

Impact of Flash Glucose Monitoring in Adults with Inherited Metabolic Disorders at Risk of Hypoglycemia

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Data Collection
2.4. Outcomes
2.5. Statistical Analysis
3. Results
Hypoglycemia and Safety
4. Case 1
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saudubray, J.-M.; Sedel, F.; Walter, J.H. Clinical Approach to Treatable Inborn Metabolic Diseases: An Introduction. J. Inherit. Metab. Dis. 2006, 29, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Quarta, A.; Iannucci, D.; Guarino, M.; Blasetti, A.; Chiarelli, F. Hypoglycemia in Children: Major Endocrine-Metabolic Causes and Novel Therapeutic Perspectives. Nutrients 2023, 15, 3544. [Google Scholar] [CrossRef] [PubMed]
- Douillard, C.; Mention, K.; Dobbelaere, D.; Wemeau, J.-L.; Saudubray, J.-M.; Vantyghem, M.-C. Hypoglycaemia Related to Inherited Metabolic Diseases in Adults. Orphanet J. Rare Dis. 2012, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Douillard, C.; Jannin, A.; Vantyghem, M.-C. Rare Causes of Hypoglycemia in Adults. Ann. Endocrinol. 2020, 81, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, D.A.; Steuerwald, U.; De Souza, C.F.M.; Derks, T.G.J. Inborn Errors of Metabolism with Hypoglycemia: Glycogen Storage Diseases and Inherited Disorders of Gluconeogenesis. Pediatr. Clin. N. Am. 2018, 65, 247–265. [Google Scholar] [CrossRef]
- Fronczyk, A.; Romanowska, H.; Majkowska, L. Rare causes of hypoglycemia in adults—Disorders of gluconeogenesis and fatty acid oxidation disorders. Pol. Merkur. Lek. Organ Pol. Tow. Lek. 2011, 30, 147–149. [Google Scholar]
- Mason, E.; Hindmarch, C.C.T.; Dunham-Snary, K.J. Medium-chain Acyl-COA Dehydrogenase Deficiency: Pathogenesis, Diagnosis, and Treatment. Endocrinol. Diabetes Metab. 2022, 6, e385. [Google Scholar] [CrossRef]
- Melis, D.; Rossi, A.; Pivonello, R.; Salerno, M.; Balivo, F.; Spadarella, S.; Muscogiuri, G.; Casa, R.D.; Formisano, P.; Andria, G.; et al. Glycogen Storage Disease Type Ia (GSDIa) but Not Glycogen Storage Disease Type Ib (GSDIb) Is Associated to an Increased Risk of Metabolic Syndrome: Possible Role of Microsomal Glucose 6-Phosphate Accumulation. Orphanet J. Rare Dis. 2015, 10, 91. [Google Scholar] [CrossRef]
- Dios-Fuentes, E.; Gonzalo Marin, M.; Remón-Ruiz, P.; Benitez Avila, R.; Bueno Delgado, M.A.; Blasco Alonso, J.; Doulatram Gamgaram, V.K.; Olveira, G.; Soto-Moreno, A.; Venegas-Moreno, E. Cardiometabolic and Nutritional Morbidities of a Large, Adult, PKU Cohort from Andalusia. Nutrients 2022, 14, 1311. [Google Scholar] [CrossRef]
- Oki, Y.; Okubo, M.; Tanaka, S.; Nakanishi, K.; Kobayashi, T.; Murase, T. Diabetes Mellitus Secondary to Glycogen Storage Disease Type III. Diabet. Med. 2000, 17, 810–812. [Google Scholar] [CrossRef]
- Spiegel, R.; Rakover-Tenenbaum, Y.; Mandel, H.; Lumelski, D.; Admoni, O.; Horovitz, Y. Secondary Diabetes Mellitus: Late Complication of Glycogen Storage Disease Type 1b. J. Pediatr. Endocrinol. Metab. JPEM 2005, 18, 617–619. [Google Scholar] [CrossRef] [PubMed]
- Spengos, K.; Michelakakis, H.; Vontzalidis, A.; Zouvelou, V.; Manta, P. Diabetes Mellitus Associated with Glycogen Storage Disease Type III. Muscle Nerve 2009, 39, 876–877. [Google Scholar] [CrossRef] [PubMed]
- Cohn, A.; Ohri, A. Diabetes Mellitus in a Patient with Glycogen Storage Disease Type Ia: A Case Report. J. Med. Case Rep. 2017, 11, 319. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Patel, D.; Kulshreshtha, B. Secondary Diabetes as a Rare Complication of Glycogen Storage Disease 1a: Case Report and Review of Literature. Pediatr. Endocrinol. Diabetes Metab. 2021, 27, 283–286. [Google Scholar] [CrossRef]
- Kanemaru, Y.; Harada, N.; Wada, N.; Yasuda, T.; Okamura, E.; Fujii, T.; Ogura, M.; Inagaki, N. A Case Report of Diabetes in a Patient with Glycogen Storage Disease Type 1a. Intern. Med. Tokyo Jpn. 2024, 63, 2153–2156. [Google Scholar] [CrossRef]
- Kaiser, N.; Gautschi, M.; Bosanska, L.; Meienberg, F.; Baumgartner, M.R.; Spinas, G.A.; Hochuli, M. Glycemic Control and Complications in Glycogen Storage Disease Type I: Results from the Swiss Registry. Mol. Genet. Metab. 2019, 126, 355–361. [Google Scholar] [CrossRef]
- Hochuli, M.; Christ, E.; Meienberg, F.; Lehmann, R.; Krützfeldt, J.; Baumgartner, M.R. Alternative Nighttime Nutrition Regimens in Glycogen Storage Disease Type I: A Controlled Crossover Study. J. Inherit. Metab. Dis. 2015, 38, 1093–1098. [Google Scholar] [CrossRef]
- Bolinder, J.; Antuna, R.; Geelhoed-Duijvestijn, P.; Kröger, J.; Weitgasser, R. Novel Glucose-Sensing Technology and Hypoglycaemia in Type 1 Diabetes: A Multicentre, Non-Masked, Randomised Controlled Trial. Lancet 2016, 388, 2254–2263. [Google Scholar] [CrossRef]
- Evans, M.; Welsh, Z.; Ells, S.; Seibold, A. The Impact of Flash Glucose Monitoring on Glycaemic Control as Measured by HbA1c: A Meta-Analysis of Clinical Trials and Real-World Observational Studies. Diabetes Ther. Res. Treat. Educ. Diabetes Relat. Disord. 2020, 11, 83–95. [Google Scholar] [CrossRef]
- Haak, T.; Hanaire, H.; Ajjan, R.; Hermanns, N.; Riveline, J.-P.; Rayman, G. Flash Glucose-Sensing Technology as a Replacement for Blood Glucose Monitoring for the Management of Insulin-Treated Type 2 Diabetes: A Multicenter, Open-Label Randomized Controlled Trial. Diabetes Ther. 2017, 8, 55–73. [Google Scholar] [CrossRef]
- Hershkovitz, E.; Rachmel, A.; Ben-Zaken, H.; Phillip, M. Continuous Glucose Monitoring in Children with Glycogen Storage Disease Type I. J. Inherit. Metab. Dis. 2001, 24, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Maran, A.; Crepaldi, C.; Avogaro, A.; Catuogno, S.; Burlina, A.; Poscia, A.; Tiengo, A. Continuous Glucose Monitoring in Conditions Other than Diabetes. Diabetes Metab. Res. Rev. 2004, 20 (Suppl. S2), S50–S55. [Google Scholar] [CrossRef] [PubMed]
- White, F.J.; Jones, S.A. The Use of Continuous Glucose Monitoring in the Practical Management of Glycogen Storage Disorders. J. Inherit. Metab. Dis. 2011, 34, 631–642. [Google Scholar] [CrossRef]
- Kasapkara, Ç.S.; Cinasal Demir, G.; Hasanoğlu, A.; Tümer, L. Continuous Glucose Monitoring in Children with Glycogen Storage Disease Type I. Eur. J. Clin. Nutr. 2014, 68, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Herbert, M.; Pendyal, S.; Rairikar, M.; Halaby, C.; Benjamin, R.W.; Kishnani, P.S. Role of Continuous Glucose Monitoring in the Management of Glycogen Storage Disorders. J. Inherit. Metab. Dis. 2018, 41, 917–927. [Google Scholar] [CrossRef]
- Peeks, F.; Hoogeveen, I.J.; Feldbrugge, R.L.; Burghard, R.; de Boer, F.; Fokkert-Wilts, M.J.; van der Klauw, M.M.; Oosterveer, M.H.; Derks, T.G.J. A Retrospective In-Depth Analysis of Continuous Glucose Monitoring Datasets for Patients with Hepatic Glycogen Storage Disease: Recommended Outcome Parameters for Glucose Management. J. Inherit. Metab. Dis. 2021, 44, 1136–1150. [Google Scholar] [CrossRef]
- Du, C.Q.; Wei, H.; Zhang, C.; Zhang, M.; Hu, M.H.; Hou, L.; Wu, W.; Liang, Y.; Luo, X.P. The application of continuous glucose monitoring in the management of hepatic glycogen storage disease. Zhonghua Er Ke Za Zhi Chin. J. Pediatr. 2021, 59, 452–458. [Google Scholar] [CrossRef]
- Rossi, A.; Venema, A.; Haarsma, P.; Feldbrugge, L.; Burghard, R.; Rodriguez-Buritica, D.; Parenti, G.; Oosterveer, M.H.; Derks, T.G.J. A Prospective Study on Continuous Glucose Monitoring in Glycogen Storage Disease Type Ia: Toward Glycemic Targets. J. Clin. Endocrinol. Metab. 2022, 107, e3612–e3623. [Google Scholar] [CrossRef]
- Overduin, R.J.; Venema, A.; Lubout, C.M.A.; Fokkert-Wilts, M.J.; De Boer, F.; Schreuder, A.B.; Rossi, A.; Derks, T.G.J. Continuous Glucose Monitoring Metrics in People with Liver Glycogen Storage Disease and Idiopathic Ketotic Hypoglycemia: A Single-Center, Retrospective, Observational Study. Mol. Genet. Metab. 2024, 143, 108573. [Google Scholar] [CrossRef]
- Gugelmo, G.; Maines, E.; Boscari, F.; Lenzini, L.; Fadini, G.P.; Burlina, A.; Avogaro, A.; Vitturi, N. Continuous Glucose Monitoring in Patients with Inherited Metabolic Disorders at Risk for Hypoglycemia and Nutritional Implications. Rev. Endocr. Metab. Disord. 2024, 25, 897–910. [Google Scholar] [CrossRef]
- Choudhary, P.; Geddes, J.; Freeman, J.V.; Emery, C.J.; Heller, S.R.; Frier, B.M. Frequency of Biochemical Hypoglycaemia in Adults with Type 1 Diabetes with and without Impaired Awareness of Hypoglycaemia: No Identifiable Differences Using Continuous Glucose Monitoring. Diabet. Med. 2010, 27, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Amiel, S.A.; Aschner, P.; Childs, B.; Cryer, P.E.; Galan, B.E.d.; Frier, B.M.; Gonder-Frederick, L.; Heller, S.R.; Jones, T.; Khunti, K.; et al. Hypoglycaemia, Cardiovascular Disease, and Mortality in Diabetes: Epidemiology, Pathogenesis, and Management. Lancet Diabetes Endocrinol. 2019, 7, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Van Beers, C.A.J.; DeVries, J.H.; Kleijer, S.J.; Smits, M.M.; Geelhoed-Duijvestijn, P.H.; Kramer, M.H.H.; Diamant, M.; Snoek, F.J.; Serné, E.H. Continuous Glucose Monitoring for Patients with Type 1 Diabetes and Impaired Awareness of Hypoglycaemia (IN CONTROL): A Randomised, Open-Label, Crossover Trial. Lancet Diabetes Endocrinol. 2016, 4, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef]
- Riddlesworth, T.D.; Beck, R.W.; Gal, R.L.; Connor, C.G.; Bergenstal, R.M.; Lee, S.; Willi, S.M. Optimal Sampling Duration for Continuous Glucose Monitoring to Determine Long-Term Glycemic Control. Diabetes Technol. Ther. 2018, 20, 314–316. [Google Scholar] [CrossRef]
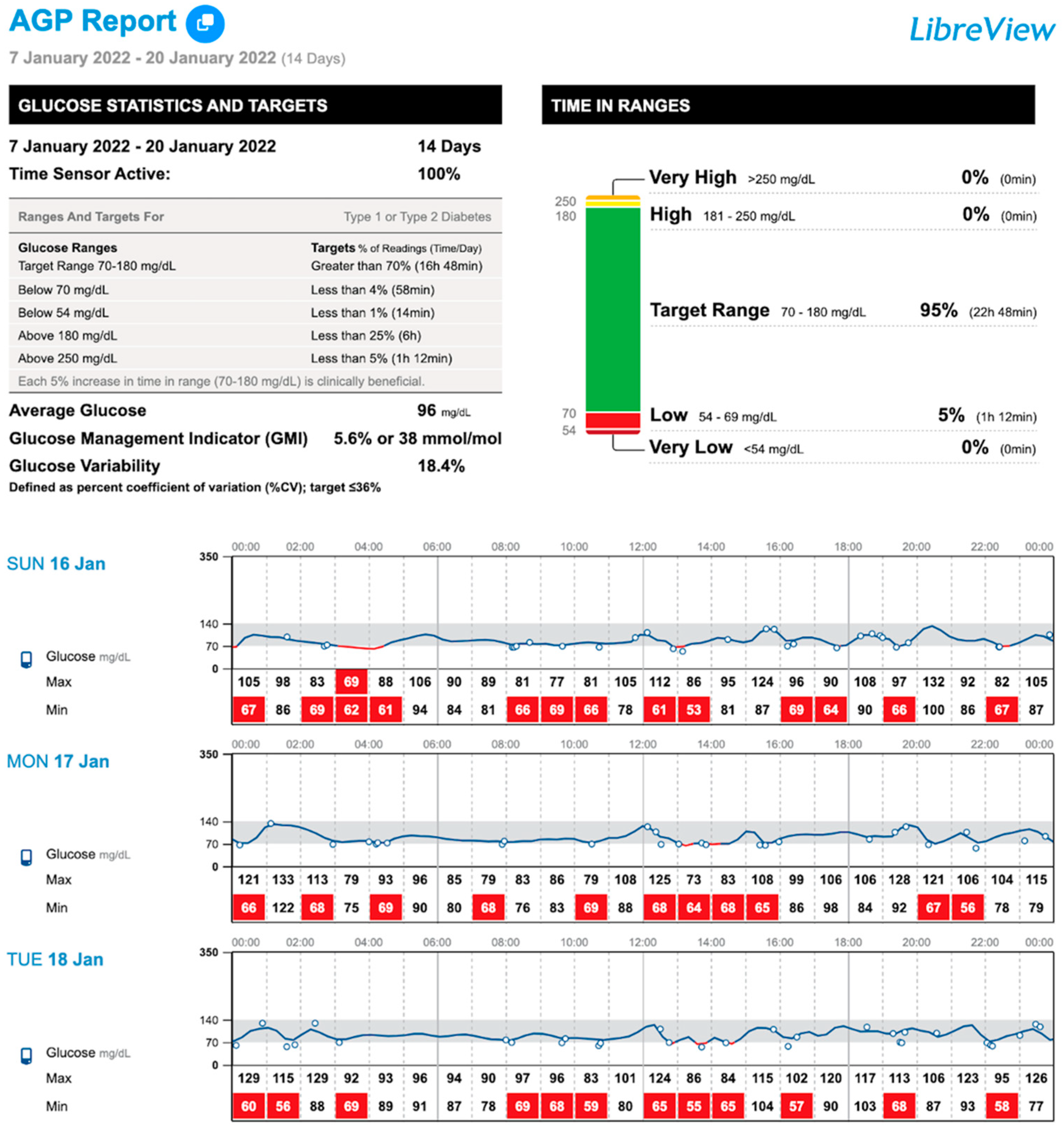

{kind=link}
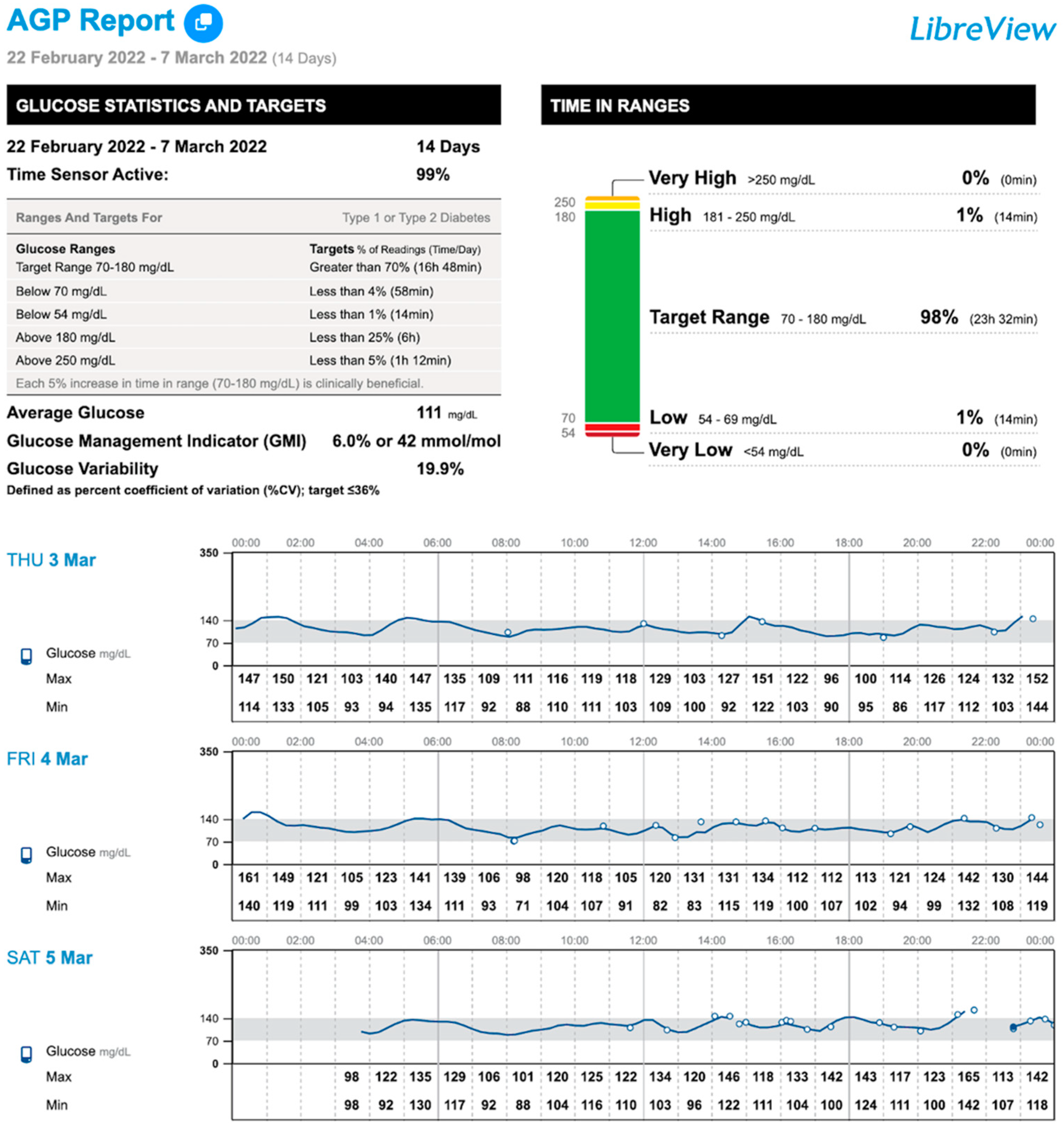
{kind=link}
| Number of Patients | n = 18 | ||
|---|---|---|---|
| Age (years) | 30.5 ± 12.5 | ||
| Gender (male)—n (%) | 11 (61.1) | ||
| BMI (kg/m2) | 28.1 ± 5.3 | ||
| HbA1c (%) | 5.5 ± 0.6 | ||
| IMDs type—n (%) | |||
| FAODs | 9 (50) | MCAD deficiency (n = 4) | |
| LCAD deficiency (n = 1) | |||
| CACT deficiency (n = 1) | |||
| CPT II deficiency (n = 2) | |||
| MADD deficiency (n = 1) | |||
| GSD | 5 (27.8) | Hepatic: 4 (80) | Type Ib (n = 1) |
| Type IIIa (n = 1) | |||
| Type IX (n = 2) | |||
| Muscle: 1 (20) | Type V (n = 1) | ||
| GLUD-1 deficiency | 2 (11.2) | ||
| MMA | 1 (5.5) | ||
| HFI | 1 (5.5) | ||
| History of hypoglycemia—n (%) | Symptomatic 9 (50) | ||
| Nocturnal 6 (33.3) | |||
| Severe 2 (11.1) | |||
| IMD Subgroups (n) | FAODs (9) | GSD (5) | GLUD-1 | MMA | HFI | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MCAD | LCAD | CACT | CPTII | MADD | Ib | IIIa | IX | V | ||||
| N | 4 | 1 | 1 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 1 | 1 |
| Type of nighttime nutrition | ||||||||||||
| UCCS | 2 (22.2) | 1 (11.1) | 0 | 1 (11.1) | 0 | 1 (20) | 0 | 2 (40) | 0 | 1 (50) | 0 | 0 |
| UCCS intake (g/day/person) | 40 | 20 | 0 | 20 | 0 | 40 | 0 | 20 | 0 | 20 | 0 | 0 |
| History of hypoglycemia | ||||||||||||
| Childhood | 2 (22.2) | 0 | 0 | 0 | 0 | 0 | 1 (20) | 0 | 0 | 1 (50) | 0 | 1 |
| Adults | 1 (11.1) | 0 | 0 | 0 | 1 (11.1) | 1 (20) | 0 | 2 (40) | 0 | 2 (100) | 0 | 1 |
| Symptomatic | 2 (22.2) | 0 | 0 | 0 | 1 (11.1) | 1 (20) | 0 | 2 (20) | 0 | 2 (100) | 0 | 1 |
| Nocturnal | 2 (22.2) | 0 | 0 | 0 | 0 | 1 (20) | 0 | 1 (20) | 0 | 2 (100) | 0 | 0 |
| Severe | 1 (11.1) | 0 | 0 | 0 | 0 | 1 (20) | 0 | 0 | 0 | 0 | 0 | 0 |
| IMDs (n = 18) | ||||
|---|---|---|---|---|
| 1 Week | 2 Weeks | 2 Months | p | |
| N | 18 | 18 | 18 | |
| TIR (%, 70–140 mg/dL) 1 | 94 (88–97) | 95 (88–97) | 94.5 (87–98) | 0.214 |
| TIR (%, 70–180 mg/dL) 1 | 98 (94–100) a | 98.5 (95–100) | 99 (98–100) b | 0.020 |
| TAR (%, >140 mg/dL) 1 | 2 (1–7) | 2.5 (1–8) | 2 (2–11.5) | 0.167 |
| TAR (%, >180 mg/dL) 1 | 0 (0–0) | 0 (0–0) | 0 (0–0.2) | 0.751 |
| TAR (%, >250 mg/dL) 1 | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.368 |
| TBR (%, <70 mg/dL) 1 | 1.5 (0–3) a | 1 (0–2) | 0 (0–1) b | 0.005 |
| TBR (%, <54 mg/dL) 1 | 0 (0–2) | 0 (0–0) | 0 (0–0) | 0.035 |
| TBR total (%) 1 | 1.5 (0–4) a | 1 (0–3) | 0 (0–1) b | 0.021 |
| Low glucose events (n) 1 | 1 (0–7) a | 1 (0–6) | 0 (0–3) b | 0.040 |
| Average duration (min) 2 | 61.4 ± 62.5 | 57 ± 54.4 | 33.8 ± 41.5 | 0.223 |
| CV (%) 1 | 17.4 (14–19) a | 16.6 (14–19) | 16.6 (14–19) b | 0.476 |
| Mean glucose (mg/dL) 2 | 103 ± 10.3 a | 105.8 ± 11.8 | 105.3 ± 9.7 b | 0.034 |
| GMI (%) 2 | 5.8 ± 0.2 | 5.8 ± 0.2 | 5.8 ± 0.2 | 0.697 |
| Sensor use (%) 1 | 93 (72–99) | 93 (86–99) | 93 (78–98) | 0.129 |
| Scans/day (n) 1 | 6 (5–13) a | 7 (4–15) | 5 (4–12) b | 0.021 |
| IMDs (n) | TBR, % | Low Glucose Events (n) | Average Duration (Min) | ||
|---|---|---|---|---|---|
| <70 mg/dL | <54 mg/dL | Total | |||
| FAODs (9) | |||||
| 1 Week | 1.6 ± 3.6 | 0.4 ± 0.9 | 2 ± 4.3 | 2.2 ± 4.1 | 47.4 ± 81.2 |
| 2 Weeks | 1.2 ± 2.2 | 0 ± 0 | 1.2 ± 2.2 | 1.9 ± 2.9 | 42.1 ± 69.4 |
| 2 Months | 0.3 ± 0.5 | 0 ± 0 | 0.3 ± 0.5 | 1.6 ± 3.6 | 27.5 ± 33.7 |
| GSD (5) | |||||
| 1 Week | 2.2 ± 0.8 | 0.4 ± 0.9 | 2.6 ± 1.5 | 4.4 ± 4.2 | 72 ± 25.4 |
| 2 Weeks | 1.6 ± 0.5 | 0.2 ± 0.4 | 1.8 ± 0.8 | 2.8 ± 1.8 | 61.6 ± 28 |
| 2 Months | 0.4 ± 0.5 | 0 ± 0 | 0.4 ± 0.5 | 2.6 ± 2.8 | 60.8 ± 35 |
| GLUD-1 (2) | |||||
| 1 Week | 6.5 ± 5 | 0.5 ± 0.7 | 7 ± 5.6 | 6 ± 4.2 | 80 ± 28.3 |
| 2 Weeks | 5.5 ± 5 | 2 ± 2.8 | 7.5 ± 7.7 | 5.5 ± 5 | 83.5 ± 0.7 |
| 2 Months | 2.5 ± 3.5 | 0 ± 0 | 2.5 ± 3.5 | 3 ± 2.8 | 57 ± 38.2 |
| MMA (1) | |||||
| 1 Week | 0 | 0 | 0 | 1 | 45 |
| 2 Weeks | 0 | 0 | 0 | 1 | 45 |
| 2 Months | 0 | 0 | 0 | 1 | 45 |
| HFI (1) | |||||
| 1 Week | 7 | 1 | 8 | 8 | 151 |
| 2 Weeks | 5 | 0 | 5 | 10 | 128 |
| 2 Months | 2 | 0 | 2 | 3 | 136 |
| FAODs (9) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MCAD (4) | LCAD (1) | CACT (1) | CPT II (2) | MADD (1) | |||||||||||
| 1 Week | 2 Weeks | 2 Months | 1 Week | 2 Weeks | 2 Months | 1 Week | 2 Weeks | 2 Months | 1 Week | 2 Weeks | 2 Months | 1 Week | 2 Weeks | 2 Months | |
| TBR (%, <70 mg/dL) | 0 ± 0 | 0 ± 0 | 0 ± 0 | 11 | 5 | 1 | 2 | 5 | 0 | 0 ± 0 | 0 ± 0 | 0.5 ± 0.7 | 1 | 1 | 1 |
| TBR (%, <54 mg/dL) | 0 ± 0 | 0 ± 0 | 0 ± 0 | 2 | 0 | 0 | 2 | 0 | 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 | 0 | 0 |
| TBR total (%) | 0 ± 0 | 0 ± 0 | 0 ± 0 | 13 | 5 | 1 | 4 | 5 | 0 | 0 ± 0 | 0 ± 0 | 0.5 ± 0.7 | 1 | 1 | 1 |
| Low glucose events (n) | 0 ± 0 | 0 ± 0 | 0 ± 0 | 11 | 9 | 5 | 3 | 10 | 0 | 0 ± 0 | 0 ± 0 | 4.5 ± 4.9 | 1 | 1 | 3 |
| Average duration (min) | 0 ± 0 | 0 ± 0 | 0 ± 0 | 151 | 156 | 65 | 216 | 163 | 0 | 0 ± 0 | 0 ± 0 | 59 ± 22.6 | 60 | 60 | 65 |
| GSD (5) | |||||||||||||||
| Type Ib (1) | Type IIIa (1) | Type IX (2) | Type V (1) | ||||||||||||
| 1 Week | 2 Weeks | 2 Months | 1 Week | 2 Weeks | 2 Months | 1 Week | 2 Weeks | 2 Months | 1 Week | 2 Weeks | 2 Months | ||||
| TBR (%, <70 mg/dL) | 3 | 1 | 1 | 2 | 2 | 1 | 1.5 ± 0.7 | 1.5 ± 0.7 | 0 ± 0 | 0 | 0 | 0 | |||
| TBR (%, <54 mg/dL) | 0 | 0 | 0 | 0 | 0 | 0 | 0 ± 0 | 0 ± 0 | 0 ± 0 | 0 | 0 | 0 | |||
| TBR total (%) | 3 | 1 | 1 | 2 | 2 | 1 | 1.5 ± 0.7 | 1.5 ± 0.7 | 0 ± 0 | 0 | 0 | 0 | |||
| Low glucose events (n) | 11 | 3 | 2 | 6 | 6 | 5 | 2 ± 1.4 | 2.5 ± 2.1 | 0 ± 0 | 1 | 1 | 0 | |||
| Average duration (min) | 93 | 46 | 40 | 55 | 95 | 50 | 76 ± 41 | 78.5 ± 44 | 0 ± 0 | 0 | 0 | 0 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amuedo, S.; Dios-Fuentes, E.; Benítez-Ávila, R.; Remón-Ruiz, P.; Soto-Moreno, A.; Venegas-Moreno, E. Impact of Flash Glucose Monitoring in Adults with Inherited Metabolic Disorders at Risk of Hypoglycemia. Nutrients 2025, 17, 222. https://doi.org/10.3390/nu17020222
Amuedo S, Dios-Fuentes E, Benítez-Ávila R, Remón-Ruiz P, Soto-Moreno A, Venegas-Moreno E. Impact of Flash Glucose Monitoring in Adults with Inherited Metabolic Disorders at Risk of Hypoglycemia. Nutrients. 2025; 17(2):222. https://doi.org/10.3390/nu17020222
Chicago/Turabian StyleAmuedo, Sandra, Elena Dios-Fuentes, Rosa Benítez-Ávila, Pablo Remón-Ruiz, Alfonso Soto-Moreno, and Eva Venegas-Moreno. 2025. "Impact of Flash Glucose Monitoring in Adults with Inherited Metabolic Disorders at Risk of Hypoglycemia" Nutrients 17, no. 2: 222. https://doi.org/10.3390/nu17020222
APA StyleAmuedo, S., Dios-Fuentes, E., Benítez-Ávila, R., Remón-Ruiz, P., Soto-Moreno, A., & Venegas-Moreno, E. (2025). Impact of Flash Glucose Monitoring in Adults with Inherited Metabolic Disorders at Risk of Hypoglycemia. Nutrients, 17(2), 222. https://doi.org/10.3390/nu17020222