Dietary Intakes and Nutritional Issues in Neurologically Impaired Children





Abstract
:1. Introduction
2. Nutritional Factors
2.1. Dietary Intake

{kind=link}
| Author-Year-Country | Population | Method | Main Findings |
|---|---|---|---|
| Thommessen M. et al. 1991, Norway [2] | Disabled children aged 1–16 years (n = 221) | Energy and nutrient intakes assessed with a 4-day food record. | Children with feeding problems or alternative feeding practices had lower energy and nutrient intakes than did children without these factors. |
| Hals J. et al. 1996, Norway [3] | Severely neurologically impaired children age range 2–13 years (n = 13) | Energy and nutrient intakes assessed with a 4-day food record. | Low dietary intakes of energy and of several nutrients with corresponding low hemoglobin values and serum values of ferritin, selenium and vitamins E and D in the study population. |
| Dahl M. et al. 1996, Norway [1] | Children with CP (n = 35, median age 8 years). | Parental interviews and medical records to assess feeding problems. | 60% of children (21/35) reported to have daily feeding problems. |
| Reilly S. et al. 1996, United Kingdom [13] | Children with CP (n = 49, median age range 12–72 months). | Parental interview and video recording of mealtime to assess feeding problems. | Sucking (57%) and swallowing (38%) problems common in the first 12 months of life. 80% of children fed non-orally at least on one occasion. |
| Hals J. et al. 2000, Norway [4] | Severely neurologically disabled children age range 2–13 years (n = 13) | Dietary intakes assessed with a 4-day food record. | Low intake of essential fatty acids (EFA) and low serum concentrations of several EFA compared to those of a reference group of children. |
| Sullivan P.B. et al. 2000, United Kingdom [5] | Children with cerebral palsy age range 4.2–13.1 years (n = 271) | Questionnaire regarding gastrointestinal and feeding problems | Feeding problems were prevalent: 89% needed help with feeding and 56% choked with food; 20% described feeding as stressful and unenjoyable. Prolonged feeding time was reported by 28%. |
| Gangil A. et al. 2001 [6] | Children with CP (n = 100, age range 1–9 years) | Feeding problems assessed by observing feeding session. | Oral motor dysfunction observed in all cases. Spastic quadriplegic CP and hypotonic patients had significantly lower feeding skill scores. Inability to self feed in 16% of cases, swallowing problems in 19% of cases, drooling in 20% of cases. |
| Kilpinen-Loisa P. et al. 2009, Finland [7] | Children with motor disabilities (n = 54, age range 5–15.5 years). | Parental interview to assess feeding problems. A 3-day food diary to assess nutrient intake. | 20% (11/54) reported to have feeding problems. Low intake of energy in 57% of cases, low intake of vitamin D on average 76% of recommendations, low intake of iron on average 87% of recommendations, poor intake of fiber on average only half of recommendations. |
| Hillesund E. et al. 2007, Norway [8] | Children with CP (n = 36, aged 1.5–17 years) | A 4-day food diary to assess micronutrient intake | Low intake of iron, folates, niacin, calcium, vitamin E and vitamin D was common even in those receiving nutritional supplements. |
| Grammatikopoulou M.G. et al. 2009, Greece [9] | Children with CP (n = 16, median age 10.1 ± 2.9 years) and their healthy siblings. | A 3-day food diary to assess nutrient intake. | Low energy intake in children with CP, covering 74.6% of their energy requirements. No differences in macronutrient distribution between CP children and healthy siblings. Subjects with CP had low vitamin A, biotin, folate, vitamin K, and copper intakes. |
| Calis E.A.C. et al. 2010, Netherlands [10] | Children with generalized cerebral palsy and intellectual disability (n = 176, median age 10 years). | A 7-day food diary to assess nutrient intakes. | Low intake of energy (62% of recommendations), calcium (87% of recommendations), vitamin A (77% of recommendations), vitamin D (73% of recommendations), vitamin B6 (13% of recommendations) and folates (78% of recommendations). |
| Walker J.L. et al. 2012, Australia [14] | Children with CP (n = 73, aged 2.8 ± 0.9 years), 16 typically developing children (TDC). | A validated 3-day weighed food record to assess nutrient intakes. | No significant differences in energy intakes between CP and TDC children. In CP group, considering for gross motor functional ability non-ambulant children had lower energy intakes compared to ambulant children (p < 0.01). Macronutrient composition of the diet was similar for all children. Protein intake was above the national recommended intake for all children. |
| Lopes P.A.C. et al. 2013, Brasil [11] | Children with CP (n = 90, age range 2–12.8 years). | Parental interview for feeding difficulties. A 24-h recall and food frequency questionnaire. | Prevalence of chewing and swallowing problems in children with spastic quadriplegia 41% and 12.8% respectively. Dietary pattern with low in carbohydrates (52%), adequate in protein (53%), and high in lipids (43%). Average energy intake below recommendations in children aged 9–13 years. |
| Sangermano M. et al. 2014, Italy [12] | Children with psychomotor developmental delay (n = 30, aged 2–15 years). | A 3-day food diary to quantify calorie and nutrient intake. | Low daily calorie intake in 43.3% of cases with unbalanced macronutrients: low in carbohydrates and high in lipids and protein (according to the Italian recommended daily intake of energy and nutrients). |
| Benfer K.A. et al. 2015, Australia [15] | Children with CP (n = 99, aged 18–36 months). | A 3-day weighed food record to assess dietary intake. | Energy intake of children decreased with poorer gross motor function. Food/fluid texture modifications occurred in 39% of cases and this proportion increased as gross motor function declined. Children on average had 50% of intake as fluid, which was most commonly unsafely swallowed. |
2.2. Micronutrient Deficiencies
2.3. Altered Energy Requirements
2.4. Gastrointestinal Disorders Affecting Nutrient Intake
2.5. Dysphagia
2.6. Gastroesophageal Reflux
2.7. Constipation
3. Non-Nutritional Factors
3.1. Intellectual Disability
3.2. Antiepileptic Therapy: Gastrointestinal Disturbances and Bone Disease
- -
- Gastrointestinal disturbances: Among the dose-dependent adverse effects of VPA, gastrointestinal disturbances have been described [57,58]. The main symptoms are feeding difficulties including anorexia and food refusal. Additionally, nausea, vomiting and dyspepsia secondary to gastric intolerance have been described and a single case of VPA-induced gastritis has been reported. More rarely, diarrhea, weight loss, abdominal cramps and constipation may also occur. The above-described gastrointestinal side effects may contribute to poor nutritional status in NI children.
- -
- Osteopenia: Children with neurological impairment are at increased risk for low bone mineral density (BMD) as a result of multifactorial etiology including poor dietary intake of calcium and vitamin D, poor sun-light exposure, muscular weakness, limited mobility, poor weight bearing and use of antiepileptic medications [59]. A growing body of evidence indicates that patients on long-term AEDs are at increased risk for metabolic bone disease including changes in bone turnover, osteoporosis, alterations in bone quality, and most importantly, fractures [60,61]. This issue is particularly important in pediatric age, as this is a critical periods for skeletal mineralization; peak bone mineral density is achieved by the end of adolescence and determines the risk for pathological fractures and osteoporosis later in life. In addition to antiepileptic treatment, patients with epilepsy are at increased risk for fractures secondary to seizure-related falls. As a matter of fact, fractures are reported to be two to six times more common in patients with epilepsy than in the general population [62]. Some AEDs (for example phenytoin, phenobarbital and carbamazepine) induce the hepatic enzyme cytochrome P-450 (CYP-450), increasing the catabolism of vitamin D and inducing a state of hypovitaminosis D with subsequent hyperparathyroidism, increased bone turnover and reduced bone density [48]. In addition, the use of non-enzyme inducing AEDs and polytherapy have been associated with vitamin D deficiency and osteopenia [63,64]. For example, long-term use of VPA is associated with bone metabolism abnormalities, which include reduced BMD and changes in bone turnover, with a dose-response relation. The effect of VPA cannot be explained by vitamin D metabolism, since VPA is not an inducer of CYP-450 system; it is instead thought to act by stimulating osteoclast activity and causing an imbalance between bone formation and reabsorption, hence contributing to bone loss [65]. The effects of the newer AEDs such as gabapentin, lamotrigine, levetiracetam, oxcarbazepine, topiramate and zonisamide on bone and calcium metabolism need to be better defined due to the limited number of studies conducted in this field.
4. Nutritional Assessment and Intervention
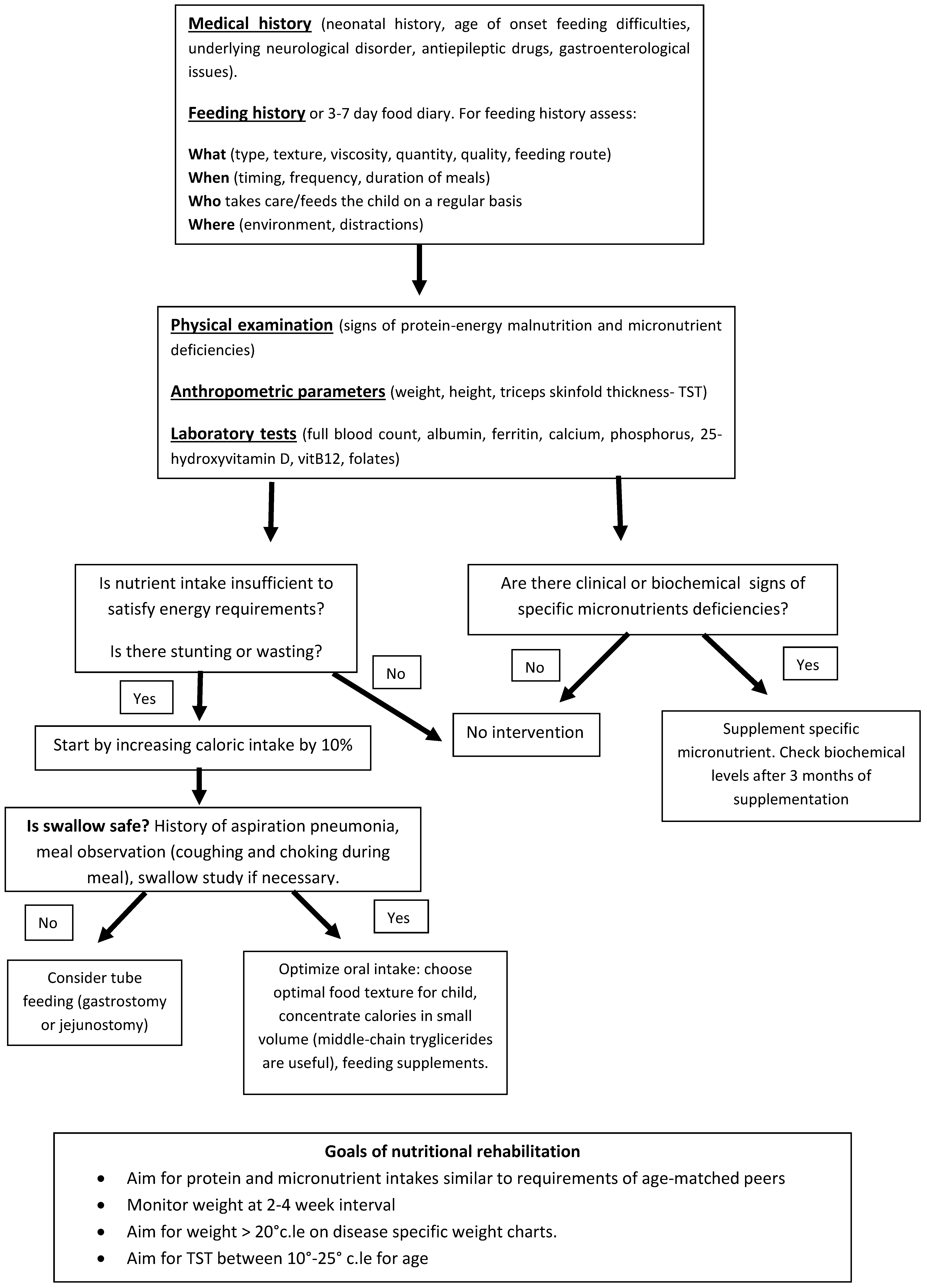
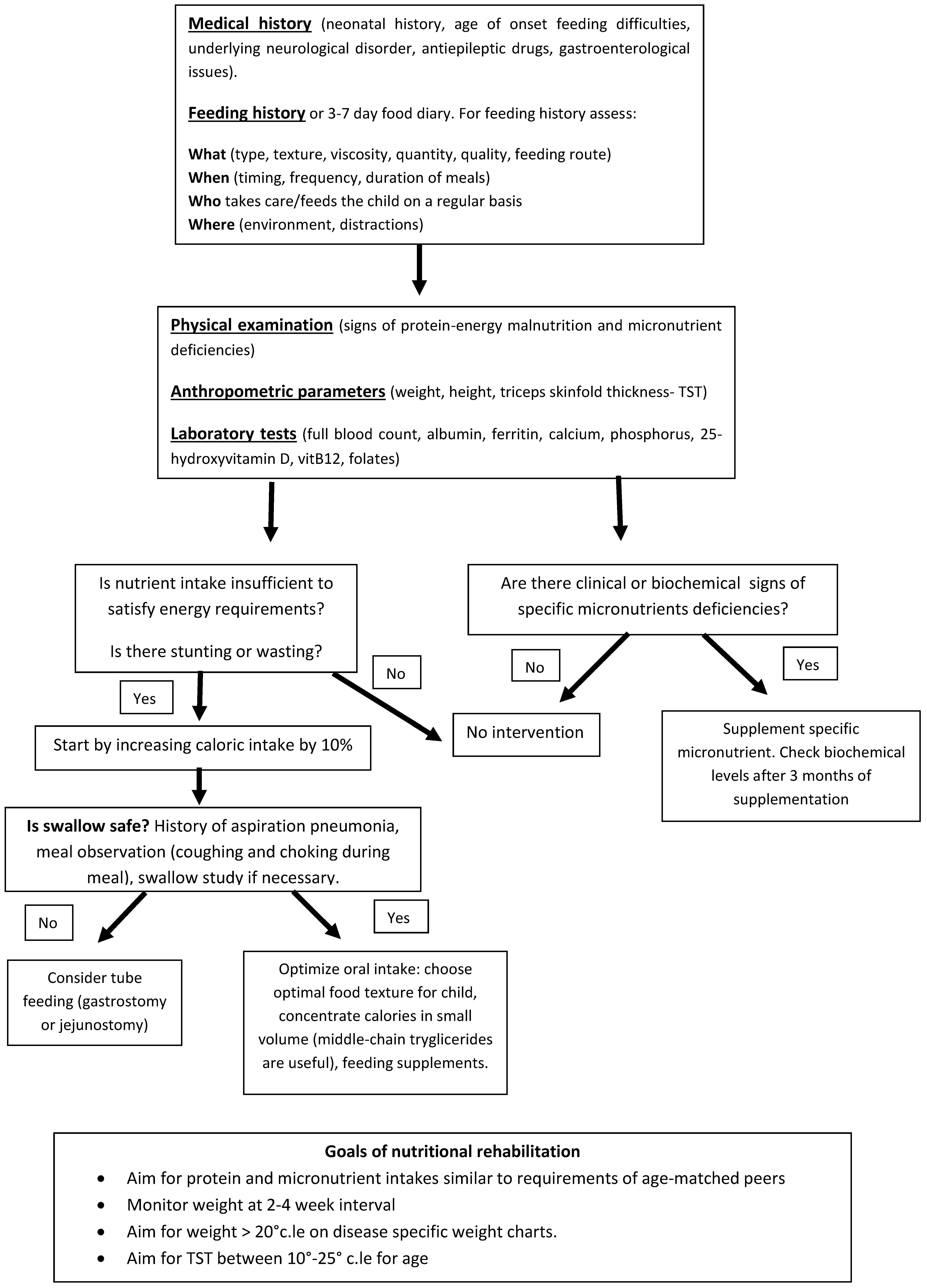
Nutritional Assessment and Intervention
- -
- Physical examination: Physical examination should search for signs of protein energy malnutrition and for signs of specific micronutrient deficiencies. Skin (color, level of hydration, rashes, decubitus ulcers) and distribution of subcutaneous fat should be accurately observed. Pallor can be suggestive for iron deficiency anemia, decubitus ulcers and poor subcutaneous fat can be suggestive for protein energy malnutrition. Tone and trophism of muscle masses, activity level and athetoid movements should be examined with attention and are important because they influence energy needs. Trophism of nails and hair are also important because they can suggest iron, zinc and copper deficiencies if severely dystrophic. The mouth should also be carefully inspected and specific attention given to the presence of ulcers and gingival bleeding, suggestive for micronutrient deficiencies (vitamin A and C) and to caries which are often present in children with CP due to difficulties in oral hygiene and to gastroesophageal reflux.
- -
- Anthropometrics and body composition. Measuring nutritional status can be challenging in NI children. Weight and height are often difficult to measure due to inability to stand, scoliosis or joint contractures of patients. Segmental measures are a reliable method for obtaining an estimated height for patients who cannot stand. Equations are available to calculate height from ulnar length, knee height and tibial length [66,67,68,69]. Wheelchair scales or weighing a child along with a parent and subtracting parental weights provide a reliable weight if a child cannot stand on a scale. Descriptive growth curves specific for children with gross motor impairment are available and are a reliable tool to assess whether a child is growing adequately, most important is to follow a child over time and make sure he/she is growing along his/her own growth curve [70]. Body mass index (BMI) or weight-for-height are frequently used to estimate nutritional status, yet they are poor predictors of body fat percentage. Additionally, BMI does not allow differentiation between lean and fat mass and has been shown to have only a low to moderate correlation with body fat in individuals with moderate to severe CP [71,72]. Knowledge on body composition is useful as it can help determine the requirement for nutritional intervention; some experts recommend that body composition be measured routinely in nutritional assessment of children with CP [73]. There is ongoing research to find safe, non-invasive, cost-effective, and valid methods to assess the body composition of children with CP. Dual-energy X-ray absorptiometry (DXA) is not always feasible in clinical practice due to cost constraints and availability. Simpler and less expensive methods to assess body composition include skinfold measurements and bioelectrical impedance assessment (BIA). Skinfold thicknesses, in particular triceps skinfold thickness, have long been considered important and valid measurements of subcutaneous fat. However, given a tendency of children with CP to store fat centrally, reduced peripheral skinfold thicknesses may not necessarily mean low fat stores and in addition, no skinfold reference curves specific for CP children are available [74]. Cerebral palsy specific equations have been developed by Gurka et al., these permit to estimate percentage of body fat from two skinfold measurements; their validity is currently being evaluated in ongoing studies [75]. Recently, Oeffinger et al. have shown that that BIA and two skinfold measurements (using CP specific equations) are accurate and non-invasive methods to estimate body fat percentage in children with CP [76].
- -
- Feeding history and nutrient intake: The most reliable method to assess dietary intake is by means of a seven-day feeding history collected by an experienced dietitian but this may not be always feasible and available in clinical practice. The majority of scientific literature on dietary intakes in CP children has used a three-day food diary. Recently, a modified three-day weighed food record for measuring energy intake has been validated for preschool-aged children with CP by Walker et al. [77]. Nevertheless, it must be noted that dietary histories and food records even though easy to perform, have some limitations for example they might not truly reflect the real dietary intakes of the subject. This is for two reasons, in first instance food diaries might not report the correct frequency and quantity of food consumed by the patient. Secondly, the food composition tables, which are used to calculate the specific macro- and micronutrients, are often inaccurate, in particular with regards to vitamins and minerals. When evaluating NI children for feeding problems, parents/caregivers should pay attention to the time needed to feed the child. If mealtimes last more than 30 min on a regular basis and/or mealtimes tend to be stressful for the child or parents, a referral for a more comprehensive feeding evaluation by a specialized feeding therapist might be useful. If during mealtimes respiratory symptoms such as coughing, choking, gagging, wet/gurgly respiration or rattly chest should occur, confirmation of swallowing impairment is useful with videofluoroscopic swallow study (VFSS). Adequate positioning and physical support, for example head support to avoid hyperextension or flexion, is important to ensure safety of the swallowing process. The feeding history should also take into account the modality of feeding (orally vs. tube feeding), the textures of food and thickness of fluids in the diet. Textures of food and thickness of fluids may need to be modified, to ensure airway safety, maximize eating efficiency and reduce fatigue during mealtimes. In case of tube feeding, the type of formula, the route of administration (gastric vs. jejunal), the quantity and tolerability should be assessed.
- -
- Laboratory tests: Blood tests are less reliable indicators of nutritional status, there is no single blood biomarker that can identify a status of calorie-protein malnutrition with good sensitivity and specificity. For example serum albumin concentrations are influenced by numerous non-nutritional factors such as inflammatory status (negative acute phase protein), hydration status, fluid distribution and hepatic function. It also has a long half-life (21 days) and hence its serum concentrations decrease slowly in case of malnutrition. Laboratory tests may be useful to identify specific micronutrient deficiencies for example a full blood count and ferritin levels can show iron deficiency anemia. Abnormal serum calcium, phosphorus, alkaline phosphatase and 25-hydroxyvitamin D levels may reflect poor bone mineral status.
- -
- Estimating nutritional requirements: Estimating the nutritional needs of NI children is challenging. Many children with CP have decreased energy requirements (ER) in comparison with neurologically normal children, and these tend to decrease with increasing severity of motor impairment. Energy needs of children with severe CP who are nonambulant have been reported to be between 60% and 70% of neurologically normal children [27,78,79,80]. Participation in physical and social activities may increase the energy requirements of children with CP and need to be taken into account when estimating ER. Equations to calculate ERs of NI children are available and have already been mentioned above [24,25,26]. Even though none of them is perfect and overestimation of ERs is frequent, the Krick method is one of the most reliable as it takes into account mobility, muscle tone, activity level, altered metabolism and growth [24].
- -
- Nutritional intervention: Nutritional intervention should always be tailored on the singular case according to ERs, degree of OPD, safety of swallowing and entity of malnutrition. According to North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition, the indications to start a nutritional intervention are as follows: evidence of oral motor feeding difficulties, undernutrition (weight-for-height <80% expected, BMI <5th percentile), growth failure (height-for-age <90% of expected), overweight (BMI >95th percentile), and individual nutrient deficiencies [81,82]. If oral intake is insufficient to promote weight gain and linear growth, if the amount of time spent to feed the child is excessive because of chewing and swallowing dysfunction, or if aspiration is a risk, enteral tube feeding should be considered. A gastrostomy tube is recommended for long-term enteral nutrition because it is more comfortable for the child and is less easily dislodged than a nasogastric tube. Gastrostomy feedings may promote weight gain, improve the child’s health, and reduce the time spent feeding the child [81,82]. With regards to specific nutrient requirements, unfortunately there are no evidence-based guidelines for nutrient allowances specific for NI children and there is no evidence to support increased protein, vitamin and mineral requirements in this population. The daily recommended intakes (DRI) for typically developing children can be used unless the child is severely undernourished [83]. In the latter case, Kuperminc et al. suggest that an intake of 2 g/kg per day of protein and an additional 15%–20% increase of calorie intake may be sufficient to guarantee “catch up growth” [84]. In addition, for micronutrients, standard recommendations of vitamins, minerals and trace elements can be followed with exception of vitamin D, given the increased risk of deficiency due to antiepileptic treatment and insufficient sunlight exposure. Even if there are no consistent clinical data to suggest a dose or formulation for vitamin D supplementation in this population, expert opinion of bone health specialists suggest that a higher daily requirement around 800–1000 UI of vitamin D is safe and should be considered in children with CP [85,86].
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dahl, M.; Thommessen, M.; Rasmussen, M.; Selberg, T. Feeding and nutritional characteristics in children with moderate or severe cerebral palsy. Acta Pediatr. 1996, 85, 697–701. [Google Scholar] [CrossRef]
- Thommessen, M.; Riis, G.; Kase, B.F.; Larsen, S.; Heiberg, A. Energy and nutrient intakes of disabled children: Do feeding problems make a difference? J. Am. Diet. Assoc. 1991, 12, 1522–1525. [Google Scholar]
- Hals, J.; Ek, J.; Svalastog, A.G.; Nilsen, H. Studies on nutrition in severely neurologically disabled children in an institution. Acta Paediatr. 1996, 12, 1469–1475. [Google Scholar] [CrossRef]
- Hals, J.; Bierve, K.S.; Nilsen, H.; Svalastog, A.G.; Ek, J. Essential fatty acids in the nutrition of severely neurologically disabled children. Br. J. Nutr. 2000, 83, 219–225. [Google Scholar] [PubMed]
- Sullivan, P.B.; Lambert, B.; Rose, M.; Ford-Adams, M.; Johnson, A.; Griffiths, P. Prevalence and severity of feeding and nutritional problems in children with neurological impairment: Oxford Feeding Study. Dev. Med. Child Neurol. 2000, 42, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Gangil, A.; Patwari, A.K.; Aneja, S.; Ahuja, B.; Anand, V.K. Feeding problems in children with cerebral palsy. Indian J. Pediatr. 2001, 38, 839–846. [Google Scholar]
- Kilpinen-Loisa, P.; Pihko, H.; Vesander, U.; Paganus, A.; Ritanen, U.; Mäkitie, O. Insufficient energy and nutrient intake in children with motor disability. Acta Paediatr. 2009, 98, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Hillesund, E.; Skranes, J.; Trygg, K.U.; Bøhmer, T. Micronutrient status in children with cerebral palsy. Acta Paediatr. 2007, 96, 1195–1198. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, M.G.; Daskalou, E.; Tsigga, M. Diet, feeding practices, and anthropometry of children and adolescents with cerebral palsy and their siblings. Nutrition 2009, 25, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Calis, E.A.C.; Veugelers, R.; Rieken, R.; Tibboel, D.; Evenhuis, H.M. Energy intake does not correlate with nutritional state in children with severe generalized cerebral palsy and intellectual disability. Clin. Nutr. 2010, 29, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Lopes, P.A.C.; Amancio, O.M.S.; Araùjo, R.F.C.; Vitalle, M.S.D.S.; Braga, J.A.P. Food pattern and nutritional status of children with cerebral palsy. Rev. Paul. Pediatr. 2013, 31, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Sangermano, M.; D’aniello, R.; Massa, G.; Albano, R.; Piano, R.; Budetta, M.; Scuccimarra, G.; Papa, E.; Coppola, G.; Vaijro, P. Nutritional problems in children with neuromotor disabilities: An Italian case series. Ital. J. Pediatr. 2014, 40, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Reilly, S.; Skuse, D.; Poblete, X. Prevalence of feeding problems and oral motor dysfunction in children with cerebral palsy: A community survey. J. Pediatr. 1996, 129, 877–882. [Google Scholar] [CrossRef]
- Walker, J.L.; Bell, K.L.; Steveneson, R.D.; Weir, K.A.; Boyd, R.N.; Davies, P.S.W. Relationship between Dietary Intake and Body Composition according to Gross Motor Functional Ability in Preschool-Aged Children with Cerebral Palsy. Ann. Nutr. Metable 2012, 61, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Benfer, K.A.; Weir, K.A.; Bell, K.L.; Ware, R.S.; Davies, P.S.W.; Boyd, R.N. Food and fluid texture consumption in a population-based cohort of preschool children with cerebral palsy: Relationship to dietary intake. Dev. Med. Child Neurol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Aggarwal, A.; Chillar, N.; Faridi, M.M. Comparison of micronutrient levels in children with cerebral palsy and neurologically normal controls. Indian J. Pediatr. 2015, 82, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, R.; Gelio, S.; Fratucello, A.; Valletta, E. Risk of low micronutrient intake in neurologically disabled children artificially fed. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, A.; Ntaios, G.; Kaifa, G.; Girtovitis, F.; Saouli, Z.; Kontoninas, Z.; Diamantidis, M.D.; Savopoulos, C.; Hatzitolios, A. Increased incidence of iron deficiency anemia secondary to inadequate iron intake in institutionalized, young patients with cerebral palsy. Int. J. Hematol. 2008, 88, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Etani, Y.; Nishimoto, Y.; Kawamoto, K.; Yamada, H.; Shouji, Y.; Kawahara, H.; Ida, S. Selenium deficiency in children and adolescents nourished by enteral nutrition and/or selenium-deficient enteral formula. J. Trace Elem. Med. Biol. 2014, 28, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Castro-Gago, M.; Eiris-Punal, J.; Novo-Rodriguez, M.I.; Couceiro, J.; Camina, F.; Rodriguez-Segade, S. Serum carnitine levels in epileptic children before and during treatment with valproic acid, carbamazepine, and phenobarbital. J. Child Neurol. 1998, 13, 546–549. [Google Scholar] [CrossRef] [PubMed]
- Verrotti, A.; Greco, R.; Morgese, G.; Chiarelli, F. Carnitine deficiency and hyperammoniemia in children receiving valproic acid with and without other anticonvulsant drugs. Int. J. Clin. Lab. Res. 1999, 29, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Coulter, D.L. Carnitine deficiency in epilepsy: Risk factors and treatment. J. Child Neurol. 1995, 10, S32–S39. [Google Scholar] [PubMed]
- Fukada, M.; Kawabe, M.; Takehara, M.; Iwano, S.; Kuwabara, K.; Kiku, C.; Wakamoto, H.; Morimoto, T.; Suzuki, Y.; Ishii, E. Carnitine deficiency: Risk factors and incidence in children with epilepsy. Brain Dev. 2015, 37, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Krick, J.; Murphy, P.E.; Markham, J.F.; Shapiro, B.K. A proposed formula for calculating energy needs of children with cerebral palsy. Dev. Med. Child Neurol. 1992, 34, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Rieken, R.; van Goudoever, J.B.; Schierbeek, H.; Willemsen, S.P.; Calis, E.A.C.; Tibboel, D.; Evenhuis, H.M.; Penning, C. Measuring body composition and energy expenditure in children with severe neurological impairment and intellectual disability. Am. J. Clin. Nutr. 2011, 94, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar] [PubMed]
- Walker, J.L.; Bell, K.L.; Boyd, R.N.; Davies, P.S.W. Energy requirements in preschool-age children with cerebral palsy. Am. J. Clin. Nutr. 2012, 96, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, P.B.; McInture, E. Gastrointestinal problems in disabled children. Cur. Paediatr. 2005, 15, 347–353. [Google Scholar] [CrossRef]
- Sullivan, P.B. Gastrointestinal disorders in children with neurodevelopmental disabilities. Dev. Dis. Res. Rev. 2008, 14, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, E.; Staiano, A.; Capano, G.; Romano, A.; Florimonet, L.; Miele, E.; Ciarla, C.; Campanozzi, A.; Crisanti, A.F. Gastrointestinal manifestations in children with cerebral palsy. Brain Dev. 1999, 21, 307–311. [Google Scholar] [CrossRef]
- Reilly, S. Feeding problems in children with cerebral palsy. Lancet 1990, 335, 1253–1254. [Google Scholar] [CrossRef]
- Morgan, A.T. Dysphagia in childhood traumatic brain injury: A reflection on the evidence and its implications for practice. Dev. Neurorehabil. 2010, 13, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Cornwell, P.L.; Murdoch, B.E.; Ward, E.C.; Morgan, A. Dysarthria and dysphagia following treatment for a fourth ventricle choroid plexus papilloma. J. Clin. Neurosci. 2003, 10, 506–512. [Google Scholar] [CrossRef]
- Faulks, D.; Collado, V.; Mazille, M.N.; Veyrune, J.L.; Hennequin, M. Masticatory dysfunction in persons with Down's syndrome. Part 1: Aetiology and incidence. J. Oral Rehabil. 2008, 35, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Morton, R.E.; Bonas, R.; Minford, J.; Kerr, A.; Ellis, R.E. Feeding ability in Rett syndrome. Dev. Med. Child Neurol. 1997, 39, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, J.S.; Murdock, M.; Lane, J.; Percy, A.K. Eating difficulties in girls with Rett syndrome compared with other developmental disabilities. J. Am. Diet. Assoc. 2003, 103, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Philpot, J.; Bagnall, A.; King, C.; Dubowitz, V.; Muntoni, F. Feeding problems in merosin deficient congenital muscular dystrophy. Arch. Dis. Child 1999, 80, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Parkes, J.; Hill, N.; Platt, M.J.; Donnelly, C. Oromotor dysfunction and communication impairments in children with cerebral palsy: A register study. Dev. Med. Child Neurol. 2010, 52, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Calis, E.A.; Veugelers, R.; Sheppard, J.J.; Tibboel, D.; Evenhuis, H.M.; Penning, C. Dysphagia in children with severe generalized cerebral palsy and intellectual disability. Dev. Med. Child Neurol. 2008, 50, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Casaer, P.; Daniels, H.; Devlieger, J.; DeCock, P.; Eggermont, E. Feeding behavior in preterm neonates. Early Hum. Dev. 1982, 7, 331–336. [Google Scholar] [CrossRef]
- Arvedson, J.C. Feeding children with cerebral palsy and swallowing difficulties. Eur. J. Clin Nutr. 2013, 67, S9–S12. [Google Scholar] [CrossRef] [PubMed]
- Fung, E.B.; Samson-Fang, L.; Stallings, V.A.; Conaway, M.; Liptak, G.; Henderson, R.C.; Worley, G.; O’Donnell, M.; Calvert, R.; Rosenbaum, P.; et al. Feeding dysfunction is associated with poor growth and health status in children with cerebral palsy. J. Am. Diet. Assoc. 2002, 102, 361–373. [Google Scholar] [CrossRef]
- Ortega Ade, O.; Ciamponi, A.L.; Mendes, F.M.; Santos, M.T. Assessment scale of the oral motor performance of children and adolescents with neurological damages. J. Oral Rehabil. 2009, 36, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, S.; Basar, P.; Gisel, E.G. Assessment of feeding performance in patients with cerebral palsy. Int. J. Rehabil. Res. 2004, 27, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Erkin, G.; Culha, C.; Ozel, S.; Kirbiyik, E.G. Feeding and gastrointestinal problems in children with cerebral palsy. Int. J. Rehabil. Res. 2010, 33, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Lang, M.B.; Moretti, E.; Sellari-Franceschin, I.; Orazini, L.; Cipriani, P.; Cioni, G.; Battini, R. A proposed multidisciplinary approach for identifying feeding abnormalities in children with cerebral palsy. J. Child Neurol. 2012, 27, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Benfer, K.A.; Weir, K.A.; Bell, K.L.; Ware, R.S.; Davies, P.S.W.; Boyd, R.N. Oropharyngeal dysphagia and gross motor skills in children with cerebral palsy. Pediatrics 2013, 131, e1553–e1562. [Google Scholar] [CrossRef] [PubMed]
- Benfer, K.A.; Weir, K.A.; Bell, K.L.; Ware, R.S.; Davies, P.S.W.; Boyd, R.N. Oropharyngeal dysphagia in preschool children with cerebral palsy: Oral phase impairments. Res. Dev. Dis. 2014, 35, 3469–3481. [Google Scholar] [CrossRef] [PubMed]
- Benfer, K.A.; Weir, K.A.; Bell, K.L.; Ware, R.S.; Davies, P.S.W.; Boyd, R.N. Clinical signs suggestive of pharyngeal dysphagia in preschool children with cerebral palsy. Res. Dev. Dis. 2015, 38, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Arvedson, J.C.; Rogers, B.; Buck, G.; Smart, P.; Msall, M. Silent aspiration prominent in children with dysphagia. Int. J. Pedatr. Otorhinolaryngol. 1994, 28, 173–181. [Google Scholar] [CrossRef]
- Ravelli, A.M.; Milla, P.J. Vomiting and gastroesophageal motor activity in children with disorders of the central nervous system. J. Pediatr. Gastroenterol. Nutr. 1998, 26, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Sondheimer, J.M.; Morris, B.A. Gastroesophageal reflux among severely retarded children. J. Pediatr. 1979, 94, 710–714. [Google Scholar] [CrossRef]
- Veugelers, R.; Benninga, M.A.; Calis, E.A.; Willemsen, S.P.; Evenhuis, H.; Tibboel, D.; Penning, C. Prevalence and clinical presentation of constipation in children with severe generalized cerebral palsy. Dev. Med. Child Neurol. 2010, 52, e216–e221. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Lastres, J.; Eiris-Punal, J.; Otero-Cepeda, J.L.; Pavon-BellinchÓn, P.; Castro-Gago, M. Nutritional status of mentally retarded children in north-west Spain. I. Anthropometric indicators. Acta Paediatr. 2003, 92, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Thommenssen, M.; Heideberg, A.; Kase, B.F.; Larsen, S.; Riis, G. Feeding problems, height and weight in different groups of disabled children. Acta Pediatr. Scand. 1991, 80, 527–533. [Google Scholar] [CrossRef]
- Gouge, A.L.; Ekvall, S.W. Diets of handicapped children: Physical, psychological and socioeconomic correlation. Am. J. Ment. Defic. 1975, 80, 149–157. [Google Scholar] [PubMed]
- Perrucca, E. Pharmacological and Therapeutic Properties of Valproate. A Summary after 35 Years of Clinical Experience. CNS Drugs 2002, 16, 695–714. [Google Scholar] [CrossRef]
- Gerstner, T.; Bell, N.; König, S. Oral valproic acid for epilepsy- long-term experience in therapy and side effects. Expert Opin. Pharmacother. 2008, 9, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Shellhaas, E.A.; Joshi, S.M. Vitamin D and Bone Health Among Children with Epilepsy. Pediatr. Neurol. 2010, 42, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Verrotti, A.; Coppola, G.; Parisi, P.; Mohn, A.; Chiarelli, F. Bone and calcium metabolism and antiepileptic drugs. Clin. Neurol. Neurosurg. 2010, 112, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Samaniego, E.A.; Sheth, R.D. Bone consequences of epilepsy and antiepileptic medications. Semin. Pediatr. Neurol. 2007, 14, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Souverein, P.C.; Webb, D.J.; Petri, H.; Weil, J.; van Staa, T.P.; Egberts, A.C. Incidence of fractures among epilepsy patients: A population-based retrospective color study in the General Practice Research Database. Epilepsia 2005, 46, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Verrotti, A.; Greco, R.; Latini, G.; Morgese, G.; Chiarelli, F. Increased bone turnover in prepubertal, pubertal, and postpubertal patients receiving carbamazepine. Epilepsia 2002, 43, 1488–1492. [Google Scholar] [CrossRef] [PubMed]
- Sheth, R.D.; Wesolowski, C.A.; Jacob, J.C.; Penney, S.; Hobbs, G.R.; Riggs, J.E.; Bodensteiner, J.B. Effect of carbamazepine and valproate on bone mineral density. J. Pediatr. 1995, 127, 256–262. [Google Scholar] [CrossRef]
- Sato, Y.; Kondo, I.; Ishida, S.; Motooka, H.; Takayama, K.; Tomita, Y.; Maeda, H.; Satoh, K. Decreased bone mass and increased bone turnover with valproate therapy in adult epilepsy. Neurology 2001, 57, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Gauld, L.M.; Kappers, J.; Carlin, J.B.; Robertson, C.F. Height prediction from ulna length. Dev. Med. Child Neurol. 2004, 46, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.D. Use of segmental measures to estimate stature in children with cerebral palsy. Arch. Pediatr. Adolesc. Med. 1995, 149, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Chumlea, W.C.; Guo, S.S.; Steinbaugh, M.L. Prediction of stature from knee height for black and white adults and children with application to mobility- impaired or handicapped èpersosn. J. Am. Diet. Assoc. 1994, 94, 1385–1388. [Google Scholar] [CrossRef]
- Hogan, S.E. Knee height as predictor of recumbent length for individuals with mobility-impaired cerebral palsy. J. Am. Coll. Nutr. 1999, 18, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.; Day, S.; Shavelle, R.; Strauss, D. Low weight, morbidity, and mortality in children with cerebral palsy: New clinical growth charts. Pediatrics 2011, 128, e299–e307. [Google Scholar] [CrossRef] [PubMed]
- Kuperminc, M.N.; Gurka, M.J.; Bennis, J.A.; Busby, M.G.; Grossberg, R.I.; Henderson, R.C.; Stevenson, R.D. Anthropometric measures: Poor predictors of body fat in children with moderate to severe cerebral palsy. Dev. Med. Child Neurol. 2010, 52, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Zemel, B.S.; Riley, E.M.; Stallings, V.A. Evaluation of methodology for nutritional assessment in children: Anthropometry, body composition, and energy expenditure. Annu. Rev. Nutr. 1997, 17, 211–235. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, P. Measurement of body composition should become routine in nutritional assessment of children with cerebral palsy. Dev. Med. Child Neurol. 2015, 57, 793–794. [Google Scholar] [CrossRef] [PubMed]
- Addo, O.Y.; Himes, J.H. Reference curves for triceps and subscapular skinfold thicknesses in US children and adolescents. Am. J. Clin. Nutr. 2010, 91, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Gurka, M.J.; Kuperminc, M.N.; Busby, M.G.; Bennis, J.A.; Grossberg, R.I.; Houlihan, C.M.; Stevenson, R.D.; Henderson, R.C. Assessment and correction of skinfold thickness equations in estimating body fat in children with cerebral palsy. Dev. Med. Child Neurol. 2010, 52, e35–e41. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, D.J.; Gurka, M.J.; Kuperminc, M.; Hassani, S.; Buhr, N.; Tylkowski, C. Accuracy of skinfold and bioelectrical impedance assessments of body fat percentage in ambulatory individuals with cerebral palsy. Dev. Med. Child Neurol. 2014, 56, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Bell, K.L.; Boyd, R.N.; Davies, P.S.W. Validation of a modified three-day weighed food record for measuring energy intake in preschool-aged children with cerebral palsy. Clin. Nutr. 2013, 32, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Stallings, V.A.; Zemel, B.S.; Davies, J.C.; Cronk, C.E.; Charney, E.B. Energy expenditure of children and adolescents with severe disabilities: A cerebral palsy model. Am. J. Clin. Nutr. 1996, 64, 627–634. [Google Scholar] [PubMed]
- Azcue, M.P.; Zello, G.A.; Levy, L.D.; Pencharz, P.B. Energy expenditure and body composition in children with spastic quadriplegic cerebral palsy. J. Pediatr. 1996, 129, 870–876. [Google Scholar] [CrossRef]
- Culley, W.J.; Middleton, T.O. Caloric requirements of mentally retarded children with and without motor dysfunction. J. Pediatr. 1969, 75, 380–384. [Google Scholar] [CrossRef]
- Motil, K.J. Enteral nutrition in the neurologically impaired child. In Pediatric Enteral Nutrition; Baker, S.B., Baker, R.D., Jr., et al., Eds.; Chapman & Hall: New York, NY, USA, 1994; pp. 217–237. [Google Scholar]
- Marchand, V.; Motil, K. Nutrition support for neurologically impaired children: A clinical report of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2006, 43, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Livelli di Assunzione di Riferimento di Nutrienti e di Energia per la popolazione italiana. Avaliable online: http://www.sinu.it/html/pag/tabelle_larn_2014_rev.asp (accessed on 18 September 2015).
- Kuperminc, M.N.; Gottrand, F.; Samson-Fang, L.; Arvedson, J.; Bell, K.; Craig, G.M.; Sullivan, P.B. Nutritional management of children with cerebral palsy: A practical guide. Eur. J. Clin. Nutr. 2013, 67, S21–S23. [Google Scholar] [CrossRef] [PubMed]
- Fehlings, D.; Switzer, L.; Agarwal, P.; Wong, C.; Sochett, E.; Stevenson, R.; Sonnenberg, L.; Smile, S.; Young, E.; Huber, J.; et al. Informing evidence-based clinical practice guidelines for children with cerebral palsy at risk of osteoporosis: A systematic review. Dev. Med. Child Neurol. 2012, 54, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Pacaud, D.; Petryk, A.; Collet-Solberg, P.F. Vitamin D deficiency in children and its management: Review of current knowledge and recommendations. Pediatrics 2008, 122, 398–417. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penagini, F.; Mameli, C.; Fabiano, V.; Brunetti, D.; Dilillo, D.; Zuccotti, G.V. Dietary Intakes and Nutritional Issues in Neurologically Impaired Children. Nutrients 2015, 7, 9400-9415. https://doi.org/10.3390/nu7115469
Penagini F, Mameli C, Fabiano V, Brunetti D, Dilillo D, Zuccotti GV. Dietary Intakes and Nutritional Issues in Neurologically Impaired Children. Nutrients. 2015; 7(11):9400-9415. https://doi.org/10.3390/nu7115469
Chicago/Turabian StylePenagini, Francesca, Chiara Mameli, Valentina Fabiano, Domenica Brunetti, Dario Dilillo, and Gian Vincenzo Zuccotti. 2015. "Dietary Intakes and Nutritional Issues in Neurologically Impaired Children" Nutrients 7, no. 11: 9400-9415. https://doi.org/10.3390/nu7115469
APA StylePenagini, F., Mameli, C., Fabiano, V., Brunetti, D., Dilillo, D., & Zuccotti, G. V. (2015). Dietary Intakes and Nutritional Issues in Neurologically Impaired Children. Nutrients, 7(11), 9400-9415. https://doi.org/10.3390/nu7115469