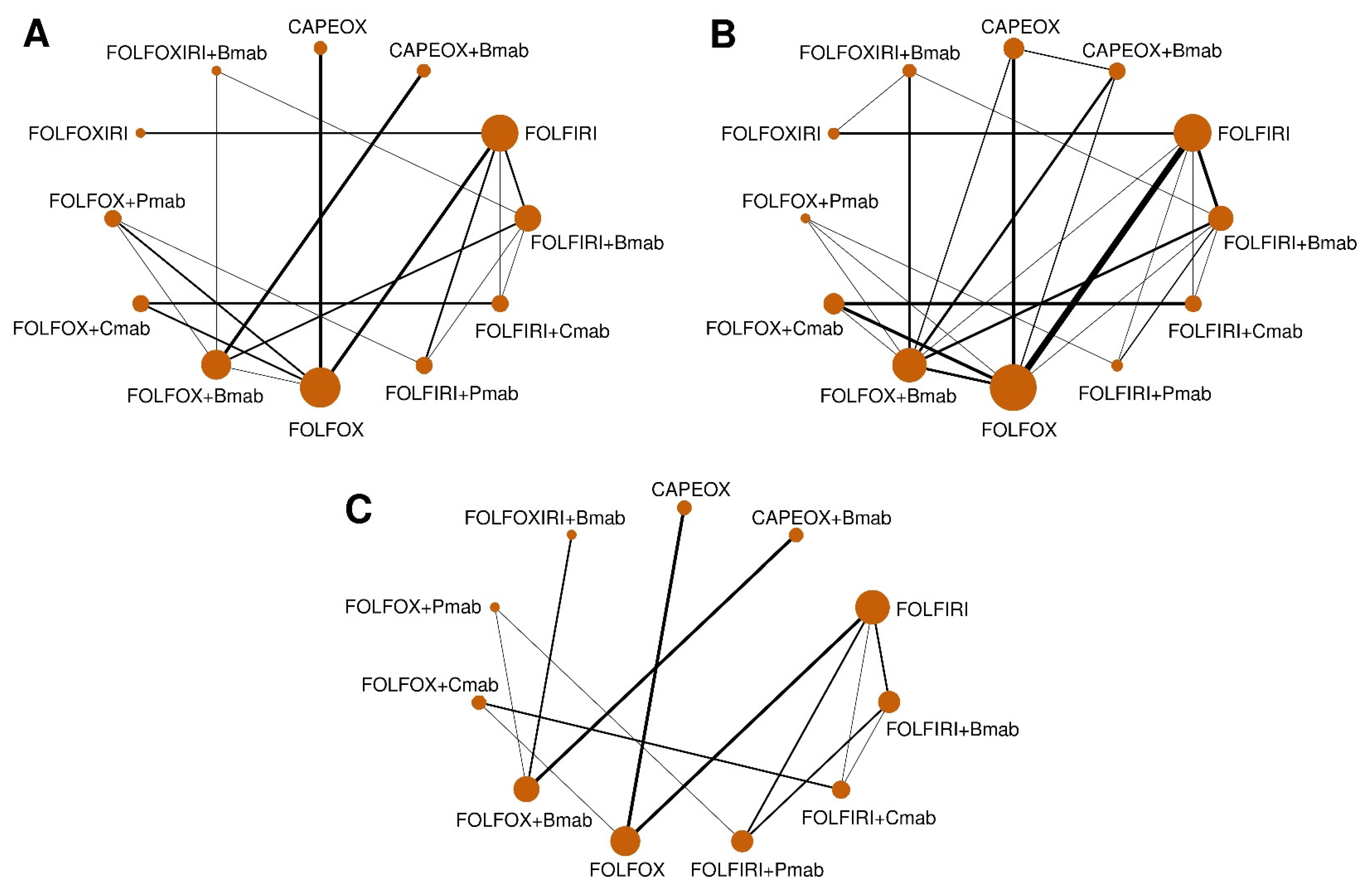
3.2. Network Geometry for the Efficacy and Safety of CRC Treatments
3.3. Pairwise Treatment Effect of Included Regimens
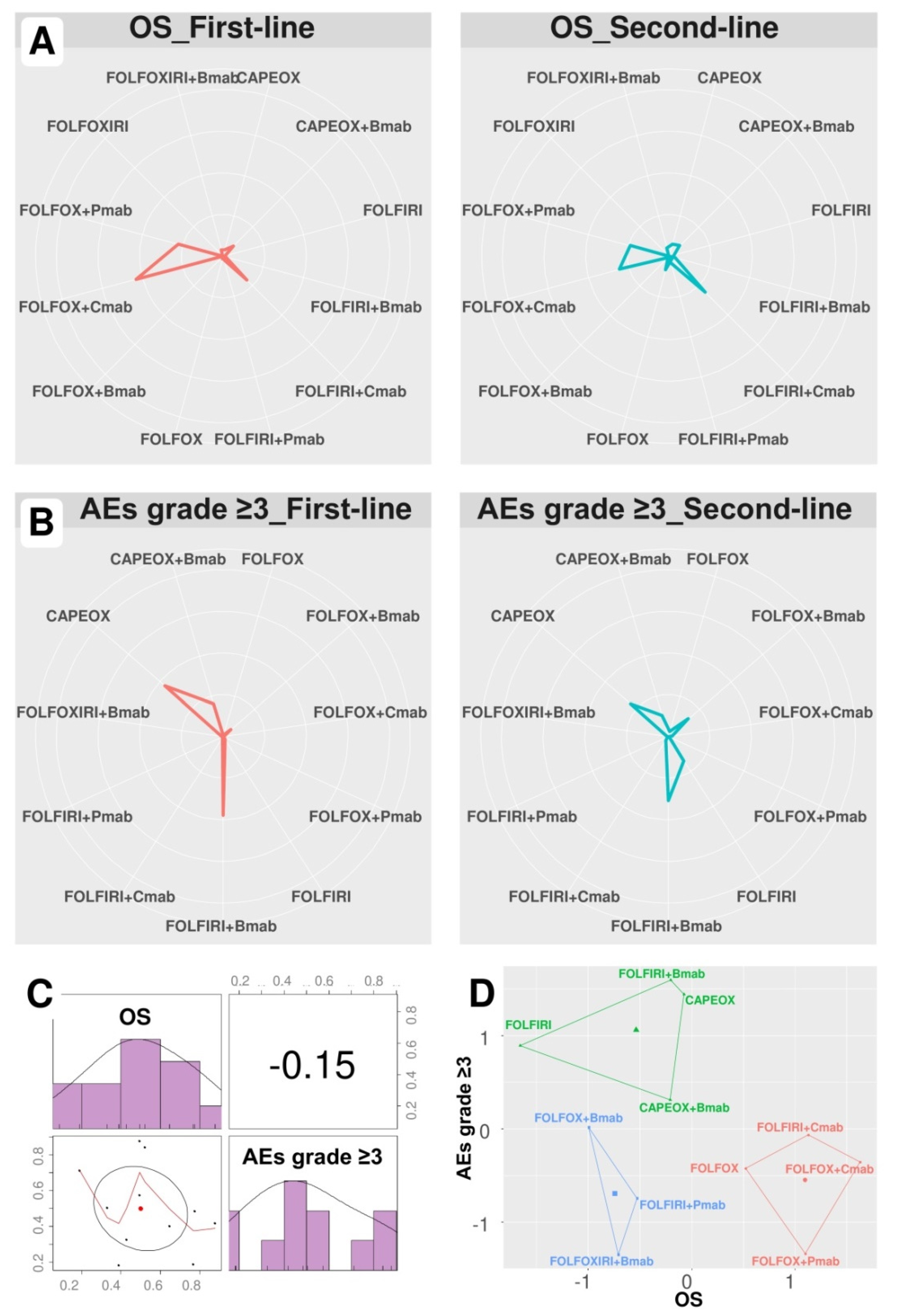
3.4. Investigation of Treatment Ranking
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D.; Group, E.G.W. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25 (Suppl. 3), iii1–iii9. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network (NCCN) Guidelines for Patients. Colon Cancer. Available online: https://www.nccn.org/patients/guidelines/colon/files/assets/common/downloads/files/colon.pdf (accessed on 4 July 2019).
- National Comprehensive Cancer Network (NCCN) Guidelines for Patients. Rectal Cancer. Available online: https://www.nccn.org/patients/guidelines/rectal/files/assets/common/downloads/files/rectal.pdf (accessed on 4 July 2019).
- Kim, L.A.; D’Amore, P.A. A brief history of anti-VEGF for the treatment of ocular angiogenesis. Am. J. Pathol. 2012, 181, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Downward, J. Targeting RAS signalling pathways in cancer therapy. Nat. Rev. Cancer 2003, 3, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Goodsell, D.S. The molecular perspective: The ras oncogene. Oncologist 1999, 4, 263–264. [Google Scholar] [CrossRef]
- Hoang, T.; Son, D.K.; Kim, B.C.; Cha, Y.; Kim, J. Efficacy and safety of systemic treatments among colorectal cancer patients: A network meta-analysis of randomized controlled trials. Crit. Rev. Oncol. Hematol. 2020. under review. [Google Scholar]
- Driscoll, J.J.; Rixe, O. Overall survival: Still the gold standard: Why overall survival remains the definitive end point in cancer clinical trials. Cancer J. 2009, 15, 401–405. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- World Health Organization. WHO Handbook for Reporting Results of Cancer Treatment. Available online: https://apps.who.int/iris/handle/10665/37200 (accessed on 12 December 2019).
- U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER) Center for Biologics Evaluation and Research (CBER). Guidance for Industry: Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics. Available online: https://www.fda.gov/downloads/drugsGuidanceComplianceRegulatoyInformation/Guidance/UCM071590.pdf (accessed on 12 December 2019).
- Uetake, H.; Emi, Y.; Yamanaka, T.; Muro, K.; Oki, E.; Takahashi, T.; Nagasaka, T.; Hatano, E.; Ojima, H.; Manaka, D.; et al. A randomized phase II study of mFOLFOX6 plus bevacizumab versus mFOLFOX6 plus cetuximab for previously untreated, liverlimited metastatic colorectal cancer that is unsuitable for resection (ATOM trial). J. Clin. Oncol. 2018, 36. [Google Scholar] [CrossRef]
- Qin, S.; Guo, W.; Xu, J.M.; Li, Q.; Cheng, Y.; Liu, T.S.; Chen, J.; Chen, W.F.; Li, J. Final overall survival (OS) analysis of first-line (1L) FOLFOX-4 ± cetuximab (cet) in patients (pts) with RAS wild-type (wt) metastatic colorectal cancer (mCRC) in the phase 3 TAILOR trial. J. Clin. Oncol. 2018, 36. [Google Scholar] [CrossRef]
- Maiello, E.; Di Maggio, G.; Cordio, S.S.; Cinieri, S.; Giuliani, F.; Pisconti, S.; Rinaldi, A.; Febbraro, A.; Pia Latiano, T.; Aieta, M.; et al. Bevacizumab (B) + bi-weekly capecitabine (C) and oxaliplatin (O) (XELOX2) or FOLFOX4 in first-line treatment of metastatic colorectal cancer (mCRC): Final results of a multicenter randomized phase II trial of the Gruppo Oncologico dell’Italia Meridionale (GOIM protocol 2802). J. Clin. Oncol. 2018, 36. [Google Scholar] [CrossRef]
- Hurwitz, H.I.; Tan, B.R.; Reeves, J.A.; Xiong, H.; Somer, B.; Lenz, H.J.; Hochster, H.S.; Scappaticci, F.; Palma, J.F.; Price, R.; et al. Phase II randomized trial of sequential or concurrent FOLFOXIRI-bevacizumab versus FOLFOX-bevacizumab for metastatic colorectal cancer (STEAM). Oncologist 2019, 24, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Hou, G.; Song, R.; Yang, J.; Zhang, Y.; Xiao, C.; Wang, C.; Yuan, J.; Chai, T.; Liu, Z. Treatment effect of conversion therapy and its correlation with VEGF expression in unresectable rectal cancer with liver metastasis. Oncol. Lett. 2018, 16, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Gomez, A.; Vieitez, J.M.; Gil, S.; Salvia, A.S.; Suárez, B.G.; Alfonso, P.G.; De Castro, E.M.; Quintero Aldana, G.A.; Reina, J.J.; Flores, E.G.; et al. Safety analysis of a phase III randomized trial comparing FOLFOX + Bevacizumab vs FOLFOXIRI + Bevacizumab as 1st line treatment in patients with metastatic colorectal cancer (mCRC) with ≥3 circulating tumor cells (CTCs) (VISNU-1 TTD TRIAL). J. Clin. Oncol. 2018, 36. [Google Scholar] [CrossRef]
- Schmoll, H.J.; Meinert, F.M.; Cygon, F.; Garlipp, B.; Junghanss, C.; Leithäuser, M.; Vogel, A.; Schaefers, M.; Kaiser, U.; Hoeffkes, H.G.; et al. “CHARTA”: FOLFOX/bevacizumab vs. FOLFOXIRI/bevacizumab in advanced colorectal cancer-Final results, prognostic, and potentially predictive factors from the randomized phase II trial of the AIO. J. Clin. Oncol. 2017, 35, 3533. [Google Scholar] [CrossRef]
- Carrato, A.; Abad, A.; Massuti, B.; Gravalos, C.; Escudero, P.; Longo-Munoz, F.; Manzano, J.L.; Gomez, A.; Safont, M.J.; Gallego, J.; et al. First-line panitumumab plus FOLFOX4 or FOLFIRI in colorectal cancer with multiple or unresectable liver metastases: A randomised, phase II trial (PLANET-TTD). Eur. J. Cancer 2017, 81, 191–202. [Google Scholar] [CrossRef]
- Yamazaki, K.; Nagase, M.; Tamagawa, H.; Ueda, S.; Tamura, T.; Murata, K.; Eguchi Nakajima, T.; Baba, E.; Tsuda, M.; Moriwaki, T.; et al. Randomized phase III study of bevacizumab plus FOLFIRI and bevacizumab plus mFOLFOX6 as first-line treatment for patients with metastatic colorectal cancer (WJOG4407G). Ann. Oncol. 2016, 27, 1539–1546. [Google Scholar] [CrossRef]
- Shitara, K.; Yonesaka, K.; Denda, T.; Yamazaki, K.; Moriwaki, T.; Tsuda, M.; Takano, T.; Okuda, H.; Nishina, T.; Sakai, K.; et al. Randomized study of FOLFIRI plus either panitumumab or bevacizumab for wild-type KRAS colorectal cancer-WJOG 6210G. Cancer Sci. 2016, 107, 1843–1850. [Google Scholar] [CrossRef]
- Ciardiello, F.; Normanno, N.; Martinelli, E.; Troiani, T.; Pisconti, S.; Cardone, C.; Nappi, A.; Bordonaro, A.R.; Rachiglio, M.; Lambiase, M.; et al. Cetuximab continuation after first progression in metastatic colorectal cancer (CAPRI-GOIM): A randomized phase II trial of FOLFOX plus cetuximab versus FOLFOX. Ann. Oncol. 2016, 27, 1055–1061. [Google Scholar] [CrossRef]
- Tournigand, C.; Chibaudel, B.; Samson, B.; Scheithauer, W.; Lledo, G.; Artru, P.; Viret, F.; Ramee, J.F.; Tubiana-Mathieu, N.; Dauba, J.; et al. Improving safety in first-line metastatic colorectal cancer (MCRC) therapy with bevacizumab: Modified FOLFOX7 versus XELOX2-Results of the induction phase of the GERCOR DREAM randomized phase III study. J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Passardi, A.; Nanni, O.; Tassinari, D.; Turci, D.; Cavanna, L.; Fontana, A.; Ruscelli, S.; Mucciarini, C.; Lorusso, V.; Ragazzini, A.; et al. Effectiveness of bevacizumab added to standard chemotherapy in metastatic colorectal cancer: Final results for first-line treatment from the ITACa randomized clinical trial. Ann. Oncol. 2015, 26, 1201–1207. [Google Scholar] [CrossRef]
- Hecht, J.R.; Cohn, A.; Dakhil, S.; Saleh, M.; Piperdi, B.; Cline-Burkhardt, M.; Tian, Y.; Go, W.Y. SPIRITT: A randomized, multicenter, phase II study of panitumumab with FOLFIRI and bevacizumab with FOLFIRI as second-line treatment in patients with unresectable wild type KRAS metastatic colorectal cancer. Clin. Colorectal Cancer 2015, 14, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Gruenberger, T.; Bridgewater, J.; Chau, I.; Garcia Alfonso, P.; Rivoire, M.; Mudan, S.; Lasserre, S.; Hermann, F.; Waterkamp, D.; Adam, R. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: The OLIVIA multinational randomised phase II trial. Ann. Oncol. 2015, 26, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Schwartzberg, L.S.; Rivera, F.; Karthaus, M.; Fasola, G.; Canon, J.L.; Hecht, J.R.; Yu, H.; Oliner, K.S.; Go, W.Y. PEAK: A randomized, multicenter phase II study of panitumumab plus modified fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) or bevacizumab plus mFOLFOX6 in patients with previously untreated, unresectable, wild-type KRAS exon 2 metastatic colorectal cancer. J. Clin. Oncol. 2014, 32, 2240–2247. [Google Scholar] [CrossRef]
- Peeters, M.; Price, T.J.; Cervantes, A.; Sobrero, A.F.; Ducreux, M.; Hotko, Y.; André, T.; Chan, E.; Lordick, F.; Punt, C.J.A.; et al. Final results from a randomized phase 3 study of FOLFIRI ± panitumumab for second-line treatment of metastatic colorectal cancer. Ann. Oncol. 2014, 25, 107–116. [Google Scholar] [CrossRef]
- Heinemann, V.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.E.; Heintges, T.; Lerchenmuller, C.; Kahl, C.; Seipelt, G.; et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): A randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1065–1075. [Google Scholar] [CrossRef]
- Folprecht, G.; Gruenberger, T.; Bechstein, W.; Raab, H.R.; Weitz, J.; Lordick, F.; Hartmann, J.T.; Stoehlmacher-Williams, J.; Lang, H.; Trarbach, T.; et al. Survival of patients with initially unresectable colorectal liver metastases treated with FOLFOX/cetuximab or FOLFIRI/cetuximab in a multidisciplinary concept (CELIM study). Ann. Oncol. 2014, 25, 1018–1025. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Siena, S.; Cassidy, J.; Tabernero, J.; Burkes, R.; Barugel, M.; Humblet, Y.; Bodoky, G.; Cunningham, D.; Jassem, J.; et al. Final results from PRIME: Randomized phase III study of panitumumab with FOLFOX4 for first-line treatment of metastatic colorectal cancer. Ann. Oncol. 2014, 25, 1346–1355. [Google Scholar] [CrossRef]
- Cao, R.; Zhang, S.; Ma, D.; Hu, L. A multi-center randomized phase II clinical study of bevacizumab plus irinotecan, 5-fluorouracil, and leucovorin (FOLFIRI) compared with FOLFIRI alone as second-line treatment for Chinese patients with metastatic colorectal cancer. Med. Oncol. 2014, 32, 1–5. [Google Scholar] [CrossRef]
- Personeni, N.; Rimassa, L.; Verusio, C.; Barni, S.; Destro, A.; Raschioni, C.; Armenia, S.; Floriani, I.; Gerardi, C.; Monteforte, M.; et al. Prognostic factors in KRAS wild-type (wt) metastatic colorectal cancer (mCRC) patients (pts) treated with biweekly cetuximab (C) plus irinotecan, fluorouracil, and leucovorin (FOLFIRI): A phase II study. J. Clin. Oncol. 2013, 31, e14611. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Kohne, C.H.; Lang, I.; Folprecht, G.; Nowacki, M.P.; Cascinu, S.; Shchepotin, I.; Maurel, J.; Cunningham, D.; Tejpar, S.; et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: Updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J. Clin. Oncol. 2011, 29, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- Masi, G.; Vasile, E.; Loupakis, F.; Cupini, S.; Fornaro, L.; Baldi, G.; Salvatore, L.; Cremolini, C.; Stasi, I.; Brunetti, I.; et al. Randomized trial of two induction chemotherapy regimens in metastatic colorectal cancer: An updated analysis. J. Natl. Cancer Inst. 2011, 103, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Guan, Z.Z.; Xu, J.M.; Luo, R.C.; Feng, F.Y.; Wang, L.W.; Shen, L.; Yu, S.Y.; Ba, Y.; Liang, J.; Wang, D.; et al. Efficacy and safety of bevacizumab plus chemotherapy in Chinese patients with metastatic colorectal cancer: A randomized phase III ARTIST trial. Chin. J. Cancer 2011, 30, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Bennouna, J.; Hebbar, M.; Ychou, M.; Lledo, G.; Conroy, T.; Adenis, A.; Faroux, R.; Rebischung, C.; Bergougnoux, L.; et al. Capecitabine plus oxaliplatin (XELOX) versus 5-fluorouracil/leucovorin plus oxaliplatin (FOLFOX-6) as first-line treatment for metastatic colorectal cancer. Int. J. Cancer 2011, 128, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.; Clarke, S.; Diaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Rittweger, K.; Gilberg, F.; Saltz, L. XELOX vs FOLFOX-4 as first-line therapy for metastatic colorectal cancer: NO16966 updated results. Br. J. Cancer 2011, 105, 58–64. [Google Scholar] [CrossRef]
- Vamvakas, L.; Athanasiadis, A.; Karampeazis, A.; Kakolyris, S.; Polyzos, A.; Kouroussis, C.; Ziras, N.; Kalbakis, K.; Georgoulias, V.; Souglakos, J. Clinical outcome of elderly patients with metastatic colorectal cancer treated with FOLFOXIRI versus FOLFIRI: Subgroup analysis of a randomized phase III trial from the Hellenic Oncology Research Group (HORG). Crit. Rev. Oncol. Hematol. 2010, 76, 61–70. [Google Scholar] [CrossRef]
- Peeters, M.; Price, T.J.; Cervantes, A.; Sobrero, A.F.; Ducreux, M.; Hotko, Y.; Andre, T.; Chan, E.; Lordick, F.; Punt, C.J.; et al. Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J. Clin. Oncol. 2010, 28, 4706–4713. [Google Scholar] [CrossRef]
- Ocvirk, J.; Brodowicz, T.; Wrba, F.; Ciuleanu, T.E.; Kurteva, G.; Beslija, S.; Koza, I.; Papai, Z.; Messinger, D.; Yilmaz, U.; et al. Cetuximab plus FOLFOX6 or FOLFIRI in metastatic colorectal cancer: CECOG trial. World J. Gastroenterol. 2010, 16, 3133–3143. [Google Scholar] [CrossRef]
- Folprecht, G.; Gruenberger, T.; Bechstein, W.O.; Raab, H.R.; Lordick, F.; Hartmann, J.T.; Lang, H.; Frilling, A.; Stoehlmacher, J.; Weitz, J.; et al. Tumour response and secondary resectability of colorectal liver metastases following neoadjuvant chemotherapy with cetuximab: The CELIM randomised phase 2 trial. Lancet Oncol. 2010, 11, 38–47. [Google Scholar] [CrossRef]
- Bokemeyer, C.; Bondarenko, I.; Makhson, A.; Hartmann, J.T.; Aparicio, J.; de Braud, F.; Donea, S.; Ludwig, H.; Schuch, G.; Stroh, C.; et al. Fluorouracil, leucovorin, and oxaliplatin with and without cetuximab in the first-line treatment of metastatic colorectal cancer. J. Clin. Oncol. 2009, 27, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Rothenberg, M.L.; Cox, J.V.; Butts, C.; Navarro, M.; Bang, Y.J.; Goel, R.; Gollins, S.; Siu, L.L.; Laguerre, S.; Cunningham, D. Capecitabine plus oxaliplatin (XELOX) versus 5-fluorouracil/folinic acid plus oxaliplatin (FOLFOX-4) as second-line therapy in metastatic colorectal cancer: A randomized phase III noninferiority study. Ann. Oncol. 2008, 19, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Hochster, H.S.; Hart, L.L.; Ramanathan, R.K.; Childs, B.H.; Hainsworth, J.D.; Cohn, A.L.; Wong, L.; Fehrenbacher, L.; Abubakr, Y.; Saif, M.W.; et al. Safety and efficacy of oxaliplatin and fluoropyrimidine regimens with or without bevacizumab as first-line treatment of metastatic colorectal cancer: Results of the TREE Study. J. Clin. Oncol. 2008, 26, 3523–3529. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.; Clarke, S.; Diaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.S.; Rivera, F.; et al. Randomized phase III study of capecitabine plus oxaliplatin compared with fluorouracil/folinic acid plus oxaliplatin as first-line therapy for metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 2006–2012. [Google Scholar] [CrossRef] [PubMed]
- Porschen, R.; Arkenau, H.T.; Kubicka, S.; Greil, R.; Seufferlein, T.; Freier, W.; Kretzschmar, A.; Graeven, U.; Grothey, A.; Hinke, A.; et al. Phase III study of capecitabine plus oxaliplatin compared with fluorouracil and leucovorin plus oxaliplatin in metastatic colorectal cancer: A final report of the AIO Colorectal Study Group. J. Clin. Oncol. 2007, 25, 4217–4223. [Google Scholar] [CrossRef]
- Falcone, A.; Ricci, S.; Brunetti, I.; Pfanner, E.; Allegrini, G.; Barbara, C.; Crino, L.; Benedetti, G.; Evangelista, W.; Fanchini, L.; et al. Phase III trial of infusional fluorouracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment for metastatic colorectal cancer: The Gruppo Oncologico Nord Ovest. J. Clin. Oncol. 2007, 25, 1670–1676. [Google Scholar] [CrossRef]
- Goldberg, R.M.; Sargent, D.J.; Morton, R.F.; Fuchs, C.S.; Ramanathan, R.K.; Williamson, S.K.; Findlay, B.P.; Pitot, H.C.; Alberts, S. Randomized controlled trial of reduced-dose bolus fluorouracil plus leucovorin and irinotecan or infused fluorouracil plus leucovorin and oxaliplatin in patients with previously untreated metastatic colorectal cancer: A North American Intergroup Trial. J. Clin. Oncol. 2006, 24, 3347–3353. [Google Scholar] [CrossRef]
- Polikoff, J.; Mitchell, E.P.; Badarinath, S.; Graham, C.D.; Jennis, A.; Chen, T.T.; Gustafson, T.N.; Langer, C. Erbitux (cetuximab) plus FOLFOX for colorectal cancer (EXPLORE): Preliminary efficacy analysis of a randomized phase III trial. Annu. Meet. ASCO 2005, 23, 264. [Google Scholar]
- Kalofonos, H.P.; Aravantinos, G.; Kosmidis, P.; Papakostas, P.; Economopoulos, T.; Dimopoulos, M.; Skarlos, D.; Bamias, A.; Pectasides, D.; Chalkidou, S.; et al. Irinotecan or oxaliplatin combined with leucovorin and 5-fluorouracil as first-line treatment in advanced colorectal cancer: A multicenter, randomized, phase II study. Ann. Oncol. 2005, 16, 869–877. [Google Scholar] [CrossRef]
- Comella, P.; Massidda, B.; Filippelli, G.; Palmeri, S.; Natale, D.; Farris, A.; De Vita, F.; Buzzi, F.; Tafuto, S.; Maiorino, L.; et al. Oxaliplatin plus high-dose folinic acid and 5-fluorouracil i.v. bolus (OXAFAFU) versus irinotecan plus high-dose folinic acid and 5-fluorouracil i.v. bolus (IRIFAFU) in patients with metastatic colorectal carcinoma: A Southern Italy Cooperative Oncology Group phase III trial. Ann. Oncol. 2005, 16, 878–886. [Google Scholar] [CrossRef]
- Colucci, G.; Gebbia, V.; Paoletti, G.; Giuliani, F.; Caruso, M.; Gebbia, N.; Carteni, G.; Agostara, B.; Pezzella, G.; Manzione, L.; et al. Phase III randomized trial of FOLFIRI versus FOLFOX4 in the treatment of advanced colorectal cancer: A multicenter study of the Gruppo Oncologico Dell’Italia Meridionale. J. Clin. Oncol. 2005, 23, 4866–4875. [Google Scholar] [CrossRef] [PubMed]
- Tournigand, C.; Andre, T.; Achille, E.; Lledo, G.; Flesh, M.; Mery-Mignard, D.; Quinaux, E.; Couteau, C.; Buyse, M.; Ganem, G.; et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: A randomized GERCOR study. J. Clin. Oncol. 2004, 22, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef]
- Goldberg, R.M.; Sargent, D.J.; Morton, R.F.; Fuchs, C.S.; Ramanathan, R.K.; Williamson, S.K.; Findlay, B.P.; Pitot, H.C.; Alberts, S.R. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J. Clin. Oncol. 2004, 22, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Rougier, P.; Lepille, D.; Bennouna, J.; Marre, A.; Ducreux, M.; Mignot, L.; Hua, A.; Méry-Mignard, D. Antitumor activity of three second-line treatment combinations in patients with metastatic colorectal cancer after optimal 5-FU regimen failure: A randomised, multicentre phase II study. Ann. Oncol. 2002, 13, 1558–1567. [Google Scholar] [CrossRef]
- Nct. Study of Bevacizumab + mFOLFOX6 Versus Bevacizumab + FOLFIRI with Biomarker Stratification in Participants with Previously Untreated Metastatic Colorectal Cancer (mCRC). Available online: https://clinicaltrials.gov/show/nct01374425 (accessed on 22 December 2019).
- Nct. Study Evaluating the Safety and Efficacy of FOLFIRI Plus Cetuximab or FOLFOX Plus Cetuximab as First-Line Therapy in Subjects with KRAS Wild-Type Metastatic Colorectal Cancer (APEC-Study) (APEC). Available online: https://clinicaltrials.gov/show/nct00778830 (accessed on 22 December 2019).
- Bujkiewicz, S.; Thompson, J.R.; Sutton, A.J.; Cooper, N.J.; Harrison, M.J.; Symmons, D.P.; Abrams, K.R. Multivariate meta-analysis of mixed outcomes: A Bayesian approach. Stat. Med. 2013, 32, 3926–3943. [Google Scholar] [CrossRef]
- Elia, E.G.; Stadler, N.; Ciani, O.; Taylor, R.S.; Bujkiewicz, S. Combining tumour response and progression free survival as surrogate endpoints for overall survival in advanced colorectal cancer. arXiv 2018, arXiv:1809.02935. [Google Scholar] [CrossRef]
- Dias, S.; Sutton, A.J.; Ades, A.E.; Welton, N.J. Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Mak. 2013, 33, 607–617. [Google Scholar] [CrossRef]
- Dias, S.; Sutton, A.J.; Welton, N.J.; Ades, A.E. Evidence synthesis for decision making 3: Heterogeneity—Subgroups, meta-regression, bias, and bias-adjustment. Med. Decis. Mak. 2013, 33, 618–640. [Google Scholar] [CrossRef]
- van Valkenhoef, G.; Kuiper, J. Gemtc: Network Meta-Analysis Using Bayesian Methods. Available online: https://cran.r-project.org/web/packages/gemtc/gemtc.pdf (accessed on 17 August 2019).
- Daly, C.H.; Neupane, B.; Beyene, J.; Thabane, L.; Straus, S.E.; Hamid, J.S. Empirical evaluation of SUCRA-based treatment ranks in network meta-analysis: Quantifying robustness using Cohen’s kappa. BMJ Open 2019, 9, e024625. [Google Scholar] [CrossRef]
- Kassambara, A.; Fabian, M. Factoextra: Extract and Visualize the Results of Multivariate Data Analyses. Available online: http://www.sthda.com/english/rpkgs/factoextra (accessed on 22 December 2019).
- van de Schoot, R.; Kaplan, D.; Denissen, J.; Asendorpf, J.B.; Neyer, F.J.; van Aken, M.A.G. A gentle introduction to bayesian analysis: Applications to developmental research. Child. Dev. 2014, 85, 842–860. [Google Scholar] [CrossRef] [PubMed]
- Haslam, A.; Hey, S.P.; Gill, J.; Prasad, V. A systematic review of trial-level meta-analyses measuring the strength of association between surrogate end-points and overall survival in oncology. Eur. J. Cancer 2019, 106, 196–211. [Google Scholar] [CrossRef] [PubMed]
- Kemp, R.; Prasad, V. Surrogate endpoints in oncology: When are they acceptable for regulatory and clinical decisions, and are they currently overused? BMC Med. 2017, 15, 134. [Google Scholar] [CrossRef]
- Cicero, G.; De Luca, R.; Dieli, F. Progression-free survival as a surrogate endpoint of overall survival in patients with metastatic colorectal cancer. Onco. Targets Ther. 2018, 11, 3059–3063. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Antoniotti, C.; Pietrantonio, F.; Berenato, R.; Tampellini, M.; Baratelli, C.; Salvatore, L.; Marmorino, F.; Borelli, B.; Nichetti, F.; et al. Surrogate Endpoints in Second-Line Trials of Targeted Agents in Metastatic Colorectal Cancer: A Literature-Based Systematic Review and Meta-Analysis. Cancer Res. Treat. 2017, 49, 834–845. [Google Scholar] [CrossRef]
- Montagnani, F.; Di Leonardo, G.; Pino, M.S.; Martella, F.; Perboni, S.; Ribecco, A.; Fioretto, L. Progression-free Survival as a Surrogate End-point in Advanced Colorectal Cancer Treated with Antiangiogenic Therapies. Anticancer Res. 2016, 36, 4259–4265. [Google Scholar]
- Sidhu, R.; Rong, A.; Dahlberg, S. Evaluation of progression-free survival as a surrogate endpoint for survival in chemotherapy and targeted agent metastatic colorectal cancer trials. Clin. Cancer Res. 2013, 19, 969–976. [Google Scholar] [CrossRef]
- Tang, P.A.; Bentzen, S.M.; Chen, E.X.; Siu, L.L. Surrogate end points for median overall survival in metastatic colorectal cancer: Literature-based analysis from 39 randomized controlled trials of first-line chemotherapy. J. Clin. Oncol. 2007, 25, 4562–4568. [Google Scholar] [CrossRef]
- Petrelli, F.; Ghidini, M.; Costanzo, A.; Rampulla, V.; Varricchio, A.; Tomasello, G. Surrogate endpoints in immunotherapy trials for solid tumors. Ann. Transl. Med. 2019, 7, 154. [Google Scholar] [CrossRef]
- Schuster Bruce, C.; Brhlikova, P.; Heath, J.; McGettigan, P. The use of validated and nonvalidated surrogate endpoints in two European Medicines Agency expedited approval pathways: A cross-sectional study of products authorised 2011–2018. PLoS Med. 2019, 16, e1002873. [Google Scholar] [CrossRef]
- Giessen, C.; Laubender, R.P.; Ankerst, D.P.; Stintzing, S.; Modest, D.P.; Mansmann, U.; Heinemann, V. Progression-free survival as a surrogate endpoint for median overall survival in metastatic colorectal cancer: Literature-based analysis from 50 randomized first-line trials. Clin. Cancer Res. 2013, 19, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.; de Gramont, A.; Grothey, A.; Zalcberg, J.; Chibaudel, B.; Schmoll, H.J.; Seymour, M.T.; Adams, R.; Saltz, L.; Goldberg, R.M.; et al. Individual patient data analysis of progression-free survival versus overall survival as a first-line end point for metastatic colorectal cancer in modern randomized trials: Findings from the analysis and research in cancers of the digestive system database. J. Clin. Oncol. 2015, 33, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Mohelnikova-Duchonova, B.; Melichar, B.; Soucek, P. FOLFOX/FOLFIRI pharmacogenetics: The call for a personalized approach in colorectal cancer therapy. World J. Gastroenterol. 2014, 20, 10316–10330. [Google Scholar] [CrossRef] [PubMed]
- Neugut, A.I.; Lin, A.; Raab, G.T.; Hillyer, G.C.; Keller, D.; O’Neil, D.S.; Accordino, M.K.; Kiran, R.P.; Wright, J.; Hershman, D.L. FOLFOX and FOLFIRI Use in Stage IV Colon Cancer: Analysis of SEER-Medicare Data. Clin. Colorectal Cancer 2019, 18, 133–140. [Google Scholar] [CrossRef]
- Zhao, Z.; Pelletier, E.; Barber, B.; Bhosle, M.; Wang, S.; Gao, S.; Klingman, D. Patterns of treatment with chemotherapy and monoclonal antibodies for metastatic colorectal cancer in Western Europe. Curr. Med. Res. Opin. 2012, 28, 221–229. [Google Scholar] [CrossRef]
- Wu, C.C.; Wang, J.H.; Lin, P.C.; Liang, C.A.; Huang, C.Y.; Lien, H.C.; Chen, C.Y.; Chou, K.J.; Su, Y.C. Tumor sidedness and efficacy of first-line therapy in patients with RAS/BRAF wild-type metastatic colorectal cancer: A network meta-analysis. Crit. Rev. Oncol. Hematol. 2019, 145, 102823. [Google Scholar] [CrossRef]
- Bupathi, M.; Ahn, D.H.; Bekaii-Saab, T. Spotlight on bevacizumab in metastatic colorectal cancer: Patient selection and perspectives. Gastrointest Cancer 2016, 6, 21–30. [Google Scholar] [CrossRef]
- Munker, S.; Gerken, M.; Fest, P.; Ott, C.; Schnoy, E.; Fichtner-Feigl, S.; Wiggermann, P.; Vogelhuber, M.; Herr, W.; Stroszczynski, C.; et al. Chemotherapy for metastatic colon cancer: No effect on survival when the dose is reduced due to side effects. BMC Cancer 2018, 18, 455. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Treatment Line | Treatment Arms | OR (95% CI) for Overall Response Rate | HR (95% CI) for Progression-Free Survival | Observed HR (95% CI) for Overall Survival | Predicted HR (95% CrI) for Overall Survival | OR (95% CI) for Adverse Events Grade ≥3 | |
|---|---|---|---|---|---|---|---|---|
| Intervention Arm | Comparison Arm | |||||||
| Uetake 2018 et al. [13] | 1-line | FOLFOX+Cmab | FOLFOX+Bmab | 2.94 (1.16–7.47) | 0.80 (0.51–1.26) | 0.81 (0.54–1.21) | ||
| Qin 2018 et al. [14] | 1-line | FOLFOX+Cmab | FOLFOX | 2.89 (1.92–4.36) | 0.63 (0.50–0.79) | 0.76 (0.61–0.95) | ||
| Maiello 2018 et al. [15] | 1-line | FOLFOX+Bmab | CAPEOX+Bmab | 1.34 (0.65–2.76) | 0.96 (0.65–1.41) | 1.21 (0.77–1.92) | ||
| Hurwitz 2018 et al. [16] | 1-line | FOLFOXIRI+Bmab | FOLFOX+Bmab | 1.60 (0.95–2.71) | 0.68 (0.50–0.92) | 0.72 (0.48–1.07) | ||
| Hou 2018 et al. [17] | 1-line | FOLFOXIRI+Bmab | FOLFOXIRI | 2.41 (1.12–5.18) | 0.82 (0.47–1.42) | |||
| Gomez 2018 et al. [18] | 1-line | FOLFOX+Bmab | FOLFOXIRI+Bmab | 0.51 (0.32–0.81) | ||||
| Schmoll 2017 et al. [19] | 1-line | FOLFOX+Bmab | FOLFOXIRI+Bmab | 0.64 (0.37–1.08) | 0.80 (0.61–1.04) | 0.81 (0.54–1.21) | ||
| Carrato 2017 et al. [20] | 1-line | FOLFOX+Pmab | FOLFIRI+Pmab | 1.40 (0.52–3.74) | 0.90 (0.60–1.50) | 1.00 (0.60–1.80) | 1.60 (0.51–5.04) | |
| Yamazaki 2016 et al. [21] | 1-line | FOLFIRI+Bmab | FOLFOX+Bmab | 1.07 (0.70–1.64) | 0.91 (0.72–1.13) | 0.99 (0.79–1.25) | ||
| Shitara 2016 et al. [22] | 2-line | FOLFIRI+Pmab | FOLFIRI+Bmab | 14.3 (3.95–51.7) | ||||
| Ciardiello 2016 et al. [23] | 2-line | FOLFOX+Cmab | FOLFOX | 1.90 (0.80–4.52) | 0.81 (0.58–1.12) | 0.57 (0.32–1.02) | ||
| Tournigand 2015 et al. [24] | 1-line | FOLFOX+Bmab | CAPEOX+Bmab | 0.98 (0.74–1.31) | 1.24 (0.98–1.59) | 0.63 (0.39–1.02) | ||
| Passardi 2015 et al. [25] | 1-line | FOLFOX+Bmab | FOLFOX | 1.29 (0.76–2.19) | 0.85 (0.49–1.47) | |||
| FOLFIRI+Bmab | FOLFIRI | 0.74 (0.39–1.41) | 0.96 (0.55–1.68) | |||||
| Hecht 2015 et al. [26] | 2-line | FOLFIRI+Pmab | FOLFIRI+Bmab | 1.99 (0.98–4.03) | 1.01 (0.68–1.50) | 1.06 (0.75–1.49) | 2.20 (1.06–4.56) | |
| Gruenberger 2015 et al. [27] | 1-line | FOLFOXIRI+Bmab | FOLFOX+Bmab | 2.58 (0.94–7.05) | 0.43 (0.26–0.72) | 0.35 (0.15–0.80) | 3.68 (0.69–19.5) | |
| Cremolini 2015 et al. [28] | 1-line | FOLFIRI+Bmab | FOLFOXIRI+Bmab | 0.63 (0.44–0.90) | 0.77 (0.65–0.93) | 0.80 (0.65–0.98) | ||
| Schwartzberg 2014 et al. [29] | 1-line | FOLFOX+Pmab | FOLFOX+Bmab | 1.20 (0.75–1.92) | 0.87 (0.65–1.17) | 0.62 (0.44–0.89) | 2.02 (0.98–4.16) | |
| Peeters 2014 et al. [30] | 2-line | FOLFIRI+Pmab | FOLFIRI | 5.19 (3.29–8.19) | 0.82 (0.69–0.97) | 0.92 (0.78–1.10) | ||
| 0.89 (0.53–1.50) | 0.94 (0.78–1.14) | 0.93 (0.77–1.13) | ||||||
| Peeters 2010 et al. [42] | FOLFIRI+Pmab | FOLFIRI | 2.46 (1.75–3.47) | |||||
| 1.76 (1.22–2.53) | ||||||||
| Heinemann 2014 et al. [31] | 1-line | FOLFIRI+Cmab | FOLFIRI+Bmab | 1.18 (0.85–1.64) | 1.06 (0.88–1.26) | 0.77 (0.62–0.96) | 1.40 (0.99–1.97) | |
| Folprecht 2014 et al. [32] | 1-line | FOLFOX+Cmab | FOLFIRI+Cmab | 1.03 (0.66–1.61) | 1.18 (0.79–1.74) | |||
| Folprecht 2010 et al. [44] | 1-line | 1.62 (0.74–3.59) | 0.81 (0.47–1.40) | 0.81 (0.35–1.88) | ||||
| Douillard 2014 et al. [33] | 1-line | FOLFOX+Pmab | FOLFOX | 1.47 (1.08–2.01) | 0.80 (0.67–0.95) | 0.88 (0.73–1.06) | ||
| 0.97 (0.66–1.43) | 1.27 (1.04–1.55) | 1.17 (0.95–1.45) | ||||||
| Cao 2014 et al. [34] | 2-line | FOLFIRI+Bmab | FOLFIRI | 2.28 (1.14–4.56) | 0.75 (0.43–1.31) | 0.56 (0.27–1.15) | ||
| Personeni 2013 et al. [35] | 1-line | FOLFIRI | FOLFIRI+Cmab | 0.98 (0.42–2.30) | 0.90 (0.52–1.56) | |||
| Van 2011 et al. [36] | 1-line | FOLFIRI+Cmab | FOLFIRI | 1.40 (1.11–1.76) | 0.85 (0.73–1.00) | 0.88 (0.77–1.00) | 2.46 (1.90–3.18) | |
| Masi 2011 et al. [37] | 1-line | FOLFIRI | FOLFOXIRI | 0.59 (0.45–0.76) | 0.74 (0.56–0.96) | |||
| Falcone 2007 et al. [50] | 1-line | FOLFIRI | FOLFOXIRI | 0.43 (0.26–0.72) | 1.08 (0.60–1.95) | |||
| Guan 2011 et al. [38] | 1-line | FOLFIRI+Bmab | FOLFIRI | 2.62 (1.26–5.48) | 0.44 (0.31–0.63) | 0.62 (0.41–0.95) | ||
| Ducreux 2011 et al. [39] | 1-line | CAPEOX | FOLFOX | 0.75 (0.46–1.24) | 1.00 (0.79–1.27) | 1.02 (0.80–1.29) | ||
| Cassidy 2011 et al. [40] | 1-line | FOLFOX | CAPEOX | 0.95 (0.84–1.07) | 1.42 (1.11–1.83) | |||
| FOLFOX+Bmab | CAPEOX+Bmab | 0.95 (0.80–1.13) | 1.78 (1.22–2.61) | |||||
| Cassidy 2008 et al. [48] | FOLFOX | CAPEOX | 0.96 (0.81–1.13) | |||||
| FOLFOX+Bmab | CAPEOX+Bmab | 1.01 (0.85–1.12) | ||||||
| Vamvakas 2010 et al. [41] | 1-line | FOLFIRI | FOLFOXIRI | 0.67 (0.41–1.08) | 1.15 (0.86–1.48) | 1.08 (0.80–1.45) | ||
| Ocvirk 2010 et al. [43] | 1-line | FOLFOX+Cmab | FOLFIRI+Cmab | 0.93 (0.49–1.77) | 1.06 (0.74–1.52) | 0.98 (0.67–1.44) | 1.66 (0.87–3.16) | |
| Bokemeyer 2009 et al. [45] | 1-line | FOLFOX | FOLFOX+Cmab | 0.66 (0.43–1.03) | 0.93 (0.71–1.23) | 0.91 (0.61–1.36) | 0.73 (0.45–1.18) | |
| Rothenberg 2008 et al. [46] | 2-line | FOLFOX | CAPEOX | 0.88 (0.59–1.31) | 0.97 (0.83–1.14) | 1.03 (0.87–1.23) | 3.25 (2.20–4.80) | |
| Hochster 2008 et al. [47] | 1-line | FOLFOX | CAPEOX | 2.69 (1.11–6.55) | 0.73 (0.41–1.27) | 1.15 (0.46–2.85) | ||
| FOLFOX+Bmab | CAPEOX+Bmab | 1.29 (0.67–2.48) | 0.85 (0.49–1.47) | 1.31 (0.67–2.58) | ||||
| Porschen 2007 et al. [49] | 1-line | CAPEOX | FOLFOX | 0.79 (0.55–1.13) | 1.17 (0.96–1.43) | 1.08 (0.72–1.63) | ||
| Goldberg 2006 et al. [51] | 1-line | FOLFOX | FOLFIRI | 1.98 (1.25–3.16) | 0.55 (0.43–0.70) | 0.76 (0.60–0.97) | ||
| Polikoff 2005 et al. [52] | 2-line | FOLFOX+Cmab | FOLFOX | 0.13 (0.05–0.34) | 1.40 (0.69–2.90) | |||
| Kalofonos 2005 et al. [53] | 1-line | FOLFIRI | FOLFOX | 1.08 (0.66–1.76) | 0.88 (0.51–1.53) | |||
| Comella 2005 et al. [54] | 1-line | FOLFIRI | FOLFOX | 0.58 (0.35–0.95) | 1.01 (0.57–1.80) | 1.46 (0.91–2.35) | ||
| Colucci 2005 et al. [55] | 1-line | FOLFIRI | FOLFOX | 0.89 (0.57–1.38) | 1.04 (0.80–1.37) | |||
| Tournigand 2004 et al. [56] | 1-line | FOLFIRI | FOLFOX | 1.12 (0.66–1.90) | 0.88 (0.51–1.52) | 0.40 (0.23–0.70) | ||
| 2-line | FOLFOX | FOLFIRI | 3.83 (1.03–14.2) | 0.67 (0.37–1.20) | 1.21 (0.63–2.30) | |||
| Hurwitz 2004 et al. [57] | 1-line | FOLFIRI+Bmab | FOLFIRI | 1.52 (1.15–2.02) | 0.82 (0.47–1.42) | 0.50 (0.35–0.72) | ||
| Goldberg 2004 et al. [58] | 1-line | FOLFOX | FOLFIRI | 1.81 (1.27–2.58) | 0.74 (0.61–0.89) | 0.66 (0.54–0.82) | ||
| Rougier 2002 et al. [59] | 2-line | FOLFIRI | FOLFOX | 0.48 (0.13–1.82) | 1.05 (0.59–1.89) | |||
| NCT01374425 [60] | 1-line | FOLFOX+Bmab | FOLFIRI+Bmab | 0.83 (0.55–1.27) | 0.79 (0.61–1.01) | 0.76 (0.56–1.04) | ||
| NCT00778830 [61] | 1-line | FOLFIRI+Cmab | FOLFOX+Cmab | 0.76 (0.47–1.24) | 0.95 (0.54–1.67) | |||
| Model parameters | Model 1 (N = 26) | Model 2 (N = 24) | Model 3 (N = 23) |
|---|---|---|---|
| Intercept | −0.11 (−0.23, 0.02) | 0.21 (−0.06, 0.47) | −0.04 (−0.14, 0.06) |
| Slope | −0.22 (−0.42, −0.04) | 0.79 (0.49–1.09) | 0.76 (0.46–1.06) |
| Variance | 0.07 (0.04–0.13) | 0.02 (0.01–0.04) | 0.04 (0.02–0.07) |
| R-squared | 0.24 (0.01–0.56) | 0.54 (0.25–0.76) | 0.53 (0.22–0.76) |
| Heading | FOLFOX | FOLFOX+Bmab | FOLFOX+Cmab | FOLFOX+Pmab | FOLFIRI | FOLFIRI+Bmab | FOLFIRI+Cmab | FOLFIRI+Pmab | FOLFOXIRI | FOLFOXIRI+Bmab | CAPEOX | CAPEOX+Bmab |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FOLFOX | 1.84 | 1.16 | 3.07 | 0.63 | 0.46 | 1.00 | 1.36 | 4.94 | 0.45 | 1.71 | ||
| (0.09–8.75) | (0.29–3.19) | (0.29–12.7) | (0.22–1.44) | (0.13–1.17) | (0.27–2.64) | (0.38–3.57) | (0.19–24.7) | (0.17–1.00) | (0.08–8.37) | |||
| FOLFOX+Bmab | 0.90 | 2.09 | 2.52 | 1.10 | 0.77 | 1.76 | 2.13 | 2.60 | 0.92 | 0.92 | ||
| (0.71–1.12) | (0.11–9.77) | (0.60–7.19) | (0.08–4.87) | (0.05–3.43) | (0.11–8.02) | (0.17–9.10) | (0.92–6.13) | (0.05–4.25) | (0.46–1.68) | |||
| FOLFOX+Cmab | 1.12 | 1.26 | 3.14 | 0.65 | 0.46 | 0.95 | 1.39 | 5.06 | 0.50 | 1.74 | ||
| (0.92–1.35) | (0.97–1.60) | (0.31–12.9) | (0.24–1.43) | (0.15–1.07) | (0.41–1.89) | (0.43–3.43) | (0.20–25.6) | (0.14–1.29) | (0.08–8.59) | |||
| FOLFOX+Pmab | 1.06 | 1.20 | 0.96 | 0.43 | 0.30 | 0.68 | 0.83 | 1.55 | 0.35 | 0.55 | ||
| (0.87–1.30) | (0.91–1.54) | (0.73–1.24) | (0.06–1.55) | (0.04–1.09) | (0.08–2.60) | (0.13–2.82) | (0.24–5.44) | (0.03–1.40) | (0.10–1.71) | |||
| FOLFIRI | 0.84 | 0.95 | 0.76 | 0.80 | 0.73 | 1.61 | 2.16 | 7.76 | 0.80 | 2.69 | ||
| (0.73–0.98) | (0.76–1.18) | (0.62–0.94) | (0.63–1.00) | (0.38–1.26) | (0.74–3.07) | (1.09–3.84) | (0.39–37.4) | (0.30–1.79) | (0.16–12.5) | |||
| FOLFIRI+Bmab | 0.95 | 1.07 | 0.85 | 0.90 | 1.13 | 2.34 | 3.14 | 11.3 | 1.21 | 3.93 | ||
| (0.77–1.18) | (0.88–1.29) | (0.67–1.09) | (0.69–1.17) | (0.93–1.35) | (1.01–4.66) | (1.51–5.89) | (0.56–55.2) | (0.37–3.03) | (0.23–18.4) | |||
| FOLFIRI+Cmab | 1.06 | 1.20 | 0.95 | 1.01 | 1.26 | 1.13 | 1.50 | 5.46 | 0.56 | 1.89 | ||
| (0.86–1.31) | (0.92–1.53) | (0.78–1.17) | (0.76–1.32) | (1.04–1.52) | (0.90–1.39) | (0.56–3.32) | (0.24–27.0) | (0.17–1.41) | (0.10–9.10) | |||
| FOLFIRI+Pmab | 0.93 | 1.04 | 0.83 | 0.88 | 1.10 | 0.98 | 0.88 | 3.56 | 0.41 | 1.24 | ||
| (0.74–1.17) | (0.79–1.36) | (0.63–1.09) | (0.66–1.15) | (0.90–1.33) | (0.77–1.23) | (0.67–1.13) | (0.21–16.7) | (0.12–1.05) | (0.09–5.57) | |||
| FOLFOXIRI | 0.77 | 0.87 | 0.69 | 0.73 | 0.91 | 0.82 | 0.73 | 0.84 | ||||
| (0.59–1.01) | (0.63–1.17) | (0.51–0.94) | (0.53–1.00) | (0.72–1.15) | (0.61–1.07) | (0.54–0.97) | (0.62–1.12) | |||||
| FOLFOXIRI+Bmab | 0.91 | 1.02 | 0.82 | 0.87 | 1.08 | 0.96 | 0.86 | 0.99 | 1.20 | 0.45 | 0.45 | |
| (0.68–1.23) | (0.80–1.31) | (0.60–1.13) | (0.62–1.20) | (0.82–1.43) | (0.76–1.23) | (0.64–1.17) | (0.72–1.36) | (0.86–1.65) | (0.02–2.17) | (0.12–1.16) | ||
| CAPEOX | 0.96 | 1.09 | 0.87 | 0.91 | 1.15 | 1.03 | 0.92 | 1.05 | 1.27 | 1.08 | 4.16 | |
| (0.81–1.12) | (0.81–1.42) | (0.67–1.10) | (0.69–1.16) | (0.91–1.40) | (0.77–1.32) | (0.69–1.17) | (0.78–1.37) | (0.91–1.71) | (0.74–1.46) | (0.19–20.5) | ||
| CAPEOX+Bmab | 0.95 | 1.06 | 0.86 | 0.90 | 1.13 | 1.01 | 0.90 | 1.04 | 1.25 | 1.05 | 1.00 | |
| (0.70–1.28) | (0.87–1.29) | (0.62–1.17) | (0.64–1.24) | (0.83–1.51) | (0.75–1.31) | (0.65–1.23) | (0.73–1.44) | (0.86–1.78) | (0.76–1.41) | (0.70–1.40) |
| Network Meta-Analysis Assumptions | Overall Survival | Adverse Events Grade ≥3 |
|---|---|---|
| Consistency Assumption | ||
| Comparison (p-Value) | ||
| FOLFIRI+Bmab vs. FOLFIRI | 0.14 | 0.11 |
| FOLFIRI+Cmab vs. FOLFIRI | 0.08 | 0.29 |
| FOLFIRI+Pmab vs. FOLFIRI | 0.87 | 0.39 |
| FOLFOX vs. FOLFIRI | 0.93 | 0.81 |
| FOLFIRI+Cmab vs. FOLFIRI+Bmab | 0.24 | 0.35 |
| FOLFOX+Bmab vs. FOLFIRI+Bmab | 0.05 | 0.39 |
| FOLFOXIRI+Bmab vs. FOLFIRI+Bmab | 0.10 | |
| FOLFOX+Cmab vs. FOLFIRI+Cmab | 0.41 | 0.81 |
| FOLFOX+Pmab vs. FOLFIRI+Pmab | 0.63 | |
| FOLFOX+Bmab vs. FOLFOX | 0.33 | |
| FOLFOX+Cmab vs. FOLFOX | 0.42 | 0.82 |
| FOLFOX+Pmab vs. FOLFOX | 0.26 | |
| FOLFOX+Cmab vs. FOLFOX+Bmab | 0.96 | |
| FOLFOX+Pmab vs. FOLFOX+Bmab | 0.08 | |
| FOLFOXIRI+Bmab vs. FOLFOX+Bmab | 0.11 | |
| FOLFOXIRI+Bmab vs. FOLFOXIRI | 0.90 | |
| Heterogeneity Assumption | ||
| Global pairwise I2 (%) | 28.94 | 71.38 |
| Global consistent I2 (%) | 36.41 | 76.41 |
| Treatment | 1st Line | 2nd Line | 3rd Line | 4th Line | 5th Line | 6th Line | 7th Line | 8th Line | 9th Line | 10th Line | 11th Line | 12th Line |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FOLFOX | 1.29 | 6.79 | 16.79 | 23.08 | 18.86 | 12.94 | 9.11 | 6.17 | 3.50 | 1.19 | 0.24 | 0.04 |
| FOLFOX+Bmab | 0.14 | 0.78 | 1.86 | 3.32 | 5.24 | 8.11 | 12.12 | 16.11 | 17.95 | 16.65 | 12.31 | 5.40 |
| FOLFOX+Cmab | 43.34 | 24.57 | 12.78 | 7.57 | 4.80 | 2.87 | 1.77 | 1.09 | 0.65 | 0.37 | 0.14 | 0.06 |
| FOLFOX+Pmab | 22.17 | 19.43 | 16.95 | 12.07 | 9.75 | 6.67 | 4.70 | 3.36 | 2.41 | 1.40 | 0.77 | 0.33 |
| FOLFIRI | 0.00 | 0.01 | 0.03 | 0.14 | 0.49 | 1.89 | 5.37 | 9.98 | 14.96 | 23.88 | 34.92 | 8.33 |
| FOLFIRI+Bmab | 1.26 | 3.13 | 6.24 | 9.00 | 11.48 | 15.96 | 17.42 | 15.02 | 11.16 | 6.17 | 2.43 | 0.74 |
| FOLFIRI+Cmab | 16.24 | 24.60 | 18.33 | 12.98 | 10.84 | 6.82 | 4.31 | 2.76 | 1.76 | 0.95 | 0.31 | 0.11 |
| FOLFIRI+Pmab | 2.07 | 3.36 | 5.08 | 6.54 | 8.59 | 12.44 | 12.46 | 11.79 | 12.24 | 13.34 | 8.12 | 3.98 |
| FOLFOXIRI | 0.13 | 0.24 | 0.41 | 0.65 | 0.95 | 1.58 | 2.29 | 3.29 | 4.83 | 7.44 | 13.91 | 64.28 |
| FOLFOXIRI+Bmab | 3.25 | 3.97 | 5.01 | 5.66 | 6.53 | 8.18 | 9.72 | 11 | 12.18 | 12.35 | 13.93 | 8.21 |
| CAPEOX | 3.14 | 6.02 | 8.72 | 11.23 | 14.2 | 12.35 | 10.45 | 9.55 | 8.86 | 7.61 | 5.05 | 2.79 |
| CAPEOX+Bmab | 6.96 | 7.10 | 7.79 | 7.75 | 8.28 | 10.18 | 10.27 | 9.89 | 9.51 | 8.65 | 7.88 | 5.74 |
| Treatment | 1st Line | 2nd Line | 3rd Line | 4th Line | 5th Line | 6th Line | 7th Line | 8th Line | 9th Line | 10th Line | 11th Line |
|---|---|---|---|---|---|---|---|---|---|---|---|
| FOLFOX | 0.47 | 2.46 | 4.47 | 11.03 | 10.56 | 15.06 | 14.08 | 11.18 | 11.44 | 9.70 | 9.55 |
| FOLFOX+Bmab | 5.04 | 12.97 | 8.29 | 7.98 | 8.63 | 7.81 | 8.55 | 14.57 | 19.83 | 6.11 | 0.23 |
| FOLFOX+Cmab | 0.71 | 2.15 | 4.29 | 9.92 | 14.56 | 15.13 | 14.25 | 11.69 | 11.14 | 9.14 | 7.02 |
| FOLFOX+Pmab | 0.18 | 0.34 | 1.22 | 2.46 | 3.08 | 4.51 | 6.06 | 10.75 | 12.18 | 31.72 | 27.50 |
| FOLFIRI | 1.64 | 14.02 | 34.98 | 18.06 | 15.19 | 9.22 | 4.76 | 1.58 | 0.45 | 0.11 | 0.01 |
| FOLFIRI+Bmab | 37.84 | 30.76 | 14.14 | 9.38 | 4.81 | 2.04 | 0.68 | 0.25 | 0.08 | 0.02 | 0.00 |
| FOLFIRI+Cmab | 0.42 | 2.15 | 5.39 | 16.15 | 18.28 | 16.84 | 13.85 | 11.41 | 8.42 | 5.05 | 2.05 |
| FOLFIRI+Pmab | 0.01 | 0.13 | 0.64 | 3.49 | 7.04 | 13.58 | 22.39 | 15.35 | 17.52 | 12.73 | 7.11 |
| FOLFOXIRI+Bmab | 0.48 | 0.78 | 4.26 | 3.26 | 3.38 | 4.53 | 4.76 | 5.54 | 7.54 | 19.83 | 45.64 |
| CAPEOX | 37.05 | 23.78 | 14.23 | 9.67 | 6.78 | 3.93 | 2.20 | 1.27 | 0.66 | 0.35 | 0.07 |
| CAPEOX+Bmab | 16.15 | 10.45 | 8.10 | 8.59 | 7.70 | 7.35 | 8.40 | 16.42 | 10.74 | 5.27 | 0.82 |
| Treatment | Overall Survival | Adverse Events Grade ≥ 3 |
|---|---|---|
| FOLFOX | 0.65 | 0.40 |
| FOLFOX+Bmab | 0.33 | 0.50 |
| FOLFOX+Cmab | 0.88 | 0.42 |
| FOLFOX+Pmab | 0.77 | 0.19 |
| FOLFIRI | 0.19 | 0.71 |
| FOLFIRI+Bmab | 0.50 | 0.87 |
| FOLFIRI+Cmab | 0.77 | 0.49 |
| FOLFIRI+Pmab | 0.43 | 0.32 |
| FOLFOXIRI | 0.09 | - |
| FOLFOXIRI+Bmab | 0.39 | 0.18 |
| CAPEOX | 0.52 | 0.84 |
| CAPEOX+Bmab | 0.49 | 0.57 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoang, T.; Kim, J. Combining Correlated Outcomes and Surrogate Endpoints in a Network Meta-Analysis of Colorectal Cancer Treatments. Cancers 2020, 12, 2663. https://doi.org/10.3390/cancers12092663
Hoang T, Kim J. Combining Correlated Outcomes and Surrogate Endpoints in a Network Meta-Analysis of Colorectal Cancer Treatments. Cancers. 2020; 12(9):2663. https://doi.org/10.3390/cancers12092663
Chicago/Turabian StyleHoang, Tung, and Jeongseon Kim. 2020. "Combining Correlated Outcomes and Surrogate Endpoints in a Network Meta-Analysis of Colorectal Cancer Treatments" Cancers 12, no. 9: 2663. https://doi.org/10.3390/cancers12092663
APA StyleHoang, T., & Kim, J. (2020). Combining Correlated Outcomes and Surrogate Endpoints in a Network Meta-Analysis of Colorectal Cancer Treatments. Cancers, 12(9), 2663. https://doi.org/10.3390/cancers12092663