Abstract
The selection of food depends on various factors such as cultural, social, economic and biological. This paper determines the factors associated with dietary patterns in Colombia. It is an observational, descriptive exploratory study collecting secondary data from the National Survey of Nutritional Status of Colombia (ENSIN, 2015) of 16,216 people between 15 and 64 years of age. The variables were the following: area, age range, sex, educational level, high blood pressure arterial hypertension (HTA), diabetes (DM), cancer, wealth quartile and dietary pattern. For the data analysis, logistic regression models were generated for each pattern and OR was used as a measure of association. Of those studied, 74.6% live in urban areas, all were aged between 15 and 49 years and 45.4% were in the first wealth quartile (Q1). There was a greater probability of traditional and conservative dietary patterns in people with diabetes and hypertension. Consumption of the conservative pattern was associated with being a woman, while consumption of the traditional pattern was associated with people in the first and second wealth level. Consumption of grill/beverage was more likely in men. Socio-demographic factors and chronic non-communicable diseases are associated with dietary patterns. This makes it relevant for health professionals to take into account these characteristics for nutritional interventions.
1. Introduction
Eating patterns are given by the consumption of those foods that are ingested more frequently and that exert synergistic effects on the body to meet physiological needs. In addition, they are an important component in understanding the relationship between food systems and food and nutrition security [1].
Nutritional epidemiological studies have focused on the analysis of the pattern that describes the general diet of a population, in order to understand the relationship between this and health status, which should guide the development of food policies. That is, the effectiveness of food policies and strategies depend on the knowledge and contextualization of the behavior of the population’s eating behavior, its culture and other factors that may influence the modification of lifestyles, which are capable of influencing the adoption of new eating patterns [2].
In this sense, the eating behavior of the population is influenced by the economic and structural development of society. In Western and high-income countries, the pattern is usually marked by a high consumption of fats, mainly saturated, sugars, processed foods and animal proteins, and a low intake of fiber and complex carbohydrates [3].
On the other hand, in the countries of Latin America and the Caribbean, the United Nations Organization reports that dietary patterns have traditionally been marked by a set of staple foods formed by cereals, roots and tubers. It is estimated that 39% of the dietary energy available in the countries of the region comes from these foods. For the Caribbean and South America it is 37%, while in Mesoamerica it accounts for 44% of the daily kilocalories available [1].
The origin of the kilocalories consumed has changed, causing a change in dietary patterns and an increase in the availability of proteins of animal origin, as well as animal and vegetable fats [4].
In Colombia, Meneses et al., through data obtained from the National Survey of the Nutritional Situation of Colombia (ENSIN) of 2015, with a population aged 15 to 64, identified four food patterns. The first, called “traditional pattern”, was made up of the food groups: dairy, potatoes/legumes, cereals, fried foods, coffee, panela/sugar/honey and meat/fish/eggs/sausages. The second food pattern, “industrial pattern”, included packaged treats, fast food and soft drinks. The third, called “conservative”, was made up of whole foods, light foods/supplements, fruits and vegetables. Finally, the fourth, “grilled food/processed drinks pattern”, was made up of alcoholic beverages, grill foods and energy drinks [5].
Therefore, we took as a reference these four patterns (traditional, industrialized, preservative, grilled food/processed drinks) and the influence of factors such as age, sex, socioeconomic level, schooling, ethnicity, etc. in feeding practices [6,7]. The research aimed to determine the factors associated with these patterns and their spatial distribution by the departments of Colombia.
2. Methodology
This is an observational, descriptive exploratory study that uses secondary data from the sample of 16,216 people, between 15 and 64 years old, who participated in the National Survey of the Nutritional Situation of Colombia (ENSIN, 2015), a cross-sectional population study with probabilistic, cluster, stratified and multistage sampling [8].
The independent variables were area, age range, sex, education level, hypertension (HTN), diabetes (DM), cancer and quartile of wealth. The dependent variable was “dietary patterns”, defined according to the results obtained by this group and previously [5,7]. In this research, the authors defined the four food patterns discussed above: traditional pattern, industrial pattern, the preservative and the grill/beverage.
To determine the factors associated with dietary patterns and their spatial distribution in the Departments of Colombia, it was necessary to generate a new dichotomous dependent variable, through a binomial distribution, as follows: the cases that presented some degree of consumption of the corresponding pattern were categorized as 1, while those that did not reported a level of consumption of the pattern was categorized as 0. This was necessary to perform non-conditional logistic regression models [7].
These were elaborated, including all the available variables, that is, explanatory and adjustment, which were measured in a polytomous way (area, age ranges, educational level, quartile of wealth) and dichotomous (sex, hypertension, diabetes, cancer). From them, the coefficients associated with each variable were obtained, and the adjusted odds ratio (OR), where the reference category of each independent variable was the first.
The authors used backward modelling (as usual in this research type [9]). This modelling consists of starting with a saturated model that includes as many explanatory variables as possible (a p-value < 0.2 was set for the first modelling [9]) and then eliminating in consecutive steps those with p > 0.05. That is, only the significant ones remain (p < 0.05).
The R2 of Cox and Snell, the Hosmer and Lemeshow test and the logarithm of the likelihood (LL) were used as measures of goodness of fit of the models to assess the association of these variables with the explanation of each of the dietary patterns, generating logistic regression models for each pattern and using the OR association measure with its corresponding 95% confidence interval.
From the data, a description of the behavior of food consumption by department was made, elaborating a map of Colombia that described the consolidation of these in quartiles (Q), each one represented by color intensity. The most intense meant greater presentation of consumption of the pattern in the upper quartile. Qgis version 3.10.13 [10] and SPSS version 27 was used for statistical analysis.
Ethical Considerations
The study was endorsed by the Institutional Ethics Review Committee of the Santiago de Cali University Approval Act No. 11 of 29 May 2020. The database used was authorized by the Colombian Institute of Family Welfare (ICBF) to conduct the research.
3. Results
Most of the participants resided in the city (74.6%) and the most frequent age range was 15 to 29 years (54.0%). The majority were women (57.0%), and, in terms of educational level, it prevailed between primary and secondary school (79.5%). A quarter (25.1%) had high blood pressure, 1.6% diabetes mellitus and less than 1% had a history of cancer. In relation to the quartile of wealth, 45.4% were located in the first quartile (Table 1).

Table 1.
Description of the variables included in the study, represented in absolute and relative frequencies.
In the patterns of food consumption by department, the traditional pattern (pattern 1) had a higher consumption (between 57.1% and 60.5%) in the departments of Atlántico, Caldas, Tolima, Caquetá, Santander and Norte de Santander. The industrial pattern (pattern 2) was in the departments of La Guajira, Magdalena, Cesar, Cundinamarca, Meta, San Andrés and Providencia, with an average consumption between 41.3 and 52.5%. The conservative pattern (pattern 3) was more present in the departments of Córdoba, Santander, Norte de Santander, Cundinamarca, Boyacá, Caquetá, Nariño, San Andrés and Providencia, with percentages between 34.3% and 37.1%. The grill/beverage (pattern 4) stood out in the departments of La Guajira, Córdoba, Choco, Norte de Santander, Boyacá, Casanare, Guainía and Mitú, with the average consumption between 15.5% and 20.65% (Figure 1).
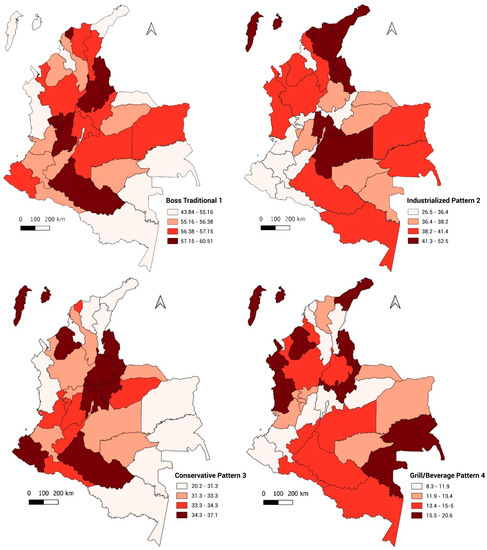
Figure 1.
Map of the distribution of dietary patterns by department.
A modelling process was carried out for each dietary pattern. It started with a saturated model including eight explanatory variables: area, age range, sex, education level, hypertension (HTN), diabetes mellitus (DM), cancer and quartile of wealth. After the modeling process that began with the eight variables discussed above, four dietary patterns were identified (Table 2). Pattern 1, called “Boss Traditional”, was defined by six variables, highlighting its relationship with HTN and diabetes. Pattern 2, named “Industralized”, included six variables prominently related to different educational levels, wealth quartiles and HTN. In addition, pattern 3, which included five variables, was called “Conservative Pattern”, highlighting among them HTN, cancer and diabetes, which led us to believe that it was a dietary pattern more common in people with a chronic non-communicable disease and in which adherence to a healthy diet is a fundamental part of the treatment. Finally, pattern 4, called “Grill/Beverage”, maintained the eight initial variables of the saturated model, emphasizing its relationship with cancer, diabetes and living in a rural area. Possibly, this pattern represents subjects whose lifestyles (especially dietary habits) are related to the origin of these chronic pathologies; however, unlike the individuals most characterized by pattern 3, perhaps they have not abandoned these unhealthy dietary habits, which possibly played a role in the development of these diseases. More details about the patterns, the variables included in each one, and their degree of significance are available in Table 2 and Table 3.
Table 2.
Comparison of logistic regression models for each dietary pattern with their respective measures of goodness of fit. Colombia.
Table 3.
Adjusted association measures obtained from the definitive logistic regression model for each dietary pattern. Colombia.
Figure 2 shows the graph of the OR and confidence intervals adjusted by the dietary pattern, where the relevance of suffering from a chronic disease in relation to adopting pattern 1 and 3, the positive relationship between socioeconomic and cultural characteristics with patterns 2 and 3 or the role of the youngest age group in relation to pattern 4 can be observed.
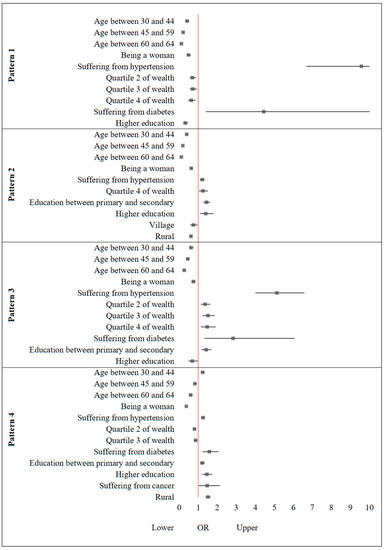
Figure 2.
Confidence intervals (95%) of the odds ratios adjusted for the models obtained according to consumption pattern in Colombia.
4. Discussion
The findings demonstrated the association between each eating pattern with the following variables: age group, sex, quartile of wealth and educational level. Similarly, it was found that living in a certain population area of Colombia (city, village, rural) or suffering from hypertension, diabetes mellitus or cancer, were not determining variables in the construction of the associated factors of some dietary patterns.
The population between 15 and 29 years old had a greater tendency to consume foods included in the industrialized pattern (sweets/package foods, fast food and soft drinks), followed by the traditional pattern (dairy, potatoes/legumes, cereals, fried foods, coffee, panela/sugar/honey and meat/fish/eggs/sausages). Like us, the study reported by Khandpur et al., found a greater tendency in young people to consume foods included in this pattern, probably influenced by marketing and marketing practices of these products [11].
In the population between 30 and 64 years, the consumption of foods included in the grill/beverage (alcoholic beverages; grill foods; energy drinks) was significantly more frequent, followed by the conservative pattern (whole foods, light foods/supplements, fruits and vegetables). This was similar to that found by Adrogue et al., where the average consumption of fruits and vegetables increased from the age of 35 [12].
Men were most likely to consume the grill/beverage pattern, followed by the traditional pattern. Women tended to consume more foods from the conservative pattern, followed by the industrialized pattern. Along these lines, several authors have indicated that women have greater awareness and knowledge of nutrition than men, greater motivation for weight control and prioritize healthy eating [13,14]. On the other hand, studies report that the consumption of energy drinks is associated with masculinity and extreme sports [15,16].
Suffering from hypertension was associated with all dietary patterns, with a greater tendency to consume foods included in the traditional pattern, followed by the conservative pattern. On the other hand, suffering from diabetes mellitus was strongly associated with the traditional pattern, followed by the conservative pattern and grill/beverage, while suffering from cancer was strongly associated with the conservative pattern, followed by the grill/beverage. Contrary to what might be expected, the conservative pattern had a significant association with these diseases, which could be explained by the years of diagnostic evolution and the probable modification of eating habits to control the evolution of the disease. According to several studies, there is a positive relationship between the frequency of fruit and vegetable consumption in chronic disease [17,18].
Regarding the traditional pattern, our findings agree with other authors [19,20], mentioning that patients with hypertension and diabetes mellitus have a greater tendency to consume dairy products, potatoes/legumes, cereals, fried foods, coffee, panela/sugar/honey and meat/fish/eggs/sausages. These foods are part of the food culture of the Colombian population, with a high caloric intake and are easy to acquire, due to their wide availability and low economic cost [21,22]. On the other hand, it has been shown that the consumption of whole grains containing bioactive components such as dietary fiber, resistant starch, vitamins, minerals and phytoestrogens [23,24], and the consumption of fruits and vegetables, are related to the control and reduction of the risk of cancer, hypertension, diabetes mellitus, obesity and other cardiovascular diseases [25,26]. According to Afshin et al., the average consumption of fruits worldwide is two-thirds of the minimum recommended amounts [27]. These vary in Central Asia, North Africa and the Middle East, where slightly more than the recommended minimum is consumed, while sub-Saharan Africa and Oceania consume only a third of this amount. The inhabitants of the Caribbean consume the most fruits, while those of southern Africa are the least [28]. Therefore, increasing the consumption of fruits and vegetables has become a priority globally, which is why it has been linked to the UN Sustainable Development Goals for the year 2030 [28]. However, increasing the presence of this pattern entails great difficulty because it is determined both by individual factors and by factors of the social and economic structure, which in many cases cannot be controlled by the individual [29].
Regarding the wealth index, quartiles three and four were strongly associated with the conservative pattern, followed by the industrialized pattern [30,31]. Quartiles of wealth one and two had the greatest association with the traditional pattern, followed by the grill/beverage. According to Miramontes et al. [32] and in the analysis of ENSIN 2005, people with low quartiles of wealth more frequently consumed foods included in the traditional pattern, such as tubers and bananas [33]. These differences reflect the influence of purchasing power on accessibility to healthy and unhealthy foods, causing changes in purchasing patterns and resulting diets [4,34].
Regarding the level of education, the population between primary and secondary school had a greater tendency to consume foods of the industrialized pattern, followed by the conservative pattern and grill/beverage. The population with a higher education had a greater tendency to consume foods of the grill/beverage pattern, followed by the industrialized pattern. This coincides with Lacko et al. who reported that the lower the educational level, the greater the intake of foods with high sugar content and packaged foods [35].
Living in a village or rural population area was strongly related to the grill/beverage and living in the city with the industrialized pattern. A study in 18 low-, middle- and high-income countries in seven geographic regions revealed that the highest consumption of fruits and vegetables was found in the urban area or municipal capital [36], which coincides with the results of this research.
Given that health levels vary substantially between regions, it is necessary to characterize these regional variations in order to identify areas with an accumulation of health problems and to improve epidemiological research on which appropriate public health policy decision-making should be supported [37]. Recent technological advances, such as geographic information systems (GIS), have enabled the application not only of disease mapping but also of spatial analyses, such as spatial clustering and cluster detection, in epidemiological research [38]. In this context, clusters are defined as unusual concentrations of health events in both space and time [39] and knowing how they behave in these clusters allows targeted interventions.
From this perspective of spatial distribution, there is a tendency to present the influence of several eating patterns in the same department, probably due to internal migratory phenomena in Colombia [40,41,42].
Even so, in the departments of Atlántico, Caldas, Caquetá, Norte de Santander, Santander and Tolima, there was a greater tendency to the traditional pattern, which may be related to the fact that these, with the exception of Atlántico and Caquetá, concentrate the second largest food production of cereals, legumes, tubers and sugar cane in Colombia [43]. At the same time, this type of food consumption had a strong association with quartiles of wealth one/two, a level of education lower than complete primary and suffering from hypertension or diabetes mellitus. As indicated by other authors, inadequate eating practices are associated with low income and lack of adequate food plans according to their sociocultural context [20], in addition to little knowledge about eating patterns [44], which makes it difficult to control chronic diseases.
On the other hand, the departments of Boyacá, Caquetá, Córdoba, Cundinamarca, Nariño, Norte de Santander, Santander, San Andrés and Providencia, had a greater tendency to the conservative pattern and this type of food consumption had a strong association with the quartiles of wealth three/four, educational level between primary and secondary, being a woman and suffering from cancer. According to the report of the National Administrative Department of Statistics (DANE) of Colombia, the departments of Boyacá, Nariño, Risaralda, Tolima and Valle del Cauca represent 53.7% of the production of vegetables in the rural area surveyed [45], coinciding with the results obtained in the spatial distribution of the pattern that includes a high consumption of the same (conservative).
Among the limitations of the study, underreporting in the comorbidity declaration is considered, given that the figures obtained do not correspond to what was expected [46]. As it is a study carried out from a secondary source of data, it was not possible to include cultural variables that could be influencing food consumption habits, in addition to variables related to access to healthy foods, years of diagnostic evolution and modification of eating habits to control the evolution of diseases: high blood pressure, diabetes mellitus and cancer. In addition, for future studies, it is recommended that analyses be carried out by subgroups and by specific territories, so that the results of the analyses can be used to evaluate health status and thus guide the development of food policies in a more focused manner. It would be important to be able to compare the dependence of the presence of hypertension on dietary patterns in each age group and in relation to the territory, given that hypertension is an age-related disease with a multifactorial etiology.
5. Conclusions
The study’s findings show that in Colombia, four dietary patterns are consumed in different proportions in each region, probably conditioned by migratory movements and the diversity of foods in the country. In contrast, dietary patterns were influenced by educational level, gender, chronic disease and economic and social conditions rather than by residence in a given area. We consider this information relevant for conducting epidemiological studies that allow them to relate to chronic non-communicable diseases and plan population interventions by regions to promote home practices and healthy habits that reduce their incidence.
Author Contributions
L.A.M.-U. and M.H.-C. conceptualized the study. L.A.M.-U. and M.H.-C. conducted the analysis and drafted the manuscript. L.A.M.-U., M.H.-C., D.V.A., N.B.S., G.M.-R. and M.V.-A. reviewed and revised the draft. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the General Directorate of Research of Santiago de Cali University under call No. 03-2020, 01-2021, 05-2021. The authors thank the Colombian Institute of Family Welfare(ICBF), University Santiago de Cali, for providing the original database of the National Survey of the Nutritional Situation of Colombia (ENSIN); Cordoba University for providing the methodological tools for data analysis; and Universidad Santiago de Cali for funding the study (No. 441-621120-1947). The APC was funded by University Santiago of Cali, Cali-Colombia.
Institutional Review Board Statement
This study was reviewed and approved by The Human Research Ethics Committee of Santiago of Cali University (Act N°11 from the May 29th session). Written informed consent for participation was not required for this study in accordance with national legislation (Resolution 8430 of 1993) and international requirements (Declaration of Helsinki and standards of Good Clinical Practice/Harmonized Tripartite Guide of the International Council for Harmonisation).
Informed Consent Statement
Informed consents are unavailable since the article was conducted through secondary analysis of databases corresponding to national health surveys in Colombia. However, all participants in these national surveys gave their consent (verbal or signed) to the interviewers of the national health system.
Data Availability Statement
The data will be made available to anyone who requests it from the corresponding author through a reasoned request.
Acknowledgments
The authors would like to express their gratitude to the Colombian Family Welfare Institute (its Spanish acronym is ICBF); to Universidad de Córdoba for providing the methodological tools for data analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rapallo, R.; Rivera, R. Nuevos Patrones Alimentarios, Organ las Nac Unidas Para la Agric y la Aliment. 2019, Volume 11, pp. 3–27. Available online: http://www.fao.org/3/ca5449es/ca5449es.pdf (accessed on 1 September 2022).
- Maira, B.-R.; Jose, B.E.M.; Camen, B.; Adela, C.P.; Isabel, C.C.; Javier, D.; Fernando, J.G.L.; García, E.L.; González, M.Á.M.; Jurado, L.L.; et al. Nutrición en Salud Pública. In Madrid. 2017, p. 356. Available online: http://gesdoc.isciii.es/gesdoccontroller?action=download&id=11/01/2018-5fc6605fd4 (accessed on 23 September 2022).
- Popkin, G.-L. The nutrition transition: Worldwide obesity dynamics and their determinants. Nature 2018, 388, 539–547. Available online: https://pubmed.ncbi.nlm.nih.gov/15543214 (accessed on 1 August 2021). [CrossRef]
- Popkin, B.M.; Reardon, T. Obesity and the food system transformation in Latin America. Obes. Rev. 2018, 19, 1028–1064. [Google Scholar] [CrossRef] [PubMed]
- Abellan, M.V.; Sandoval, N.B.; Dolly, V.A.; Osorio Murillo, O.; Molina, R. Dietary Patterns in Colombia: An Exploratory and Confirmatory Factor Analysis. Front. Food Sci. Technol. 2022, 2, 1–14. [Google Scholar] [CrossRef]
- Krige, S.M.; Mahomoodally, F.M.; Subratty, A.H.; Ramasawmy, D. Relationship between Socio-Demographic Factors and Eating Practices in a Multicultural Society. 2012, pp. 286–295. Available online: https://www.scirp.org/journal/home.aspx?issueid=1504#17955 (accessed on 26 October 2022). [CrossRef]
- Xu, H. Comparing spatial and multilevel regression models for binary outcomes in neighborhood studies. Am. Sociagical. Assoc. 2014, 44, 229–272. [Google Scholar] [CrossRef]
- ICBF, MINSALUD I. Encuesta Nacional de la Situación Nutricional—ENSIN 2015. Volume 151. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/ED/GCFI/documento-metodologico-ensin-2015.pdf (accessed on 3 February 2022).
- Mauricio, H.C.; Martínez, M.I.G. Factores de Riesgo Asociados a la Intimidación Escolar en Instituciones Educativas Públicas de Cuatro Municipios del Departamento del Valle del Cauca 2009. Rev Colomb Psiquiatr. 2013, 42, 238–247. Available online: https://www.redalyc.org/pdf/806/80629821002.pdf (accessed on 1 October 2022).
- Baghdadi, N.; Mallet, C.; Zribi, M. QGIS and Generic Tools; ISTE Ltd.: Reino Unido London; John Wiley & Sons: Hoboken, NJ, USA, 2018; 293p. [Google Scholar]
- Neha, K.; Gustavo, C.; Ayala, O.; Jaime, P.C.; Parra, D.C. Factores sociodemográficos asociados al consumo de alimentos ultraprocesados en Colombia. Rev Saude Pública. 2019, 54, 19. [Google Scholar] [CrossRef]
- Adrogué, C.; Orlicki, M.E. Factores relacionados al consumo de frutas y verduras en base a la Encuesta Nacional de Factores de Riesgo en Argentina. Pilquen. Rev. Pilquen 2019, 22, 70–82. Available online: http://revele.uncoma.edu.ar/htdoc/revele/index.php/Sociales/article/view/2404/PDF (accessed on 19 March 2023).
- de Melo Simplício, A.P.; de Carvalho Lavôr, L.C.; Rodrigues LA, R.L.; de Lima Sousa, P.V.; de Sousa Ibiapina CR, L.; Frota KD, M.G. Consumo alimentar e sua associação com aspectos sociodemográficos e de estilo de vida em adultos e idosos: Um estudo de base populacional food consumption and its association with sociodemographic and lifestyle aspects in adults and elderly: A populatio. Rev. Eletrônica Acervo Saúde 2022, 15, e10388. [Google Scholar] [CrossRef]
- Kiefer, I.; Rathmanner, T.; Kunze, M. Eating and dieting differences in men and women. J. Men’s Health Gend. 2005, 2, 194–201. [Google Scholar] [CrossRef]
- Wimer, D.J.; Levant, R.F. Energy Drink Use and Its Relationship to Masculinity, Jock Identity, and Fraternity Membership Among Men. Am J Men´s Health 2013, 7, 317–328. [Google Scholar] [CrossRef]
- Miller, K.E. Wired: Energy Drinks, Jock identify, Masculine Norms, and Risk Taking. J. Am. Coll. Health 2008, 56, 481–489. [Google Scholar] [CrossRef]
- Pienovi, L.; Lara, M.; Bustos, P.; Amigo, H. Consumo de frutas, verduras y presión arterial. Un estudio poblacional. Arch Lat. Nutr. 2015, 65, 21–26. Available online: http://ve.scielo.org/pdf/alan/v65n1/art03.pdf (accessed on 3 December 2022).
- Barouti, A.A.; Tynelius, P.; Lager, A.; Björklund, A. Fruit and vegetable intake and risk of prediabetes and type 2 diabetes: Results from a 20-year long prospective cohort study in Swedish men and women. Eur. J. Nutr. 2022, 61, 3175–3187. [Google Scholar] [CrossRef] [PubMed]
- Jerez Tirado, Y.; Porras Ramírez, A. Relación entre patrones alimentarios, diabetes, hipertensión arterial y obesidad según aspectos sociogeográficos, Colombia. Rev. Cuba. Salud Pública 2021, 46, 4111. [Google Scholar] [CrossRef]
- Forero, A.Y.; Hernández, J.A.; Rodríguez, S.M.; Romero, J.J.; Morales, G.E.; Ramírez, G.Á. La Alimentación Para Pacientes con Diabetes Mellitus de Tipo 2 en Tres Hospitales Públicos de Cundinamarca, Colombia. 2018, pp. 355–362. Available online: http://www.scielo.org.co/scielo.php?script=sci_abstract&pid=S0120-41572018000300355&lng=en&nrm=iso&tlng=es (accessed on 19 March 2023). [CrossRef]
- Gil, D.; Giraldo, N.; Estrada, A. Ingesta de alimentos y su relación con factores socioeconómicos en un grupo de adultos mayores. Rev. Salud Pública 2017, 19, 304–310. [Google Scholar] [CrossRef]
- FAO; OPS; WFP; UNICEF. Panorama de la Seguridad alimentaria y Nutricional. En América Latina y el Caribe Panorama de la Seguridad Alimentaria y Nutricional. 2019. Available online: https://www.fao.org/3/ca6979es/ca6979es.pdf (accessed on 21 November 2022).
- Villarroel, P.; Gomez, C.; Camila, V.; Torres, J. Almidón Resistente: Características Tecnológicas e Intereses Fisiológicos. Rev. Chil. Nutr. 2018, 45, 271–278. Available online: https://www.scielo.cl/pdf/rchnut/v45n3/0717-7518-rchnut-45-03-0271.pdf (accessed on 3 December 2022). [CrossRef]
- Kuhnle, G.G.C.; Aquila, C.D.; Aspinall, S.M.; Runswick, S.A.; Mulligan, A.A.; Bingham, S.A. Phytoestrogen Content of Cereals and Cereal-Based Foods Consumed in the UK. 2009, 61, 302–309. Available online: https://www.tandfonline.com/doi/abs/10.1080/01635580802567141?journalCode=hnuc20 (accessed on 21 September 2021). [CrossRef]
- López González, F.; Alarcón Osuna, M.A. Cambio generacional del consumo de frutas y verduras en México a través de un análisis de edad-periodo-cohorte 1994–2014. Población Salud Mesoamérica 2018, 15, 1–13. [Google Scholar] [CrossRef]
- Original, T.; Matías, D.; Pérez, E. Incremento en el Consumo de Fibra Dietética Complementaria al Tratamiento del Síndrome Metabólico. 2018, Volume 35, pp. 582–587. Available online: https://scielo.isciii.es/pdf/nh/v35n3/1699-5198-nh-35-03-00582.pdf (accessed on 12 January 2023). [CrossRef]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [PubMed]
- Agricultura O de las NU Para la A y la. Frutas y Verduras—Esenciales en tu Dieta Año Internacional. 2021. Available online: https://www.fao.org/3/cb2395es/cb2395es.pdf (accessed on 23 June 2021).
- Croz, D.M.; Bogard, J.R.; Sulser, T.B.; Cenacchi, N.; Dunston, S.; Herrero, M.; Wiebe, K. Articles Gaps between fruit and vegetable production, demand, and recommended consumption at global and national levels: An integrated modelling study. Lancet Planet. Health 2019, 3, e318–e329. [Google Scholar] [CrossRef]
- Parra, D.C.; de Costa-Louzada, M.L.; Moubarac, J.C.; Bertazzi-Levy, R.; Khandpur, N.; Cediel, G.; Monteiro, C.A. Association between ultra-processed food consumption and the nutrient profile of the Colombian diet in 2005. Salud Pública Mex 2019, 61, 147–154. [Google Scholar] [CrossRef]
- Silva, F.M.; Giatti, L.; de Figueiredo, R.C.; del Carmen Bisi Molina, M.; de Oliveira Cardoso, L.; Duncan, B.B.; Barreto, S.M. Consumption of ultra-processed food and obesity: Cross sectional result from the brazilian longitudinal study of adult health (ELSA-Brasil) cohort (2008–2010). Public Health Nutr. 2021, 12, 2271–2279. [Google Scholar] [CrossRef] [PubMed]
- Miramontes-Escobar, H.A.; Prado-Guzmán, G.A.; Toledo-Palomera MD, J.; Báez-García, J.E.; Sáyago-Ayerdi, S.G. Perfil nutricional según los niveles socio-económicos y menús proporcionados en un comedor social de México. Univ. Salud 2020, 22, 203–212. [Google Scholar] [CrossRef]
- González-zapata, L.I.; Restrepo-mesa, S.L.; Mancilla-lópez, L.; Sepúlveda-herrera, D.; Estrada-restrepo, A. Inequalities in food consumption the Colombian households: Results from the National Survey of Nutritional Status. Hacia Promoc Salud. 2021, 7577, 98–110. Available online: https://revistasojs.ucaldas.edu.co/index.php/hacialapromociondelasalud/article/view/4322/3974 (accessed on 23 June 2021). [CrossRef]
- Kern, D.M.; Auchincloss, A.H.; Stehr, M.F.; Roux AV, D.; Moore, K.A.; Kanter, G.P.; Robinson, L.F. Neighborhood price of healthier food relative to unhealthy food and its association with type 2 diabetes and insulin resistance: The Multi-Ethnic Study of Artherosclerosis. Prev. Med. 2018, 106, 122–129. [Google Scholar] [CrossRef]
- Lacko, A.; Delamater, P.; Gordon-Larsen, P.; Wen Ng, S. Geographic patterns and socioeconomic differences in the nutritional quality of household packaged food purchases in the United States. Health Place 2021, 69, 102567. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.; Mente, A.; Dehghan, M.; Rangarajan, S.; Zhang, X.; Swaminathan, S.; Dagenais, G.; Gupta, R.; Mohan, V.; Lear, S.; et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): A prospective cohort study. Lancet 2017, 390, 2037–2049. [Google Scholar] [CrossRef]
- Organizacion Panamericana de la salud. Módulos de Principios de Epidemiología para el Control de Enfermedades, 2nd ed.; OPS: Washington, DC, USA, 2002; p. 49. Available online: https://www3.paho.org/col/dmdocuments/MOPECE4.pdf (accessed on 2 December 2022).
- Jacquez, G.M. Cluster Morphology Analysis. NIH Public Access 2009, 1, 19–29. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2838429/pdf/nihms151579.pdf (accessed on 1 October 2022). [CrossRef]
- Ascuntar-tello, J.; Jaimes, F. Ronda clínica y epidemiológica: Sistemas de información geográfica [SIG] en salud. IATREIA 2016, 29, 97–103. [Google Scholar] [CrossRef]
- Karina, A.; Gu, H. Documento de Trabajo Sobre Economía Regional y Urbana. Vol. 304, Banco de la República. Cartagena. 2022. Available online: https://repositorio.banrep.gov.co/bitstream/handle/20.500.12134/10262/DTSERU_304.pdf (accessed on 24 September 2022).
- Ramírez, S.M.C.; Barbieri, A.F.; Rigotti, J.I.R. La migración interna en Colombia en la transición al siglo XXi. Rev Lat. Población. 2018, 12, 1–16. [Google Scholar]
- Rankin, S.; Hurtado, L.J.; Bonilla-Findji, O.; Mosquera, E.E.; Lundy, M. Perfil del Sistema Alimentario de Cali, Ciudad-Región; Centro Internacional de Agricultura Tropical: Cali, Colombia, 2021; 27p, Available online: https://hdl.handle.net/10568/114362 (accessed on 24 September 2022).
- Procolombia. Cadena de Agroalimentos 2021. Available online: https://www.camara.gov.co/sites/default/files/2021-08/ANEXO1MINCOMERCIO—Productos_potencial_exportador_agroindustrial_Colombia.pdf (accessed on 2 December 2022).
- Gómez-encino, G.C.; Cruz-león, A.; Zapata-Vázquez, R.; Morales, F. Nivel de Conocimiento que Tienen los Pacientes con Diabetes Mellitus Tipo 2 en Relación a su Enfermedad. 2015, Volume 21, pp. 17–25. Available online: https://www.redalyc.org/pdf/487/48742127004.pdf (accessed on 15 November 2022).
- MINAGRICULTURA D. Censo Nacional Agropecuario.pdf. 2014. Available online: https://www.dane.gov.co/files/CensoAgropecuario/entrega-definitiva/Boletin-10-produccion/10-presentacion.pdf (accessed on 3 November 2022).
- Hugo, V.; Castaño, A. Análisis de Situación de Salud (ASIS) Colombia. Bogotá-Colombia, 2016. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/ED/PSP/asis-colombia-2016.pdf (accessed on 3 October 2022).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).