Elevation of Fasting Ghrelin in Healthy Human Subjects Consuming a High-Salt Diet: A Novel Mechanism of Obesity?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Protocol
2.3. Biochemical Analyses
2.4. 24-h Urinary Sodium and Potassium Determination
2.5. Statistical Analysis
3. Result
3.1. Profiles of Study Subjects
3.2. Effects of Salt Intake on BP and 24-h Urinary Sodium Excretion
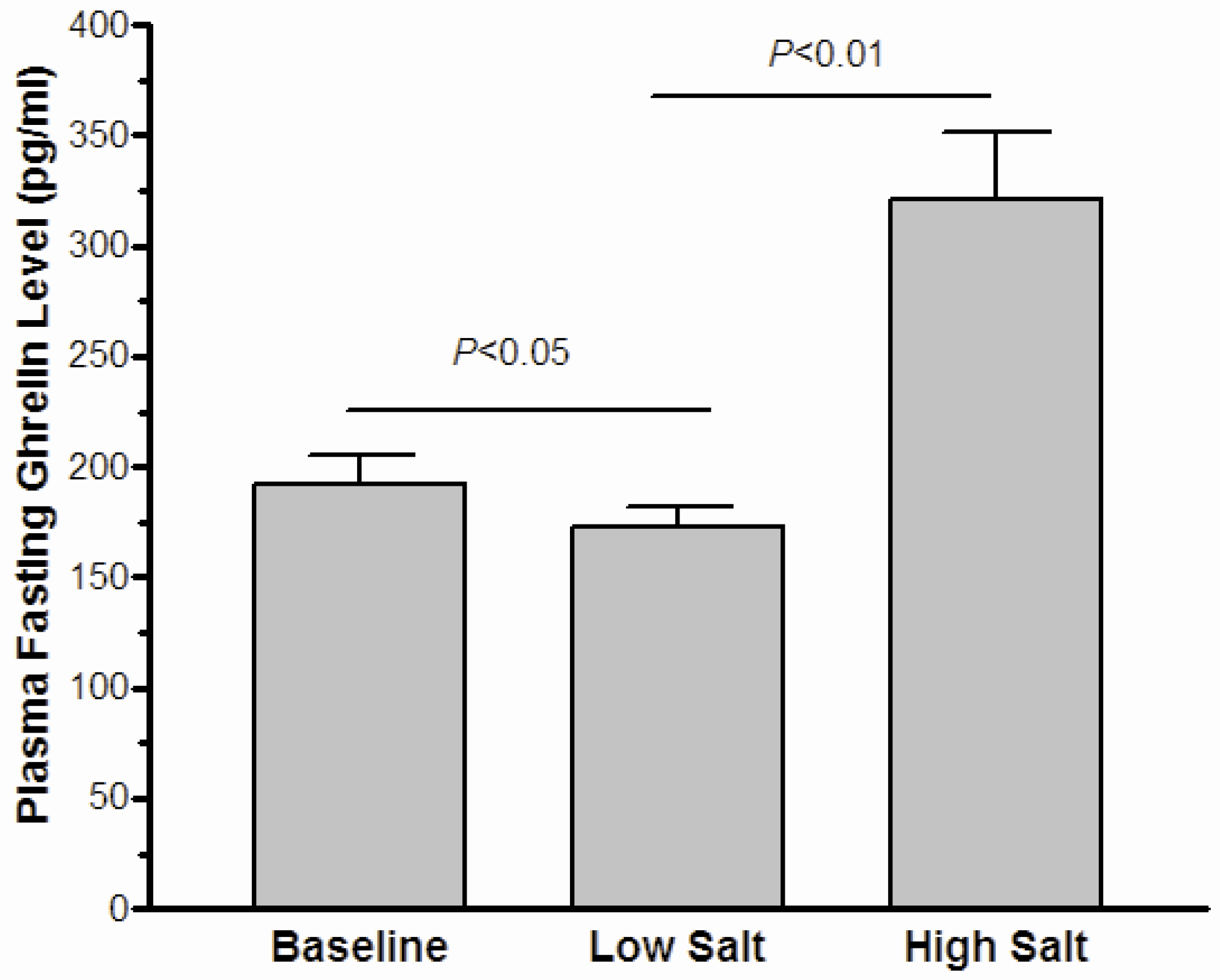
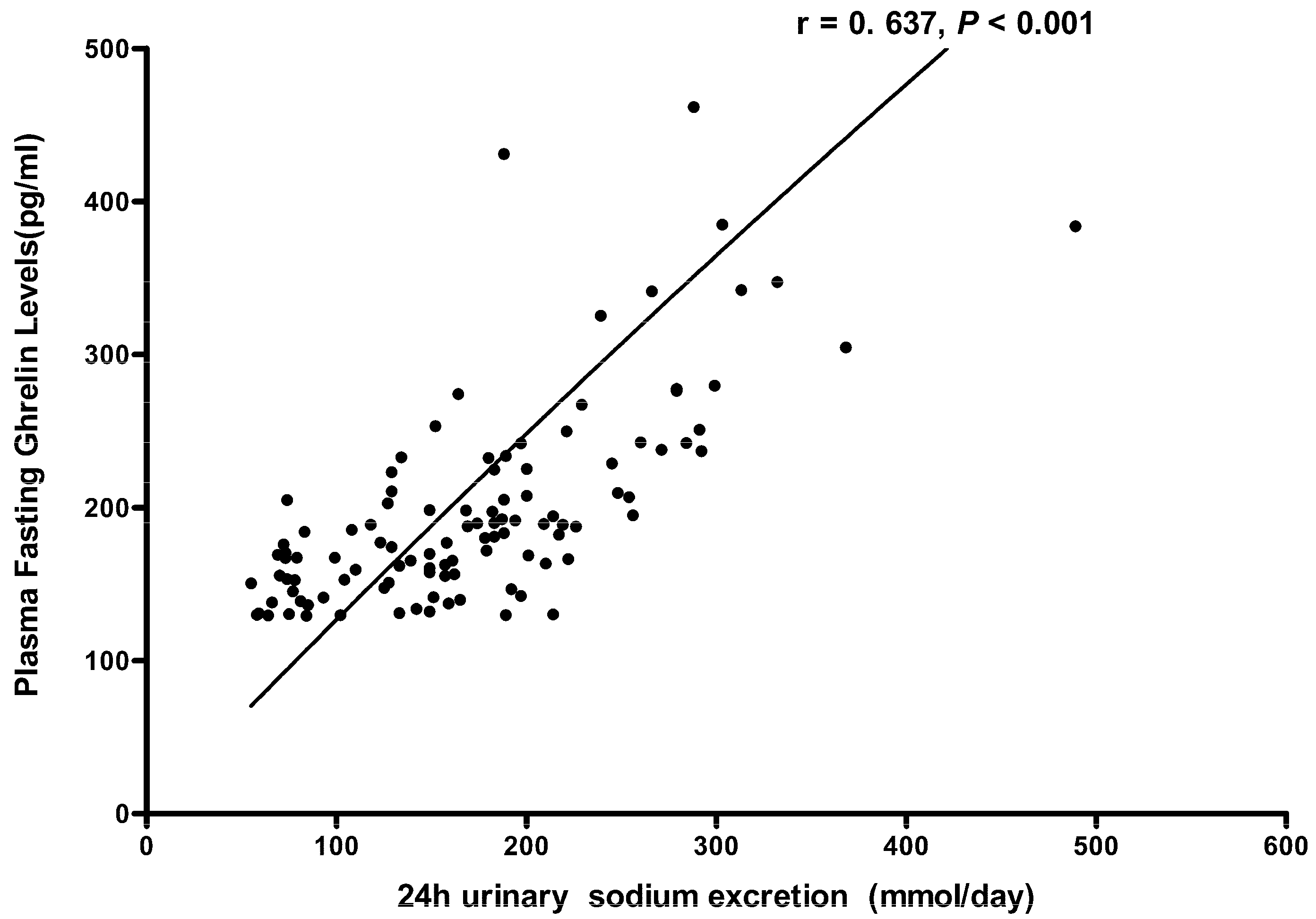
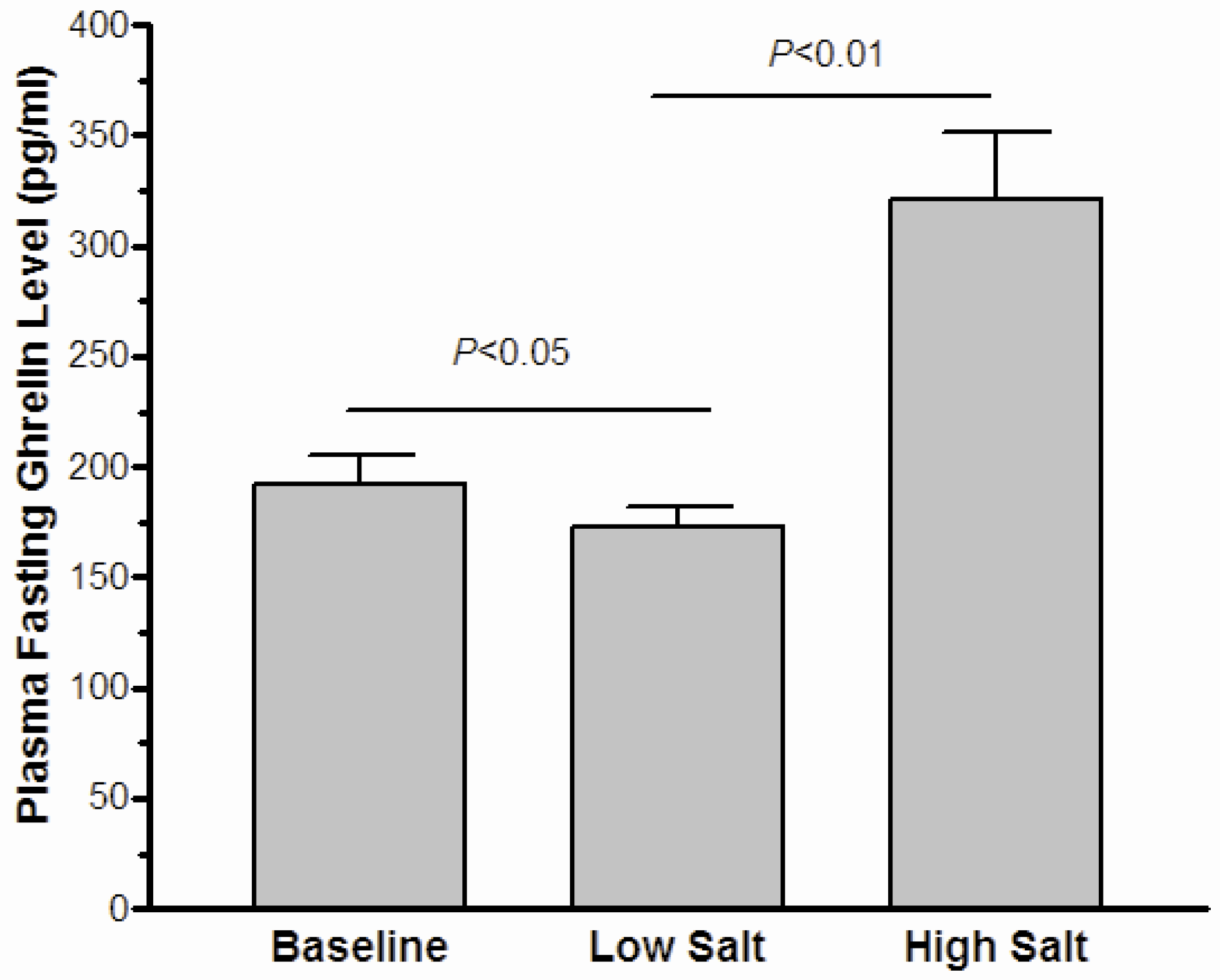
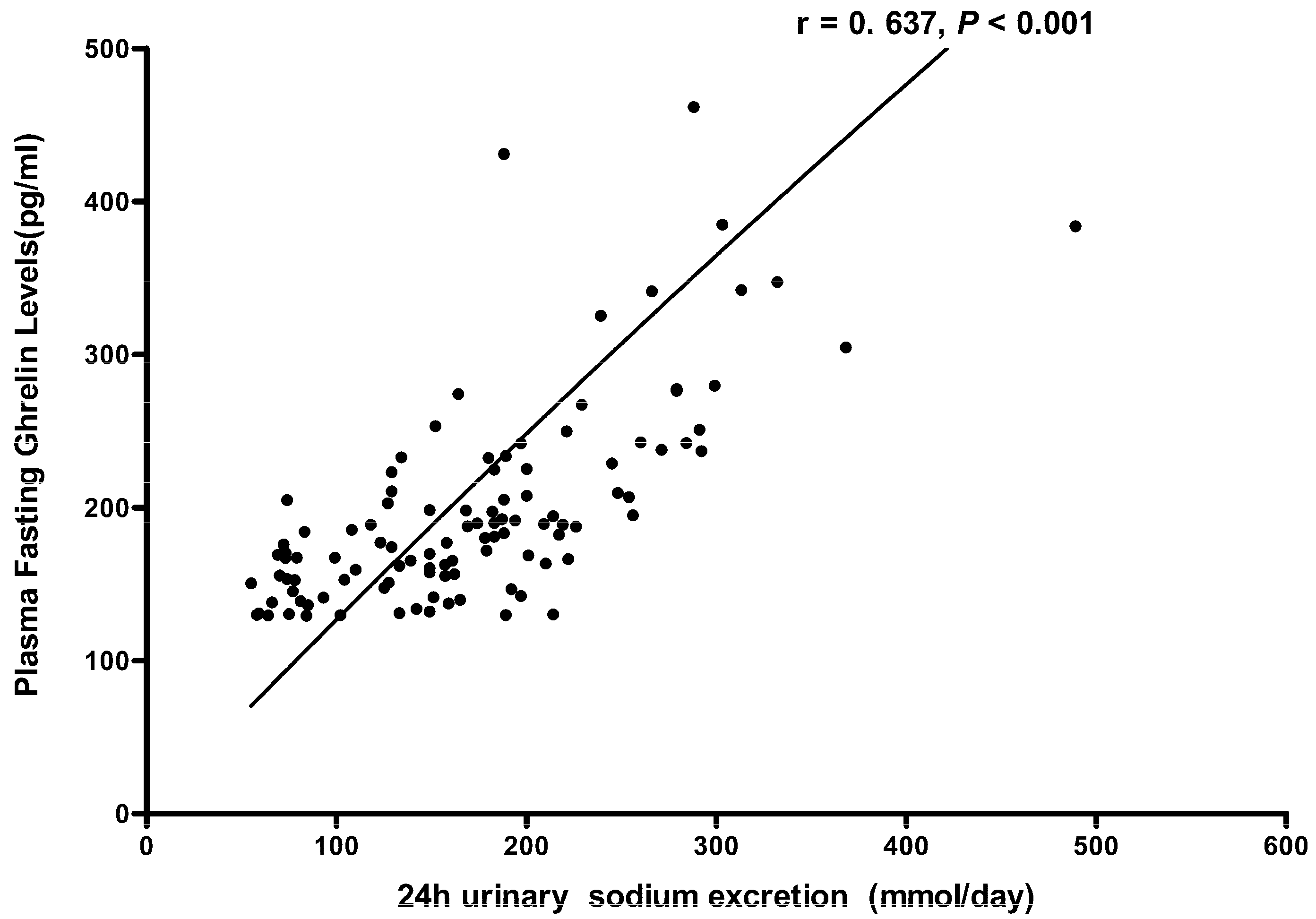
3.3. The Effect of High-Salt Intake on Fasting Ghrelin Levels
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Fact sheet N°311. Updated January 2015. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 27 July 2015).
- Navia, B.; Aparicio, A.; Perea, J.M.; Pérez-Farinós, N.; Villar-Villalba, C.; Labrado, E.; Ortega, R.M. Sodium intake may promote weight gain: Results of the FANPE study in a representative sample of the adult Spanish population. Nutr. Hosp. 2014, 29, 1283–1289. [Google Scholar] [PubMed]
- Fowler, S.P.; Williams, K.; Resendez, R.G.; Hunt, K.J.; Hazuda, H.P.; Stern, M.P. Fueling the obesity epidemic? Artificially sweetened beverage use and long-term weight gain. Obesity 2008, 16, 1894–1900. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Yuan, F.; Ji, W.J.; Guo, Z.Z.; Zhang, L.; Lu, R.Y.; Liu, X.; Liu, H.M.; Zhang, W.C.; Jiang, T.M.; et al. High-salt intake induced visceral adipose tissue hypoxia and its association with circulating monocyte subsets in humans. Obesity 2014, 22, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Baudrand, R.; Campino, C.; Carvajal, C.A.; Olivieri, O.; Guidi, G.; Faccini, G.; Vöhringer, P.A.; Cerda, J.; Owen, G.; Kalergis, A.M.; et al. High sodium intake is associated with increased glucocorticoid production, insulin resistance and metabolic syndrome. Clin. Endocrinol. 2014, 80, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.S.; Oh, S.W. Sodium density and obesity; The Korea National Health and Nutrition Examination Survey 2007–2010. Eur. J. Clin. Nutr. 2013, 67, 141–146. [Google Scholar] [PubMed]
- Hoffmann, I.S.; Cubeddu, L.X. Salt and the metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Cocores, J.A.; Gold, M.S. The Salted Food Addiction Hypothesis may explain overeating and the obesity epidemic. Med. Hypotheses 2009, 73, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F.; Guo, Z.Z.; Ji, W.J.; Ji, W.J.; Ma, Y.Q.; Zhang, Z.L.; Zhou, X.; Li, Y.M. BOLD-MRI evaluation of subcutaneous and visceral adipose tissue oxygenation status: effect of dietary salt intake. Am. J. Transl. Res. 2015, 7, 598–606. [Google Scholar] [PubMed]
- Ma, Y.; He, F.J.; MacGregor, G.A. High salt intake: Independent risk factor for obesity? Hypertension 2015, 66, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Kim, M.K.; Kim, S.M.; Park, H.; Park, C.G.; Park, H.K. Gender-based differences on the association between salt-sensitive genes and obesity in Korean children aged between 8 and 9 years. PLoS ONE 2015, 10, e0120111. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Hosoda, H.; Date, Y.; Nakazato, M.; Matsui, H.; Kangawa, K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature 1999, 402, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Ida, T.; Nakamura, Y.; Shiimura, Y.; Kangawqa, K.; Kojima, M. Physiological roles of ghrelin on obesity. Obes. Res. Clin. Pract. 2014, 8, e405–e413. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Nakamura, Y.; Shiimura, Y.; Ohgusu, H.; Kangawa, K.; Kojima, M. Structure, regulation and function of ghrelin. J. Biochem. 2012, 151, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Wiedmer, P.; Nogueiras, R.; Broglio, F.; D’Alessio, D.; Tschöp, M.H. Ghrelin, obesity and diabetes. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, F.Q.; Wang, D.; Chu, C.; Mu, J.J.; Ren, K.Y.; Guo, T.S.; Chu, C.; Wang, L.; Geng, L.K.; et al. Effect of salt intake and potassium supplementation on serum renalase levels in Chinese adults: A randomized trial. Medicine 2014, 93, e44. [Google Scholar] [CrossRef] [PubMed]
- Cummings, D.E. Ghrelin and the short-and long-term regulation of appetite and body weight. Physiol. Behav. 2006, 89, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Inoue, K.; Fu, M.; Inui, A.; Herzog, H. Chronic overproduction of ghrelin in the hypothalamus leads to temporal increase in food intake and body weight. Neuropeptides 2015, 50, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Nass, R.; Pezzoli, S.S.; Oliver, M.C.; Patrie, J.T.; Harrell, F.E.; Clasey, J.L.; Heymsfield, S.B.; Bach, M.A.; Vance, M.L.; Thorner, M.O. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: A randomized trial. Ann. Intern. Med. 2008, 149, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Tschop, M.; Smiley, D.L.; Heiman, M.L. Ghrelin induces adiposity in rodents. Nature 2000, 407, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, M.; Murakami, N.; Date, Y.; Kojima, M.; Matsuo, H.; Kangawa, K.; Matsukura, S. A role for ghrelin in the central regulation of feeding. Nature 2001, 409, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Wren, A.M.; Small, C.J.; Abbott, C.R.; Dhillo, W.S.; Seal, L.J.; Cohen, M.A.; Batterham, R.L.; Taheri, S.; Stanley, S.A.; Ghatei, M.A.; et al. Ghrelin causes hyperphagia and obesity in rats. Diabetes 2001, 50, 2540–2547. [Google Scholar] [CrossRef] [PubMed]
- Keen-Rhinehart, E.; Bartness, T.J. Peripheral ghrelin injections stimulate food intake, foraging and food hoarding in Siberian hamsters. Am. J. Physiol. 2005, 288, R716–R722. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, P.; Zheng, H.; Smith, R.G. Ghrelin stimulation of growth hormone release and appetite is mediated through the growth hormone secretagogue receptor. Proc. Natl. Acad. Sci. USA 2004, 101, 4679–4684. [Google Scholar] [CrossRef] [PubMed]
- Wortley, K.E.; Anderson, K.D.; Garcia, K.; Murray, J.D.; Malinova, L.; Liu, R.; Moncrieffe, M.; Thabet, K.; Cox, H.J.; Yancopoulos, G.D.; et al. Genetic deletion of ghrelin does not decrease food intake but influences metabolic fuel preference. Proc. Natl. Acad. Sci. USA 2004, 101, 8227–8232. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ahmed, S.; Smith, R.G. Deletion of ghrelin impairs neither growth nor appetite. Mol. Cell. Biol. 2003, 23, 7973–7981. [Google Scholar] [CrossRef] [PubMed]
- Asakawa, A.; Inui, A.; Kaga, T.; Katsuura, G.; Fujimiya, M.; Fujino, M.A.; Kasuga, M. Antagonism of ghrelin receptor reduces food intake and body weight gain in mice. Gut 2003, 52, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Shuto, Y.; Shibasaki, T.; Otagiri, A.; Kuriyama, H.; Ohata, H.; Tamura, H.; Kamegai, J.; Sugihara, H.; Oikawa, S.; Wakabayashi, I. Hypothalamic growth hormone secretagogue receptor regulates growth hormone secretion, feeding, and adiposity. J. Clin. Investig. 2002, 109, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Bagnasco, M.; Tulipano, G.; Melis, M.R.; Argiolas, A.; Cocchi, D.; Muller, E.E. Endogenous ghrelin is an orexigenic peptide acting in the arcuate nucleus in response to fasting. Regul. Pept. 2003, 111, 161–167. [Google Scholar] [CrossRef]
- Murakami, N.; Hayashida, T.; Kuroiwa, T.; Nakahara, K.; Ida, T.; Mondal, M.S.; Nakazato, M.; Kojima, M.; Kangawa, K. Role for central ghrelin in food intake and secretion profile of stomach ghrelin in rats. J. Endocrinol. 2002, 174, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, M.; Santoro, N.; Cirillo, G.; Raimondo, P.; Grandone, A.; D’Aniello, A.; Di Nardo, M.; Perrone, L. Molecular screening of the ghrelin gene in Italian obese children: The Leu72Met variant is associated with an earlier onset of obesity. Int. J. Obes. 2004, 28, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Pöykkö, S.; Ukkola, O.; Kauma, H.; Savolainen, M.J.; Kesäniemi, Y.A. Ghrelin Arg51Gln mutation is a risk factor for Type 2 diabetes and hypertension in a random sample of middle-aged subjects. Diabetologia 2003, 46, 455–458. [Google Scholar] [PubMed]
- Ukkola, O.; Ravussin, E.; Jacobson, P.; Pérusse, L.; Rankinen, T.; Tschöp, M.; Heiman, M.L.; Leon, A.S.; Rao, D.C.; Skinner, J.S.; et al. Role of ghrelin polymorphisms in obesity based on three different studies. Obes. Res. 2002, 10, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Reimer, M.K.; Pacini, G.; Ahrén, B. Dose-dependent inhibition by ghrelin of insulin secretion in the mouse. Endocrinology 2003, 44, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Dezaki, K.; Hosoda, H.; Kakei, M.; Hashiguchi, S.; Watanabe, M.; Kangawa, K.; Yada, T. Endogenous ghrelin in pancreatic islets restricts insulin release by attenuating Ca2+ signaling in beta-cells: Implication in the glycemic control in rodents. Diabetes 2004, 53, 3142–3151. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.; Prigeon, R.L.; Davis, H.W.; Bidlingmaier, M.; Kahn, S.E.; Cummings, D.E.; Tschöp, M.H.; D’Alessio, D. Ghrelin suppresses glucose-stimulated insulin secretion and deteriorates glucose tolerance in healthy humans. Diabetes 2010, 59, 2145–2151. [Google Scholar] [CrossRef] [PubMed]
- Na, E.S.; Morris, M.J.; Johnson, A.K. Opioid mechanisms that mediate the palatability of and appetite for salt in sodium replete and deficient states. Physiol. Behav. 2012, 106, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Bolhuis, D.P.; Costanzo, A.; Newman, L.P.; Keast, R.S. Salt Promotes Passive Overconsumption of Dietary Fat in Humans. J. Nutr. 2016, 146, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Cong, W.N.; Daimon, C.M.; Wang, R.; Tschöp, M.H.; Sévigny, J.; Martin, B.; Maudsley, S. Altered lipid and salt taste responsivity in ghrelin and GOAT null mice. PLoS ONE 2013, 8, e76553. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Parameter | Values |
|---|---|
| Mean age (year) | 50.6 ± 2.1 |
| Sex (male/female) | 21/17 |
| BMI (kg/m2) | 22.8 ± 0.4 |
| Systolic BP (mmHg) | 110.6 ± 5.8 |
| Diastolic BP (mmHg) | 72.1 ± 2.7 |
| Glucose, mmol/L | 3.91 ± 0.11 |
| Total cholesterol, mmol/L | 4.18 ± 0.14 |
| Triglycerides, mmol/L | 1.32 ± 0.11 |
| LDL-cholesterol, mmol/L | 2.35 ± 0.11 |
| HDL-cholesterol, mmol/L | 1.21 ± 0.04 |
| SBP | DBP | 24 h Urinary Na+ (mmol/Day) | |
|---|---|---|---|
| Baseline | 110.6 ± 5.8 | 72.1 ± 2.7 | 175.8 ± 11.1 |
| Low-salt diet | 108.7 ± 2.8 | 73.5 ± 2.0 | 98.8 ± 9.3 |
| High-salt diet | 116.4 ± 5.8 * | 77.3 ± 4.2 * | 268 ± 10.2 * |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Li, F.; Liu, F.-Q.; Chu, C.; Wang, Y.; Wang, D.; Guo, T.-S.; Wang, J.-K.; Guan, G.-C.; Ren, K.-Y.; et al. Elevation of Fasting Ghrelin in Healthy Human Subjects Consuming a High-Salt Diet: A Novel Mechanism of Obesity? Nutrients 2016, 8, 323. https://doi.org/10.3390/nu8060323
Zhang Y, Li F, Liu F-Q, Chu C, Wang Y, Wang D, Guo T-S, Wang J-K, Guan G-C, Ren K-Y, et al. Elevation of Fasting Ghrelin in Healthy Human Subjects Consuming a High-Salt Diet: A Novel Mechanism of Obesity? Nutrients. 2016; 8(6):323. https://doi.org/10.3390/nu8060323
Chicago/Turabian StyleZhang, Yong, Fenxia Li, Fu-Qiang Liu, Chao Chu, Yang Wang, Dan Wang, Tong-Shuai Guo, Jun-Kui Wang, Gong-Chang Guan, Ke-Yu Ren, and et al. 2016. "Elevation of Fasting Ghrelin in Healthy Human Subjects Consuming a High-Salt Diet: A Novel Mechanism of Obesity?" Nutrients 8, no. 6: 323. https://doi.org/10.3390/nu8060323
APA StyleZhang, Y., Li, F., Liu, F.-Q., Chu, C., Wang, Y., Wang, D., Guo, T.-S., Wang, J.-K., Guan, G.-C., Ren, K.-Y., & Mu, J.-J. (2016). Elevation of Fasting Ghrelin in Healthy Human Subjects Consuming a High-Salt Diet: A Novel Mechanism of Obesity? Nutrients, 8(6), 323. https://doi.org/10.3390/nu8060323