Maternal Dietary Patterns and Gestational Diabetes Mellitus in a Multi-Ethnic Asian Cohort: The GUSTO Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
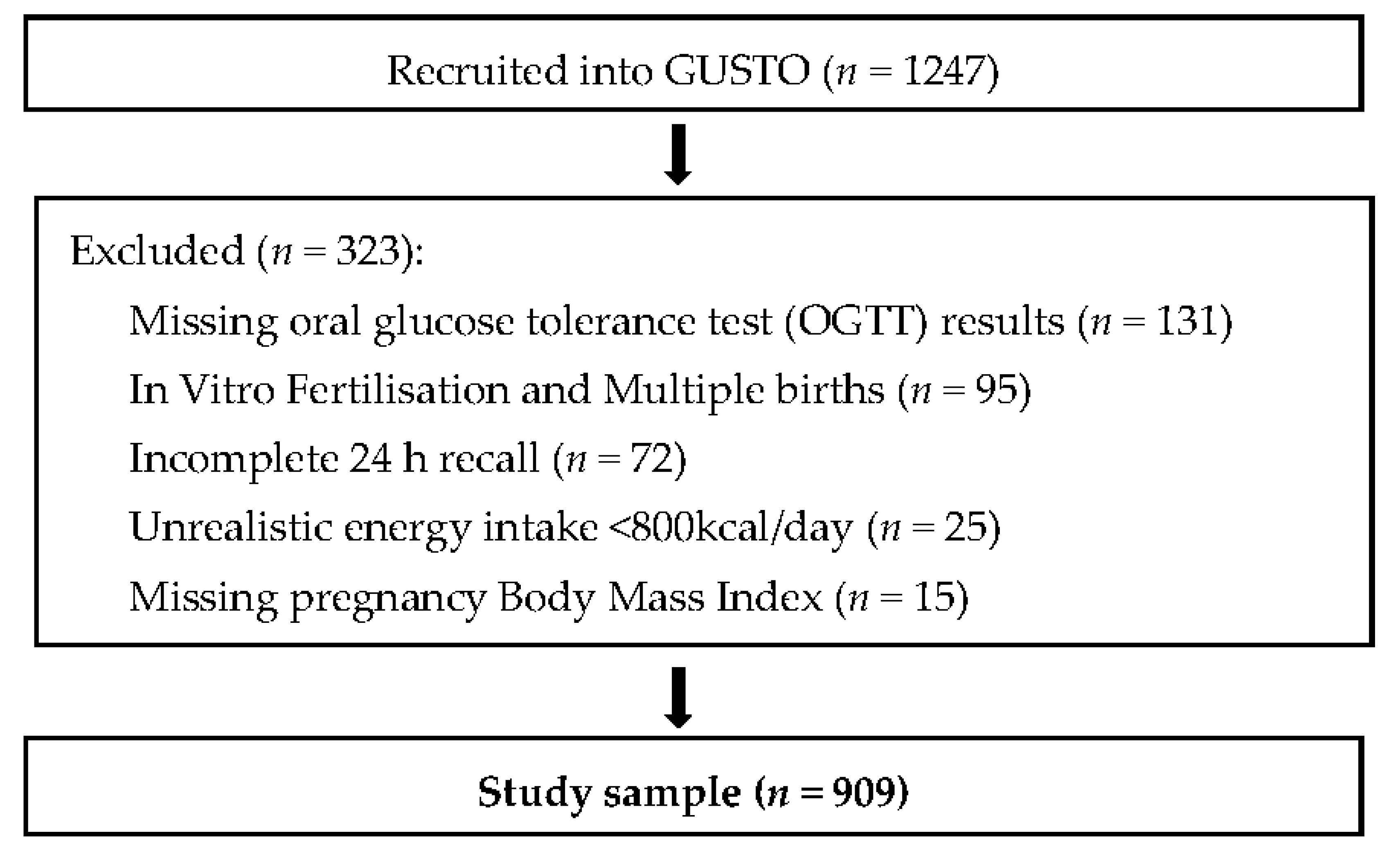
2.1. Growing up in Singapore towards Healthy Outcomes (GUSTO) Study
2.2. Maternal Dietary Assessment
2.3. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Dietary Patterns
3.2.1. Validation of Dietary Patterns
3.3. Dietary Patterns and Gestational Diabetes Mellitus
3.4. Nutrient Composition Comparison between Quintiles of Seafood-Noodle-Based-Diet Consumption
3.5. Dietary Patterns and Linear Association with Blood Glucose Levels Following OGTT
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Metzger, B.E.; Coustan, D.R. Summary and recommendations of the fourth international workshop-conference on gestational diabetes mellitus. The Organizing Committee. Diabetes Care 1998, 21, B161–B167. [Google Scholar] [PubMed]
- Yogeva, Y.; Visser, G. Obesity, gestational diabetes and pregnancy outcome. Semin. Fetal Neonatal Med. 2009, 14, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.; Ehrlich, S.; Sridhar, S.; Darbinian, J.; Moore, S.; Ferrara, A. Racial/ethnic disparities in the prevalence of gestational diabetes mellitus by BMI. Diabetes Care 2012, 35, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- Makgoba, M.; Savvidou, M.D.; Steer, P.J. An analysis of the interrelationship between maternal age, body mass index and racial origin in the development of gestational diabetes mellitus. BJOG 2012, 119, 276–282. [Google Scholar] [CrossRef] [PubMed]
- DeSisto, C.L.; Kim, S.Y.; Sharma, A.J. Prevalence estimates of gestational diabetes mellitus in the United States, pregnancy risk assessment monitoring system (PRAMS), 2007–2010. Prev. Chronic Dis. 2014, 11, 130415. [Google Scholar] [CrossRef] [PubMed]
- Seshiah, V.; Balaji, V.; Balaji, M.S.; Sanjeevi, C.B.; Green, A. Gestational diabetes mellitus in India. J. Assoc. Physicians India 2004, 52, 707–711. [Google Scholar] [PubMed]
- Bellamy, L.; Casas, J.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Boney, C.M.; Verma, A.; Tucker, R.; Vohr, B.R. Metabolic syndrome in childhood: Association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 2005, 115, e290–e296. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.M.; Lucas, M.J.; McIntire, D.D.; Leveno, K.J. Pregnancy outcomes in women with gestational diabetes compared with the general obstetric population. Obstet. Gynecol. 1997, 90, 869–873. [Google Scholar] [CrossRef]
- Hedderson, M.M.; Ferrara, A.; Sacks, D.A. Gestational diabetes mellitus and lesser degrees of pregnancy hyperglycemia: Association with increased risk of spontaneous preterm birth. Obstet. Gynecol. 2003, 102, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Langer, O.; Yogev, Y.; Most, O.; Xenakis, E.M. Gestational diabetes: The consequences of not treating. Am. J. Obstet. Gynecol. 2005, 192, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Robert, M.F.; Neff, R.K.; Hubbell, J.P.; Taeusch, H.W.; Avery, M.E. Association between maternal diabetes and the respiratory-distress syndrome in the newborn. N. Engl. J. Med. 1976, 294, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Silverman, B.L.; Rizzo, T.A.; Cho, N.H.; Metzger, B.E. Long-term effects of the intrauterine environment: The northwestern university diabetes in pregnancy center. Diabetes Care 1998, 21, B142–B149. [Google Scholar] [PubMed]
- Bowers, K.; Yeung, E.; Williams, M.A.; Qi, L.; Tobias, D.K.; Hu, F.B.; Zhang, C. A prospective study of prepregnancy dietary iron intake and risk for gestational diabetes mellitus. Diabetes Care 2011, 34, 1557–1563. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Williams, M.A.; Sorensen, T.K.; King, I.B.; Kestin, M.M.; Thompson, M.L.; Luthy, D.A. Maternal plasma ascorbic acid (vitamin C) and risk of gestational diabetes mellitus. Epidemiology 2004, 15, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Poel, Y.H.M.; Hummel, P.; Lips, P.T.A.M.; Stam, F.; Van Der Ploeg, T.; Simsek, S. Vitamin D and gestational diabetes: A systematic review and meta-analysis. Eur. J. Int. Med. 2012, 23, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Corrado, F.; D’Anna, R.; Di Vieste, G.; Giordano, D.; Pintaudi, B.; Santamaria, A.; Di Benedetto, A. The effect of myoinositol supplementation on insulin resistance in patients with gestational diabetes. Diabet. Med. 2011, 28, 972–975. [Google Scholar] [CrossRef] [PubMed]
- Motulsky, A.G. Diet and Health: Implications for Reducing Chronic Disease Risk; National Academies Press: Washington, DC, USA, 1989. [Google Scholar]
- Lee, C.; Reed, D.; Maclean, C.; Yano, K.; Chiu, D. Dietary potassium and stroke. N. Engl. J. Med. 1988, 318, 995–996. [Google Scholar] [PubMed]
- Zhang, C.; Schulze, M.B.; Solomon, C.G.; Hu, F.B. A prospective study of dietary patterns, meat intake and the risk of gestational diabetes mellitus. Diabetologia 2006, 49, 2604–2613. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Zhang, C.; Chavarro, J.; Bowers, K.; Rich-Edwards, J.; Rosner, B.; Hu, F.B. Prepregnancy adherence to dietary patterns and lower risk of gestational diabetes mellitus. Am. J. Clin. Nutr. 2012, 96, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Bowers, K.; Tobias, D.K.; Olsen, S.F.; Chavarro, J.; Vaag, A.; Zhang, C. Prepregnancy low-carbohydrate dietary pattern and risk of gestational diabetes mellitus: A prospective cohort study. Am. J. Clin. Nutr. 2014, 99, 1378–1384. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Yuan, M.; Chen, N.; Lu, J.; Hu, C.; Mai, W.; Qiu, X. Maternal dietary patterns and gestational diabetes mellitus: A large prospective cohort study in China. Br. J. Nutr. 2015, 113, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Soh, S.; Lee, S.; Hoon, S.; Tan, M.; Goh, A.; Lee, B.; Shek, L.P.; Teoh, O.H.; Kwek, K.; Saw, S.M.; et al. The methodology of the GUSTO cohort study: A novel approach in studying pediatric allergy. Asia Pac. Allergy 2012, 2, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Multiple imputation after 18+ years. J. Am. Stat. Assoc. 1996, 91, 473–489. [Google Scholar] [CrossRef]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [PubMed]
- Lim, G.H.; Toh, J.Y.; Aris, I.M.; Chia, A.-R.; Han, W.M.; Saw, S.M.; Godfrey, K.M.; Gluckman, P.D.; Chong, Y.-S.; Yap, F.; et al. Dietary pattern trajectories from 6 to 12 months of age in a multi-ethnic Asian cohort. Nutrients 2016, 8, 365. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Dietary pattern is associated with obesity in older people in China: Data from China Health and Nutrition Survey (CHNS). Nutrients 2015, 7, 8170–8188. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Spiegelman, D.; Willett, W.C. Prospective study of major dietary patterns and risk of coronary heart disease in men. Am. J. Clin. Nutr. 2000, 72, 912–921. [Google Scholar] [PubMed]
- Newby, P.K.; Muller, D.; Hallfrisch, J.; Andres, R.; Tucker, K.L. Food patterns measured by factor analysis and anthropometric changes in adults. Am. J. Clin. Nutr. 2004, 80, 504–513. [Google Scholar] [PubMed]
- Ley, S.H.; Hanley, A.J.; Retnakaran, R.; Sermer, M.; Zinman, B.; O’Connor, D.L. Effect of macronutrient intake during the second trimester on glucose metabolism later in pregnancy. Am. J. Clin. Nutr. 2011, 94, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Bowers, K.; Tobias, D.K.; Yeung, E.; Hu, F.B.; Zhang, C. A prospective study of prepregnancy dietary fat intake and risk of gestational diabetes. Am. J. Clin. Nutr. 2012, 95, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Saldana, T.M.; Siega-Riz, A.M.; Adair, L.S. Effect of macronutrient intake on the development of glucose intolerance during pregnancy. Am. J. Clin. Nutr. 2004, 79, 479–486. [Google Scholar] [PubMed]
- Villegas, R.; Liu, S.; Gao, Y.; Yang, G.; Li, H.; Zheng, W.; Shu, X.O. Prospective study of dietary carbohydrates, glycemic index, glycemic load and incidence of type 2 diabetes mellitus in middle-aged chinese women. Arch. Int. Med. 2007, 167, 2310–2316. [Google Scholar] [CrossRef] [PubMed]
- Nanri, A.; Mizoue, T.; Noda, M.; Takahashi, Y.; Kato, M.; Inoue, M.; Tsugane, S. Rice intake and type 2 diabetes in Japanese men and women: The Japan public health center--based prospective study. Am. J. Clin. Nutr. 2010, 92, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, M.; Tang, A.; Wakaki, Y.; Koyama, W. Glycemic index of single and mixed meal foods among common Japanese foods with white rice as a reference food. Eur. J. Clin. Nutr. 2003, 57, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.; English, D.; O’Dea, K.; Giles, G. Glycemic index and dietary fiber and the risk of type 2 diabetes (metabolic syndrome/insulin resistance syndrome/pre-diabetes). Diabetes Care 2004, 27, 2701–2706. [Google Scholar] [CrossRef] [PubMed]
- Mohan, V.; Radhika, G.; Sathya, R.; Tamil, S.; Ganesan, A.; Sudha, V. Dietary carbohydrates, glycaemic load, food groups and newly detected type 2 diabetes among urban Asian Indian population in chennai, India (chennai urban rural epidemiology study 59). Br. J. Nutr. 2009, 102, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- Salmerón, J.; Manson, J.; Stampfer, M.; Colditz, G.; Wing, A.; Willett, W. Dietary fiber, glycemic load, and risk of non-insulin-dependent diabetes mellitus in women. JAMA 1997, 277, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.F.F.; Chia, A.R.; Colega, M.; Tint, M.T.; Aris, I.M.; Chong, Y.S.; Yap, F. Maternal protein intake during pregnancy is not associated with offspring birth weight in a multiethnic Asian population. J. Nutr. 2015, 145, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Maki, K.C.; Slavin, J.L.; Rains, T.M.; Kris-Etherton, P.M. Limitations of observational evidence: Implications for evidence-based dietary recommendations. Adv. Nutr. 2014, 5, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Davies, H.T.O.; Crombie, I.K.; Tavakoli, M. When can odds ratios mislead? BMJ 1998, 316, 989–991. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Gestational Diabetes Mellitus | |||||
|---|---|---|---|---|---|
| Yes n = 160 (17.6%) | No n = 749 (82.4%) | p-Value | |||
| Pregnancy BMI (mean ± SD) | 26.6 ± 3.9 | 25.9 ± 4.4 | 0.03 *,a | ||
| Age (mean ± SD) | 33 ± 5 | 30 ± 5 | <0.001 *,a | ||
| Ethnicity n (%) | Chinese | 109 (68.1) | Chinese | 406 (54.2) | |
| Malay | 18 (11.2) | Malay | 216 (28.8) | ||
| Indian | 33 (20.6) | Indian | 127 (17.0) | <0.001 * | |
| Education n (%) | <Secondary | 31 (19.4) | <Secondary | 247 (33.0) | |
| Post-Secondary | 56 (35.0) | Post-Secondary | 277 (37.0) | ||
| University | 73 (45.6) | University | 225 (30.0) | <0.001 * | |
| Household Monthly Income n (%) | <2000 | 14 (8.8) | <2000 | 113 (15.1) | |
| 2000–6000 | 92 (57.5) | 2000–6000 | 447 (59.7) | ||
| >6000 | 54 (33.8) | >6000 | 189 (25.2) | 0.02 * | |
| Smoking n (%) | No | 157 (98.1) | No | 728 (97.2) | |
| Yes | 3 (1.9) | Yes | 21 (2.8) | 0.51 | |
| Alcohol Consumption n (%) | No | 156 (97.5) | No | 715 (95.5) | |
| Yes | 4 (2.5) | Yes | 34 (4.5) | 0.24 | |
| Previous history of GDM n (%) | No | 142 (88.8) | No | 737 (98.4) | |
| Yes | 18 (11.2) | Yes | 12 (1.6) | <0.001 * | |
| Family history of Diabetes n (%) | No | 104 (65.0) | No | 533 (71.2) | |
| Yes | 56 (35.0) | Yes | 216 (28.8) | 0.12 | |
| Birth Order n (%) | First child | 58 (36.2) | First child | 322 (43.0) | |
| Not first child | 102 (63.7) | Not first child | 427 (57.0) | 0.12 | |
| Birthweight (g) (mean ± SD) | 3067 ± 494 | 3098 ± 426 | 0.47 | ||
| Gestational Age at Delivery (days) (mean ± SD) | 269 ± 12 | 268 ± 33 | 0.38 a | ||
| Odds Ratio (OR) (95% CI) | p-Value | ||
|---|---|---|---|
| Vegetable-fruit-rice-based-diet | |||
| Unadjusted model | 1.37 (1.16, 1.63) | <0.01 * | |
| Multivariate model 1 | 1.10 (0.90, 1.35) | 0.36 | |
| Seafood-noodle-based-diet | |||
| Unadjusted model | 0.85 (0.73, 1.01) | 0.06 | |
| Multivariate model 1 | 0.74 (0.59, 0.93) | <0.01 * | |
| Pasta-cheese-processed-meat-diet | |||
| Unadjusted model | 0.97 (0.81, 1.16) | 0.72 | |
| Multivariate model 1 | 0.96 (0.79, 1.17) | 0.71 | |
| Quintile 1 of Seafood-Noodle-Based-Diet (Lowest Scores) | Quintile 5 of Seafood-Noodle-Based-Diet (Highest Scores) | p-Value | ||
|---|---|---|---|---|
| Gestational Diabetes Mellitus n (%) | Yes | 41 (22.5) | 26 (14.3) | 0.06 b |
| No | 141 (77.5) | 156 (85.7) | ||
| Pregnancy BMI (mean ± SD) | 26.8 ± 4.2 | 25.4 ± 3.9 | 0.01 *,c | |
| Age (mean ± SD) | 30.3 ± 5.3 | 30.9 ± 4.8 | 0.34 c | |
| Ethnicity n (%) | Chinese | 41 (22.5) | 154 (84.6) | |
| Malay | 43 (23.6) | 24 (13.2) | ||
| Indian | 98 (53.8) | 4 (2.2) | <0.001 *,b | |
| Education n (%) | <Secondary | 41 (22.5) | 62 (34.1) | |
| Post-Secondary | 60 (33) | 64 (35.2) | ||
| University | 81 (44.5) | 56 (30.8) | 0.01 *,b | |
| Household Monthly Income n (%) | <2000 | 21 (11.5) | 22 (12.1) | |
| 2000–6000 | 108 (59.3) | 98 (53.8) | ||
| >6000 | 53 (29.1) | 62 (34.1) | 0.55 b | |
| Smoking n (%) | No | 173 (95.1) | 179 (98.4) | 0.14 b |
| Yes | 9 (4.9) | 3 (1.6) | ||
| Alcohol Consumption n (%) | No | 175 (96.2) | 174 (95.6) | 0.99 b |
| Yes | 7 (3.8) | 8 (4.4) | ||
| Previous history of GDM n (%) | No | 178 (97.8) | 172 (94.5) | 0.17 b |
| Yes | 4 (2.2) | 10 (5.5) | ||
| Family history of Diabetes n (%) | No | 110 (60.4) | 140 (76.9) | 0.001 *,b |
| Yes | 72 (39.6) | 42 (23.1) | ||
| Birth Order n (%) | First Child | 65 (35.7) | 80 (44.0) | |
| Not first child | 117 (64.3) | 102 (56.0) | 0.13 b | |
| Birthweight (g) (mean ± SD) | 3070 ± 388 | 3141 ± 456 | 0.12 c | |
| Gestational Age at Delivery (days) (mean ± SD) | 269 ± 30 | 268 ± 30 | 0.87 c | |
| Energy (kcal) | 1839 (1474, 2301) a | 2075 (1735, 2445) a | <0.001 *,d | |
| Nutrient Composition | ||||
| Protein, % of Energy | 14.6 (12.5, 17.3) a | 16.3 (13.7, 18.6) a | <0.001 *,d | |
| Total Fat, % of Energy | 31.2 (25.0, 37.7) a | 33.2 (29.0, 38.1) a | 0.004 *,d | |
| Carbohydrate, % of Energy | 53.0 (47.5, 60.9) a | 49.6 (44.2, 55.4) a | <0.001 *,d | |
| Saturated Fat (g) | 25 (15, 34) a | 29 (22, 40) a | <0.001 *,d | |
| Monounsaturated Fat (g) | 21.41 (14.77, 29.60) a | 27.66 (21.03, 41.01) a | <0.001 *,d | |
| Polyunsaturated Fat (g) | 10.9 (6.9, 16.5) a | 11.8 (8.1, 16.2) a | 0.13 d | |
| Protein (g) | 69.13 (51.17, 85.33) a | 81.38 (67.96, 101.71) a | <0.001 *,d | |
| Carbohydrate (g) | 244.48 (198.09, 303.00) a | 254.98 (204.18, 305.66) a | 0.27 d | |
| Total Fat (g) | 64.71 (43.52, 85.83) a | 75.38 (59.74, 100.69) a | <0.001 *,d | |
| Fasting Blood Glucose β (95% CI) | p-Value | 2-Hour Blood Glucose β (95% CI) | p-Value | |
|---|---|---|---|---|
| Vegetable-fruit-rice-based-diet | ||||
| unadjusted model | −0.03 (−0.04, 0.02) | 0.36 | 0.15 (0.13, 0.31) | <0.01 ** |
| Multivariate model 1 | −0.04 (−0.07, –0.005) | 0.03 * | 0.08 (−0.02, 0.18) | 0.11 |
| Seafood-noodle-based-diet | ||||
| Unadjusted model | −0.05 (−0.05, 0.007) | 0.14 | −0.04 (−0.15, 0.04) | 0.27 |
| Multivariate model 1 | −0.01 (−0.05, 0.02) | 0.44 | −0.11 (−0.21, 0.001) | 0.05 |
| Pasta-cheese-processed-meat-diet | ||||
| Unadjusted model | −0.05 (−0.05, 0.008) | 0.16 | −0.05 (−0.17, 0.02) | 0.13 |
| Multivariate model 1 | −0.006 (−0.03, 0.02) | 0.70 | −0.07 (−0.16, 0.03) | 0.16 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Seymour, J.; Chia, A.; Colega, M.; Jones, B.; McKenzie, E.; Shirong, C.; Godfrey, K.; Kwek, K.; Saw, S.-M.; Conlon, C.; et al. Maternal Dietary Patterns and Gestational Diabetes Mellitus in a Multi-Ethnic Asian Cohort: The GUSTO Study. Nutrients 2016, 8, 574. https://doi.org/10.3390/nu8090574
De Seymour J, Chia A, Colega M, Jones B, McKenzie E, Shirong C, Godfrey K, Kwek K, Saw S-M, Conlon C, et al. Maternal Dietary Patterns and Gestational Diabetes Mellitus in a Multi-Ethnic Asian Cohort: The GUSTO Study. Nutrients. 2016; 8(9):574. https://doi.org/10.3390/nu8090574
Chicago/Turabian StyleDe Seymour, Jamie, Airu Chia, Marjorelee Colega, Beatrix Jones, Elizabeth McKenzie, Cai Shirong, Keith Godfrey, Kenneth Kwek, Seang-Mei Saw, Cathryn Conlon, and et al. 2016. "Maternal Dietary Patterns and Gestational Diabetes Mellitus in a Multi-Ethnic Asian Cohort: The GUSTO Study" Nutrients 8, no. 9: 574. https://doi.org/10.3390/nu8090574
APA StyleDe Seymour, J., Chia, A., Colega, M., Jones, B., McKenzie, E., Shirong, C., Godfrey, K., Kwek, K., Saw, S.-M., Conlon, C., Chong, Y.-S., Baker, P., & Chong, M. F. F. (2016). Maternal Dietary Patterns and Gestational Diabetes Mellitus in a Multi-Ethnic Asian Cohort: The GUSTO Study. Nutrients, 8(9), 574. https://doi.org/10.3390/nu8090574