
The Association between Plant-Based Diet Indices and Metabolic Syndrome in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey

 , , ,
, , , 
 and
and
Abstract
1. Introduction
2. Methods
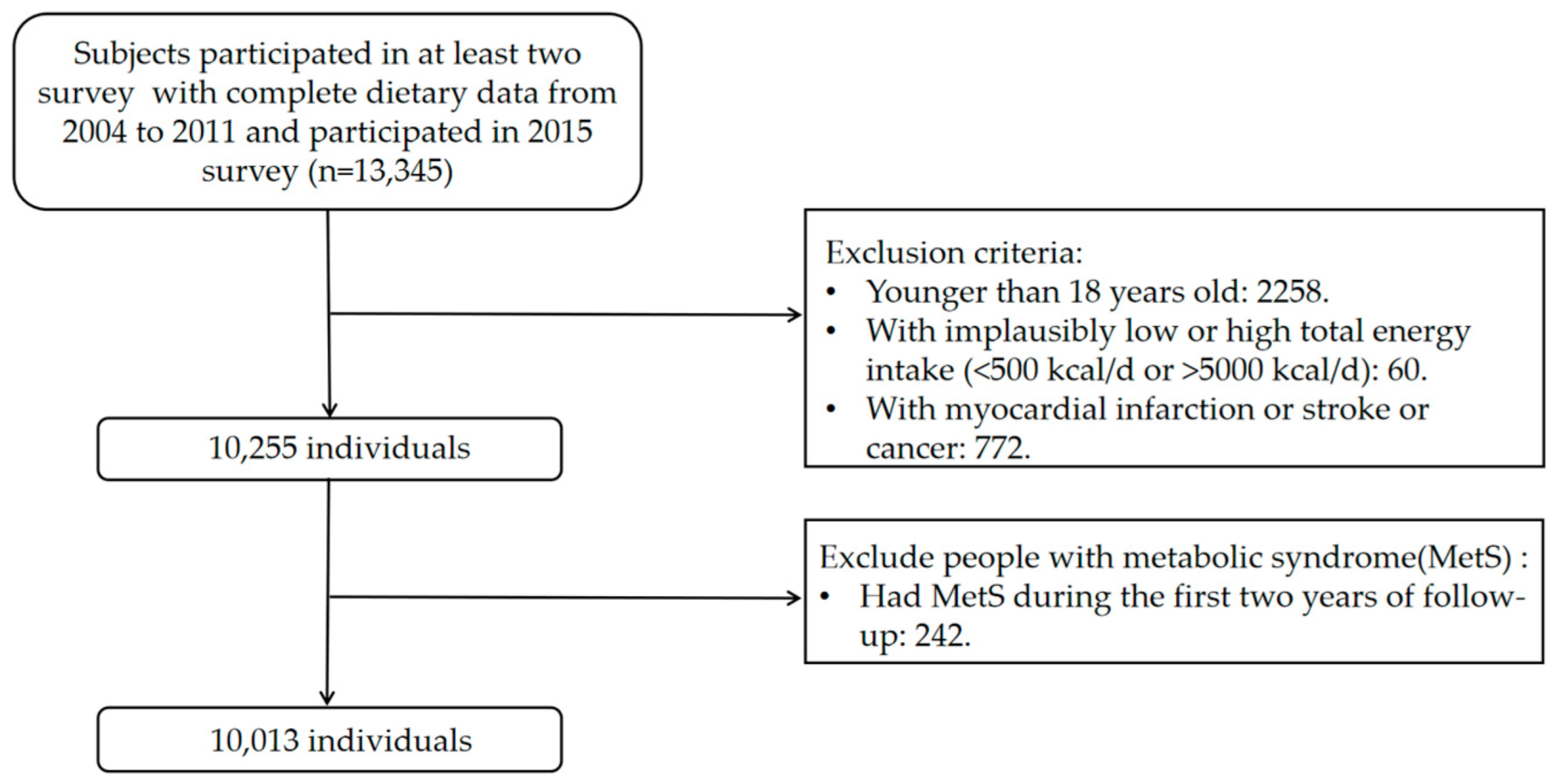
2.1. Study Design and Study Population
2.2. Plant-Based Diet Indices
2.3. Outcome Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Association between Plant-Based Diet Indices and MetS
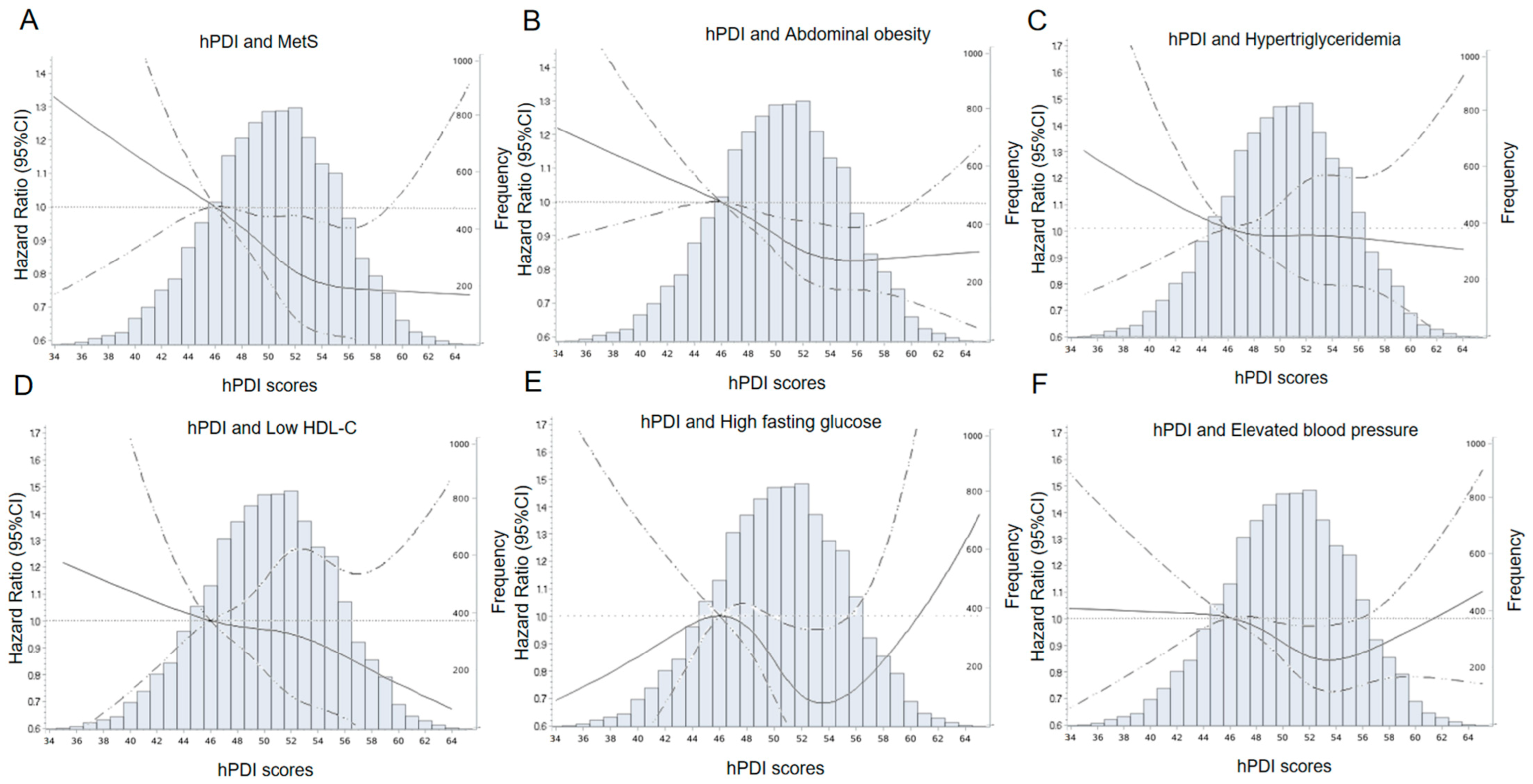
3.3. Explore Analysis
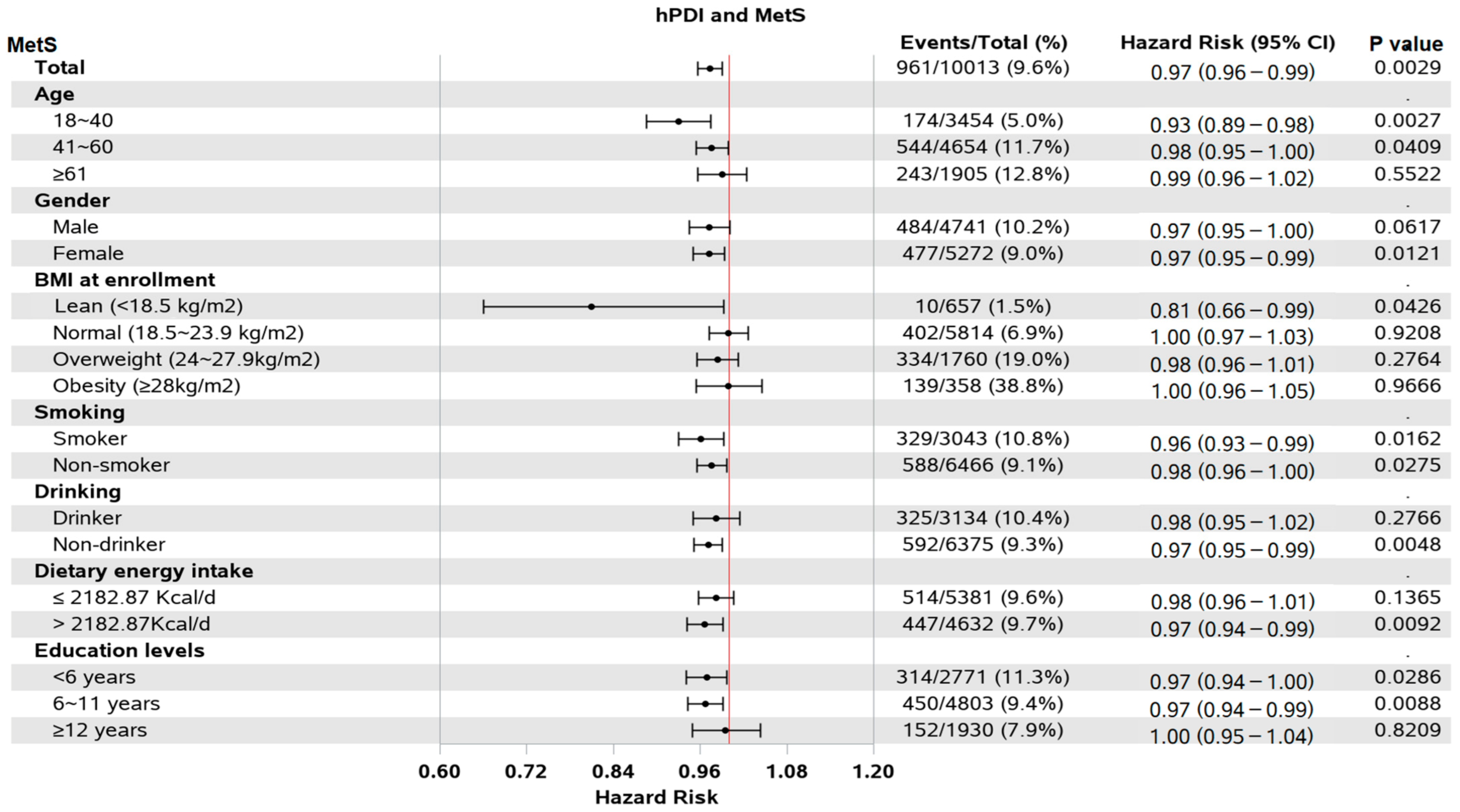
3.4. Subgroups and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maison, P.; Byrne, C.D.; Hales, C.N.; Day, N.E.; Wareham, N.J. Do Different Dimensions of the Metabolic Syndrome Change Together Over Time?: Evidence supporting obesity as the central feature. Diabetes Care 2001, 24, 1758–1763. [Google Scholar] [CrossRef] [PubMed]
- Kutschman, R.F.; Hadley, S. Diagnosing and treating metabolic syndrome. Geriatr. Nurs. 2004, 25, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The metabolic syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, P.; Mathangasinghe, Y.; Jayawardena, R.; Hills, A.P.; Misra, A. Prevalence and trends of metabolic syndrome among adults in the asia-pacific region: A systematic review. BMC Public Health 2017, 17, 101. [Google Scholar] [CrossRef]
- Li, R.; Li, W.; Lun, Z.; Zhang, H.; Sun, Z.; Kanu, J.S.; Qiu, S.; Cheng, Y.; Liu, Y. Prevalence of metabolic syndrome in Mainland China: A meta-analysis of published studies. BMC Public Health 2016, 16, 296. [Google Scholar] [CrossRef]
- Zimmet, P.; Alberti, K.G.; Shaw, J. Global and societal implications of the diabetes epidemic. Nature 2001, 414, 782–787. [Google Scholar] [CrossRef]
- Carr, D.B.; Utzschneider, K.M.; Hull, R.L.; Kodama, K.; Retzlaff, B.M.; Brunzell, J.D.; Shofer, J.B.; Fish, B.E.; Knopp, R.H.; Kahn, S.E. Intra-abdominal fat is a major determinant of the National Cholesterol Education Program Adult Treatment Panel III criteria for the metabolic syndrome. Diabetes 2004, 53, 2087–2094. [Google Scholar] [CrossRef]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Huang, R.Y.; Huang, C.C.; Hu, F.B.; Chavarro, J.E. Vegetarian Diets and Weight Reduction: A Meta-Analysis of Randomized Controlled Trials. J. Gen. Intern. Med. 2016, 31, 109–116. [Google Scholar] [CrossRef]
- Patel, H.; Chandra, S.; Alexander, S.; Soble, J.; Williams, K.A. Plant-Based Nutrition: An Essential Component of Cardiovascular Disease Prevention and Management. Curr. Cardiol. Rep. 2017, 19, 104. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, K.; Rebholz, C.M.; Kim, J. Plant-based diets and incident metabolic syndrome: Results from a South Korean prospective cohort study. PLoS Med. 2020, 17, e1003371. [Google Scholar] [CrossRef]
- Chen, Z.; Zuurmond, M.G.; van der Schaft, N.; Nano, J.; Wijnhoven, H.A.H.; Ikram, M.A.; Franco, O.H.; Voortman, T. Plant versus animal based diets and insulin resistance, prediabetes and type 2 diabetes: The Rotterdam Study. Eur. J. Epidemiol. 2018, 33, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant-Based Diets Are Associated with a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All-Cause Mortality in a General Population of Middle-Aged Adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar] [CrossRef] [PubMed]
- Trautwein, E.A.; McKay, S. The Role of Specific Components of a Plant-Based Diet in Management of Dyslipidemia and the Impact on Cardiovascular Risk. Nutrients 2020, 12, 2671. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Sánchez-Tainta, A.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Arós, F.; Gómez-Gracia, E.; Fiol, M.; Lamuela-Raventós, R.M.; Schröder, H.; et al. A provegetarian food pattern and reduction in total mortality in the Prevención con Dieta Mediterránea (PREDIMED) study. Am. J. Clin. Nutr. 2014, 100 (Suppl. S1), 320S–328S. [Google Scholar] [CrossRef]
- Storz, M.A. What makes a plant-based diet? A review of current concepts and proposal for a standardized plant-based dietary intervention checklist. Eur. J. Clin. Nutr. 2022, 76, 789–800. [Google Scholar] [CrossRef]
- Baden, M.Y.; Liu, G.; Satija, A.; Li, Y.; Sun, Q.; Fung, T.T.; Rimm, E.B.; Willett, W.C.; Hu, F.B.; Bhupathiraju, S.N. Changes in Plant-Based Diet Quality and Total and Cause-Specific Mortality. Circulation 2019, 140, 979–991. [Google Scholar] [CrossRef]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- Chen, J.P.; Chen, G.C.; Wang, X.P.; Qin, L.; Bai, Y. Dietary Fiber and Metabolic Syndrome: A Meta-Analysis and Review of Related Mechanisms. Nutrients 2017, 10, 24. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Chrysoula, L.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2021, 13, 1514. [Google Scholar] [CrossRef]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Liu, S.; Qu, J.; Li, X.; Hu, J.; Zhang, L.; Liu, X.; Li, X.; Wang, X.; Wen, L.; et al. A Lard and Soybean Oil Mixture Alleviates Low-Fat-High-Carbohydrate Diet-Induced Nonalcoholic Fatty Liver Disease in Mice. Nutrients 2022, 14, 560. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989-2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Li, J.; Li, S.; Zhang, B.; Du, S.; Gordon-Larsen, P.; Adair, L.; Popkin, B. The expanding burden of cardiometabolic risk in China: The China Health and Nutrition Survey. Obes. Rev. 2012, 13, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Zeng, J.; Qin, M.; Xu, W.; Zhang, Z.; Li, X.; Xu, S. The Association Between Plant-Based Diet Indices and Obesity and Metabolic Diseases in Chinese Adults: Longitudinal Analyses From the China Health and Nutrition Survey. Front. Nutr. 2022, 9, 881901. [Google Scholar] [CrossRef]
- Batis, C.; Sotres-Alvarez, D.; Gordon-Larsen, P.; Mendez, M.A.; Adair, L.; Popkin, B. Longitudinal analysis of dietary patterns in Chinese adults from 1991 to 2009. Br. J. Nutr. 2014, 111, 1441–1451. [Google Scholar] [CrossRef]
- Kim, H.; Rebholz, C.M.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Caulfield, L.E. Operational Differences in Plant-Based Diet Indices Affect the Ability to Detect Associations with Incident Hypertension in Middle-Aged US Adults. J. Nutr. 2019, 150, 842–850. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition Tables; Peking University Medical Press: Beijing, China, 2018. [Google Scholar]
- Hu, F.B.; Stampfer, M.J.; Rimm, E.; Ascherio, A.; Rosner, B.A.; Spiegelman, D.; Willett, W.C. Dietary Fat and Coronary Heart Disease: A Comparison of Approaches for Adjusting for Total Energy Intake and Modeling Repeated Dietary Measurements. Am. J. Epidemiol. 1999, 149, 531–540. [Google Scholar] [CrossRef]
- Yang, W. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition). Chin. J. Pract. Intern. Med. 2018, 38, 5–14. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.F. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults--study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Environ. Sci. 2002, 15, 83–96. [Google Scholar] [PubMed]
- Valeri, L.; VanderWeele, T.J. SAS macro for causal mediation analysis with survival data. Epidemiology 2015, 26, e23–e24. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S. Multiple imputation of discrete and continuous data by fully conditional specification. Stat. Methods Med. Res. 2007, 16, 219–242. [Google Scholar] [CrossRef]
- Lim, R.B.T.; Wee, W.K.; For, W.C.; Ananthanarayanan, J.A.; Soh, Y.H.; Goh, L.M.L.; Tham, D.K.T.; Wong, M.L. Correlates, Facilitators and Barriers of Healthy Eating Among Primary Care Patients with Prediabetes in Singapore—A Mixed Methods Approach. Nutrients 2019, 11, 1014. [Google Scholar] [CrossRef]
- Kao, F.J.; Chiu, Y.S.; Tsou, M.J.; Chiang, W.D. Effects of Chinese domestic cooking methods on the carotenoid composition of vegetables in Taiwan. LWT 2012, 46, 485–492. [Google Scholar] [CrossRef]
- Livingstone, M.B.; Pourshahidi, L.K. Portion size and obesity. Adv. Nutr. 2014, 5, 829–834. [Google Scholar] [CrossRef]
- Lutsey, P.L.; Steffen, L.M.; Stevens, J. Dietary intake and the development of the metabolic syndrome: The Atherosclerosis Risk in Communities study. Circulation 2008, 117, 754–761. [Google Scholar] [CrossRef]
- Kim, S.Y.; Freeland-Graves, J.H.; Kim, H.J. Nineteen-year trends in fermented food consumption and sodium intake from fermented foods for Korean adults from 1998 to 2016. Public Health Nutr. 2020, 23, 515–524. [Google Scholar] [CrossRef]
- Septembre-Malaterre, A.; Remize, F.; Poucheret, P. Fruits and vegetables, as a source of nutritional compounds and phytochemicals: Changes in bioactive compounds during lactic fermentation. Food Res. Int. 2018, 104, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, K.; Rebholz, C.M.; Kim, J. Association between unhealthy plant-based diets and the metabolic syndrome in adult men and women: A population-based study in South Korea. Br. J. Nutr. 2021, 125, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.M.; Chiu, T.H.T.; Chang, C.C.; Lin, M.N.; Lin, C.L. Plant-Based Diet, Cholesterol, and Risk of Gallstone Disease: A Prospective Study. Nutrients 2019, 11, 335. [Google Scholar] [CrossRef]
- Schösler, H.; de Boer, J.; Boersema, J.J.; Aiking, H. Meat and masculinity among young Chinese, Turkish and Dutch adults in the Netherlands. Appetite 2015, 89, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Tan, S.; Zhao, A.; Wang, M.; Wang, P.; Zhang, Y. Association between nutrient patterns and serum lipids in Chinese adult women: A cross-sectional study. Nutr. Diet. 2019, 76, 184–191. [Google Scholar] [CrossRef]
- Allès, B.; Baudry, J.; Méjean, C.; Touvier, M.; Péneau, S.; Hercberg, S.; Kesse-Guyot, E. Comparison of Sociodemographic and Nutritional Characteristics between Self-Reported Vegetarians, Vegans, and Meat-Eaters from the NutriNet-Santé Study. Nutrients 2017, 9, 1023. [Google Scholar] [CrossRef]
- González-Rodríguez, L.G.; Perea Sánchez, J.M.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. Intake and Dietary Food Sources of Fibre in Spain: Differences with Regard to the Prevalence of Excess Body Weight and Abdominal Obesity in Adults of the ANIBES Study. Nutrients 2017, 9, 326. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.A.; Thomas, K.S. Increasing total fiber intake reduces risk of weight and fat gains in women. J. Nutr. 2009, 139, 576–581. [Google Scholar] [CrossRef]
- Solah, V.A.; Kerr, D.A.; Hunt, W.J.; Johnson, S.K.; Boushey, C.J.; Delp, E.J.; Meng, X.; Gahler, R.J.; James, A.P.; Mukhtar, A.S.; et al. Erratum: Effect of Fibre Supplementation on Body Weight and Composition, Frequency of Eating and Dietary Choice in Overweight Individuals. Nutrients 2017, 9, 149. [Google Scholar] [CrossRef]
- Farrell, P.; Negin, J.; Awoke, M.; Thow, A.M.; Taua, M.; Faumuina, T.; Mihrshahi, S.; Vizintin, P.; Richards, J. Associations between sociodemographic and behaviour factors, and dietary risk factors for overweight and obesity, in Samoan women. Appetite 2019, 134, 155–161. [Google Scholar] [CrossRef]
- Cominato, L.; Di Biagio, G.F.; Lellis, D.; Franco, R.R.; Mancini, M.C.; de Melo, M.E. Obesity Prevention: Strategies and Challenges in Latin America. Curr. Obes. Rep. 2018, 7, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Aminianfar, A.; Hassanzadeh Keshteli, A.; Esmaillzadeh, A.; Adibi, P. Association between adherence to MIND diet and general and abdominal obesity: A cross-sectional study. Nutr. J. 2020, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Kesztyüs, D.; Erhardt, J.; Schönsteiner, D.; Kesztyüs, T. Therapeutic Treatment for Abdominal Obesity in Adults. Dtsch. Arztebl. Int. 2018, 115, 487–493. [Google Scholar] [CrossRef]
- Gutiérrez-Pliego, L.E.; Camarillo-Romero Edel, S.; Montenegro-Morales, L.P.; Garduño-García Jde, J. Dietary patterns associated with body mass index (BMI) and lifestyle in Mexican adolescents. BMC Public Health 2016, 16, 850. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.J.; Oldmeadow, C.; Mishra, G.D.; Garg, M.L. Plant-based dietary patterns are associated with lower body weight, BMI and waist circumference in older Australian women. Public Health Nutr. 2022, 25, 18–31. [Google Scholar] [CrossRef]
- Jaceldo-Siegl, K.; Estevez, D.; Fraser, G.E.; Hayes-Bautista, D.E.; Flores, H.; Jordan, M.; Singh, P.N. Plant-Based Diets in Hispanic/Latino Adult Adventists in the United States and Their Association With Body Mass Index. Am. J. Health Promot. 2019, 33, 869–875. [Google Scholar] [CrossRef]
- Kim, N.H.; Lee, J.; Kim, T.J.; Kim, N.H.; Choi, K.M.; Baik, S.H.; Choi, D.S.; Pop-Busui, R.; Park, Y.; Kim, S.G. Body Mass Index and Mortality in the General Population and in Subjects with Chronic Disease in Korea: A Nationwide Cohort Study (2002–2010). PLoS ONE 2015, 10, e0139924. [Google Scholar] [CrossRef]
- Gurka, M.J.; Filipp, S.L.; Musani, S.K.; Sims, M.; DeBoer, M.D. Use of BMI as the marker of adiposity in a metabolic syndrome severity score: Derivation and validation in predicting long-term disease outcomes. Metabolism 2018, 83, 68–74. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | p Value b |
|---|---|---|---|---|---|---|
| hPDI | ||||||
| Sample size, n | 2033 | 2175 | 2481 | 1366 | 1958 | |
| Median score (range) | 44 (34–46) | 48 (47–49) | 51 (50–52) | 53 (53–54) | 56 (55–65) | <0.001 |
| Age, year | 47.5 ± 15.0 | 46.3 ± 14.6 | 46.1 ± 14.7 | 46.9 ± 14.9 | 47.8 ± 14.4 | <0.001 |
| Female, % | 1017 (50.0) | 1059 (48.7) | 1160 (46.8) | 616 (45.1) | 889 (45.4) | 0.009 |
| Urban, % | 1006 (51.4) | 786 (38.1) | 767 (32.8) | 335 (26.1) | 406 (21.8) | <0.001 |
| Education, year | ||||||
| 0–6 | 399 (20.4) | 519 (25.1) | 645 (27.6) | 421 (32.8) | 787 (42.2) | <0.001 |
| 6–11 | 972 (49.7) | 1080 (52.3) | 1216 (52.0) | 665 (51.9) | 870 (46.6) | |
| ≥12 | 583 (29.8) | 466 (22.6) | 476 (20.4) | 196 (15.3) | 209 (11.2) | |
| BMI, kg/m2 | ||||||
| Lean (<18.5) | 118 (6.7) | 135 (7.2) | 166 (7.9) | 98 (8.5) | 140 (8.2) | <0.001 |
| Normal (18.5~23.9) | 1104 (62.6) | 1227 (65.8) | 1444 (68.8) | 799 (68.9) | 1240 (72.8) | |
| Overweight (24~27.9) | 442 (25.1) | 411 (22.1) | 395 (18.8) | 226 (19.5) | 286 (16.8) | |
| Obesity (≥28) | 100 (5.7) | 91 (4.9) | 94 (4.5) | 36 (3.1) | 37 (2.2) | |
| Smoking, % | 667 (34.1) | 686 (33.2) | 714 (30.5) | 402 (31.4) | 574 (30.7) | 0.054 |
| Drinking, % | 738 (37.7) | 678 (32.8) | 755 (32.3) | 378 (29.5) | 585 (31.3) | <0.001 |
| SBP, mmHg | 121.1 ± 16.5 | 121.7 ± 17.4 | 120.4 ± 17.2 | 120.7 ± 18.3 | 120.6 ± 18.1 | 0.111 |
| DBP, mmHg | 78.9 ± 10.7 | 78.9 ± 10.8 | 77.9 ± 10.6 | 77.9 ± 10.7 | 77.8 ± 11.0 | <0.001 |
| Physical activity, MET-H/d | 20.9 ± 16.4 | 22.1 ± 18.6 | 22.6 ± 18.0 | 22.7 ± 18.8 | 24.2 ± 19.6 | <0.001 |
| Healthy plant foods c | 9.6 ± 2.3 | 10.7 ± 2.1 | 11.7 ± 2.0 | 12.8 ± 1.8 | 14.2 ± 1.9 | <0.001 |
| Less-healthy plant foods d | 20.4 ± 2.3 | 21.7 ± 2.1 | 22.5 ± 1.8 | 23.1 ± 1.7 | 23.9 ± 1.4 | <0.001 |
| Animal foods e | 13.7 ± 3.0 | 15.6 ± 2.6 | 16.8 ± 2.2 | 17.6 ± 1.9 | 18.7 ± 1.6 | <0.001 |
| Total Energy, kcal | 2177.7 ± 658.6 | 2149.3 ± 671.9 | 2142.2 ± 645.5 | 2188.1 ± 648.2 | 2273.4 ± 638.1 | <0.001 |
| Total Carbohydrate, g | 277.6 ± 94.8 | 293.0 ± 98.3 | 311.7 ± 101.8 | 336.9 ± 109.7 | 371.2 ± 114.8 | <0.001 |
| Total Fat, g | 83.2 ± 39.5 | 76.6 ± 39.5 | 68.2 ± 34.4 | 63.8 ± 33.4 | 55.8 ± 31.3 | <0.001 |
| Total Protein, g | 71.9 ± 24.8 | 67.3 ± 24.1 | 64.2 ± 23.7 | 64.1 ± 22.5 | 65.7 ± 22.9 | <0.001 |
| uPDI | ||||||
| Sample size, n | 2674 | 1607 | 2416 | 1461 | 1855 | |
| Median score (range) | 43 (28–45) | 47 (46–47) | 49 (48–50) | 51 (51–52) | 55 (53–65) | <0.001 |
| Age, year | 47.0 ± 15.0 | 46.5 ± 14.5 | 46.7 ± 14.9 | 46.3 ± 14.4 | 45.2 ± 14.0 | 0.001 |
| Female, % | 1470 (55.0) | 847 (52.7) | 1299 (53.8) | 737 (50.4) | 919 (49.5) | <0.001 |
| Urban, % | 1139 (44.6) | 568 (36.8) | 764 (33.2) | 383 (27.8) | 446 (25.8) | <0.001 |
| Education, year | ||||||
| 0–6 | 561 (22.0) | 447 (28.9) | 716 (31.1) | 452 (32.8) | 595 (34.5) | |
| 6–11 | 1264 (49.6) | 771 (49.9) | 1171 (50.9) | 702 (50.9) | 895 (51.8) | <0.001 |
| ≥12 | 725 (28.4) | 327 (21.2) | 416 (18.1) | 225 (16.3) | 237 (13.7) | |
| BMI, kg/m2 | ||||||
| Lean (<18.5) | 183 (7.9) | 108 (7.8) | 172 (8.3) | 88 (7.0) | 106 (6.8) | |
| Normal (18.5~23.9) | 1555 (67.4) | 962 (69.1) | 1414 (67.8) | 845 (67.6) | 1038 (66.8) | 0.577 |
| Overweight (24~27.9) | 470 (20.4) | 259 (18.6) | 418 (20.0) | 266 (21.3) | 347 (22.3) | |
| Obesity (≥28) | 98 (4.3) | 64 (4.6) | 82 (3.9) | 51 (4.1) | 63 (4.1) | |
| Smoking, % | 734 (28.8) | 498 (32.2) | 755 (32.8) | 462 (33.5) | 594 (34.4) | <0.001 |
| Drinking, % | 806 (31.6) | 535 (34.6) | 764 (33.2) | 460 (33.3) | 569 (33.0) | 0.366 |
| SBP, mmHg | 120.6 ± 17.5 | 120.8 ± 16.9 | 121.0 ± 17.7 | 121.7 ± 18.1 | 120.8 ± 17.0 | 0.454 |
| DBP, mmHg | 77.7 ± 9.9 | 78.4 ± 10.2 | 78.2 ± 11.1 | 79.3 ± 10.7 | 79.1 ± 11.5 | <0.001 |
| Physical activity, MET-H/d | 20.7 ± 15.9 | 21.6 ± 17.5 | 23.1 ± 18.8 | 23.8 ± 19.2 | 24.2 ± 20.4 | <0.001 |
| Healthy plant foods | 22.5 ± 2.3 | 23.6 ± 2.1 | 24.4 ± 2.1 | 25.3 ± 2.0 | 26.6 ± 1.9 | <0.001 |
| Less-healthy plant foods | 6.3 ± 1.6 | 6.8 ± 1.8 | 7.6 ± 1.8 | 8.5 ± 1.9 | 10.1 ± 2.1 | <0.001 |
| Animal foods | 13.9 ± 2.8 | 16.2 ± 2.4 | 16.9 ± 2.3 | 17.7 ± 2.1 | 18.5 ± 1.7 | <0.001 |
| Total Energy, kcal | 2191.2 ± 626.4 | 2183.1 ± 615.1 | 2167.5 ± 656.5 | 2198.1 ± 673.7 | 2178.6 ± 707.6 | 0.623 |
| Total Carbohydrate, g | 299.9 ± 100.0 | 316.6 ± 104.4 | 314.9 ± 107.9 | 331.1 ± 119.0 | 327.0 ± 113.2 | <0.001 |
| Total Fat, g | 74.5 ± 35.4 | 69.0 ± 34.7 | 69.1 ± 37.7 | 67.3 ± 37.3 | 68.1 ± 40.6 | <0.001 |
| Total Protein, g | 75.6 ± 23.95 | 67.1 ± 22.1 | 64.8 ± 23.4 | 62.6 ± 22.3 | 59.2 ± 23.1 | <0.001 |
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | p-Trend | |
|---|---|---|---|---|---|---|
| hPDI | ||||||
| Incidence Mets | ||||||
| cases/total | 223/2016 | 232/2164 | 219/2472 | 115/1357 | 172/1940 | |
| Crude model | Reference | 0.91 (0.75, 1.09) | 0.71 (0.59, 0.86) | 0.64 (0.51, 0.81) | 0.63 (0.51, 0.77) | <0.001 |
| Adjusted model * | Reference | 0.94 (0.76, 1.16) | 0.74 (0.59, 0.93) | 0.74 (0.57, 0.97) | 0.72 (0.56, 0.93) | 0.021 |
| Abdominal obesity | ||||||
| cases/total | 723/2016 | 742/2164 | 807/2472 | 412/1357 | 616/1940 | |
| Crude model | Reference | 0.90 (0.81, 1.00) | 0.79 (0.72, 0.87) | 0.69 (0.62, 0.78) | 0.68 (0.61, 0.76) | <0.001 |
| Adjusted model | Reference | 0.93 (0.83, 1.05) | 0.88 (0.78, 0.99) | 0.79 (0.68, 0.91) | 0.80 (0.70, 0.92) | 0.004 |
| Hypertriglyceridemia | ||||||
| cases/total | 231/384 | 239/437 | 227/406 | 133/234 | 190/362 | |
| Crude model | Reference | 0.89 (0.74, 1.07) | 0.89 (0.74, 1.07) | 0.92 (0.75, 1.14) | 0.82 (0.67, 0.99) | 0.354 |
| Adjusted model | Reference | 0.91 (0.73, 1.13) | 0.91 (0.72, 1.14) | 0.95 (0.72, 1.23) | 0.87 (0.68, 1.13) | 0.844 |
| Low HDL-C | ||||||
| cases/total | 130/384 | 116/437 | 122/406 | 63/234 | 90/362 | |
| Crude model | Reference | 0.78 (0.61, 1.00) | 0.86 (0.67, 1.10) | 0.79 (0.59, 1.07) | 0.71 (0.54, 0.93) | 0.110 |
| Adjusted model | Reference | 0.75 (0.55, 1.03) | 0.92 (0.67, 1.27) | 0.89 (0.61, 1.30) | 0.74 (0.51, 1.08) | 0.331 |
| High fasting glucose | ||||||
| cases/total | 78/2016 | 96/2164 | 88/2472 | 39/1357 | 58/1940 | |
| Crude model | Reference | 1.04 (0.77, 1.41) | 0.79 (0.59, 1.08) | 0.59 (0.40, 0.87) | 0.57 (0.41, 0.80) | <0.001 |
| Adjusted model | Reference | 1.21 (0.86, 1.70) | 0.83 (0.57, 1.21) | 0.89 (0.57, 1.38) | 0.84 (0.55, 1.28) | 0.224 |
| Elevated blood pressure | ||||||
| cases/total | 796/2016 | 904/2164 | 973/2472 | 520/1357 | 863/1940 | |
| Crude model | Reference | 0.97 (0.89, 1.07) | 0.85 (0.78, 0.94) | 0.78 (0.69, 0.87) | 0.84 (0.76, 0.92) | <0.001 |
| Adjusted model | Reference | 0.96 (0.86, 1.08) | 0.91 (0.81, 1.02) | 0.83 (0.73, 0.95) | 0.94 (0.83, 1.06) | 0.070 |
| uPDI | ||||||
| Incidence Mets | ||||||
| cases/total | 251/2662 | 137/1600 | 223/2399 | 154/1452 | 196/1836 | |
| Crude model | Reference | 0.88 (0.72, 1.09) | 0.95 (0.79, 1.13) | 1.04 (0.85, 1.28) | 1.08 (0.89, 1.30) | 0.398 |
| Adjusted model | Reference | 0.97 (0.76, 1.24) | 1.07 (0.86, 1.33) | 1.26 (0.99, 1.62) | 1.31 (1.03, 1.66) | 0.075 |
| Abdominal obesity | ||||||
| cases/total | 821/2662 | 515/1600 | 777/2399 | 513/1452 | 674/1836 | |
| Crude model | Reference | 1.01 (0.90, 1.13) | 1.02 (0.92, 1.12) | 1.09 (0.98, 1.22) | 1.10 (0.99, 1.22) | 0.246 |
| Adjusted model | Reference | 1.16 (1.02, 1.31) | 1.14 (1.02, 1.28) | 1.35 (1.19, 1.54) | 1.36 (1.20, 1.54) | <0.001 |
| Hypertriglyceridemia | ||||||
| cases/total | 270/486 | 158/276 | 241/440 | 158/283 | 193/338 | |
| Crude model | Reference | 1.07 (0.88, 1.30) | 0.97 (0.81, 1.15) | 0.95 (0.78, 1.15) | 1.05 (0.87, 1.26) | 0.781 |
| Adjusted model | Reference | 1.05 (0.82, 1.32) | 0.92 (0.74, 1.14) | 0.93 (0.73, 1.19) | 1.12 (0.88, 1.42) | 0.465 |
| Low HDL-C | ||||||
| cases/total | 130/486 | 78/276 | 112/440 | 95/283 | 106/338 | |
| Crude model | Reference | 1.07 (0.80, 1.41) | 0.94 (0.73, 1.21) | 1.18 (0.90, 1.54) | 1.18 (0.91, 1.52) | 0.361 |
| Adjusted model | Reference | 1.09 (0.76, 1.55) | 0.97 (0.70, 1.33) | 1.24 (0.88, 1.76) | 1.37 (0.97, 1.94) | 0.255 |
| High fasting glucose | ||||||
| cases/total | 107/2662 | 54/1600 | 88/2399 | 52/1452 | 58/1836 | |
| Crude model | Reference | 0.83 (0.60, 1.15) | 0.88 (0.67, 1.17) | 0.85 (0.61, 1.18) | 0.76 (0.55, 1.05) | 0.521 |
| Adjusted model | Reference | 0.97 (0.67, 1.42) | 1.08 (0.77, 1.50) | 0.95 (0.63, 1.44) | 0.91 (0.61, 1.38) | 0.938 |
| Elevated blood pressure | ||||||
| cases/total | 1053/2662 | 634/1600 | 964/2399 | 601/1452 | 804/1836 | |
| Crude model | Reference | 0.98 (0.89, 1.08) | 0.99 (0.91, 1.08) | 1.01 (0.91, 1.11) | 1.04 (0.95, 1.14) | 0.802 |
| Adjusted model | Reference | 1.05 (0.94, 1.18) | 1.08 (0.97, 1.20) | 1.16 (1.03, 1.31) | 1.15 (1.02, 1.29) | 0.092 |
| Effect * | CDE (Controlled Direct Effect) | PNDE (Pure Natural Direct Effect) | TNIE (Total Natural Indirect Effect) | TNDE (Total Natural Direct Effect) | PNIE (Pure Natural Indirect Effect) | TE (Total Effect) | PM (Proportion Mediated) |
|---|---|---|---|---|---|---|---|
| BMI and MetS | −0.063 (−0.084, −0.041) | −0.019 (−0.022, −0.016) | −0.007 (−0.010, −0.015) | −0.019 (−0.022, −0.016) | −0.007 (−0.010, −0.005) | −0.026 (−0.030, −0.022) | 0.278 (0.203, 0.353) |
| BMI and Abdominal obesity | −0.053 (−0.066, −0.042) | −0.016 (−0.017, −0.014) | −0.007 (−0.008, −0.005) | −0.016 (−0.018, −0.014) | −0.007 (−0.008, −0.005) | −0.022 (−0.025, −0.020) | 0.297 (0.250, 0.343) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huo, Y.; Cao, S.; Liu, J.; Zhang, B.; Xu, K.; Wang, Y.; Liu, H.; Yang, P.; Zeng, L.; Yan, H.; et al. The Association between Plant-Based Diet Indices and Metabolic Syndrome in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey. Nutrients 2023, 15, 1341. https://doi.org/10.3390/nu15061341
Huo Y, Cao S, Liu J, Zhang B, Xu K, Wang Y, Liu H, Yang P, Zeng L, Yan H, et al. The Association between Plant-Based Diet Indices and Metabolic Syndrome in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey. Nutrients. 2023; 15(6):1341. https://doi.org/10.3390/nu15061341
Chicago/Turabian StyleHuo, Yating, Suixia Cao, Jingchun Liu, Binyan Zhang, Kun Xu, Yutong Wang, Huimeng Liu, Peiying Yang, Lingxia Zeng, Hong Yan, and et al. 2023. "The Association between Plant-Based Diet Indices and Metabolic Syndrome in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey" Nutrients 15, no. 6: 1341. https://doi.org/10.3390/nu15061341
APA StyleHuo, Y., Cao, S., Liu, J., Zhang, B., Xu, K., Wang, Y., Liu, H., Yang, P., Zeng, L., Yan, H., Dang, S., & Mi, B. (2023). The Association between Plant-Based Diet Indices and Metabolic Syndrome in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey. Nutrients, 15(6), 1341. https://doi.org/10.3390/nu15061341