Association between Dietary Vitamin A Intake and the Risk of Glioma: Evidence from a Meta-analysis

Abstract
:1. Introduction
2. Methods
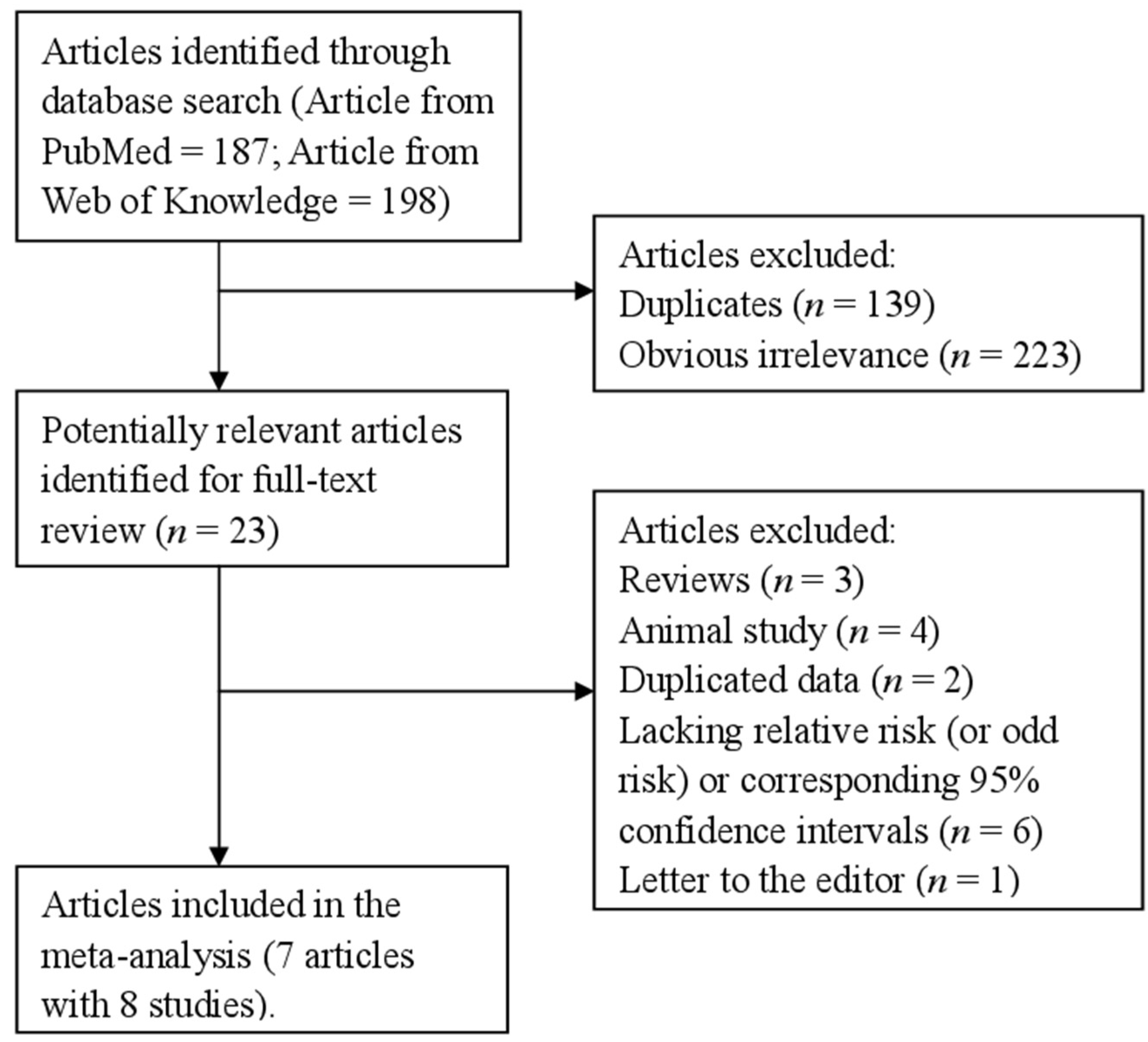
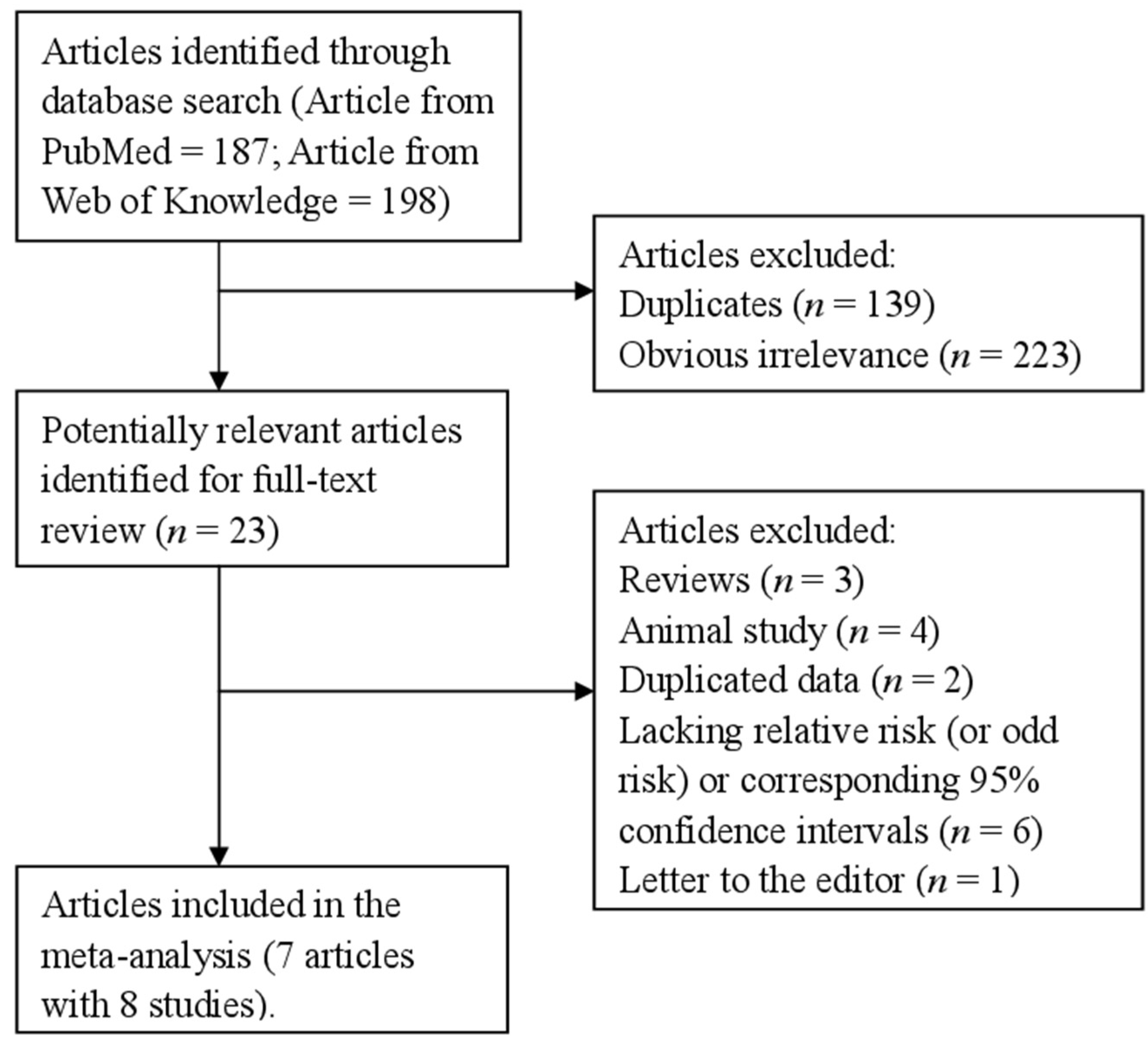
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
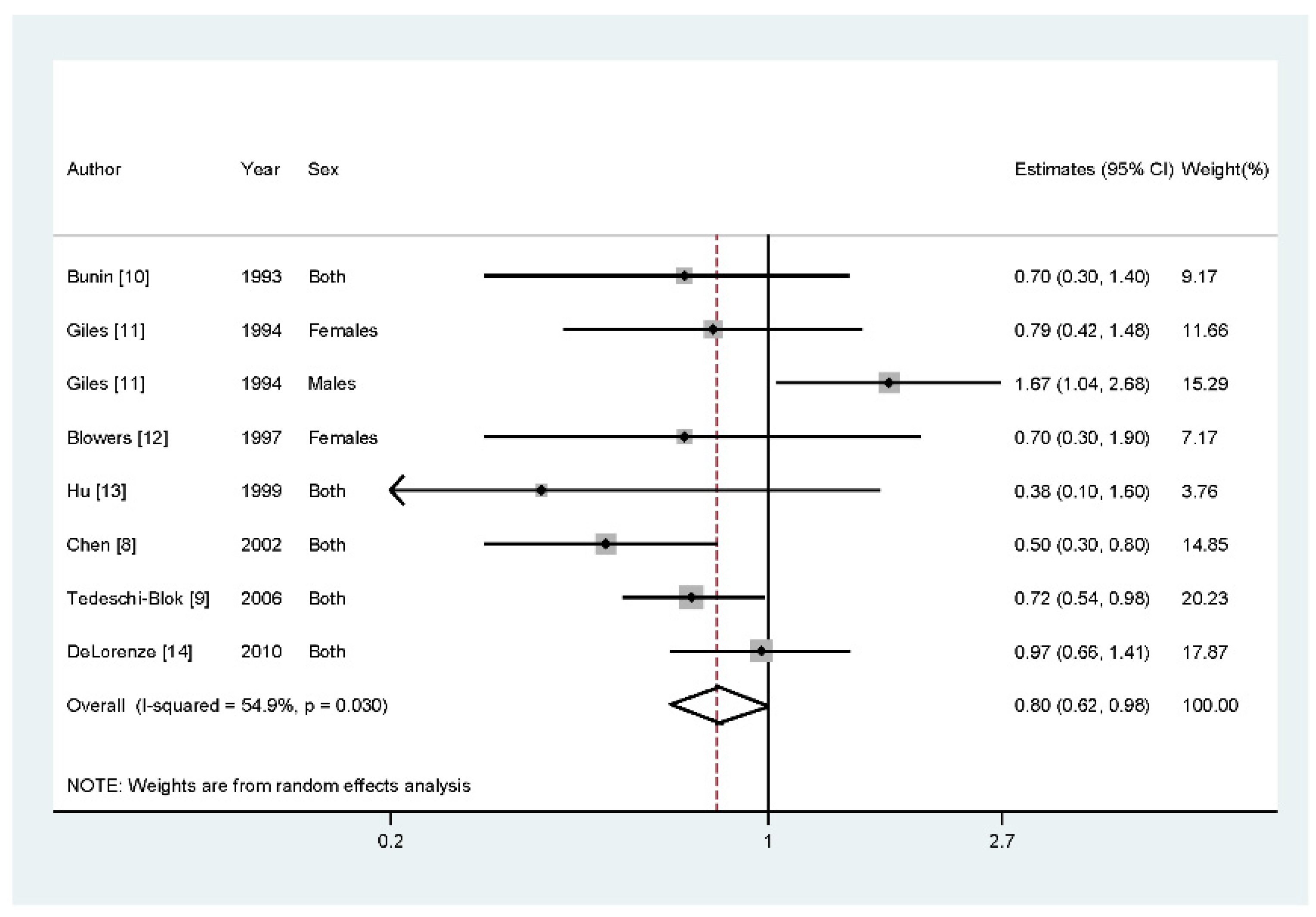
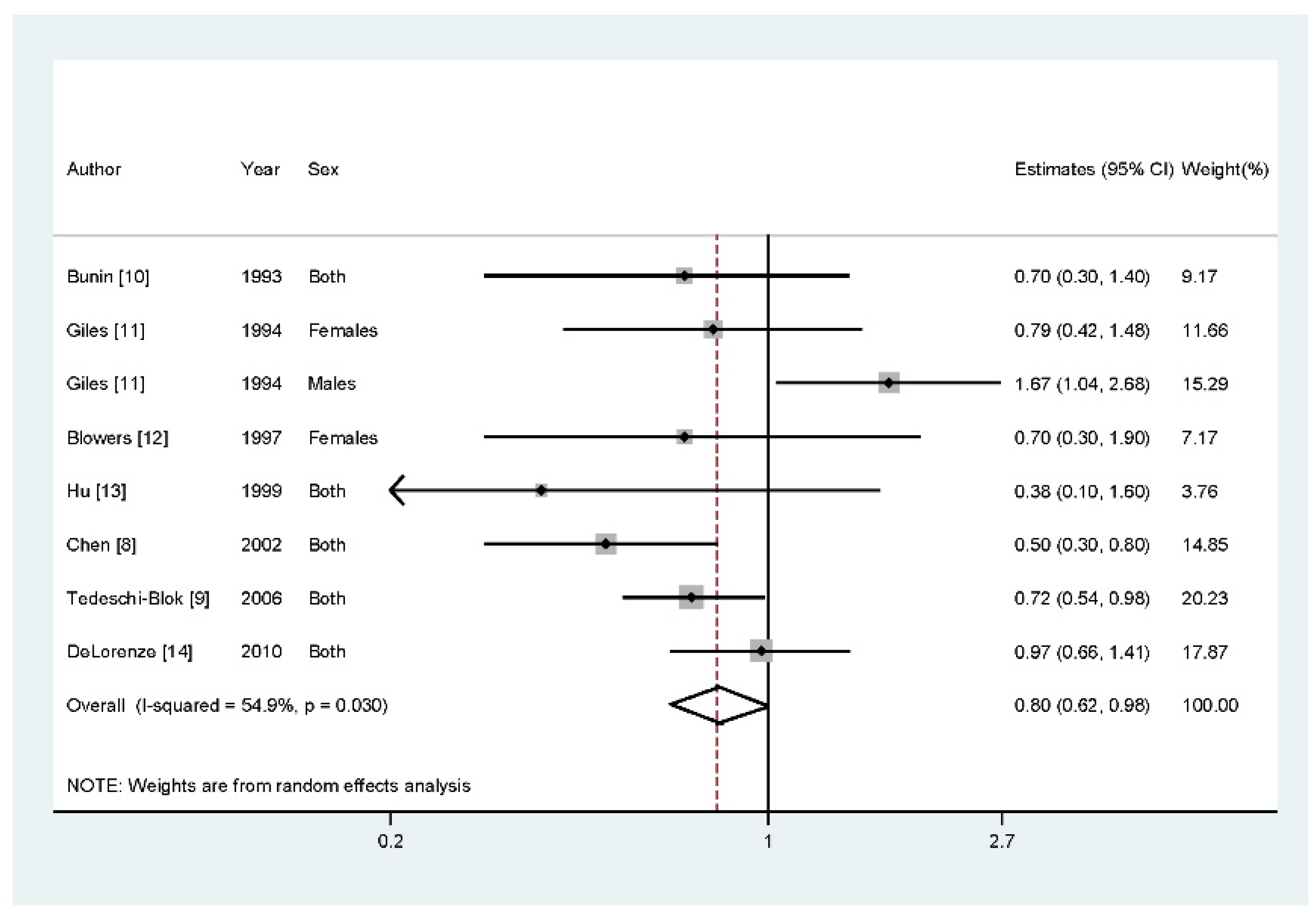
3.2. Vitamin A and Glioma
3.3. Meta-Regression
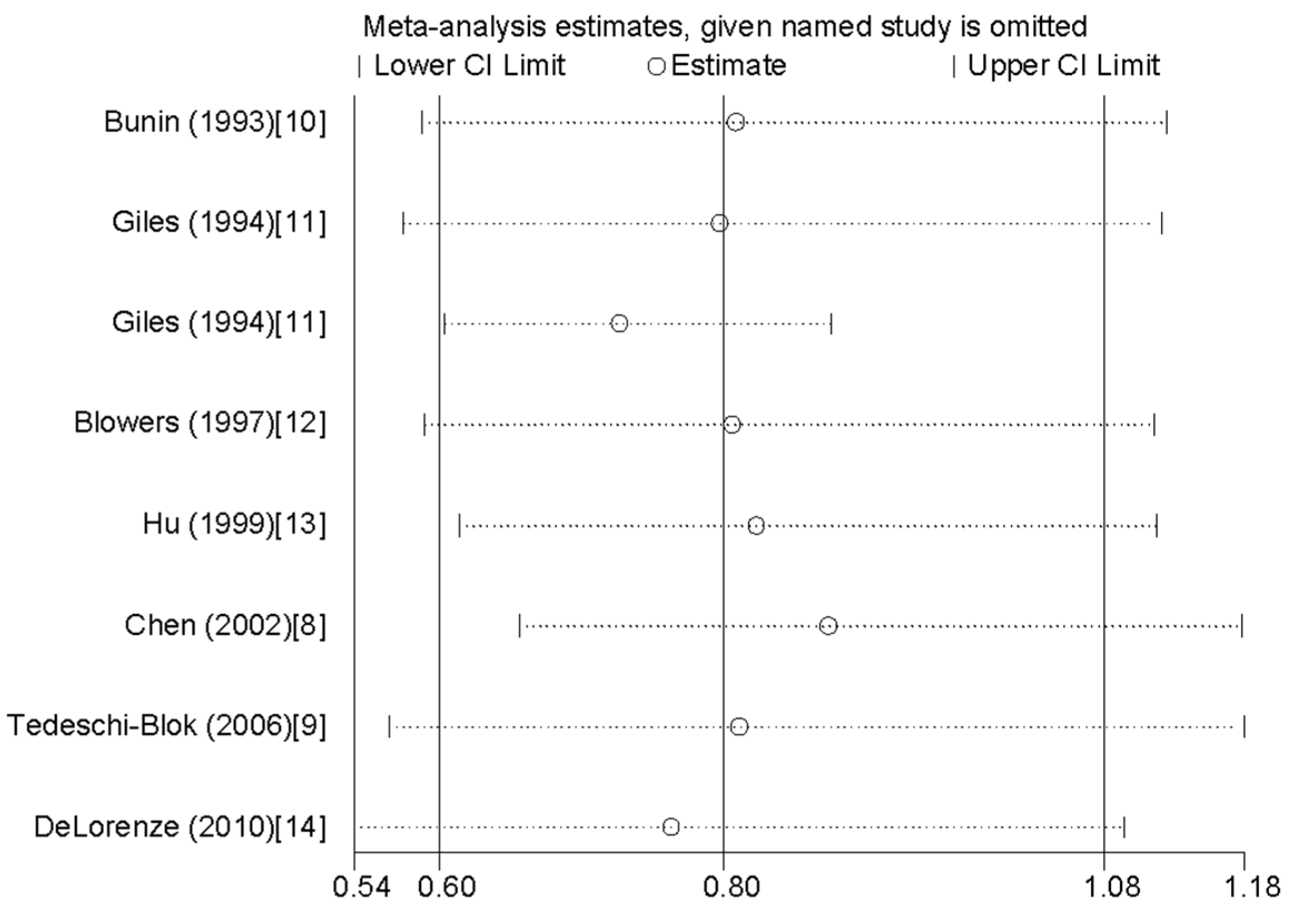
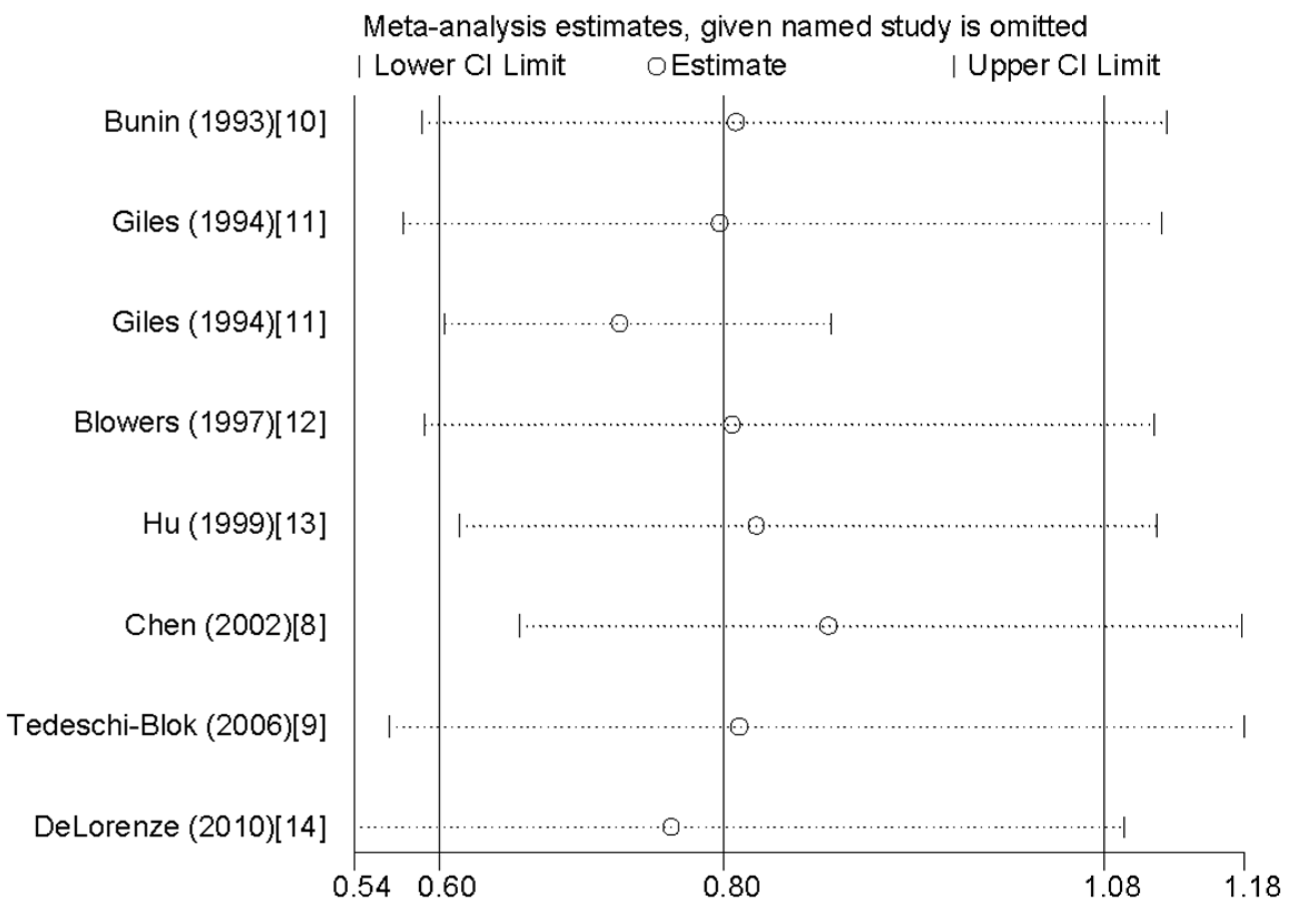
3.4. Influence Analysis and Publication Bias

{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Country | Study Design | Cases, Age (year) | Comparison Groups | Dietary Assessment | RR (95% CI) for Highest versus Lowest Category | Adjustment or Matched for |
|---|---|---|---|---|---|---|---|
| Bunin et al. 1994 [10] | United States | Case-control (PCC) | 155, <6 | Quartile 4 vs. Quartile 1 | FFQ | 0.70 (0.30–1.40) | Adjusted for income level. |
| Giles et al. 1994 [11] | Australia | Case-control (PCC) | 416, 20–70 | Tertile 3 vs. Tertile1 | FFQ | Females: 0.79 (0.42–1.48); Males: 1.67 (1.04–2.68) | Adjusted for alcohol and tobacco. |
| Blowers et al. 1997 [12] | United States | Case-control (PCC) | 94, 25–74 | Quartile 4 vs. Quartile 1 | FFQ | 0.70 (0.30–1.90) | Matched the patient on age (within five years) and race (Black or White). |
| Hu et al. 1999 [13] | China | Case-control (HCC) | 73, 20–74 | Quartile 4 vs. Quartile 1 | FFQ | 0.38 (0.10–1.60) | Matched to each case by sex, age within five-year intervals and area of residence (same or adjacent city and country). |
| Chen et al. 2002 [8] | United States | Case-control (PCC) | 236, ≥21 | Quartile 4 (mean = 5078) vs. Quartile 1 (mean = 1269.5) | FFQ | 0.50 (0.30–0.80) | Adjusting for age, age squared, gender, total energy intake, respondent type, education level, family history, and farming experience. |
| Tedeschi-Blok et al. 2006 [9] | United States | Case-control (PCC) | 802, ≥20 | Quartile 4 (mean = 5512) vs. Quartile 1 (mean = 1378) | FFQ | 0.72 (0.54–0.98) | Adjusted for age, gender, ethnicity, SES, total calories, and supplement use |
| DeLorenze et al. 2010 [14] | United States | Case-control (PCC) | 72, ≥20 | Tertile 3 (mean = 3757.6) vs. Tertile 1 (mean = 257.7) | FFQ | 0.97 (0.66–1.41) | Adjusted for reporting status, age at diagnosis, treatment, education, marital status, total calories, pack years, and age at alcoholic drink. |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
| Covariates | p-Value |
|---|---|
| Publication year | 0.185 |
| Geographic locations | 0.294 |
| Number of cases | 0.386 |
| Source of controls | 0.815 |
References
- Ricard, D.; Idbaih, A.; Ducray, F.; Lahutte, M.; Hoang-Xuan, K.; Delattre, J.Y. Primary brain tumours in adults. Lancet 2012, 379, 1984–1996. [Google Scholar] [CrossRef]
- Wen, P.Y.; Kesari, S. Malignant gliomas in adults. N. Engl. J. Med. 2008, 359, 492–507. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Wang, X.; Tan, Y.; Qiu, L.; Fang, H.; Li, W. Association between vitamin C intake and glioma risk: Evidence from a meta-analysis. Neuroepidemiology 2015, 44, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Wang, M.; Zhang, T.; Zhang, S. Vitamin E intake is not associated with glioma risk: Evidence from a meta-analysis. Neuroepidemiology 2014, 43, 253–258. [Google Scholar] [CrossRef] [PubMed]
- D’Archivio, M.; Santangelo, C.; Scazzocchio, B.; Vari, R.; Filesi, C.; Masella, R.; Giovannini, C. Modulatory effects of polyphenols on apoptosis induction: Relevance for cancer prevention. Int. J. Mol. Sci. 2008, 9, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Khoshyomn, S.; Nathan, D.; Manske, G.C.; Osler, T.M.; Penar, P.L. Synergistic effect of genistein and BCNU on growth inhibition and cytotoxicity of glioblastoma cells. J. Neurooncol. 2002, 57, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Pouliquen, D.; Olivier, C.; Hervouet, E.; Pedelaborde, F.; Debien, E.; Le Cabellec, M.T.; Gratas, C.; Homma, T.; Meflah, K.; Vallette, F.M.; et al. Dietary prevention of malignant glioma aggressiveness, implications in oxidant stress and apoptosis. Int. J. Cancer 2008, 123, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Ward, M.H.; Tucker, K.L.; Graubard, B.I.; McComb, R.D.; Potischman, N.A.; Weisenburger, D.D.; Heineman, E.F. Diet and risk of adult glioma in eastern Nebraska, United States. Cancer Causes Control 2002, 13, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi-Blok, N.; Lee, M.; Sison, J.D.; Miike, R.; Wrensch, M. Inverse association of antioxidant and phytoestrogen nutrient intake with adult glioma in the San Francisco Bay Area: A case-control study. BMC Cancer 2006, 6, 148. [Google Scholar] [CrossRef] [PubMed]
- Bunin, G.R.; Kuijten, R.R.; Boesel, C.P.; Buckley, J.D.; Meadows, A.T. Maternal diet and risk of astrocytic glioma in children: A report from the Childrens Cancer Group (United States and Canada). Cancer Causes Control 1994, 5, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Giles, G.G.; McNeil, J.J.; Donnan, G.; Webley, C.; Staples, M.P.; Ireland, P.D.; Hurley, S.F.; Salzberg, M. Dietary factors and the risk of glioma in adults: Results of a case-control study in Melbourne, Australia. Int. J. Cancer 1994, 59, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Blowers, L.; Preston-Martin, S.; Mack, W.J. Dietary and other lifestyle factors of women with brain gliomas in Los Angeles County (California, USA). Cancer Causes Control 1997, 8, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; La Vecchia, C.; Negri, E.; Chatenoud, L.; Bosetti, C.; Jia, X.; Liu, R.; Huang, G.; Bi, D.; Wang, C. Diet and brain cancer in adults: A case-control study in northeast China. Int. J. Cancer 1999, 81, 20–23. [Google Scholar] [CrossRef]
- DeLorenze, G.N.; McCoy, L.; Tsai, A.L.; Quesenberry, C.P., Jr.; Rice, T.; Il’yasova, D.; Wrensch, M. Daily intake of antioxidants in relation to survival among adult patients diagnosed with malignant glioma. BMC Cancer 2010, 10, 215. [Google Scholar] [CrossRef] [PubMed]
- Databases of PubMed. Available online: http://www.ncbi.nlm.nih.gov/pubmed (accessed on 1 April 2015).
- Web of Knowledge. Available online: http://apps.webofknowledge.com (accessed on 1 April 2015).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Controlling the risk of spurious findings from meta-regression. Stat. Med. 2004, 23, 1663–1682. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A. Assessing the in fluence of a single study in the meta-analysis estimate. Stata Tech. Bull. 1999, 8, 1–48. [Google Scholar]
- Li, Y. Association between fruit and vegetable intake and risk for glioma: A meta-analysis. Nutrition 2014, 30, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Adami, H.O. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 1765–1777. [Google Scholar] [CrossRef] [PubMed]
- Munafo, M.R.; Flint, J. Meta-analysis of genetic association studies. Trends Genet. 2004, 20, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Prentice, R.L. Dietary assessment and the reliability of nutritional epidemiology reports. Lancet 2003, 362, 182–183. [Google Scholar] [CrossRef]
- Campos, B.; Weisang, S.; Osswald, F.; Ali, R.; Sedlmeier, G.; Bageritz, J.; Mallm, J.P.; Hartmann, C.; von Deimling, A.; Popanda, O.; et al. Retinoid resistance and multifaceted impairment of retinoic acid synthesis in glioblastoma. Glia 2015, 63, 1850–1859. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.L.; Liu, S.; Cui, W.; Shi, Y.; Liu, Q.; Duan, J.J.; Yu, S.C.; Zhang, X.; Cui, Y.H.; Kung, H.F.; et al. Aldehyde dehydrogenase 1A1 circumscribes high invasive glioma cells and predicts poor prognosis. Am. J. Cancer Res. 2015, 5, 1471–1483. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lv, W.; Zhong, X.; Xu, L.; Han, W. Association between Dietary Vitamin A Intake and the Risk of Glioma: Evidence from a Meta-analysis. Nutrients 2015, 7, 8897-8904. https://doi.org/10.3390/nu7115438
Lv W, Zhong X, Xu L, Han W. Association between Dietary Vitamin A Intake and the Risk of Glioma: Evidence from a Meta-analysis. Nutrients. 2015; 7(11):8897-8904. https://doi.org/10.3390/nu7115438
Chicago/Turabian StyleLv, Wen, Xian Zhong, Lingmin Xu, and Weidong Han. 2015. "Association between Dietary Vitamin A Intake and the Risk of Glioma: Evidence from a Meta-analysis" Nutrients 7, no. 11: 8897-8904. https://doi.org/10.3390/nu7115438
APA StyleLv, W., Zhong, X., Xu, L., & Han, W. (2015). Association between Dietary Vitamin A Intake and the Risk of Glioma: Evidence from a Meta-analysis. Nutrients, 7(11), 8897-8904. https://doi.org/10.3390/nu7115438