Pain Control during the Treatment of Primary Palmar Hyperhidrosis with Botulinum Toxin A by a Topical Application of Liposomal Lidocaine: Clinical Effectiveness

 , , and
, , and
Abstract
1. Introduction
2. Results
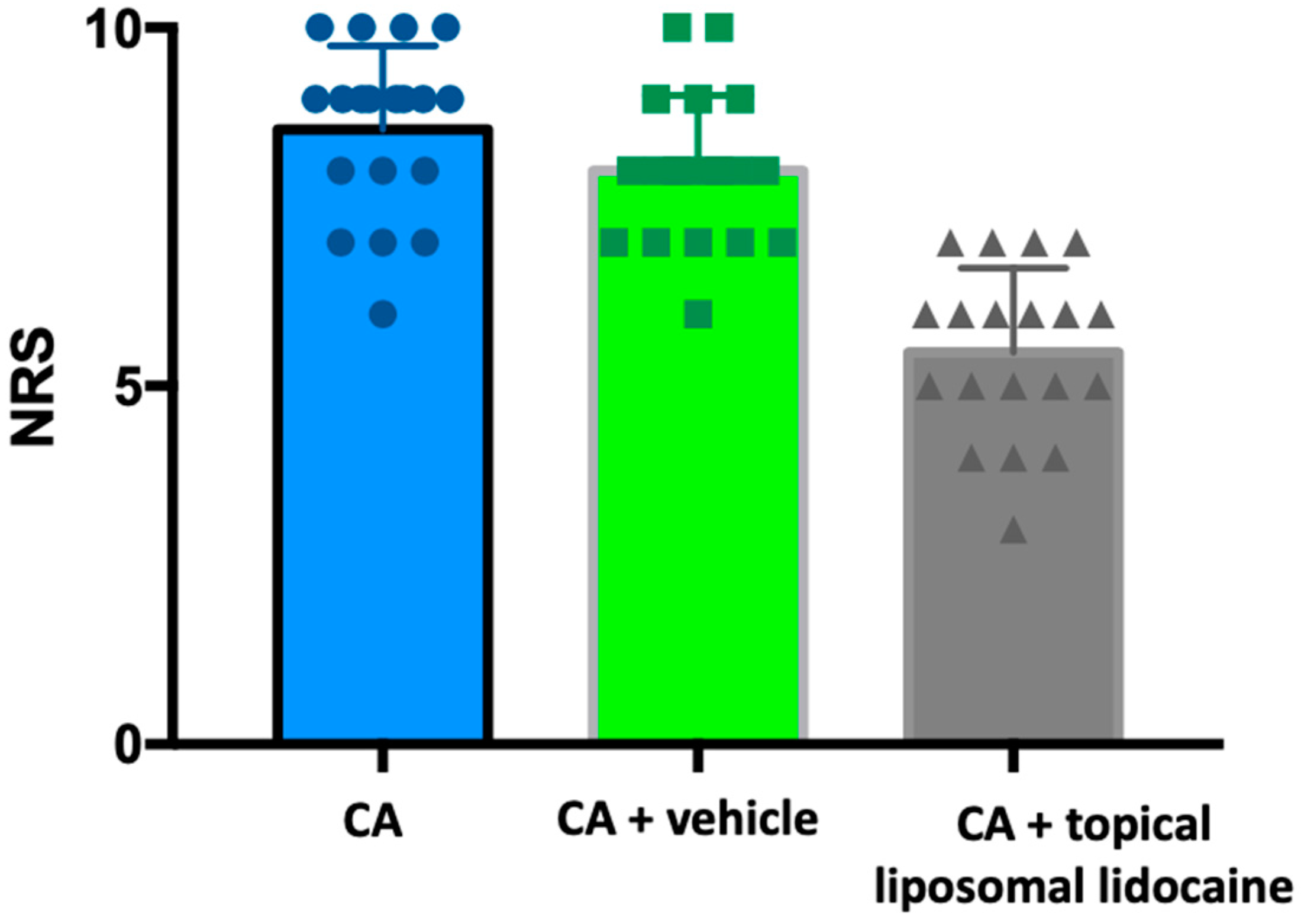
2.1. Pain Scores according to the NRS Scale
2.2. Safety Profile
3. Discussion
4. Materials and Methods
4.1. Study Design and Sample Characteristics
4.2. Botulin Toxin Type-A (BoNT-A)
4.3. Cryoanalgesia (CA)
4.4. Liposomal Lidocaine Cream
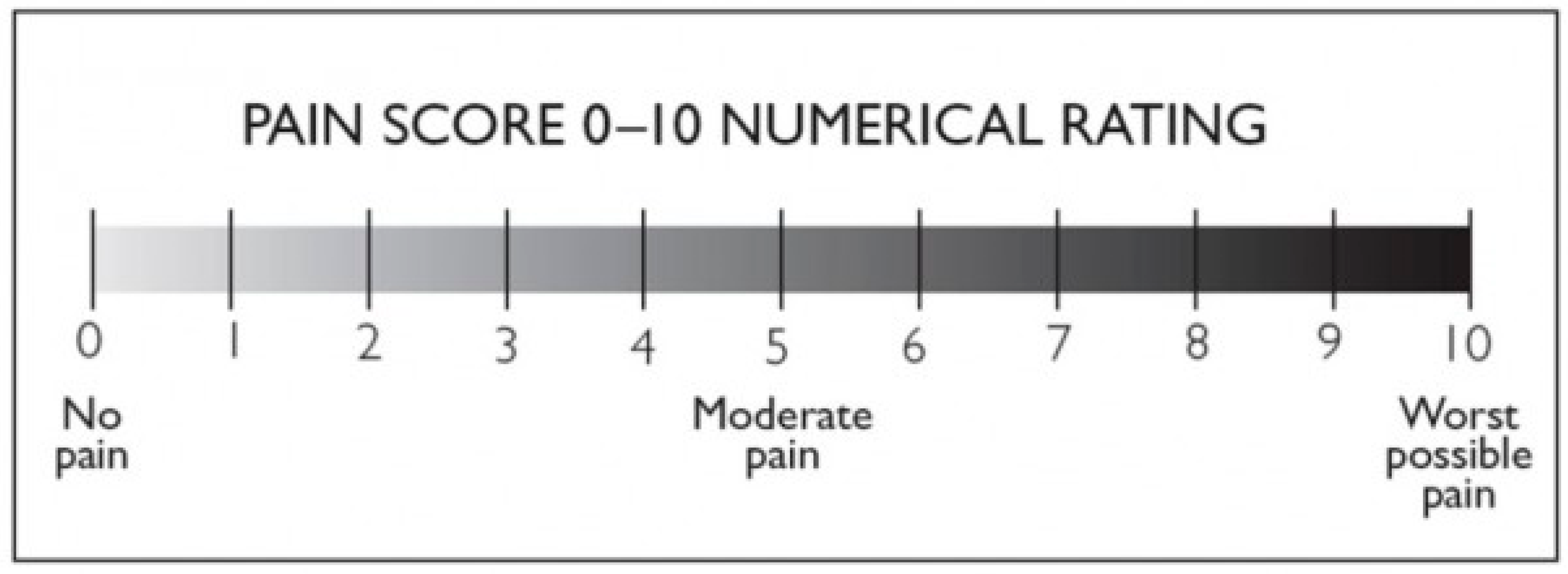
4.5. NRS Scale
4.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gregoriou, S.; Sidiropoulou, P.; Kontochristopoulos, G.; Rigopoulos, D. Management Strategies of Palmar Hyperhidrosis: Challenges and Solutions. Clin. Cosmet. Investig. Dermatol. 2019, 12, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Strutton, D.R.; Kowalski, J.W.; Glaser, D.A.; Stang, P.E. US prevalence of hyperhidrosis and impact on individuals with axillary hyperhidrosis: Results from a national survey. J. Am. Acad. Dermatol. 2004, 51, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Romero, F.R.; Haddad, G.R.; Miot, H.A.; Cataneo, D.C. Palmar hyperhidrosis: Clinical, pathophysiological, diagnostic and therapeutic aspects. An. Bras. Dermatol. 2016, 91, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Nawrocki, S.; Cha, J. The etiology, diagnosis, and management of hyperhidrosis: A comprehensive review: Etiology and clinical work-up. J. Am. Acad. Dermatol. 2019, 81, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.J.; Wu, J.J.; Lin, M.T. Autonomic dysfunction in palmar hyperhidrosis. J. Auton. Nerv. Syst. 1983, 8, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Birner, P.; Heinzl, H.; Schindl, M.; Pumprla, J.; Schnider, P. Cardiac autonomic function in patients suffering from primary focal hyperhidrosis. Eur. Neurol. 2000, 44, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Glaser, D.A.; Hebert, A.A.; Pariser, D.M.; Solish, N. Primary focal hyperhidrosis: Scope of the problem. Cutis 2007, 79 (Suppl. S5), 5–17. [Google Scholar]
- Ro, K.M.; Cantor, R.M.; Lange, K.L.; Ahn, S.S. Palmar hyperhidrosis: Evidence of genetic transmission. J. Vasc. Surg. 2002, 35, 382–386. [Google Scholar] [CrossRef]
- Higashimoto, I.; Yoshiura, K.; Hirakawa, N.; Higashimoto, K.; Soejima, H.; Totoki, T.; Mukai, T.; Niikawa, N. Primary palmar hyperhidrosis locus maps to 14q11.2-q13. Am. J. Med. Genet. Part A 2006, 140, 567–572. [Google Scholar] [CrossRef]
- Hasimoto, E.N.; Cataneo, D.C.; Reis, T.A.D.; Cataneo, A.J.M. Hyperhidrosis: Prevalence and impact on quality of life. J. Bras. Pneumol. 2018, 44, 292–298. [Google Scholar] [CrossRef]
- Murray, C.A.; Cohen, J.L.; Solish, N. Treatment of focal hyperhidrosis. J. Cutan. Med. Surg. 2007, 11, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Haider, A.; Solish, N. Focal hyperhidrosis: Diagnosis and management. CMAJ 2005, 172, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Vetrugno, R.; Liguori, R.; Cortelli, P.; Montagna, P. Sympathetic skin response: Basical mechanisms and clinical applications. Clin. Auton. Res. 2003, 13, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Muller, S.A.; Kierland, R.R. The use of a modified starch-iodine test for investigating local sweating responses to intradermal injection of methacholine. J. Investig. Dermatol. 1959, 32, 126–128. [Google Scholar] [CrossRef] [PubMed]
- Eisenach, J.H.; Atkinson, J.L.; Fealey, R.D. Hyperhidrosis: Evolving therapies for a well-established phenomenon. Mayo Clin. Proc. 2005, 80, 657–666. [Google Scholar] [CrossRef]
- Leung, A.K.; Chan, P.Y.; Choi, M.C. Hyperhidrosis. Int. J. Dermatol. 1999, 38, 561–567. [Google Scholar] [CrossRef]
- Lenefsky, M.; Rice, Z.P. Hyperhidrosis and its impact on those living with it. Am. J. Manag. Care 2018, 24 (Suppl. S23), S491–S495. [Google Scholar]
- Parashar, K.; Adlam, T.; Potts, G. The Impact of Hyperhidrosis on Quality of Life: A Review of the Literature. Am. J. Clin. Dermatol. 2023, 24, 187–198. [Google Scholar] [CrossRef]
- Wolosker, N.; Kauffman, P.; de Campos, J.R.M.; Faustino, C.B.; da Silva, M.F.A.; Teivelis, M.P.; Puech-Leão, P. Long-term results of the treatment of primary hyperhidrosis with oxybutynin: Follow-up of 1658 cases. Int. J. Dermatol. 2020, 59, 709–715. [Google Scholar] [CrossRef]
- Dogru, M.V.; Sezen, C.B.; Girgin, O.; Cansever, L.; Kocaturk, C.I.; Metin, M.; Dincer, S.I. Is there any relationship between quality of life and the level of sympathectomy in primary palmar hyperhidrosis? Single-center experience. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 273–279. [Google Scholar] [CrossRef]
- Wang, F.G.; Chen, Y.B.; Yang, W.T.; Shi, L. Comparison of compensatory sweating and quality of life following thoracic sympathetic block for palmar hyperhidrosis: Electrocautery hook versus titanium clip. Chin. Med. J. 2011, 124, 3495–3498. [Google Scholar] [PubMed]
- Hamm, H. Impact of hyperhidrosis on quality of life and its assessment. Dermatol. Clin. 2014, 32, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Pariser, D.M.; Ballard, A. Iontophoresis for palmar and plantar hyperhidrosis. Dermatol. Clin. 2014, 32, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Samizadeh, S.; De Boulle, K. Botulinum neurotoxin formulations: Overcoming the confusion. Clin. Cosmet. Investig. Dermatol. 2018, 11, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Hosp, C.; Hamm, H. Safety of available and emerging drug therapies for hyperhidrosis. Expert Opin. Drug Saf. 2017, 16, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Solish, N.; Bertucci, V.; Dansereau, A.; Hong, H.C.-H.; Lynde, C.; Lupin, M.; Smith, K.C.; Storwick, G. A comprehensive approach to the recognition, diagnosis, and severity-based treatment of focal hyperhidrosis: Recommendations of the Canadian Hyperhidrosis Advisory Committee. Dermatol. Surg. 2007, 33, 908–923. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Giuliodori, K.; Martina, E.; Giuliano, A.; Ganzetti, G.; Offidani, A. Onabotulinumtoxin type A (Botox®) versus Incobotulinumtoxin type A (Xeomin®) in the treatment of focal idiopathic palmar hyperhidrosis: Results of a comparative double-blind clinical trial. J. Neural Transm. 2014, 121, 21–26. [Google Scholar] [CrossRef]
- Mannava, S.; Mannava, K.A.; Nazir, O.F.; Plate, J.F.; Smith, B.P.; Koman, L.A.; Tuohy, C.J. Treatment of palmar hyperhidrosis with botulinum neurotoxin a. J. Hand Surg. 2013, 38, 398–400. [Google Scholar] [CrossRef]
- Gregoriou, S.; Rigopoulos, D.; Makris, M.; Liakou, A.; Agiosofitou, E.; Stefanaki, C.; Kontochristopoulos, G. Effects of botulinum toxin—A therapy for palmar hyperhidrosis in plantar sweat production. Dermatol. Surg. 2010, 36, 496–498. [Google Scholar] [CrossRef]
- Basciani, M.; Di Rienzo, F.; Bizzarrini, M.; Zanchi, M.; Copetti, M.; Intiso, D. Efficacy of botulinum toxin type B for the treatment of primary palmar hyperhidrosis: A prospective, open, single-blind, multi-centre study. Arch. Dermatol. Res. 2014, 306, 497–503. [Google Scholar] [CrossRef]
- Yi, K.H.; Lee, J.H.; Hu, H.; Kim, J.H.; Park, H.J.; Kim, K.B.; Kim, J.H.; Kim, H.J. Anatomical proposal of local anesthesia injection for median nerve block in treating hyperhidrosis with botulinum neurotoxin. Surg. Radiol. Anat. 2023, 45, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Benohanian, A. What stands in the way of treating palmar hyperhidrosis as effectively as axillary hyperhidrosis with botulinum toxin type A. Dermatol. Online J. 2009, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- Glaser, D.A.; Hebert, A.A.; Pariser, D.M.; Solish, N. Palmar and plantar hyperhidrosis: Best practice recommendations and special considerations. Cutis 2007, 79 (Suppl. S5), 18–28. [Google Scholar] [PubMed]
- Smith, K.C.; Comite, S.L.; Storwick, G.S. Ice minimizes discomfort associated with injection of botulinum toxin type a for the treatment of palmar and plantar hyperhidrosis. Dermatol. Surg. 2007, 33, S88–S91. [Google Scholar] [CrossRef] [PubMed]
- Hayton, M.; Stanley, J.; Lowe, N. A review of peripheral nerve blockade as local anaesthesia in the treatment of palmar hyperhidrosis. Br. J. Dermatol. 2003, 149, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Locke, M.C.; Davis, J.C.; Brothers, R.J.; Love, W.E. Assessing the outcomes, risks, and costs of local versus general anesthesia: A review with implications for cutaneous surgery. J. Am. Acad. Dermatol. 2018, 78, 983–988.e4. [Google Scholar] [CrossRef]
- Saijo, M.; Ito, E.; Ichinohe, T.; Kaneko, Y. Lack of pain reduction by a vibrating local anesthetic attachment: A pilot study. Anesth. Prog. 2005, 52, 62–64. [Google Scholar] [CrossRef]
- Vadoud-Seyedi, J. Treatment of plantar hyperhidrosis with botulinum toxin type A. Int. J. Dermatol. 2004, 43, 969–971. [Google Scholar] [CrossRef]
- Naumann, M.; Bergmann, I.; Hofmann, U.; Hamm, H.; Reiners, K. Botulinum toxin for focal hyperhidrosis: Technical considerations and improvements in application. Br. J. Dermatol. 1998, 139, 1123–1124. [Google Scholar] [CrossRef]
- Iannitti, T.; Di Cerbo, A.; Aspiro, A.; Palmieri, B. A preliminary study of painless and effective transdermal botulinum toxin A delivery by jet nebulization for treatment of primary hyperhidrosis. Drug Des. Devel. Ther. 2014, 8, 931–935. [Google Scholar] [CrossRef]
- Kontochristopoulos, G.; Gregoriou, S.; Zakopoulou, N.; Rigopoulos, D. Letter: Cryoanalgesia with Dichlorotetrafluoroethane Spray Versus Ice Packs in Patients Treated with Botulinum Toxin-A for Palmar Hyperhidrosis: Self-Controlled Study. Dermatol. Surg. 2006, 32, 873–874. [Google Scholar] [CrossRef]
- Lim, E.C.; Seet, R.C. Another Injection-free method to effect analgesia when injecting botulinum toxin for palmar hyperhidrosis: Cryoanalgesia. Dermatol. Online J. 2007, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.C.; Seet, R.C. Physician, treat thyself. BMJ 2006, 332, 1323. [Google Scholar] [CrossRef]
- Alsantali, A. A comparative trial of ice application versus EMLA cream in alleviation of pain during botulinum toxin injections for palmar hyperhidrosis. Clin. Cosmet. Investig. Dermatol. 2018, 11, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Söylev, M.F.; Koçak, N.; Kuvaki, B.; Özkan, S.B.; Kir, E. Anesthesia with EMLA cream for botulinum A toxin injection into eyelids. Ophthalmologica 2002, 216, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.L. Pain management with a topical lidocaine and tetracaine 7%/7% cream with laser dermatologic procedures. J. Drugs Dermatol. 2013, 12, 986–989. [Google Scholar] [PubMed]
- Greveling, K.; Prens, E.P.; Ten Bosch, N.; van Doorn, M.B. Comparison of lidocaine/tetracaine cream and lidocaine/prilocaine cream for local anaesthesia during laser treatment of acne keloidalis nuchae and tattoo removal: Results of two randomized controlled trials. Br. J. Dermatol. 2017, 176, 81–86. [Google Scholar] [CrossRef]
- Menter, A.; Black-Noller, G.; Riendeau, L.A.; Monti, K.L. The use of EMLA cream and 1% lidocaine infiltration in men for relief of pain associated with the removal of genital warts by cryotherapy. J. Am. Acad. Dermatol. 1997, 37, 96–100. [Google Scholar] [CrossRef]
- Bucalo, B.D.; Mirikitani, E.J.; Moy, R.L. Comparison of skin anesthetic effect of liposomal lidocaine, nonliposomal lidocaine, and EMLA using 30-minute application time. Dermatol. Surg. 1998, 24, 537–541. [Google Scholar] [CrossRef]
- Junputipong, N.; Rojhirunsakool, S.; Deewongkij, P.; Kamanamool, N.; Udompataikul, M. Comparison of the onset, depth, and duration of cutaneous anesthesia between topical 10% lidocaine and EMLA creams: A randomized, intraindividual, comparative trial. J. Dermatol. Treat. 2022, 33, 3047–3052. [Google Scholar] [CrossRef]
- Patel, R.; Halem, M.; Zaiac, M. The combined use of forced cold air and topical anesthetic cream for analgesia during the treatment of palmar hyperhydrosis with botulinum toxin injections. J. Drugs Dermatol. 2009, 8, 948–951. [Google Scholar] [PubMed]
- Martina, E.; Diotallevi, F.; Radi, G.; Campanati, A.; Offidani, A. Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review. Toxins 2021, 13, 120. [Google Scholar] [CrossRef] [PubMed]
- Moorjani, N.; Zhao, F.; Tian, Y.; Liang, C.; Kaluba, J.; Maiwand, M.O. Effects of cryoanalgesia on post-thoracotomy pain and on the structure of intercostal nerves: A human prospectiverandomized trial and a histological study. Eur. J. Cardiothorac. Surg. 2001, 20, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Filippiadis, D.; Efthymiou, E.; Tsochatzis, A.; Kelekis, A.; Prologo, J. Percutaneous cryoanalgesia for pain palliation: Current status and future trends. Diagn. Interv. Imaging 2021, 102, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Ernst, E.; Fialka, V. Ice freezes pain? A review of the clinical effectiveness of analgesic cold therapy. J. Pain Symptom Manage. 1994, 9, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, H.; Hollmann, M.W.; Stevens, M.F.; Lirk, P.; Brandenburger, T.; Piegeler, T.; Werdehausen, R. Molecular mechanisms of action of systemic lidocaine in acute and chronic pain: A narrative review. Br. J. Anaesth. 2019, 123, 335–349. [Google Scholar] [CrossRef]
- ASENSIL (lidocaine) [Prescribing Information]. Available online: https://farmaci.agenziafarmaco.gov.it/aifa/servlet/PdfDownloadServlet?pdfFileName=footer_003674_043742_RCP.pdf&sys=m0b1l3 (accessed on 15 July 2022).
- Childs, J.D.; Piva, S.R.; Fritz, J.M. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine 2005, 30, 1331–1334. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthr. Care Res. 2011, 63 (Suppl. S11), S240–S252. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Values | CA | CA+Vehicle | CA+Topical Liposomial Lidocaine |
|---|---|---|---|
| Number of values | 19 | 19 | 19 |
| Minimum | 6 | 6 | 3 |
| 25% percentile | 8 | 7 | 5 |
| Median | 9 | 8 | 6 |
| 75% percentile | 9 | 9 | 6 |
| Maximum | 10 | 10 | 7 |
| Mean | 8.579 | 8 | 5.474 |
| Std Deviation | 1.17 | 1.054 | 1.172 |
| Std. Error of Mean | 0.2684 | 0.2418 | 0.2689 |
| Lower 95% CI | 8.015 | 7.492 | 4.909 |
| Upper 95% CI | 9.143 | 8.508 | 6.039 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marani, A.; Gioacchini, H.; Paolinelli, M.; Bobyr, I.; Martina, E.; Radi, G.; Diotalallevi, F.; Campanati, A. Pain Control during the Treatment of Primary Palmar Hyperhidrosis with Botulinum Toxin A by a Topical Application of Liposomal Lidocaine: Clinical Effectiveness. Toxins 2024, 16, 28. https://doi.org/10.3390/toxins16010028
Marani A, Gioacchini H, Paolinelli M, Bobyr I, Martina E, Radi G, Diotalallevi F, Campanati A. Pain Control during the Treatment of Primary Palmar Hyperhidrosis with Botulinum Toxin A by a Topical Application of Liposomal Lidocaine: Clinical Effectiveness. Toxins. 2024; 16(1):28. https://doi.org/10.3390/toxins16010028
Chicago/Turabian StyleMarani, Andrea, Helena Gioacchini, Matteo Paolinelli, Ivan Bobyr, Emanuela Martina, Giulia Radi, Federico Diotalallevi, and Anna Campanati. 2024. "Pain Control during the Treatment of Primary Palmar Hyperhidrosis with Botulinum Toxin A by a Topical Application of Liposomal Lidocaine: Clinical Effectiveness" Toxins 16, no. 1: 28. https://doi.org/10.3390/toxins16010028
APA StyleMarani, A., Gioacchini, H., Paolinelli, M., Bobyr, I., Martina, E., Radi, G., Diotalallevi, F., & Campanati, A. (2024). Pain Control during the Treatment of Primary Palmar Hyperhidrosis with Botulinum Toxin A by a Topical Application of Liposomal Lidocaine: Clinical Effectiveness. Toxins, 16(1), 28. https://doi.org/10.3390/toxins16010028