Prognostic Significance of Incidental Deep Vein Thrombosis in Patients with Cancer Presenting with Incidental Pulmonary Embolism

Abstract
1. Introduction
2. Results
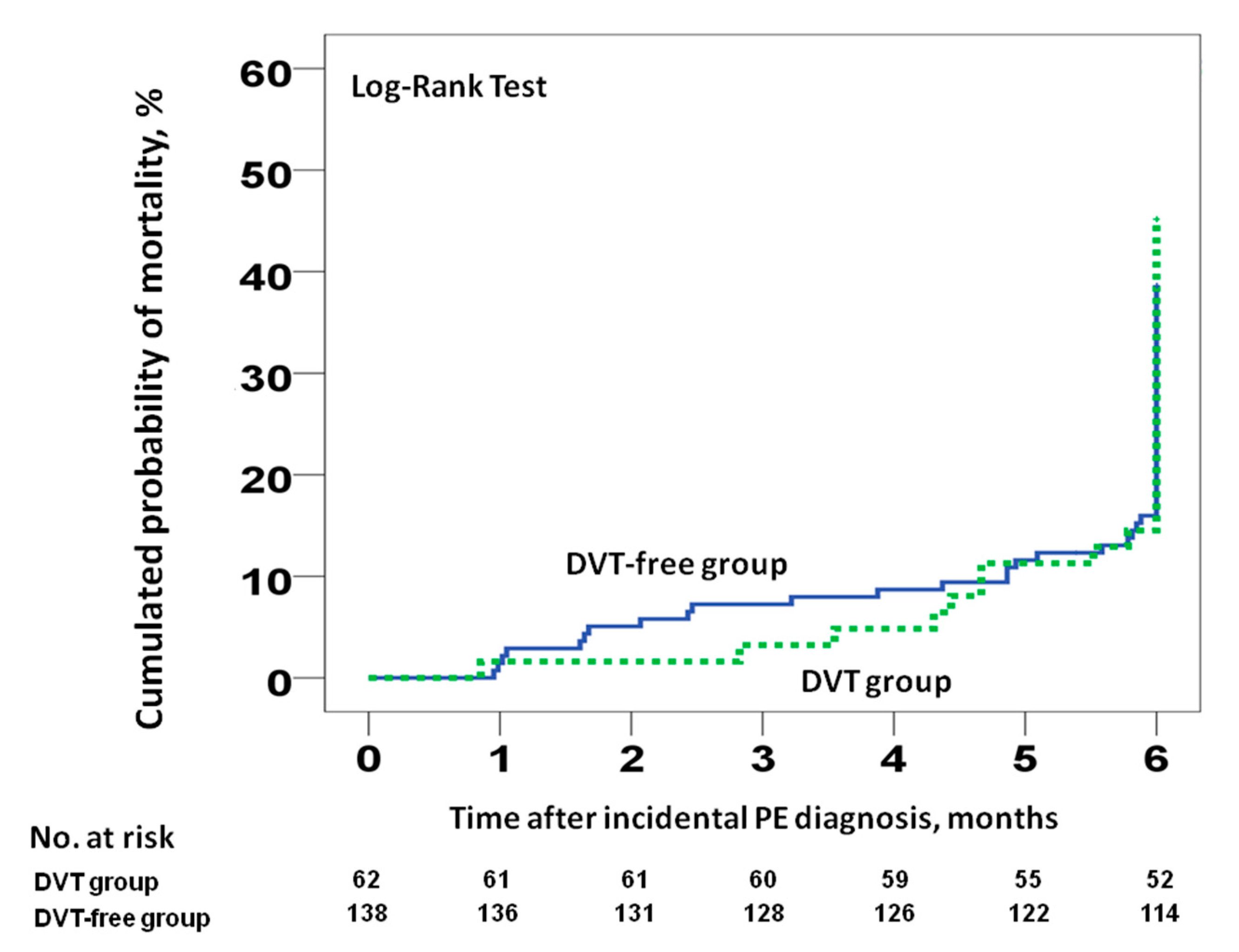
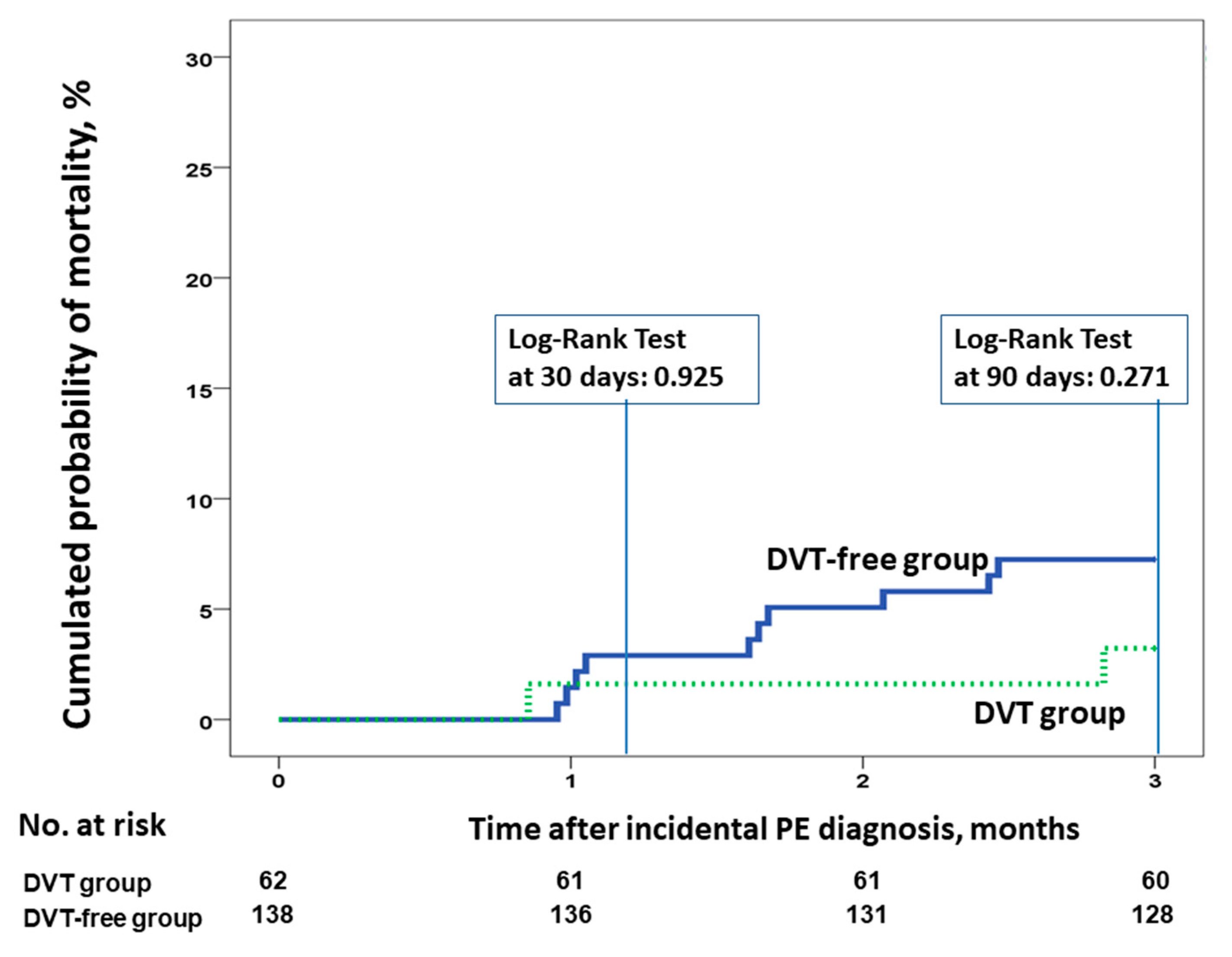
2.1. Primary and Secondary Outcomes
2.2. Venous Thromboembolism (VTE) Recurrence and Bleeding
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Setting
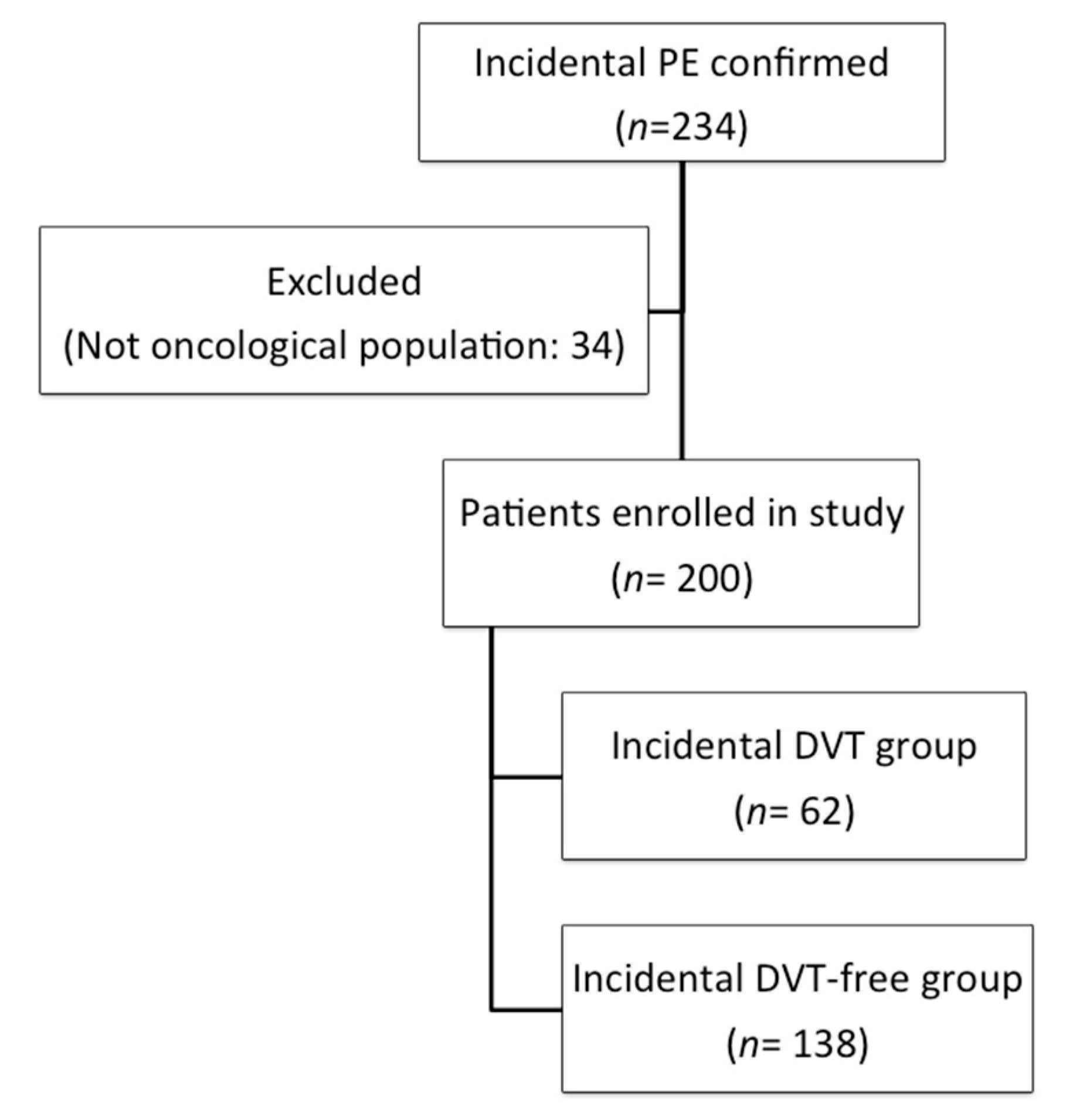
4.3. Eligibility
4.4. Lower Limb Ultrasound
4.5. Study Endpoints and Outcome Measures
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Margaglione, M.; Brancaccio, V.; De Lucia, D.; Martinelli, I.; Ciampa, A.; Grandone, E.; Di Minno, G. Inherited thrombophilic risk factors and venous thromboembolism: Distinct role in peripheral deep venous thrombosis and pulmonary embolism. Chest 2000, 118, 1405–1411. [Google Scholar] [CrossRef] [PubMed]
- Laporte, S.; Mismetti, P.; Décousus, H.; Uresandi, F.; Otero, R.; Lobo, J.L.; Monreal, M.; Arcelus, J.I.; Barba, R.; Blanco, A.; et al. Clinical predictors for fatal pulmonary embolism in 15 520 patients with venous thromboembolism: Findings from the Registro Informatizado de la Enfermedad TromboEmbolica venosa (RIETE) registry. Circulation 2008, 117, 1711–1716. [Google Scholar] [CrossRef] [PubMed]
- Goldhaber, S.Z.; Visani, L.; De Rosa, M. Acute pulmonary embolism: Clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet 1999, 353, 1386–1389. [Google Scholar] [CrossRef]
- The Columbus Investigators. Low-molecular-weight heparin in the treatment of patients with venous thromboembolism. N. Engl. J. Med. 1997, 337, 657–662. [Google Scholar]
- Huisman, M.V.; Buller, H.R.; Ten Cate, J.W.; Van Royen, E.A.; Vreeken, J.; Kersten, M.J.; Bakx, R. Unexpected high prevalence of silent pulmonary embolism in patients with deep venous thrombosis. Chest 1989, 95, 498–502. [Google Scholar] [CrossRef]
- Moser, K.M.; Fedullo, P.F.; LitteJohn, J.K.; Crawford, R. Frequent asymptomatic pulmonary embolism in patients with deep venous thrombosis. JAMA 1994, 271, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Girard, P.; Musset, D.; Parent, F.; Maitre, S.; Phlippoteau, C.; Simonneau, G. High prevalence of detectable deep venous thrombosis in patients with acute pulmonary embolism. Chest 1999, 116, 903–908. [Google Scholar] [CrossRef]
- Jiménez, D.; Aujesky, D.; Díaz, G.; Monreal, M.; Otero, R.; Martí, D.; Martín, E.; Aracil, E.; Sueiro, A.; Yusen, R.D.; et al. Prognostic significance of deep vein thrombosis in patients presenting with acute symptomatic pulmonary embolism. Am. J. Respir. Crit. Care Med. 2010, 181, 983–991. [Google Scholar] [CrossRef]
- Girard, P.; Sanchez, O.; Leroyer, C.; Musset, D.; Meyer, G.; Stern, J.B.; Parent, F. Deep Venous Thrombosis in Patients With Acute Pulmonary Embolism. Chest 2005, 128, 1593–1600. [Google Scholar] [CrossRef]
- Jiménez, D.; Aujesky, D.; Moores, L.; Gómez, V.; Martí, D.; Briongos, S.; Monreal, M.; Barrios, V.; Konstantinides, S.; Yusen, R.D. Combinations of prognostic tools for identification of high-risk normotensive patients with acute symptomatic pulmonary embolism. Thorax 2011, 66, 75–81. [Google Scholar] [CrossRef]
- Jiménez, D.; Kopecna, D.; Tapson, V.; Briese, B.; Schreiber, D.; Lobo, J.L.; Monreal, M.; Aujesky, D.; Sanchez, O.; Meyers, G.; et al. PROTECT Investigators. Derivation and validation of multimarker prognostication for normotensive patients with acute symptomatic pulmonary embolism. Am. J. Respir. Crit. Care Med. 2014, 189, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Vedovati, M.C.; Becattini, C.; Agnelli, G.; Kamphuisen, P.W.; Masotti, L.; Pruszcyk, P.; Casazza, F.; Salvi, A.; Grifoni, S.; Carugati, A.; et al. Multidetector CT scan for acute pulmonary embolism: Embolic burden and clinical outcome. Chest 2012, 142, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Nendaz, M.R.; Bandelier, P.; Aujesky, D.; Cornuz, J.; Roy, P.M.; Bounameaux, H.; Perrier, A. Validation of a risk score identifying patients with acute pulmonary embolism, who are at low risk of clinical adverse outcome. Thromb. Haemost. 2004, 91, 1232–1236. [Google Scholar] [PubMed]
- Kabrhel, C.; Okechukwu, I.; Hariharan, P.; Takayesu, J.K.; MacMahon, P.; Haddad, F.; Chang, Y. Factors associated with clinical deterioration shortly after PE. Thorax 2014, 69, 835–842. [Google Scholar] [CrossRef]
- Jiménez, D.; Yusen, R.D.; Otero, R.; Uresandi, F.; Nauffal, D.; Laserna, E.; Conget, F.; Oribe, M.; Cabezudo, M.A.; Díaz, G. Prognostic models for selecting patients with acute pulmonary embolism for initial outpatient therapy. Chest 2007, 132, 24–30. [Google Scholar] [CrossRef]
- Becattini, C.; Cohen, A.T.; Agnelli, G.; Howard, L.; Castejón, B.; Trujillo-Santos, J.; Monreal, M.; Perrier, A.; Yusen, R.D.; Jiménez, D. Risk stratification of patients with acute symptomatic pulmonary embolism based on presence or absence of lower extremity DVT: Systematic review and meta-Analysis. Chest 2016, 149, 192–200. [Google Scholar] [CrossRef]
- Prandoni, P.; Falanga, A.; Piccioli, A. Cancer and venous thromboembolism. Lancet Oncol. 2005, 6, 401–410. [Google Scholar] [CrossRef]
- Falanga, A.; Zacharski, L. Deep vein thrombosis in cancer: The scale of the problem and approaches to management. Ann. Oncol. 2005, 16, 696–701. [Google Scholar] [CrossRef]
- Font, C.; Farrús, B.; Vidal, L.; Caralt, T.M.; Visa, L.; Mellado, B.; Tàssies, D.; Monteagudo, J.; Reverter, J.C.; Gascon, P. Incidental versus symptomatic venous thrombosis in cancer: A prospective observational study of 340 consecutive patients. Ann. Oncol. 2011, 22, 2101–2106. [Google Scholar] [CrossRef]
- Gladish, G.W.; Choe, D.H.; Marom, E.M.; Sabloff, B.S.; Broemeling, L.D.; Munden, R.F. Incidental pulmonary emboli in oncology patients: Prevalence, CT evaluation, and natural history. Radiology 2006, 240, 246–255. [Google Scholar] [CrossRef]
- Den Exter, P.L.; Hooijer, J.; Dekkers, O.M.; Huisman, M.V. Risk of recurrent venous thromboembolism and mortality in patients with cancer incidentally diagnosed with pulmonary embolism: A comparison with symptomatic patients. J. Clin. Oncol. 2011, 29, 2405–2409. [Google Scholar] [CrossRef]
- Browne, A.M.; Cronin, C.G.; English, C.; Nimhuircheartaigh, J.; Murphy, J.M.; Bruzzi, J.F. Unsuspected pulmonary emboli in oncology patients undergoing routine computed tomography Imaging. J. Thorac. Oncol. 2010, 5, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Ageno, W.; Becattini, C.; Galli, L.; Gianni, M.; Riva, N.; Imberti, D.; Squizzato, A.; Venco, A.; Agnelli, G. Prevalence and Clinical History of Incidental, Asymptomatic Pulmonary Embolism: A Meta-Analysis. Thromb. Res. 2010, 125, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Kraaijpoel, N.; Bleker, S.M.; Meyer, G.; Mahé, I.; Muñoz, A.; Bertoletti, L.; Bartels-Rutten, A.; Beyer-Westendorf, J.; Porreca, E.; Boulon, C.; et al. Treatment and long-term clinical outcomes of incidental pulmonary embolism in patients with cancer: An international prospective cohort study. J. Clin. Oncol. 2019, 37, 1713–1720. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Mulder, F.I.; Di Nisio, M.; Ay, C.; Carrier, M.; Bosch, F.T.M.; Segers, A.; Kraajipoel, N.; Grosso, M.A.; Zhang, G.; Verhamme, P.; et al. Clinical implications of incidental venous thromboembolism in cancer patients. Eur. Respir. J. 2020, 55, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zondag, W.; Kooiman, J.; Klok, F.A.; Dekkers, O.M.; Huisman, M.V. Outpatient versus inpatient treatment in patients with pulmonary embolism: A meta-analysis. Eur. Respir. J. 2013, 42, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Di Nisio, M.; Lee, A.Y.Y.; Carrier, M.; Liebman, H.A.; Khorana, A.A. Diagnosis and treatment of incidental venous thromboembolism in cancer patients: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 880–883. [Google Scholar] [CrossRef]
- Wicki, J.; Perrier, A.; Perneger, T.V.; Bounameaux, H.; Junod, A.F. Predicting adverse outcome in patients with acute pulmonary embolism: A risk score. Thromb. Haemost. 2000, 84, 548–552. [Google Scholar] [CrossRef]
- Chew, H.K.; Wun, T.; Harvey, D.; Zhou, H.; White, R.H. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch. Intern. Med. 2006, 166, 458–464. [Google Scholar] [CrossRef]
- Gale, A.J.; Gordon, S.G. Update on Tumor Cell Procoagulant Factors. Acta Haematol. 2001, 106, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Den Exter, P.L.; Goḿez, V.; Jimeńez, D.; Trujillo-Santos, J.; Muriel, A.; Huisman, M.V.; Monreal, M. A clinical prognostic model for the identification of low-risk patients with acute symptomatic pulmonary embolism and active cancer. Chest 2013, 143, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 2, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Shahjehan, F.; Merchea, A.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Kasi, P.M. Body Mass Index and Long-Term Outcomes in Patients With Colorectal Cancer. Front. Oncol. 2018, 17, e620. [Google Scholar] [CrossRef]
- Kang, J.; Lee, S.H.; Son, J.H.; Lee, J.W.; Choi, Y.H.; Choi, J.H.; Paik, W.H.; Ryu, J.K.; Kim, Y.T. Body mass index and weight change during initial period of chemotherapy affect survival outcome in advanced biliary tract cancer patients. PLoS ONE 2018, 2, e13. [Google Scholar] [CrossRef]
- Tsang, N.M.; Pai, P.C.; Chuang, C.C.; Chuang, W.C.; Tseng, C.K.; Chang, K.P.; Yen, T.C.; Lin, J.D.; Chang, J.T. Overweight and obesity predict better overall survival rates in cancer patients with distant metastases. Cancer Med. 2016, 5, 665–675. [Google Scholar] [CrossRef]
- Giorgi-Pierfranceschi, M.; López-Núñez, J.J.; Monreal, M.; Cattabiani, C.; Lodigiani, C.; Di Micco, P.; Bikdeli, B.; Braester, A.; Soler, S.; Dentali, F. RIETE researchers. Morbid Obesity and Mortality in Patients With VTE: Findings From Real-Life Clinical Practice. Chest 2020, 157, 1617–1625. [Google Scholar] [CrossRef]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S.; Subcommittee on Control of Anticoagulation. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | DVT Group (n = 62) | DVT-Free Group (n = 138) | Patients (n = 200) |
|---|---|---|---|
| Male sex, n (%) | 34 (54.8) | 80 (58) | 114 (57) |
| Age (years), mean (SD) | 66.6 (10.9) | 64.7 (12.9) | 65.3 (12.4) |
| Weight (kg), mean (SD) | 75.5 (11.2) | 72.6 (5.1) | 73.6 (14.1) |
| Metastases, n (%) | 42 (72.4) | 73 (57.5) | 115 (62.2) |
| Oncological treatment at VTE event, n (%) | 47 (75.8) | 86 (62.3) | 133 (66.5) |
| Alkylating agents | 5 (8.1) | 1 (0.7) | 6 (3) |
| Platinum-based agents | 21 (33.9) | 49 (35.5) | 70 (35) |
| Topoisomerase inhibitors | 7 (11.3) | 19 (13.8) | 26 (13) |
| Mitotic inhibitors | 9 (14.5) | 9 (6.5) | 18 (9) |
| Antimetabolites | 32 (51.6) | 63 (45.7) | 95 (47.5) |
| Tyrosine kinase inhibitors | 3 (4.8) | 3 (2.2) | 6 (3) |
| Monoclonal antibody | 6 (9.7) | 18 (13) | 24 (12) |
| Hormone treatment | 0 (0) | 1 (0.7) | 1 (0.5) |
| Number of drugs, n (%) | |||
| 1 | 18 (38.3) | 27 (31.4) | 45 (22.5) |
| 2 | 24 (51.1) | 42 (48.8) | 66 (33) |
| ≥3 | 5 (10.6) | 17 (19.8) | 22 (11) |
| Central venous catheter, n (%) | 6 (12.2) | 14 (10.9) | 20 (11.3) |
| ECOG performance status, n (%) | |||
| 0 | 15 (26.3) | 37 (31.9) | 52 (30.1) |
| 1 | 34 (59.6) | 65 (56) | 99 (57.2) |
| 2 | 6 (10.5) | 10 (8.6) | 16 (9.2) |
| 3 | 1 (1.8) | 2 (1.7) | 3 (1.7) |
| 4 | 1 (1.8) | 2 (1.7) | 3 (1.7) |
| Performance status ECOG ≤2, n (%) | 55 (96.5) | 112 (96.6) | 167 (96.5) |
| Cancer type, n (%) | |||
| Colorectal | 21 (33.9) | 38 (27.5) | 59 (29.5) |
| Lung | 10 (16.1) | 25 (18.1) | 35 (17.5) |
| Breast | 6 (9.7) | 10 (7.2) | 16 (8) |
| Gynecological | 5 (8.1) | 10 (7.2) | 15 (7.5) |
| Upper gastrointestinal | 4 (6.5) | 10 (7.2) | 14 (7) |
| Bladder | 1 (1.6) | 12 (8.7) | 13 (6.5) |
| Hematological | 3 (4.8) | 4 (2.9) | 7 (3.5) |
| Pancreatic | 2 (3.2) | 5 (3.6) | 7 (3.5) |
| Kidney | 1 (1.6) | 4 (2.9) | 5 (2.5) |
| Brain | 1 (1.6) | 3 (2.2) | 4 (2) |
| Others | 8 (12.9) | 17 (12.3) | 25 (12.5) |
| Histology, n (%) | |||
| Adenocarcinoma | 37 (59.7) | 73 (52.9) | 110 (55) |
| Epidermoid | 3 (4.8) | 12 (8.7) | 15 (7.5) |
| Urothelial | 1 (1.6) | 12 (8.7) | 13 (6.5) |
| Hematological | 3 (4.8) | 4 (2.9) | 7 (3.5) |
| Oat cell | 1 (1.6) | 3 (2.2) | 4 (2) |
| Others | 17 (27.4) | 34 (24.6) | 51 (25.5) |
| Creatinine (mL/min), mean (SD) | 0.85 (0.28) | 0.87 (0.66) | 0.87 (0.57) |
| Creatinine clearance (mL/min), mean (SD) | 83.5 (24.5) | 92.9 (65.4) | 90 (56.2) |
| Anticoagulant treatment, n (%) | |||
| Enoxaparin | 28 (45.2) | 64 (46.4) | 92 (46) |
| Tinzaparin | 24 (38.7) | 46 (33.3) | 70 (35) |
| Bemiparin | 9 (14.5) | 19 (13.8) | 28 (14) |
| Dalteparin | 1 (1.6) | 8 (5.8) | 9 (4.5) |
| Vitamin K antagonist | 0 (0) | 1 (0.7) | 1 (0.5) |
| VTE recurrent, n (%) | 6 (9.7) | 15 (10.9) | 21 (10.5) |
| Bleeding, n (%) | 5 (8.2) | 10 (7.3) | 15 (7.5) |
| Major bleeding, n (%) | 1 (20) | 1 (10) | 2 (1) |
| 1-month mortality, n (%) | 1 (1.6) | 2 (1.4) | 3 (1.5) |
| 3-month mortality, n (%) | 2 (3.2) | 10 (7.2) | 12 (6) |
| 6-month mortality, n (%) | 9 (14.5) | 22 (15.9) | 31 (15.5) |
| Deaths, n (%) | 28 (45.2) | 53 (38.4) | 81 (40.5) |
| Variable | No-Deaths (n = 119) | With Deaths (n = 81) |
|---|---|---|
| Male sex, n (%) | 71 (59.7) | 43 (53.1) |
| Age (years), mean (SD) | 65.3 (12.7) | 65.4 (12) |
| Weight (kg), mean (SD) | 74.3 (14.5) | 72.5 (13.6) |
| DVT, n (%) | 34 (28.3) | 28 (34.6) |
| Metastases, n (%) | 55 (50.5) | 60 (78.9) |
| Oncological Treatment at the Time of a VTE Event, n (%) | 72 (60.5) | 61 (78.2) |
| Central venous catheter, n (%) | 15 (13.9) | 5 (7.2) |
| ECOG performance status, n (%) | ||
| 0 | 34 (32.7) | 18 (26.1) |
| 1 | 58 (55.8) | 41 (59.4) |
| 2 | 7 (6.7) | 9 (13) |
| 3 | 2 (1.9) | 1 (1.4) |
| 4 | 3 (2.9) | 0 |
| ECOG performance status ≤2, n (%) | 99 (95.2) | 58 (98.6) |
| Cancer type, n (%) | ||
| Colorectal | 41 (34.5) | 18 (22.2) |
| Lung | 17 (14.3) | 18 (22.2) |
| Breast | 7 (5.9) | 9 (11.1) |
| Gynecological | 9 (7.6) | 6 (7.4) |
| Upper gastrointestinal | 10 (8.4) | 4 (4.9) |
| Bladder | 7 (5.9) | 6 (7.4) |
| Hematological | 5 (4.2) | 2 (2.5) |
| Pancreatic | 2 (1.7) | 5 (6.2) |
| Kidney | 2 (1.7) | 3 (3.7) |
| Brain | 2 (1.7) | 2 (2.5) |
| Others | 17 (14.3) | 8 (9.9) |
| Histology, n (%) | ||
| Adenocarcinoma | 67 (56.3) | 43 (53.1) |
| Epidermoid | 8 (6.7) | 8 (9.9) |
| Urothelial | 8 (6.7) | 6 (7.4) |
| Hematological | 5 (4.2) | 2 (2.5) |
| Oat cell | 5 (4.2) | 0 (0) |
| Others | 26 (21.9) | 22 (27.1) |
| Creatinine (mL/min), mean (SD) | 0.89 (0.7) | 0.84 (0.3) |
| Creatinine clearance (mL/min), mean (SD) | 86.4 (24.6) | 95.4 (83.1) |
| Recurrence, n (%) | 15 (12.6) | 6 (7.4) |
| Bleeding, n (%) | 6 (5.1) | 9 (11.3) |
| Major bleeding, n (%) | 1 (16.7) | 1 (11.1) |
| Risk Factor | Unadjusted HR (95% CI) | p-Value | Adjusted HR (95% CI) | p-Value |
|---|---|---|---|---|
| Male sex | 1.52 (0.6–3.86) | 0.383 | ||
| Presence of DVT | 1.09 (0.43–2.75) | 0.855 | ||
| Weight, per kilogram | 0.95 (0.91–0.99) | 0.024 | 0.96 (0.92–0.99) | 0.032 |
| Age, per year | 1.03 (0.99–1.01) | 0.107 | ||
| Central venous catheter | 0.28 (0.04–2.09) | 0.213 | ||
| Creatinine clearance | 1 (0.99–1.01) | 0.613 | ||
| Metastases | 9.12 (1.96–42.34) | 0.005 | 10.26 (2.35–44.9) | 0.002 |
| Oncological treatment at thrombotic event | 2 (0.55–7.3) | 0.297 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barca-Hernando, M.; Ortega-Rivera, R.; Lopez-Ruz, S.; Elias-Hernandez, T.; Asensio-Cruz, M.I.; Marin-Romero, S.; Toral, J.; Montero, E.; Sanchez, V.; Arellano, E.; et al. Prognostic Significance of Incidental Deep Vein Thrombosis in Patients with Cancer Presenting with Incidental Pulmonary Embolism. Cancers 2020, 12, 2267. https://doi.org/10.3390/cancers12082267
Barca-Hernando M, Ortega-Rivera R, Lopez-Ruz S, Elias-Hernandez T, Asensio-Cruz MI, Marin-Romero S, Toral J, Montero E, Sanchez V, Arellano E, et al. Prognostic Significance of Incidental Deep Vein Thrombosis in Patients with Cancer Presenting with Incidental Pulmonary Embolism. Cancers. 2020; 12(8):2267. https://doi.org/10.3390/cancers12082267
Chicago/Turabian StyleBarca-Hernando, Maria, Rocio Ortega-Rivera, Sergio Lopez-Ruz, Teresa Elias-Hernandez, Maria Isabel Asensio-Cruz, Samira Marin-Romero, Javier Toral, Emilio Montero, Veronica Sanchez, Elena Arellano, and et al. 2020. "Prognostic Significance of Incidental Deep Vein Thrombosis in Patients with Cancer Presenting with Incidental Pulmonary Embolism" Cancers 12, no. 8: 2267. https://doi.org/10.3390/cancers12082267
APA StyleBarca-Hernando, M., Ortega-Rivera, R., Lopez-Ruz, S., Elias-Hernandez, T., Asensio-Cruz, M. I., Marin-Romero, S., Toral, J., Montero, E., Sanchez, V., Arellano, E., Sanchez-Diaz, J. M., Real-Dominguez, M., Otero-Candelera, R., & Jara-Palomares, L. (2020). Prognostic Significance of Incidental Deep Vein Thrombosis in Patients with Cancer Presenting with Incidental Pulmonary Embolism. Cancers, 12(8), 2267. https://doi.org/10.3390/cancers12082267