Prognostic Significance of CD105- and CD31-Assessed Microvessel Density in Paired Biopsies and Surgical Samples of Laryngeal Carcinoma

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Conventional Clinical-Pathological Variables and Prognosis
2.2. Association between Clinical-Pathological Variables and Neo-Angiogenesis Marker (CD105 and CD31) Expression in Biopsies and Surgical Specimens
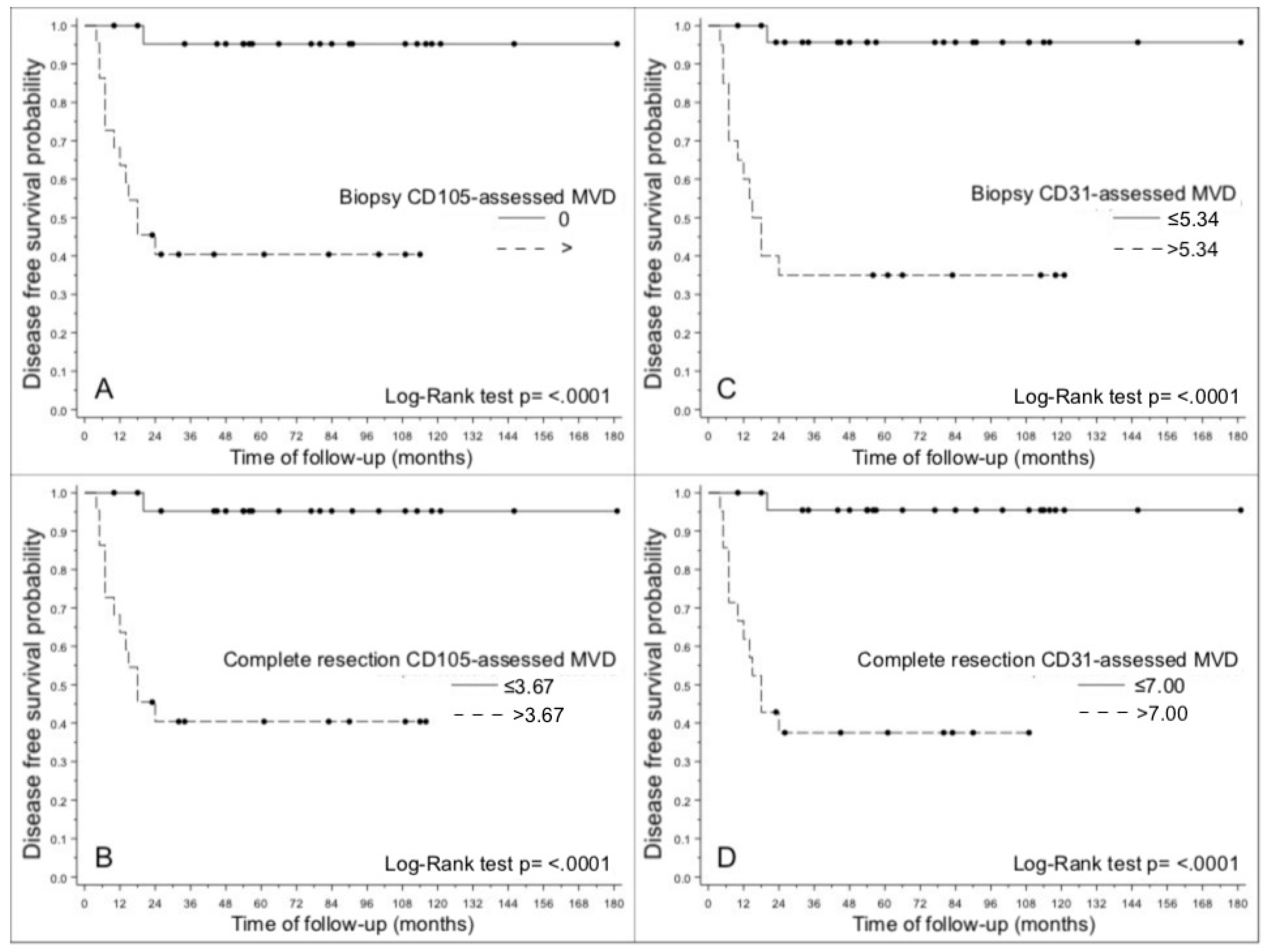
2.3. CD105- and CD31-assessed MVD in Biopsies and Paired Surgical Specimens, and LSCC Prognosis
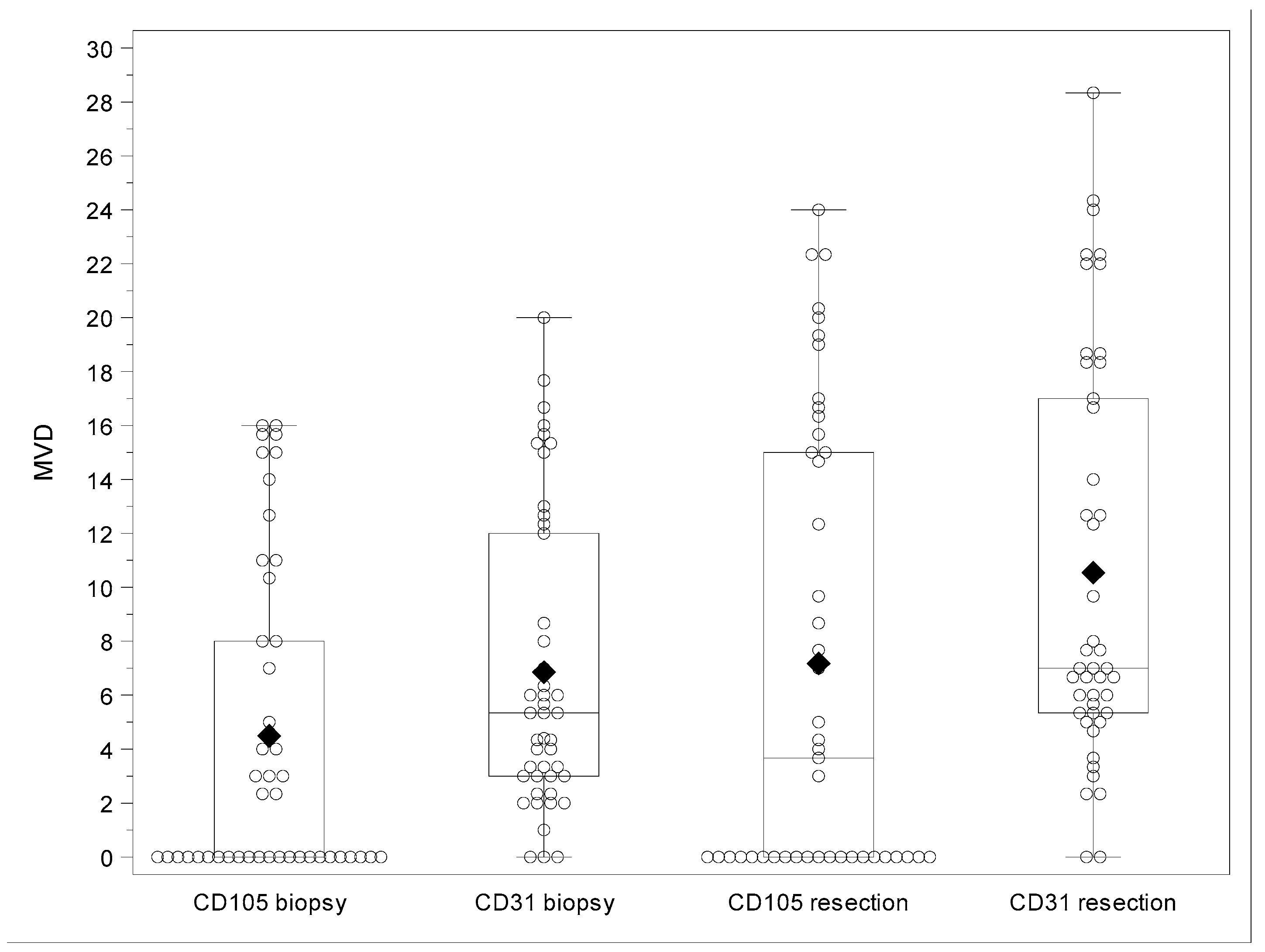
2.4. Comparison between CD105- and CD31-Assessed MVD in Biopsies and Paired Surgical Specimens of LSCC
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Immunohistochemistry
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dong, K.F.; Huo, M.Q.; Sun, H.Y.; Li, T.K.; Li, D. Mechanism of Astragalus membranaceus in the treatment of laryngeal cancer based on gene co-expression network and molecular docking. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 1–10. [Google Scholar] [CrossRef]
- Lionello, M.; Staffieri, A.; Marioni, G. Potential prognostic and therapeutic role for angiogenesis markers in laryngeal carcinoma. Acta Otolaryngol. 2012, 132, 574–582. [Google Scholar] [CrossRef]
- Franco, P.I.R.; Rodrigues, A.P.; De Menezes, L.B.; Miguel, M.P.; Francoa, P.I.R.; Leite, L.B.D.M. Tumor microenvironment components: Allies of cancer progression. Pathol. Res. Pract. 2020, 216, 152729. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; Marino, F.; Blandamura, S.; D’Alessandro, E.; Giacomelli, L.; Guzzardo, V.; Lionello, M.; De Filippis, C.; Staffieri, A. Neoangiogenesis in laryngeal carcinoma: Angiogenin and CD105 expression is related to carcinoma recurrence rate and disease-free survival. Histopathology 2010, 57, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulou, M.; Psyrri, A.; Argiris, A. Targeting angiogenesis in head and neck cancer. Oral Oncol. 2015, 51, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Franz, L.; Tealdo, G.; Contro, G.; Bandolin, L.; Carraro, V.; Bd, L.G.; Alessandrini, L.; Blandamura, S.; Marioni, G. Biological tumor markers (maspin, CD105, nm23-H1) and disease relapse in laryngeal cancer: Cluster analysis. Head Neck 2020, 42, 2129–2136. [Google Scholar] [CrossRef]
- Marioni, G.; D’Alessandro, E.; Giacomelli, L.; Staffieri, A. CD105 is a marker of tumour vasculature and a potential target for the treatment of head and neck squamous cell carcinoma. J. Oral Pathol. Med. 2010, 39, 361–367. [Google Scholar] [CrossRef]
- Dallas, N.A.; Samuel, S.; Xia, L.; Fan, F.; Gray, M.J.; Lim, S.J.; Ellis, L.M. Endoglin (CD105): A Marker of Tumor Vasculature and Potential Target for Therapy. Clin. Cancer Res. 2008, 14, 1931–1937. [Google Scholar] [CrossRef]
- Ollauri-Ibáñez, C.; Núñez-Gómez, E.; Egido-Turrión, C.; Silva-Sousa, L.; Díaz-Rodríguez, E.; Rodríguez-Barbero, A.; López-Novoa, J.M.; Pericacho, M. Continuous endoglin (CD105) overexpression disrupts angiogenesis and facilitates tumor cell metastasis. Angiogenesis 2020, 23, 231–247. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, L.; Lin, Q.; Ren, W.; Xu, G. Prognostic value of endoglin-assessed microvessel density in cancer patients: A systematic review and meta-analysis. Oncotarget 2017, 9, 7660–7671. [Google Scholar] [CrossRef]
- Marioni, G.; Blandamura, S.; Nicolè, L.; Denaro, L.; Cazzador, D.; Pavone, C.; Giacomelli, L.; Guzzardo, V.; Fassina, A.; Mazzoni, A.; et al. Endoglin-based assessment of neoangiogenesis in sporadic VIII cranial nerve schwannoma. Pathol. Res. Pract. 2019, 215, 152648. [Google Scholar] [CrossRef] [PubMed]
- Schoonderwoerd, M.J.A.; Goumans, M.-J.; Hawinkels, L. Endoglin: Beyond the Endothelium. Biomolecules 2020, 10, 289. [Google Scholar] [CrossRef] [PubMed]
- Giotakis, A.I.; Lazaris, A.C.; Kataki, A.; Kontos, C.K.; Giotakis, E.I. Positive BCL2L12 expression predicts favorable prognosis in patients with laryngeal squamous cell carcinoma. Cancer Biomark. 2019, 25, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Takes, R.P.; De Jong, R.J.B.; Keuning, J.; Hermans, J.; Schuuring, E.; Van Krieken, H.J. Protein expression of cancer associated genes: Biopsy material compared to resection material in laryngeal cancer. Anticancer Res. 1999, 18, 4787–4791. [Google Scholar]
- Marioni, G.; Bottin, R.; Staffieri, A.; Altavilla, G. Spindle-cell Tumours of the Larynx: Diagnostic Pitfalls. A Case Report and Review of the Literature. Acta Otolaryngol. 2003, 123, 86–90. [Google Scholar] [CrossRef]
- Marioni, G.; Agostini, M.; Cappellesso, R.; Bedin, C.; Ottaviano, G.; Marchese-Ragona, R.; Lovato, A.; Cacco, T.; Giacomelli, L.; Nitti, D.; et al. miR-19a and SOCS-1 expression in the differential diagnosis of laryngeal (glottic) verrucous squamous cell carcinoma. J. Clin. Pathol. 2015, 69, 415–421. [Google Scholar] [CrossRef]
- Brcic, I.; Gallob, M.; Schwantzer, G.; Zrnc, T.; Weiland, T.; Thurnher, D.; Brcic, L. Concordance of tumor infiltrating lymphocytes, PD-L1 and p16 expression in small biopsies, resection and lymph node metastases of oropharyngeal squamous cell carcinoma. Oral Oncol. 2020, 106, 104719. [Google Scholar] [CrossRef]
- Zvrko, E.; Mikic, A.; Vuckovic, L. CD105 expression as a measure of microvessel density in supraglottic laryngeal squamous cell carcinoma. Eur. Arch. Otorhinolaryngol. 2009, 266, 1971–1976. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; John Wiley & Sons: New York, NY, USA, 2000. [Google Scholar]
- Tanaka, F.; Ishikawa, S.; Yanagihara, K.; Miyahara, R.; Kawano, Y.; Li, M.; Otake, Y.; Wada, H. Expression of angiopoietins and its clinical significance in non-small cell lung cancer. Cancer Res. 2002, 62, 7124–7129. [Google Scholar]
- Saadi, R.S.; Liu, Y.L.; Nathan, G.; Celebrezze, J.; Medich, D.; Silverman, J.F. Endoglin (CD105) and vascular endothelial growth factor as prognostic markers in colorectal cancer. Mod. Pathol. 2004, 17, 197–203. [Google Scholar] [CrossRef]
- Miyata, Y.; Sagara, Y.; Watanabe, S.-I.; Asai, A.; Matsuo, T.; Ohba, K.; Hayashi, T.; Sakai, H. CD105 is a more appropriate marker for evaluating angiogenesis in urothelial cancer of the upper urinary tract than CD31 or CD34. Virchows Archiv. 2013, 463, 673–679. [Google Scholar] [CrossRef]
- Marioni, G.; Ottaviano, G.; Giacomelli, L.; Staffieri, C.; Casarotti-Todeschini, S.; Bonandini, E.; Staffieri, A.; Blandamura, S. CD105-assessed micro-vessel density is associated with malignancy recurrence in laryngeal squamous cell carcinoma. Eur. J. Surg. Oncol. EJSO 2006, 32, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; Marino, F.; Giacomelli, L.; Staffieri, C.; Mariuzzi, M.L.; Violino, E.; De Filippis, C. Endoglin expression is associated with poor oncologic outcome in oral and oropharyngeal carcinoma. Acta Otolaryngol. 2006, 126, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; Ottaviano, G.; Marchese-Ragona, R.; Fasanaro, E.; Tealdo, G.; Zanotti, C.; Randon, B.; Giacomelli, L.; Stellini, E.; Blandamura, S. Nuclear survivin expression correlates with endoglin-assessed microvascularisation in laryngeal carcinoma. J. Clin. Pathol. 2017, 70, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; D’Alessandro, E.; Giacomelli, L.; De Filippis, C.; Calgaro, N.; Sari, M.; Staffieri, A.; Blandamura, S. Maspin nuclear localization is related to reduced density of tumour-associated micro-vessels in laryngeal carcinoma. Anticancer Res. 2007, 26, 4927–4932. [Google Scholar]
- Dorff, T.B.; Longmate, J.A.; Pal, S.K.; Stadler, W.; Fishman, M.N.; Vaishampayan, U.N.; Rao, A.; Pinksi, J.K.; Hu, J.S.; Quinn, D.; et al. Bevacizumab alone or in combination with TRC105 for patients with refractory metastatic renal cell cancer. Cancer 2017, 123, 4566–4573. [Google Scholar] [CrossRef]
- Kasprzak, A.; Adamek, A. Role of Endoglin (CD105) in the Progression of Hepatocellular Carcinoma and Anti-Angiogenic Therapy. Int. J. Mol. Sci. 2018, 19, 3887. [Google Scholar] [CrossRef]
- Brossa, A.; Buono, L.; Bussolati, B. Effect of the monoclonal antibody TRC105 in combination with Sunitinib on renal tumor derived endothelial cells. Oncotarget 2018, 9, 22680–22692. [Google Scholar] [CrossRef]
- Marioni, G.; Nicolè, L.; Cazzador, D.; Pavone, C.; D’Avella, M.; Martini, A.; Mazzoni, A.; Zanoletti, E. Endoglin (CD105) expression in neurofibromatosis type 2 vestibular schwannoma. Head Neck 2019, 41, 3612–3617. [Google Scholar] [CrossRef]
- Tian, H.; Huang, J.J.; Golzio, C.; Gao, X.; Hector-Greene, M.; Katsanis, N.; Blobe, G.C. Endoglin interacts with VEGFR2 to promote angiogenesis. FASEB J. 2018, 32, 2934–2949. [Google Scholar] [CrossRef]
- Marioni, G.; Blandamura, S.; Lionello, M.; Giacomelli, L.; Lovato, A.; Favaretto, N.; Breda, S.; Tealdo, G.; Guzzardo, V.; Ottaviano, G.; et al. Indications for postoperative radiotherapy in laryngeal carcinoma: A panel of tumor tissue markers for predicting locoregional recurrence in surgically treated carcinoma. A pilot study. Head Neck 2013, 36, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; Ottaviano, G.; Lovato, A.; Franz, L.; Bandolin, L.; Contro, G.; Giacomelli, L.; Alessandrini, L.; Stramare, R.; De Filippis, C.; et al. Expression of maspin tumor suppressor and mTOR in laryngeal carcinoma. Am. J. Otolaryngol. 2020, 41, 102322. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B. AJCC Staging Manual, 8th ed.; Springer: Basel, Switzerland, 2017. [Google Scholar]
- Cappellesso, R.; Marioni, G.; Crescenzi, M.; Giacomelli, L.; Guzzardo, V.; Mussato, A.; Staffieri, A.; Martini, A.; Blandamura, S.; Fassina, A. The prognostic role of the epithelial-mesenchymal transition markers E-cadherin and Slug in laryngeal squamous cell carcinoma. Histopathology 2015, 67, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, L.; Franz, L.; Ottaviano, G.; Ghi, M.G.; Lanza, C.; Blandamura, S.; Marioni, G. Prognostic role of programmed death ligand 1 (PD-L1) and the immune microenvironment in laryngeal carcinoma. Oral Oncol. 2020, 108, 104836. [Google Scholar] [CrossRef] [PubMed]
- Weidner, N.; Semple, J.P.; Welch, W.R.; Folkman, J. Tumor angiogenesis and metastasis—Correlation in invasive breast carcinoma. N. Engl. J. Med. 1991, 324, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Uno, H.; Cai, T.; Pencina, M.J.; D’Agostino, R.B.; Wei, L.J. On the C-statistics for evaluating overall adequacy of risk prediction procedures with censored survival data. Stat. Med. 2011, 30, 1105–1117. [Google Scholar] [CrossRef]
- Lin, L.I.-K. A Concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. = 45 | Without LSCC Recurrence (No. = 31) | With LSCC Recurrence (No. = 14) | * p-Value | HR (95%CI) |
|---|---|---|---|---|
| CD105 MVD (biopsy) | ||||
| Mean (SD) | 1.56 (3.47) | 10.98 (4.86) | ||
| Median (IQR) | 0.00 (0.00–2.34) | 11.84 (8.00–15.00) | <0.0001 | 1.221 (1.118; 1.334) |
| CD31 MVD (biopsy) | ||||
| Mean (SD) | 4.36 (3.85) | 12.36 (4.65) | ||
| Median (IQR) | 3.34 (2.34–5.34) | 13.84 (8.67–15.67) | <0.0001 | 1.202 (1.107; 1.306) |
| CD105 MVD (surgical specimen) | ||||
| Mean (SD) | 3.05 (5.68) | 16.31 (5.53) | ||
| Median (IQR) | 0.00 (0.00–4.34) | 16.84 (15.00–20.00) | <0.0001 | 1.195 (1.104;1.294) |
| CD31 MVD (surgical specimen) | ||||
| Mean (SD) | 7.19 (5.54) | 17.98 (5.82) | ||
| Median (IQR) | 6.00 (5.00–7.67) | 18.67 (14.00–22.34) | <0.0001 | 1.153 (1.083; 1.228) |
| pT | ||||
| T1–T2 | 17 (54.8%) | 04 (28.6%) | ||
| T3–T4 | 14 (45.2%) | 10 (71.4%) | 0.1304 | 2.450 (0.767; 7.823) |
| Pathological grade | ||||
| G1–G2 | 23 (74.2%) | 06 (42.9%) | ||
| G3 | 08 (25.8%) | 08 (57.1%) | 0.0302 | 3.250 (1.119; 9.433) |
| N status | ||||
| N0 ** | 26 (83.9%) | 08 (57.1%) | ||
| N+ | 05 (16.1%) | 06 (42.9%) | 0.0553 | 2.832 (0.977; 8.212) |
| Tumor stage | ||||
| I–II | 15 (48.4%) | 04 (28.6%) | ||
| III–IV | 16 (51.6%) | 10 (71.4%) | 0.2510 | 1.973 (0.618; 6.298) |
| Variable | No. of Cases | CD105-Assessed MVD (biopsy) Mean (SD) Median (IQR) | CD105-Assessed MVD (Surgical Specimen) Mean (SD) Median (IQR) | CD31-Assessed MVD (Biopsy) Mean (SD) Median (IQR) | CD31-Assessed MVD (Surgical Specimen) Mean (SD) Median (IQR) | ||||
|---|---|---|---|---|---|---|---|---|---|
| pT1–2 | 21 | 3.16 (4.99) 0.00 (0.00–4.00) | p = 0.1296 | 5.87 (8.24) 0.00 (0.00–14.67) | p = 0.2542 | 6.26 (4.77) 4.40 (3.00-7.00) | p = 0.9364 | 9.27 (7.68) 7.00 (4.67–17.00) | p = 0.2318 |
| pT3–4 | 24 | 5.65 (6.45) 3.00 (0.00-12.50) | 8.32 (8.43) 6.00 (0.00–15.84) | 7.36 (6.16) 5.51 (2.17–13.84) | 11.66 (7.34) 8.84 (6.00–17.51) | ||||
| N0 * | 34 | 2.67 (4.30) 0.0 (0.00–4.00) | p = 0.0008 | 4.53 (7.45) 0.00 (0.00–7.00) | p = 0.0002 | 5.26 (4.41) 4.17 (2.34–6.00) | p = 0.0025 | 8.42 (6.74) 6.67 (5.00–8.00) | p = 0.0019 |
| pN+ | 11 | 10.12 (6.72) 14.00 (3.00-15.67) | 15.37 (5.03) 15.00 (12.34–19.34) | 11.77 (5.91) 15.00 (4.40–15.67) | 17.09 (5.98) 17.00 (12.67–22.00) | ||||
| Stage I–II | 19 | 2.91 (4.86) 0.00 (0.00–4.00) | p = 0.1112 | 4.86 (8.00) 0.00 (0.00–7.67) | p = 0.0920 | 6.00 (4.75) 4.34 (3.00–7.00) | p = 0.7042 | 8.39 (7.54) 6.67 (3.67–7.67) | p = 0.0804 |
| Stage III–IV | 26 | 5.64 (6.38) 3.00 (0.00–11.00) | 8.87 (8.32) 7.84 (0.00–16.34) | 7.47 (6.05) 5.51 (2.34–13.00) | 12.12 (7.23) 11.01 (6.00–18.34) | ||||
| Grade 1–2 | 29 | 3.76 (5.78) 0.00 (0.00–4.00) | p = 0.1536 | 5.85 (7.94) 0.00 (0.00–9.67) | p = 0.2020 | 6.41 (5.76) 4.34 (3.00–7.00) | p = 0.3363 | 9.17 (7.28) 6.67 (5.00–12.67) | p = 0.1318 |
| Grade 3 | 16 | 5.81 (6.02) 4.50 (0.00–9.50) | 9.59 (8.75) 11.84 (0.00–16.51) | 7.65 (5.16) 6.00 (3.50–12.51) | 13.03 (7.51) 12.51 (6.01–20.17) | ||||
| Variable | UNO’s Concordance Statistic | SE * | 95%CI |
|---|---|---|---|
| CD105-assessed MVD (biopsy) | 0.8461 | 0.0396 | 0.7685; 0.9237 |
| CD31-assessed MVD (biopsy) | 0.8283 | 0.0444 | 0.7413; 0.9153 |
| CD105-assessed MVD (surgical specimen) | 0.8880 | 0.0316 | 0.8261; 0.9499 |
| CD31-assessed MVD (surgical specimen) | 0.8520 | 0.0442 | 0.7654; 0.9386 |
| Variables Tested for Concordance | Concordance Coefficient * | Bootstrap 95% CI ** |
|---|---|---|
| CD105-assessed MVD(biopsy)/CD31-assessed MVD(biopsy) | 0.8519 | 0.7589; 0.9120 |
| CD105-assessed MVD(surgical specimen)/CD31-assessed MVD(surgical specimen) | 0.8593 | 0.7805; 0.9082 |
| CD105-assessed MVD(biopsy)/CD105-assessed MVD (surgical specimen) | 0.7352 | 0.565; 0.8329 |
| CD31-assessed MVD(biopsy)/CD31-assessed MVD (surgical specimen) | 0.6775 | 0.5273; 0.7865 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marioni, G.; Franz, L.; Ottaviano, G.; Contro, G.; Tealdo, G.; Carli, A.; Frigo, A.C.; Nicolai, P.; Alessandrini, L. Prognostic Significance of CD105- and CD31-Assessed Microvessel Density in Paired Biopsies and Surgical Samples of Laryngeal Carcinoma. Cancers 2020, 12, 2059. https://doi.org/10.3390/cancers12082059
Marioni G, Franz L, Ottaviano G, Contro G, Tealdo G, Carli A, Frigo AC, Nicolai P, Alessandrini L. Prognostic Significance of CD105- and CD31-Assessed Microvessel Density in Paired Biopsies and Surgical Samples of Laryngeal Carcinoma. Cancers. 2020; 12(8):2059. https://doi.org/10.3390/cancers12082059
Chicago/Turabian StyleMarioni, Gino, Leonardo Franz, Giancarlo Ottaviano, Giacomo Contro, Giulia Tealdo, Alessandro Carli, Anna Chiara Frigo, Piero Nicolai, and Lara Alessandrini. 2020. "Prognostic Significance of CD105- and CD31-Assessed Microvessel Density in Paired Biopsies and Surgical Samples of Laryngeal Carcinoma" Cancers 12, no. 8: 2059. https://doi.org/10.3390/cancers12082059
APA StyleMarioni, G., Franz, L., Ottaviano, G., Contro, G., Tealdo, G., Carli, A., Frigo, A. C., Nicolai, P., & Alessandrini, L. (2020). Prognostic Significance of CD105- and CD31-Assessed Microvessel Density in Paired Biopsies and Surgical Samples of Laryngeal Carcinoma. Cancers, 12(8), 2059. https://doi.org/10.3390/cancers12082059