Clinical Efficacy and Safety of Sodium Thiosulfate in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials

Abstract
:1. Introduction
2. Results
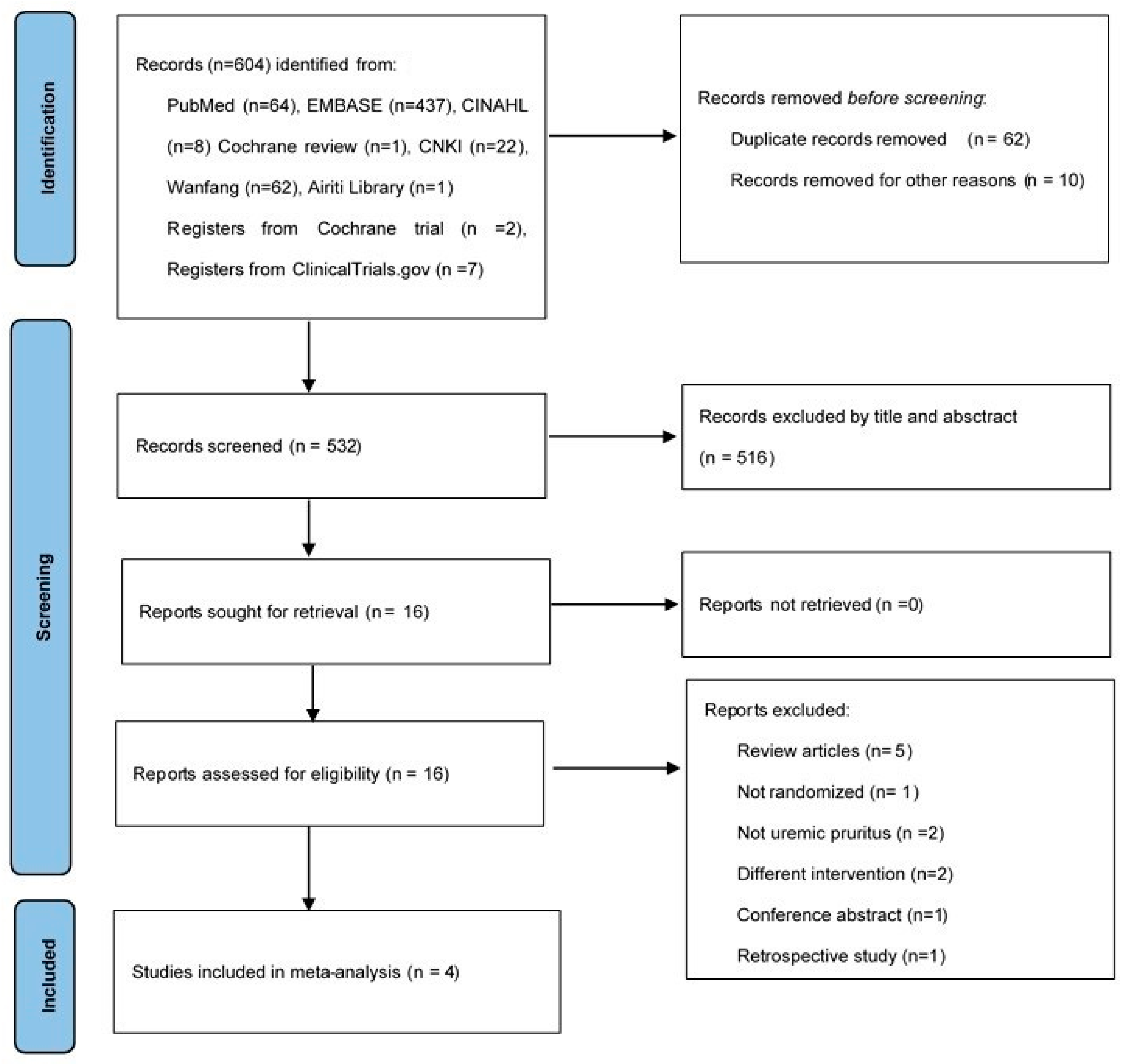
2.1. Study Characteristics
2.2. Outcomes
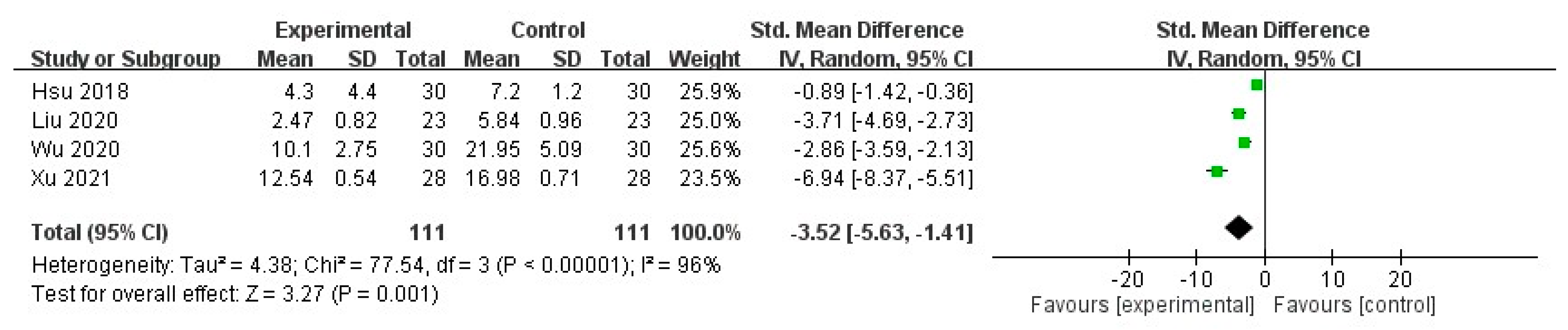
2.2.1. Pruritus Score
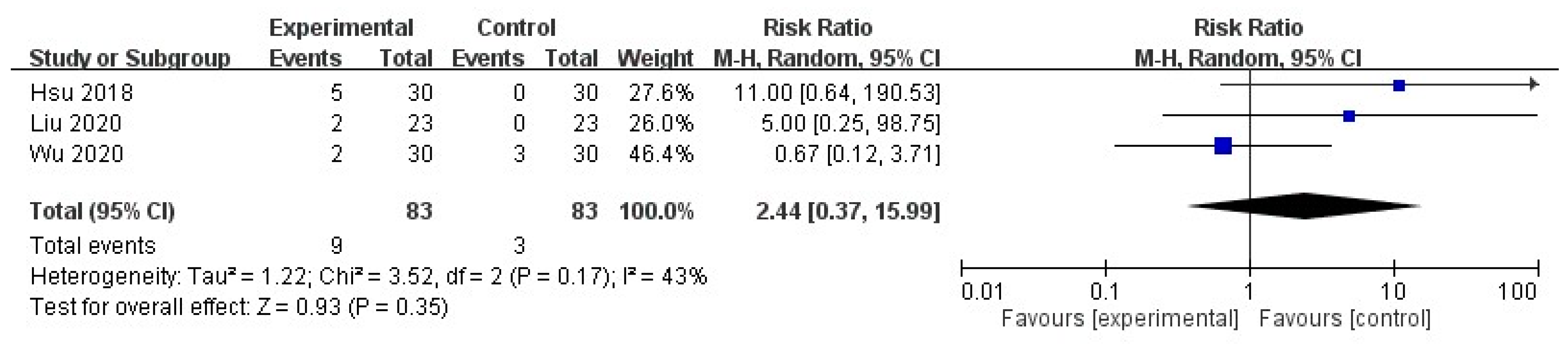
2.2.2. Adverse Drug Reaction
2.2.3. Laboratory Parameters
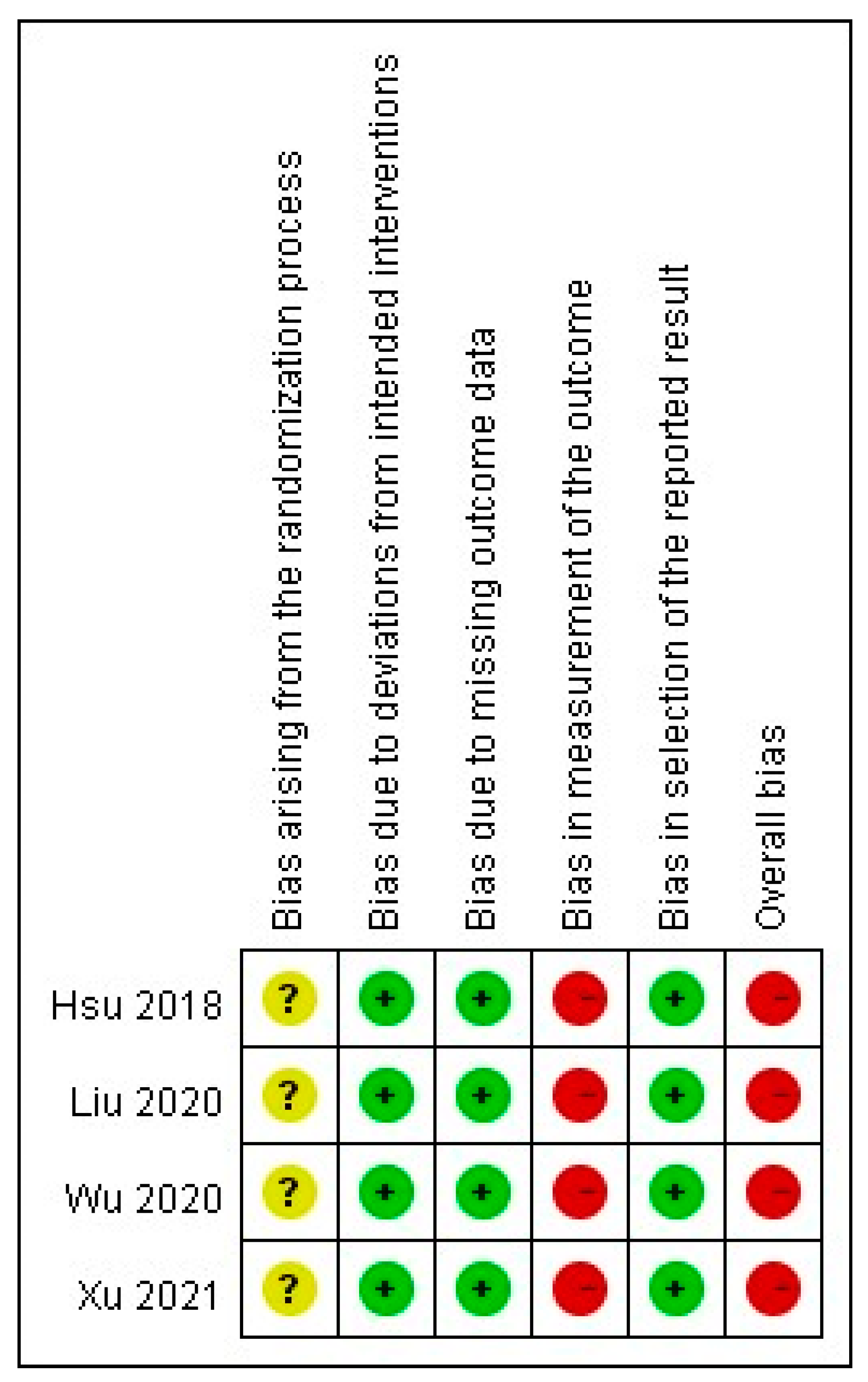
2.3. Quality of Evidence
3. Discussion
3.1. Summary of the Meta-Analysis
3.2. UP Treatment
3.3. Laboratory Parameters in UP Patient
3.4. Adverse Drug Reaction
3.5. Heterogeneity
3.5.1. Dosage of STS
3.5.2. Outcome Measurements
3.5.3. Patient Selection
3.5.4. Intervention
3.6. Limitations
4. Conclusions
5. Materials and Methods
5.1. Literature Search
5.2. Study Selection
5.3. Data Extraction and Quality Assessment
5.4. Data Synthesis and Analysis
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Effective Rate | ADR | Alb (g/L) | Calcium (mmol/L) | Phosphorus (mmol/L) | Scr (μmol/L) | BUN (mmol/L) | PTH (pg/mL) | PSQI | WHOQOL- 100 | CRP | Ferritin |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hsu et al. 2018 | -- | 5/30 0/30 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| Wu et al. 2020 | 29/30 19/30 | 2/30 3/30 | T:25.3 (1.50) →28.2 (0.92) C:28.4 (0.69) →30.1 (0.52) | -- | -- | -- | -- | -- | T:18.25 (2.30)→3.41 (0.83) C:17.96 (1.90)→8.38 (1.63) | -- | T:8.20 (0.59) →6.30 (0.35) C:9.20 (0.87) →7.60 (0.42) | T:509.30 (13.55)→486.52 (10.31) C:508.77 (11.59)→489.42 (8.59) |
| Liu et al. 2020 | 21/23 8/23 | 2/23 0/23 | -- | T: 1.9 (1.0) C:1.9 (0.4) | T: 2.2 (0.4) C: 2.1 (0.4) | T: 547.9 (29.3) C: 512.3 (19.4) | T: 13.3 (1.0) C: 12.5 (3.5) | T: 241.4 (32.2) C: 231.3 (29.8) | -- | -- | -- | -- |
| Xu et al. 2021 | -- | -- | T:28.69 (0.84)→20.29 (0.41) C:28.70 (0.85)→24.37 (0.52) | T:2.52 (0.35) →1.88 (0.41) C:2.55 (0.33 )→2.2 4(0.68) | T:2.56 (0.21) →1.95 (0.17) C:2.55 (0.23) →2.30 (0.20) | T:788.97 (22.59)→502.53 (16.38) C:789.01 (22.61)→664.35 (19.81) | T:26.34 (1.50)→14.68 (0.56) C:26.35 (1.52)→20.19 (0.97) | T:300.36 (15.37)→203.25 (9.81) C:300.31 (15.32)→256.58 (13.42) | T:14.35 (2.34)→5.61 (0.37) C:14.36 (2.33)→10.28 (0.52) | T: 56.38 (6.17) →83.59 (2.24) C:56.39 (6.20)→71.36 (3.55) | -- | -- |
References
- Hu, X.; Sang, Y.; Yang, M.; Chen, X.; Tang, W. Prevalence of chronic kidney disease-associated pruritus among adult dialysis patients: A meta-analysis of cross-sectional studies. Medicine (Baltimore) 2018, 97, e10633. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.H.; Keng, J.L.; Kuo, K.L.; Wang, Y.F.; Tai, Y.C.; Kuo, C.Y. An Apriori Algorithm-Based Association Rule Analysis to Identify Herb Combinations for Treating Uremic Pruritus Using Chinese Herbal Bath Therapy. Evid. Based Complement. Alternat. Med. 2020, 2020, 8854772. [Google Scholar] [CrossRef]
- Verduzco, H.A.; Shirazian, S. CKD-Associated Pruritus: New Insights into Diagnosis, Pathogenesis, and Management. Kidney Int. Rep. 2020, 5, 1387–1402. [Google Scholar] [CrossRef] [PubMed]
- Eusebio-Alpapara, K.M.V.; Castillo, R.L.; Dofitas, B.L. Gabapentin for uremic pruritus: A systematic review of randomized controlled trials. Int. J. Dermatol. 2020, 59, 412–422. [Google Scholar] [CrossRef]
- Wikström, B.; Gellert, R.; Ladefoged, S.D.; Danda, Y.; Akai, M.; Ide, K.; Ogasawara, M.; Kawashima, Y.; Ueno, K.; Mori, A.; et al. Kappa-opioid system in uremic pruritus: Multicenter, randomized, double-blind, placebo-controlled clinical studies. J. Am. Soc. Nephrol. 2005, 16, 3742–3747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, P.H. Western and complementary alternative medicine treatment of uremic pruritus: A literature review. Tzu Chi Med. J. 2020, 33, 350–358. [Google Scholar]
- Ozen, N.; Cinar, F.I.; Askin, D.; Mut, D. Uremic pruritus and associated factors in hemodialysis patients: A multi-center study. Kidney Res. Clin. Pract. 2018, 37, 138–147. [Google Scholar] [CrossRef] [Green Version]
- Rayner, H.C.; Larkina, M.; Wang, M.; Graham-Brown, M.; van der Veer, S.N.; Ecder, T.; Hasegawa, T.; Kleophas, W.; Bieber, B.A.; Tentori, F.; et al. International Comparisons of Prevalence, Awareness, and Treatment of Pruritus in People on Hemodialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 2000–2007. [Google Scholar] [CrossRef] [Green Version]
- Brock, P.R.; Maibach, R.; Childs, M.; Rajput, K.; Roebuck, D.; Sullivan, M.J.; Laithier, V.; Ronghe, M.; Dall'Igna, P.; Hiyama, E.; et al. Sodium Thiosulfate for Protection from Cisplatin-Induced Hearing Loss. N. Engl. J. Med. 2018, 378, 2376–2385. [Google Scholar] [CrossRef] [Green Version]
- Djuric, P.; Dimkovic, N.; Schlieper, G.; Djuric, Z.; Pantelic, M.; Mitrovic, M.; Jankovic, A.; Milanov, M.; Kuzmanovic Pficer, J.; Floege, J. Sodium thiosulphate and progression of vascular calcification in end-stage renal disease patients: A double-blind, randomized, placebo-controlled study. Nephrol. Dial. Transplant. 2020, 35, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Nigwekar, S.U.; Thadhani, R.; Brandenburg, V.M. Calciphylaxis. N. Engl. J. Med. 2018, 378, 1704–1714. [Google Scholar] [CrossRef] [PubMed]
- Peng, T.; Zhuo, L.; Wang, Y.; Jun, M.; Li, G.; Wang, L.; Hong, D. Systematic review of sodium thiosulfate in treating calciphylaxis in chronic kidney disease patients. Nephrology (Carlton) 2018, 23, 669–675. [Google Scholar] [CrossRef]
- Saengpanit, D.; Chattranukulchai, P.; Tumkosit, M.; Siribumrungwong, M.; Katavetin, P.; Sitprija, V.; Praditpornsilpa, K.; Eiam-Ong, S.; Susantitaphong, P. Effect of Sodium Thiosulfate on Arterial Stiffness in End-Stage Renal Disease Patients Undergoing Chronic Hemodialysis (Sodium Thiosulfate-Hemodialysis Study): A Randomized Controlled Trial. Nephron 2018, 139, 219–227. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Kongnatthasate, K.; Praditpornsilpa, K.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Treatment of Calciphylaxis in CKD: A Systematic Review and Meta-analysis. Kidney Int. Rep. 2019, 4, 231–244. [Google Scholar] [CrossRef] [Green Version]
- van As, J.W.; van den Berg, H.; van Dalen, E.C. Medical interventions for the prevention of platinum-induced hearing loss in children with cancer. Cochrane Database Syst. Rev. 2019, 5, Cd009219. [Google Scholar] [CrossRef]
- Song, Y.H.; Wang, S.Y.; Lang, J.H.; Xiao, Y.F.; Cai, G.Y.; Chen, X.M. Therapeutic effect of intravenous sodium thiosulfate for uremic pruritus in hemodialysis patients. Ren. Fail. 2020, 42, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Brewster, U.C. Dermatological Disease in Patients With CKD. Am. J. Kidney Dis. 2008, 51, 331–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuypers, D.R. Skin problems in chronic kidney disease. Nat. Clin. Pract. Nephrol. 2009, 5, 157–170. [Google Scholar] [CrossRef]
- Chaturvedy, M. Dermatological problems in CKD; ocular manifestations in CKD. Clin. Queries Nephrol. 2012, 1, 284–290. [Google Scholar] [CrossRef]
- Robles-Mendez, J.C.; Vazquez-Martinez, O.; Ocampo-Candiani, J. Skin manifestations of chronic kidney disease. Actas Dermosifiliogr. 2015, 106, 609–622. [Google Scholar] [CrossRef]
- Hercz, D.; Jiang, S.H.; Webster, A.C. Interventions for itch in people with advanced chronic kidney disease. Cochrane Database Syst. Rev. 2020, 12, CD011393. [Google Scholar] [CrossRef]
- Xuan, X.Y.; Li, J.F.; Liang, Z.A.; Chen, X.L.; Zhou, S.; Yang, A.C.; Ma, C.C. Sodium thiosulfate in the treatment of skin itching in maintenance hemodialysis patients. Heilong Med. J. 2019, 43, 474–475. [Google Scholar]
- Cen, Y. Experience of application of Sodium thiosulfate. J. Zhangjiakou Med. Coll. 1995, 02, 22. [Google Scholar]
- Sprague, S.M. Painful skin ulcers in a hemodialysis patient. Clin. J. Am. Soc. Nephrol. 2014, 9, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Ou, B.S.; Liu, W.B.; Li, M.L. Combined compound Zaoren capsule and intravenous Sodium thiosulfate in treatment of senile pruritus. Pract. J. Med. Pharm. 2006, 01, 80. [Google Scholar]
- Gao, F.; Li, Y.Y. Observation on clinical effect of oral Chinese medicine in the treatment of pruritus of senile patients with skin cancer. In Proceedings of the Combination of Traditional and Western Medicine Dermatology Conference, Hangzhou, China, 4–8 September 2003; p. 1. [Google Scholar]
- Mohamed, W.; Zaki, F.M.K.; Bekhit, W.H.M.; Sherif, I.S. Sodium thiosulfate (STS): A new option for hemodialysis patients with uremic pruritus. Nephrol. Dial. Transplant. 2012, 27, ii511–ii512. [Google Scholar] [CrossRef]
- Hsu, Y.S.; Zhao, J. Observation on curative effect of sodium thiosulfate in the treatment of skin itch in uremic patients. Yiyao Qianyan 2018, 8, 170. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, B.; Liu, L.F.; Hu, P.P.; Yang, T. Clinical effect of sodium thiosulfate in hemodialysis patients with refractory skin itch. J. Clin. Nephrol. 2020, 20, 194–197. [Google Scholar] [CrossRef]
- Wu, H.; Xiao, Y.F. Clinical observation of sodium thiosulfate in the treatment of intractable uremic pruritus. Chin. J. Blood Purif. 2020, 19, 92–94, 102. [Google Scholar] [CrossRef]
- Xu, P.X.; Xie, J.L. Effect of Sodium Thiosulfate on Skin Pruritus in Uremic Hemodialysis Patients. Smart Healthc. 2021, 7, 136–138. [Google Scholar]
- Rehman, I.U.; Munib, S.; Ramadas, A.; Khan, T.M. Prevalence of chronic kidney disease-associated pruritus, and association with sleep quality among hemodialysis patients in Pakistan. PLoS ONE 2018, 13, e0207758. [Google Scholar] [CrossRef] [PubMed]
- Legroux-Crespel, E.; Clèdes, J.; Misery, L. A comparative study on the effects of naltrexone and loratadine on uremic pruritus. Dermatology 2004, 208, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Badiee Aval, S.; Ravanshad, Y.; Azarfar, A.; Mehrad-Majd, H.; Torabi, S.; Ravanshad, S. A Systematic Review and Meta-analysis of Using Acupuncture and Acupressure for Uremic Pruritus. Iran. J. Kidney Dis. 2018, 12, 78–83. [Google Scholar] [PubMed]
- Xue, W.; Zhao, Y.; Yuan, M.; Zhao, Z. Chinese herbal bath therapy for the treatment of uremic pruritus: Meta-analysis of randomized controlled trials. BMC Complement. Altern. Med. 2019, 19, 103. [Google Scholar] [CrossRef]
- Altınok Ersoy, N.; Akyar, İ. Multidimensional pruritus assessment in hemodialysis patients. BMC Nephrol. 2019, 20, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narita, I.; Alchi, B.; Omori, K.; Sato, F.; Ajiro, J.; Saga, D.; Kondo, D.; Skatsume, M.; Maruyama, S.; Kazama, J.J.; et al. Etiology and prognostic significance of severe uremic pruritus in chronic hemodialysis patients. Kidney Int. 2006, 69, 1626–1632. [Google Scholar] [CrossRef] [Green Version]
- Pisoni, R.L.; Wikström, B.; Elder, S.J.; Akizawa, T.; Asano, Y.; Keen, M.L.; Saran, R.; Mendelssohn, D.C.; Young, E.W.; Port, F.K. Pruritus in haemodialysis patients: International results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transplant. 2006, 21, 3495–3505. [Google Scholar] [CrossRef] [Green Version]
- Ramakrishnan, K.; Bond, T.C.; Claxton, A.; Sood, V.C.; Kootsikas, M.; Agnese, W.; Sibbel, S. Clinical characteristics and outcomes of end-stage renal disease patients with self-reported pruritus symptoms. Int. J. Nephrol. Renovasc. Dis. 2013, 7, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimata, N.; Fuller, D.S.; Saito, A.; Akizawa, T.; Fukuhara, S.; Pisoni, R.L.; Robinson, B.M.; Akiba, T. Pruritus in hemodialysis patients: Results from the Japanese Dialysis Outcomes and Practice Patterns Study (JDOPPS). Hemodial. Int. 2014, 18, 657–667. [Google Scholar] [CrossRef]
- Yu, Z.; Gu, L.; Pang, H.; Fang, Y.; Yan, H.; Fang, W. Sodium thiosulfate: An emerging treatment for calciphylaxis in dialysis patients. Case Rep. Nephrol. Dial. 2015, 5, 77–82. [Google Scholar] [CrossRef]
- Yerram, P.; Saab, G.; Karuparthi, P.R.; Hayden, M.R.; Khanna, R. Nephrogenic systemic fibrosis: A mysterious disease in patients with renal failure—Role of gadolinium-based contrast media in causation and the beneficial effect of intravenous sodium thiosulfate. Clin. J. Am. Soc. Nephrol. 2007, 2, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.W.; Chen, H.C.; Chou, C.Y.; Yen, H.R.; Li, T.C.; Sun, M.F.; Chang, H.H.; Huang, C.C.; Tsai, F.J.; Tschen, J.; et al. Transformation of 5-D itch scale and numerical rating scale in chronic hemodialysis patients. BMC Nephrol. 2017, 18, 56. [Google Scholar] [CrossRef] [Green Version]
- Park, S.Y.; Park, E.J.; Suh, H.S.; Ha, D.; Lee, E.K. Development of a transformation model to derive general population-based utility: Mapping the pruritus-visual analog scale (VAS) to the EQ-5D utility. J. Eval. Clin. Pract. 2017, 23, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.; Kuah, C.Y.; Martin-Lopez, J.E.; Chua, S.; Shpadaruk, V.; Sanclemente, G.; Franco, J.V. Interventions for chronic pruritus of unknown origin. Cochrane Database Syst. Rev. 2020, 1, Cd013128. [Google Scholar] [CrossRef] [PubMed]
- McMaster University. GRADEpro GDT: GRADEpro Guideline Development Tool [Software] (Developed by Evidence Prime, Inc.). 2020. Available online: gradepro.org (accessed on 3 July 2021).




| Study (Year) | Study Design | Inclusion Criteria | Previous Treatment | No. of Patients | Age (Years) | STS Dosage, Route, and Frequency | Combination Therapy | Duration | Pruritus Severity Assessment | Pruritus Score (before→after) | Effective Rate | ADR |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hsu et al. 2018 | RCT | HD | LC | T:30 | T:57.1 ± 5.2 | 25 g/100 mL NS, i.v., 2~3 times/w | - | 8W | mDuo | T: 19.0(8.3)→4.3(4.4) | - | 5/30 |
| C:30 | C:56.2 ± 5.6 | C: 18.5(7.7)→7.2(1.2) | 0/30 | |||||||||
| Liu et al. 2020 | RCT | HD | TE CHT AC AH | T:23 | T:67.0 ± 10.4 | 3.84 g/20 mL NS i.v., 3 times/w | TE CHT AC AH | 8W | VAS | T: 9.12(0.34)→2.47(0.82) | 21/23 | 2/23 |
| C:23 | C:65.5 ± 13.5 | C: 9.23(0.16)→5.84(0.96) | 8/23 | 0/23 | ||||||||
| Wu et al. 2020 | RCT | HD | TE | T:30 | T:48.14 ±10.58 | 3.2~5.76 g/20 mL NS i.v., 3 times/w | AH | 3M | mDuo | T: 30.80(7.33)→10.10(2.75) | 29/30 | 2/30 |
| C:30 | C:51.22 ± 10.21 | C: 31.34(8.40)→21.95(5.09) | 19/30 | 3/30 | ||||||||
| Xu et al. 2021 | RCT | HD | LC | T:28 | 51.21 ± 4.90 | 0.64 g/20 mL NS i.v., 1~3 times/w | - | 3M | DRKS | T: 20.36(1.63)→12.54(0.54) | - | - |
| C:28 | C: 20.35(1.60)→16.98(0.71) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, P.-H.; Chuo, H.-E.; Kuo, K.-L.; Liao, J.-F.; Lu, P.-H. Clinical Efficacy and Safety of Sodium Thiosulfate in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials. Toxins 2021, 13, 769. https://doi.org/10.3390/toxins13110769
Lu P-H, Chuo H-E, Kuo K-L, Liao J-F, Lu P-H. Clinical Efficacy and Safety of Sodium Thiosulfate in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials. Toxins. 2021; 13(11):769. https://doi.org/10.3390/toxins13110769
Chicago/Turabian StyleLu, Ping-Hsun, Hui-En Chuo, Ko-Lin Kuo, Jian-Fu Liao, and Po-Hsuan Lu. 2021. "Clinical Efficacy and Safety of Sodium Thiosulfate in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials" Toxins 13, no. 11: 769. https://doi.org/10.3390/toxins13110769
APA StyleLu, P.-H., Chuo, H.-E., Kuo, K.-L., Liao, J.-F., & Lu, P.-H. (2021). Clinical Efficacy and Safety of Sodium Thiosulfate in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials. Toxins, 13(11), 769. https://doi.org/10.3390/toxins13110769