Ventilatory Function in Young Adults and Dietary Antioxidant Intake

Abstract
:1. Introduction
2. Methods
2.1. Setting and Sample
2.2. Ventilatory function
2.3. Dietary Exposures
2.3.1. Food Frequency Questionnaire (FFQ)
2.3.2. Nutrient and Antioxidant Estimates
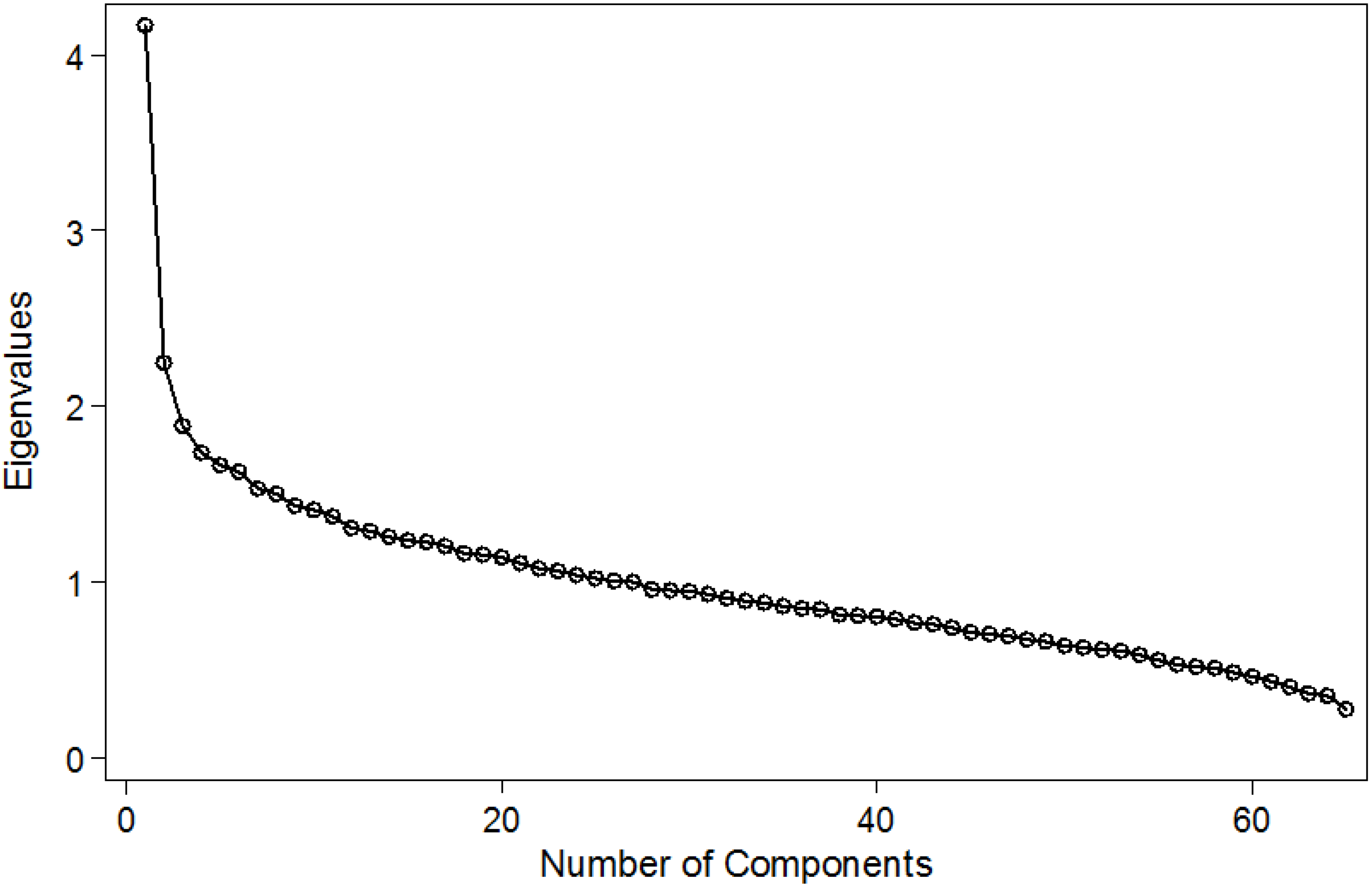
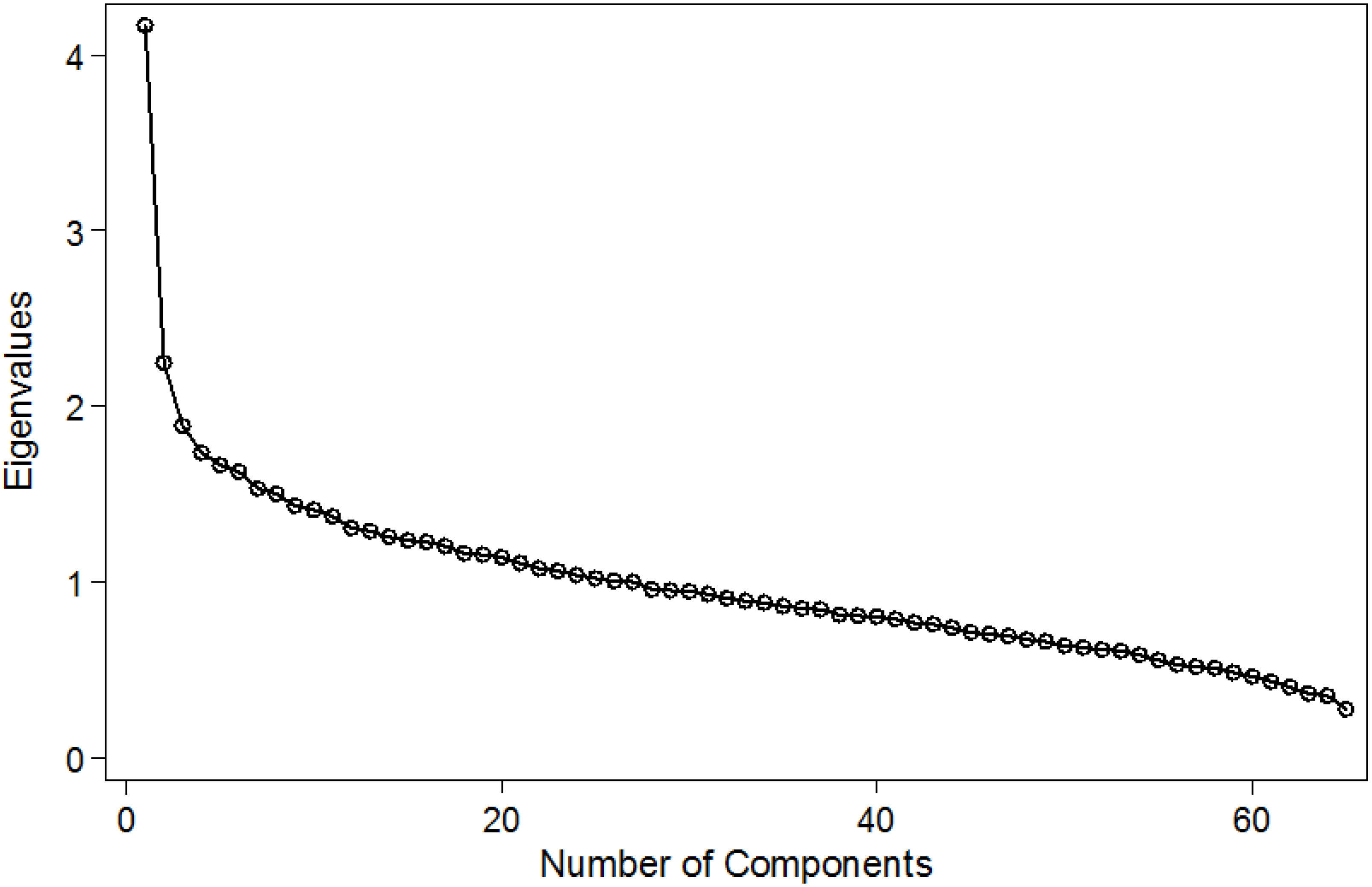
2.3.3. Assessment of Dietary Patterns
2.4. Statistical Analyses
3. Results

{kind=link}
| Variable | Males (n = 542) | Females (n = 645) |
|---|---|---|
| Age and anthropometric variables | ||
| Age (years) Mean (SD) | 24.6 (1.4) | 24.7 (1.5) |
| Adult weight (kg) Median (IQR) | 70.1 (63.0 to 77.9) | 61.5 (54.9 to 70.0) |
| Adult height (cm) Mean (SD) | 168.1 (6.1) | 156.3 (5.5) |
| BMI (kg/m2) Median (IQR) | 24.7 (22.6 to 27.2) | 25.1 (22.6 to 28.6) |
| Weight at birth (g) Mean (SD) | 3184 (488.2) | 3192 (508.0) |
| Measurements of lung function (Mean (SD)) | ||
| FEV1 (L) † | 4.12 (0.53) | 3.09 (0.38) |
| FEV1 as % of predicted value for age, height and sex | 105.2 (10.91) | 105.3 (10.69) |
| FVC (L) | 4.78 (0.63) | 3.53 (0.44) |
| FVC as % of predicted value for age, height and sex | 104.9 (7.3) | 103.2 (8.5) |
| FEV1/FVC | 0.86 (0.047) | 0.88 (0.048) |
| Bronchial hyper-responsiveness (BHR) as positive response to methacholine challenge (16 mg/mL) % | 6.3 | 15.5 |
| Wheeze in the last 12 months (%) | 26.3 | 28.4 |
| Ever had asthma (%) | 3.1 | 5.9 |
| Dr diagnosed asthma (%) | 2.6 | 5.4 |
| 12 years of full time education (%) | 50.0 | 50.0 |
| Number of household belongings (as estimation of SES) (N (%)) | ||
| 0 or 1 | 75 (13.8) | 93 (14.3) |
| 2 | 164 (30.2) | 223 (34.4) |
| 3 | 173 (31.9) | 211 (32.5) |
| 4 or 5 | 131 (24.1) | 122 (18.8) |
| Energy and Nutrients | Males | % TEI | % EAR | % RNI | Females | % TEI | % EAR | % RNI |
|---|---|---|---|---|---|---|---|---|
| Median [IQR] | Median [IQR] | |||||||
| Total Fruits (g) | 182.5 [92.0–210.8] | 175.3 [87.4–205.2] | ||||||
| Total vegetables (g) | 432.4 [390.8–462.0] | 345.2 [294.8–401.6] | ||||||
| Total energy intake (TEI) (kcal) | 3439 [2665.0–4415.0] | 134.9 | 2279 [1170.0–2844.0] | 117.5 | ||||
| Proteins (g) | 129.6 [98.4–163.3] | 18.2 | 292 | 92.1 [71.0–118.1] | 15.4 | 256 | ||
| Carbohydrates (g) | 502.6 [385.1–625.2] | 58.5 | 136.0 | 328.8 [254.4–427.8] | 57.7 | 138.0 | ||
| Total lipids (g) | 97.9 [71.1–137.6] | 23.3 | 73.1 | 66.1 [48.2–91.9] | 26.9 | 74.6 | ||
| PUFA (g) | 26.2 [18.3–36.1] | 6.9 | 106.2 | 18.7 [13.3–25.5] | 7.4 | 113.8 | ||
| MUFA (g) | 36.6 [25.5–55.1] | 9.6 | 73.8 | 23.3 [16.7–35.5] | 9.2 | 70.8 | ||
| SFA (g) | 26.1 [18.9–38.1] | 6.8 | 61.8 | 17.1 [11.7–25.1] | 6.8 | 61.8 | ||
| Omega 3 (g) | 0.24 [0.1–0.5] | 0.06 | 1.2 | 0.2 [0.1–0.4] | 0.08 | 4.0 | ||
| Omega 6 (g) | 11.9 [7.7–17.0] | 3.1 | 310 | 8.5 [5.8–13.1] | 3.4 | 340 | ||
| Carotene (µg) | 1027.0 [585.6–1707.0] | 98 | 1107.1 [681.2–1876.8] | 96 | ||||
| Total vitamin A (µg) | 1412.3 [854.4–2121.7] | 155 | 1374.5 [891.7–2328.9] | 250 | ||||
| Vitamin C (mg) | 133.3 [84.9–235.1] | 221 | 138.7 [81.7–229.2] | 230 | ||||
| Vitamin E (mg) | 19.6 [14.2–26.3] | 131 | 15.2 [10.9–19.7] | 100 | ||||
| Selenium (μg) | 163.8 [119.9–203.2] | 82 | 100.6 [77.5–129.7] | 50 | ||||
| Zinc (mg) | 11.8 [9.2–14.7] | 100 | 9.5 [7.2–10.9] | 119 | ||||
| Total catechins (mg) | 17.1 [7.8–64.4] | NA | 21.2 [9.3–68.5] | NA | ||||
| Flavonols (mg) | 26.2 [15.7–44.3] | NA | 24.7 [12.7–41.3] | NA | ||||
| Flavones (mg) | 0.1 [0.04–0.2] | NA | 0.1 [0.03–0.2] | NA |
| Nutrient | Quintiles | FEV1 (L) | FVC (L) | FEV1/FVC |
|---|---|---|---|---|
| Difference of Means (95% CI) | ||||
| Vitamin C (mg) | 1 | 0 | 0 | 0 |
| 2 | −0.05 (−0.12 to 0.01) | −0.10 (−0.14 to 0.014) | −0.0002 (−0.01 to 0.01) | |
| 3 | −0.002 (−0.07 to 0.07) | 0.04 (−0.04 to 0.12) | −0.01 (−0.02 to −0.0005) | |
| 4 | 0.004 (−0.06 to 0.07) | 0.02 (−0.10 to 0.10) | −0.002 (−0.01 to 0.007) | |
| 5 | −0.02 (−0.09 to 0.06) | −0.01 (−0.09 to 0.07) | −0.003 (−0.01 to 0.007) | |
| p for trend | 0.75 | 0.47 | 0.44 | |
| Vitamin E (mg) | 1 | 0 | 0 | 0 |
| 2 | −0.06 (−0.13 to 0.01) | −0.07 (−0.15 to 0.01) | 0.002 (−0.006 to 0.01) | |
| 3 | −0.004 (−0.08 to 0.07) | 0.02 (−0.06 to 0.10) | −0.004 (−0.01 to 0.005) | |
| 4 | −0.02 (−0.09 to 0.06) | −0.01 (−0.10 to 0.07) | −0.0002 (−0.01 to 0.01) | |
| 5 | 0.01 (−0.08 to 0.09) | 0.04 (−0.05 to 0.14) | −0.01 (−0.02 to 0.01) | |
| p for trend | 0.61 | 0.23 | 0.32 | |
| Total vitamin A (μg) | 1 | 0 | 0 | 0 |
| 2 | 0.06 (−0.004 to 0.13) | 0.05 (−0.03 to 0.13) | 0.006 (−0.003 to 0.015) | |
| 3 | 0.04 (−0.03 to 0.11) | 0.06 (−0.02 to 0.14) | −0.004 (−0.013 to 0.004) | |
| 4 | 0.01 (−0.06 to 0.08) | 0.04 (−0.04 to 0.11) | −0.004 (−0.013 to 0.005) | |
| 5 | 0.02 (−0.06 to 0.09) | 0.03 (−0.05 to 0.11) | −0.001 (−0.01 to 0.008) | |
| p for trend | 0.78 | 0.65 | 0.19 | |
| Selenium (μg) | 1 | 0 | 0 | 0 |
| 2 | −0.01 (−0.08 to 0.06) | 0.01 (−0.07 to 0.09) | −0.003 (−0.01 to 0.01) | |
| 3 | −0.04 (−0.11 to 0.03) | −0.04 (−0.12 to 0.05) | −0.001 (−0.01 to 0.01) | |
| 4 | −0.06 (−0.14 to 0.03) | −0.02 (−0.012 to 0.07 | −0.01 (−0.02 to 0.003) | |
| 5 | −0.02 (−0.13 to 0.09) | 0.06 (−0.06 to 0.18) | −0.01 (−0.03 to 0.0001) | |
| p for trend | 0.30 | 0.90 | 0.09 | |
| Zinc (mg) | 1 | 0 | 0 | 0 |
| 2 | 0.02 (−0.05 to 0.09) | −0.001 (−0.08 to 0.08) | 0.01 (−0.003 to 0.01) | |
| 3 | −0.05 (−0.12 to 0.03) | −0.04 (−0.12 to 0.04) | −0.002 (−0.01 to 0.01) | |
| 4 | −0.01 (−0.09 to 0.07) | 0.05 (−0.09 to 0.13) | −0.01 (−0.02 to 0.0001) | |
| 5 | 0.01 (−0.09 to 0.11) | 0.02 (−0.09 to 0.13) | −0.001 (−0.01 to 0.01) | |
| p for trend | 0.82 | 0.48 | 0.14 | |
| Omega 3 fatty acids (mg) | 1 | 0 | 0 | 0 |
| 2 | 0.04 (−0.03 to 0.11) | 0.05 (−0.02 to 0.13) | −0.003 (−0.01 to 0.01) | |
| 3 | 0.05 (−0.02 to 0.11) | 0.04 (−0.04 to 0.12) | 0.002 (−0.001 to 0.01) | |
| 4 | 0.08 (0.01 to 0.14) | 0.08 (0.003 to 0.16) | 0.002 (−0.01 to 0.01) | |
| 5 | 0.08 (0.005 to 0.15) | 0.08 (0.001 to 0.16) | 0.001 (−0.01 to 0.01) | |
| p for trend | 0.02 | 0.04 | 0.52 | |
| Omega 6 fatty acids (mg) | 1 | 0 | 0 | 0 |
| 2 | −0.08 (−0.14 to −0.01) | −0.08 (−0.15 to 0.001) | −0.002 (−0.1 to 0.01) | |
| 3 | −0.03 (−0.10 to 0.04) | −0.28 (−0.11 to 0.05) | −0.003 (−0.01 to 0.01) | |
| 4 | −0.01 (−0.08 to 0.10) | −0.001 (−0.08 to 0.08) | −0.002 (−0.01 to 0.007) | |
| 5 | −0.005 (−0.08 to 0.07) | 0.01 (−0.07 to 0.09) | −0.002 (−0.01 to 0.007) | |
| p for trend | 0.51 | 0.41 | 0.73 | |
| Flavones (mg) | 1 | 0 | 0 | 0 |
| 2 | 0.01 (−0.05 to 0.08) | 0.01 (−0.06 to 0.09) | −0.001 (−0.01 to 0.01) | |
| 3 | 0.02 (−0.05 to 0.09) | 0.004 (−0.07 to 0.08) | 0.002 (−0.01 to 0.01) | |
| 4 | −0.002 (−0.07 to 0.07) | 0.003 (−0.07 to 0.08) | −0.002 (−0.01 to 0.01) | |
| 5 | 0.01 (−0.06 to 0.07) | 0.01 (−0.06 to 0.09) | −0.001 (−0.01 to 0.01) | |
| p per trend | 0.96 | 0.85 | 0.77 | |
| Flavonols (mg) | 1 | 0 | 0 | |
| 2 | 0.07 (0.003 to 0.14) | 0.09 (0.01 to 0.16) | 0.001 (−0.01 to 0.01) | |
| 3 | 0.05 (−0.02 to 0.12) | 0.06 (−0.01 to 0.14) | −0.001 (−0.01 to 0.01) | |
| 4 | 0.05 (−0.02 to 0.12) | 0.07 (−0.004 to 0.15) | −0.002 (−0.01 to 0.01) | |
| 5 | 0.08 (0.01 to 0.16) | 0.10 (0.02 to 0.18) | 0.002 (−0.01 to 0.01) | |
| p for trend | 0.08 | 0.05 | 0.99 | |
| Total catechins (mg) | 1 | 0 | 0 | 0 |
| 2 | −0.04 (−0.11 to 0.03) | −0.04 (−0.13 to 0.03) | 0.0003 (−0.01 to 0.01) | |
| 3 | 0.03 (−0.03 to 0.11) | 0.06 (−0.02 to 0.13) | −0.01 (−0.02 to 0.003) | |
| 4 | 0.04 (−0.03 to 0.11) | 0.08 (0.003 to 0.16) | −0.01 (−0.02 to 0.002) | |
| 5 | 0.04 (−0.03 to 0.11) | 0.07 (0.01 to 0.15) | −0.01 (−0.01 to 0.004) | |
| p for trend | 0.06 | 0.006 | 0.09 | |
| Food Group | Quintiles | FEV1 (L) | FVC (L) | FEV1/FVC |
|---|---|---|---|---|
| Difference of Means (95% CI) | ||||
| Total fruits (g) | 1 | 0 | 0 | |
| 2 | −0.02 (−0.09 to 0.05) | −0.01 (−0.09 to 0.06) | −0.004 (−0.01 to 0.01) | |
| 3 | 0.03 (−0.04 to 0.10) | 0.04 (−0.04 to 0.11) | −0.002 (−0.01 to 0.004) | |
| 4 | 0.02 (−0.05 to 0.09) | 0.05 (−0.03 to 0.12) | −0.005 (−0.01 to 0.004) | |
| 5 | 0.05 (−0.02 to 0.12) | 0.08 (0.003 to 0.15) | −0.005 (−0.01 to 0.003) | |
| p for trend | 0.09 | 0.02 | 0.23 | |
| Total vegetables (g) | 1 | 0 | 0 | 0 |
| 2 | 0.03 (−0.04 to 0.10) | 0.02 (−0.06 to 0.09) | 0.004 (−0.01 to 0.01) | |
| 3 | 0.01 (−0.06 to 0.08) | 0.05 (−0.03 to 0.13) | −0.01 (−0.02 to 0.002) | |
| 4 | 0.01 (−0.06 to 0.08) | 0.05 (−0.03 to 0.13) | −0.01 (−0.02 to 0.0002) | |
| 5 | 0.03 (−0.05 to 0.10) | 0.05 (−0.04 to 0.13) | −0.002 (−0.01 to 0.007) | |
| p for trend | 0.74 | 0.17 | 0.10 | |
| Lung Function | Quintiles of Dietary Patterns | Unadjusted Odds Ratio (SE) | Adjusted Odds Ratio (SE) |
|---|---|---|---|
| FEV1 | “Animal proteins and starchy foods” | ||
| 1 | 0 | 0 | |
| 2 | 0.10 (0.06) | −0.05 (0.04) | |
| 3 | 0.30 (0.06) | −0.02 (0.04) | |
| 4 | 0.62 (0.06) | −0.01 (0.04) | |
| 5 | 0.75 (0.05) | −0.04 (0.05) | |
| p for trend | <0.0001 | 0.78 | |
| “Fruits and vegetables” | |||
| 1 | 0 | 0 | |
| 2 | −0.0001 (0.06) | 0.03 (0.04) | |
| 3 | −0.12 (0.06) | −0.03 (0.04) | |
| 4 | −0.04 (0.06) | 0.03 (0.04) | |
| 5 | −0.09 (0.01) | 0.03 (0.04) | |
| p for trend | 0.11 | 0.48 | |
| FVC | “Animal proteins and starchy foods” | ||
| 1 | 0 | 0 | |
| 2 | 0.14 (0.07) | −0.05 (0.04) | |
| 3 | 0.37 (0.07) | −0.008 (0.04) | |
| 4 | 0.79 (0.07) | 0.01 (0.05) | |
| 5 | 0.94 (0.07) | −0.03 (0.06) | |
| p for trend | <0.0001 | 0.93 | |
| “Fruits and vegetables” | |||
| 1 | 0 | 0 | |
| 2 | −0.008 (0.07) | 0.03 (0.04) | |
| 3 | −0.12 (0.07) | −0.008 (0.85) | |
| 4 | −0.01 (0.07) | 0.07 (0.04) | |
| 5 | −0.10 (0.07) | 0.05 (0.04) | |
| p for trend | 0.21 | 0.14 | |
| FEV1/FVC | “Animal proteins and starchy foods” | ||
| 1 | 0 | 0 | |
| 2 | −0.05 (0.004) | −0.003 (0.004) | |
| 3 | −0.008 (0.004) | −0.003 (0.005) | |
| 4 | −0.02 (0.004) | −0.005 (0.005) | |
| 5 | −0.02 (0.005) | −0.002 (0.007) | |
| p for trend | <0.0001 | 0.54 | |
| Ratio FEV1/FVC | “Fruits and vegetables” | ||
| 1 | 0 | 0 | |
| 2 | 0.003 (0.004) | 0.002 (0.004) | |
| 3 | −0.002 (0.004) | −0.004 (0.004) | |
| 4 | −0.005 (0.005) | −0.006 (0.005) | |
| 5 | 0.002 (0.005) | −0.001 (0.005) | |
| p for trend | <0.0001 | 0.37 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Appendix
| Food Item | Dietary Pattern I (Western Diet) | Dietary Pattern II (Fruit and Vegetables) |
|---|---|---|
| Orange | 0 | 0 |
| Lemon | 0 | 0.3199218 |
| Kiwi | 0 | 0 |
| Apple | 0 | 0.3203267 |
| Strawberrie | 0 | 0 |
| Mandarin | 0 | 0 |
| Beetroot | 0 | 0.4113356 |
| Chard | 0 | 0.3344303 |
| Sweetpepper | 0 | 0.3768218 |
| Garlic | 0 | 0.3903755 |
| Onion | 0 | 0.4760728 |
| Tomato | 0 | 0.3935958 |
| Potato | 0.6293718 | 0.3563259 |
| Pumpkin | 0 | 0.5209844 |
| Carrot | 0 | 0.4572368 |
| Avocado | 0.3387931 | 0 |
| Bean | 0 | 0.3883224 |
| Lentil | 0 | 0.3531107 |
| Chickpeas | 0 | 0 |
| Meataverage | 0 | 0 |
| Meatnofat | 0 | 0 |
| Meatfat | 0.3405617 | 0 |
| Chickenav | 0 | 0 |
| Chickskin | 0 | 0 |
| Chicknoskin | 0 | 0 |
| Ribs | 0.4815942 | 0 |
| Salmon | 0 | 0 |
| Fish | 0 | 0 |
| Shellfish | 0 | 0 |
| Eggs | 0.3899055 | 0 |
| Bread | 0.426953 | 0 |
| Brownbread | 0 | 0 |
| Knybread | 0 | 0 |
| Pasta | 0.4377254 | 0 |
| Rice | 0.3212484 | 0 |
| Cake | 0 | 0 |
| Oil | 0.400673 | 0 |
| Bacon | 0 | 0 |
| Sausage1 | 0.3344502 | 0 |
| Frankfurter | 0.4175243 | 0 |
| Ham | 0.5813709 | 0 |
| Offal | 0 | 0 |
| Margarine | 0 | 0 |
| Butter | 0 | 0 |
| Marbutter | 0 | 0 |
| Marglight | 0 | 0 |
| Mayonaise | 0.4619392 | 0 |
| Maylight | 0 | 0 |
| Wholemilk | 0 | 0 |
| Sskmilk | 0 | 0 |
| Smilk | 0 | 0 |
| Yoghurt | 0 | 0 |
| Cheeseg | 0.5296596 | 0 |
| Maturecheese | 0 | 0 |
| Cottagecheese | 0 | 0 |
| Sugar | 0 | 0 |
| Jam | 0 | 0 |
| Honey | 0 | 0 |
| Coke | 0.3835198 | 0 |
| Juice | 0 | 0 |
| Tealight | 0 | 0 |
| Teadark | 0 | 0 |
| Coffee | 0 | 0 |
| Redwine | 0.3425927 | 0 |
| Salt | 0 | 0 |
Conflicts of Interest
References
- James, A.L.; Palmer, L.J.; Kicic, E.; Maxwell, P.S.; Lagan, S.E.; Ryan, G.F.; Musk, A.W. Decline in lung function in the Busselton Health Study: The effects of asthma and cigarette smoking. Am. J. Respir. Crit. Care Med. 2005, 171, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Young, R.P.; Hopkins, R.; Eaton, T.E. Forced expiratory volume in one second: Not just a lung function test but a marker of premature death from all causes. Eur. Respir. J. 2007, 30, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Tockman, M.S.; Pearson, J.D.; Fleg, J.L.; Metter, E.J.; Kao, S.Y.; Rampal, K.G.; Cruise, L.J.; Fozard, J.L. Rapid decline in FEV1. A new risk factor for coronary heart disease mortality. Am. J. Respir. Crit. Care Med. 1995, 151, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, E.B.; Welch, V.L.; Couper, D.; Nieto, F.J.; Liao, D.; Rosamond, W.D.; Heiss, G. Lung function and incident coronary heart disease: The Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 2003, 158, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M.; Buist, A.S. Global burden of COPD: Risk factors, prevalence, and future trends. Lancet 2007, 370, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Tabak, C.; Smit, H.A.; Rasanen, L.; Fidanza, F.; Menotti, A.; Nissinen, A.; Feskens, E.J.; Heederik, D.; Kromhout, D. Dietary factors and pulmonary function: A cross sectional study in middle aged men from three European countries. Thorax 1999, 54, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Kelly, Y.; Sacker, A.; Marmot, M. Nutrition and respiratory health in adults: Findings from the health survey for Scotland. Eur. Respir. J. 2003, 21, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Butland, B.K.; Strachan, D.P.; Anderson, H.R. Fresh fruit intake and asthma symptoms in young British adults: Confounding or effect modification by smoking? Eur. Respir. J. 1999, 13, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Carey, I.M.; Strachan, D.P.; Cook, D.G. Effects of changes in fresh fruit consumption on ventilatory function in healthy British adults. Am. J. Respir. Crit. Care Med. 1998, 158, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Strachan, D.P.; Cox, B.D.; Erzinclioglu, S.W.; Walters, D.E.; Whichelow, M.J. Ventilatory function and winter fresh fruit consumption in a random sample of British adults. Thorax 1991, 46, 624–629. [Google Scholar] [CrossRef]
- Shaheen, S.O.; Jameson, K.A.; Syddall, H.E.; Aihie-Sayer, A.; Dennison, E.M.; Cooper, C.; Robinson, S.M.; Hertfordshire Cohort Study Group. The relationship of dietary patterns with adult lung function and COPD. Eur. Respir. J. 2010, 36, 277–284. [Google Scholar] [CrossRef] [PubMed]
- De Oca, M.M.; Tálamo, C.; Halbert, R.J.; Perez-Padilla, R.; Lopez, M.V.; Muiño, A.; Jardim, J.R.; Valdivia, G.; Pertuzé, J.; Moreno, D.; et al. Frequency of self-reported COPD exacerbation and airflow obstruction in five Latin American cities: The Proyecto Latinoamericano de Investigacion en Obstruccion Pulmonar (PLATINO) study. Chest 2009, 136, 71–78. [Google Scholar] [CrossRef]
- Amigo, H.; Bustos, P.; Zumelzu, E.; Rona, R.J. Cohort Profile: The Limache, Chile, birth cohort study. Int. J. Epidemiol. 2014, 43, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Oyarzun, M. Normal spirometric values in the Chilean population. Rev. Med. Chile 1996, 124, 1365–1367. [Google Scholar] [PubMed]
- Knudson, R.J.; Lebowitz, M.D.; Holberg, C.J.; Burrows, B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am. Rev. Respir. Dis. 1983, 127, 725–734. [Google Scholar] [PubMed]
- American Thoracic Society. Standardization of spirometry, 1994 update. Am. J. Respir. Crit. Care Med. 1994, 152, 1107–1136. [Google Scholar]
- Chilean Ministry of Health. Dietary Guidelines for Chile; Ministry of Health: Santiago, Chile, 1996. [Google Scholar]
- Pinheiro, A.C.; Fuentes, L.A. Sofnut (Software for Dietary Intake Analysis); Sofmatica, Ltd.: Santiago, Chile, 2002. [Google Scholar]
- Garcia, V.; Rona, R.J.; Chinn, S. Effect of the choice of food composition table on nutrient estimates: A comparison between the British and American (Chilean) tables. Public Health Nutr. 2004, 7, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Arts, I.C.; van de Putte, B.; Hollman, P.C. Catechin contents of foods commonly consumed in The Netherlands. 1. Fruits, vegetables, staple foods, and processed foods. J. Agric. Food Chem. 2000, 48, 1746–1751. [Google Scholar] [CrossRef] [PubMed]
- Corvalan, C.; Amigo, H.; Bustos, P.; Rona, R.J. Socioeconomic risk factors for asthma in Chilean young adults. Am. J. Public Health 2005, 95, 1375–1381. [Google Scholar] [CrossRef] [PubMed]
- Simes, R.J. An improved Bonferroni procedure for multiple tests of significance. Biometrika 1986, 73, 751–754. [Google Scholar] [CrossRef]
- Menezes, A.M.; Muiño, A.; López-Varela, M.V.; Valdivia, G.; Lisboa, C.; Jardim, J.R.; Montes de Oca, M.; Tálamo, C.; Wehrmeister, F.C.; Perez-Padilla, R.; et al. A population-based cohort study on chronic obstructive pulmonary disease in Latin America: Methods and preliminary results. The PLATINO Study Phase II. Arch. Bronconeumol. 2014, 50, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Shivappa, N.; Berthon, B.S.; Gibson, P.G.; Hebert, J.R. Dietary inflammatory index is related to asthma risk, lung function and systemic inflammation in asthma. Clin. Exp. Allergy 2015, 45, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Bentley, A.R.; Kritchevsky, S.B.; Harris, T.B.; Holvoet, P.; Jensen, R.L.; Newman, A.B.; Lee, J.S.; Yende, S.; Bauer, D.; Cassano, P.A.; et al. Dietary antioxidants and forced expiratory volume in 1 s decline: The Health, Aging and Body Composition study. Eur. Respir. J. 2012, 39, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Lago, J.H.; Toledo-Arruda, A.C.; Mernak, M.; Barrosa, K.H.; Martins, M.A.; Tibério, I.F.; Prado, C.M. Structure-activity association of flavonoids in lung diseases. Molecules 2014, 19, 3570–3595. [Google Scholar] [CrossRef] [Green Version]
- Tabak, C.; Arts, I.C.; Smit, H.A.; Heederik, D.; Kromhout, D. Chronic obstructive pulmonary disease and intake of catechins, flavonols, and flavones: The MORGEN Study. Am. J. Respir. Crit. Care Med. 2001, 164, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.; Yao, H.; Caito, S.; Hwang, J.W.; Arunachalam, G.; Rahman, I. Regulation of SIRT1 in cellular functions: Role of polyphenols. Arch. Biochem. Biophys. 2010, 501, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Caito, S.; Rajendrasozhan, S.; Cook, S.; Chung, S.; Yao, H.; Friedman, A.E.; Brookes, P.S.; Rahman, I. SIRT1 is a redox-sensitive deacetylase that is post-translationally modified by oxidants and carbonyl stress. FASEB J. 2010, 24, 3145–3159. [Google Scholar] [CrossRef] [PubMed]
- Rozowski, J.; Castillo, O. Is the Chilean diet a Mediterranean-type diet? Biol. Res. 2004, 37, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, F.; Lee, A.H.; Binns, C.W.; Hiramatsu, N.; Mori, M.; Nishimura, K. Dietary intake of isoflavones and polyunsaturated fatty acids associated with lung function, breathlessness and the prevalence of chronic obstructive pulmonary disease: Possible protective effect of traditional Japanese diet. Mol. Nutr. Food Res. 2010, 54, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Sharp, D.S.; Rodriguez, B.L.; Shahar, E.; Hwang, L.J.; Burchfiel, C.M. Fish consumption may limit the damage of smoking on the lung. Am. J. Respir. Crit. Care Med. 1994, 150, 983–987. [Google Scholar] [CrossRef] [PubMed]
- McKeever, T.M.; Lewis, S.A.; Cassano, P.A.; Ocké, M.; Burney, P.; Britton, J.; Smit, H.A. Patterns of dietary intake and relation to respiratory disease, forced expiratory volume in 1 s, and decline in 5-y forced expiratory volume. Am. J. Clin. Nutr. 2010, 92, 408–415. [Google Scholar] [CrossRef]
- Keranis, E.; Makris, D.; Rodopoulou, P.; Martinou, H.; Papamakarios, G.; Daniil, Z.; Zintzaras, E.; Gourgoulianis, K.I. Impact of dietary shift to higher-antioxidant foods in COPD: A randomised trial. Eur. Respir. J. 2010, 36, 774–780. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Larsen, V.; Amigo, H.; Bustos, P.; Bakolis, I.; Rona, R.J. Ventilatory Function in Young Adults and Dietary Antioxidant Intake. Nutrients 2015, 7, 2879-2896. https://doi.org/10.3390/nu7042879
Garcia-Larsen V, Amigo H, Bustos P, Bakolis I, Rona RJ. Ventilatory Function in Young Adults and Dietary Antioxidant Intake. Nutrients. 2015; 7(4):2879-2896. https://doi.org/10.3390/nu7042879
Chicago/Turabian StyleGarcia-Larsen, Vanessa, Hugo Amigo, Patricia Bustos, Ioannis Bakolis, and Roberto J. Rona. 2015. "Ventilatory Function in Young Adults and Dietary Antioxidant Intake" Nutrients 7, no. 4: 2879-2896. https://doi.org/10.3390/nu7042879
APA StyleGarcia-Larsen, V., Amigo, H., Bustos, P., Bakolis, I., & Rona, R. J. (2015). Ventilatory Function in Young Adults and Dietary Antioxidant Intake. Nutrients, 7(4), 2879-2896. https://doi.org/10.3390/nu7042879