
Influence of Sociodemographic Variables and Healthy Habits on the Values of Insulin Resistance Indicators in 386,924 Spanish Workers


 , ,
, ,
Abstract
:1. Introduction
2. Methods
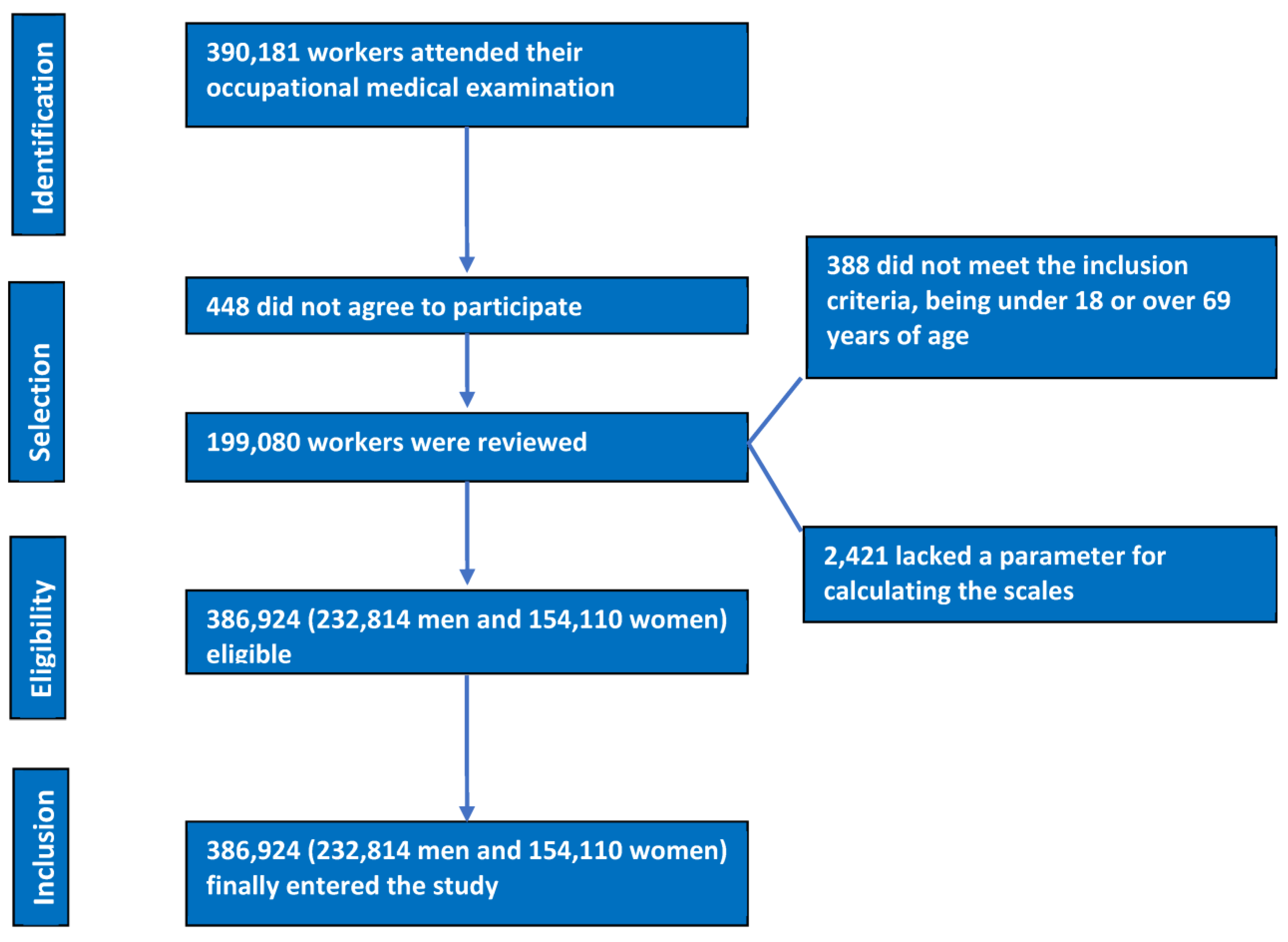
2.1. Inclusion Criteria
- Being between 18 and 69 years old.
- Having an employment contract with one of the companies participating in this study.
- Agreeing to participate in this study.
- Allowing the use of the data for epidemiological purposes.
2.2. Determination of Variables
- -
- Anamnesis. Owing to an exhaustive clinical history, the data on sociodemographic variables (age, sex, social class, and level of education) and healthy habits (tobacco, alcohol, Mediterranean diet, and physical activity) were collected.
- -
- Anthropometric and clinical determinations. These included height, weight, waist circumference, and systolic and diastolic blood pressure.
- -
- Analytical determinations. Lipid profiles and glycaemia were determined.
- Different scales were calculated to evaluate the risk of insulin resistance (IR).
- Metabolic insulin resistance score (METS-IR) [48].
- METS-IR = Ln [(2 glycaemia) + triglycerides] BMI)/(Ln[HDL-c]). Values were considered high from 50 up.
- TyG index [49] and its variants:
- ○
- TyG index = Ln [triglycerides (mg/dL) glycaemia (mg/dL)/2]. Values were considered high from 8.72 up in men and 8.67 up in women [50].
- ○
- TyG-BMI was obtained by multiplying the TyG index by the BMI. Its cut-off point was 191.53 [51].
- ○
- TyG-waist circumference [52]. This was obtained by multiplying the TyG index by the waist circumference.
- Triglycerides/HDL-c [53]. Values were considered high from 2.4 up. This was obtained by dividing the value of triglycerides by the value of HDL cholesterol.
- -
- Social class I. This includes management personnel, professionals with university training, professional athletes, and artists.
- -
- Social class II. This includes intermediate professions and qualified self-employed workers.
- -
- Social class III. This includes low-skilled workers.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freeman, A.M.; Pennings, N. Insulin Resistance. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Yang, W.; Jiang, W.; Guo, S. Regulation of Macronutrients in Insulin Resistance and Glucose Homeostasis during Type 2 Diabetes Mellitus. Nutrients 2023, 15, 4671. [Google Scholar] [CrossRef] [PubMed]
- Gołacki, J.; Matuszek, M.; Matyjaszek-Matuszek, B. Link between Insulin Resistance and Obesity-From Diagnosis to Treatment. Diagnostics 2022, 12, 1681. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S. Sociodemographic variables influencing the prevalence of insulin resistance in the italian population. Acad. J. Health Sci. 2022, 37, 107–112. [Google Scholar] [CrossRef]
- Klein, S.; Gastaldelli, A.; Yki-Järvinen, H.; Scherer, P.E. Why does obesity cause diabetes? Cell Metab. 2022, 34, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chi, X.; Wang, Y.; Setrerrahmane, S.; Xie, W.; Xu, H. Trends in insulin resistance: Insights into mechanisms and therapeutic strategy. Signal Transduct. Target Ther. 2022, 7, 216. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Gortan Cappellari, G.; Ragni, M.; Nisoli, E. Insulin resistance in obesity: An overview of fundamental alterations. Eat Weight Disord. 2018, 23, 149–157. [Google Scholar] [CrossRef]
- Constantin-Teodosiu, D.; Constantin, D. Molecular Mechanisms of Muscle Fatigue. Int. J. Mol. Sci. 2021, 22, 11587. [Google Scholar] [CrossRef]
- Tagi, V.M.; Mainieri, F.; Chiarelli, F. Hypertension in Patients with Insulin Resistance: Etiopathogenesis and Management in Children. Int. J. Mol. Sci. 2022, 23, 5814. [Google Scholar] [CrossRef]
- Bjornstad, P.; Eckel, R.H. Pathogenesis of Lipid Disorders in Insulin Resistance: A Brief Review. Curr. Diab. Rep. 2018, 18, 127. [Google Scholar] [CrossRef]
- Park, J.J. Epidemiology, Pathophysiology, Diagnosis and Treatment of Heart Failure in Diabetes. Diabetes Metab. J. 2021, 45, 146–157. [Google Scholar] [CrossRef]
- Kosmas, C.E.; Bousvarou, M.D.; Kostara, C.E.; Papakonstantinou, E.J.; Salamou, E.; Guzman, E. Insulin resistance and cardiovascular disease. J. Int. Med. Res. 2023, 51, 3000605231164548. [Google Scholar] [CrossRef] [PubMed]
- González-Saldivar, G.; Rodríguez-Gutiérrez, R.; Ocampo-Candiani, J.; González-González, J.G.; Gómez-Flores, M. Skin Manifestations of Insulin Resistance: From a Biochemical Stance to a Clinical Diagnosis and Management. Dermatol. Ther. 2017, 7, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Radu, A.M.; Carsote, M.; Dumitrascu, M.C.; Sandru, F. Acanthosis Nigricans: Pointer of Endocrine Entities. Diagnostics 2022, 12, 2519. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.A.; Li, H.; Li, W.; Pan, K.; Yee, J.K.; Chlebowski, R.T.; Lee, D.J. Association between baseline insulin resistance and psoriasis incidence: The Women’s Health Initiative. Arch. Dermatol. Res. 2022, 314, 869–880. [Google Scholar] [CrossRef] [PubMed]
- Guest, P.C. Insulin Resistance in Schizophrenia. Adv. Exp. Med. Biol. 2019, 1134, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Calkin, C.V. Insulin resistance takes center stage: A new paradigm in the progression of bipolar disorder. Ann. Med. 2019, 51, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, B.S.; Salagre, E.; Enduru, N.; Grande, I.; Vieta, E.; Zhao, Z. Insulin resistance in depression: A large meta-analysis of metabolic parameters and variation. Neurosci. Biobehav. Rev. 2022, 139, 104758. [Google Scholar] [CrossRef]
- He, Y.; Tong, L.; Guo, F.; Zhao, S.; Zhang, J.; Guo, X.; Tao, Y.; Lin, X.; Jin, L. Depression status and insulin resistance in adults with obesity: A cross-sectional study. J. Psychosom. Res. 2022, 163, 111049. [Google Scholar] [CrossRef]
- Cui, Y.; Tang, T.Y.; Lu, C.Q.; Ju, S. Insulin Resistance and Cognitive Impairment: Evidence from Neuroimaging. J. Magn. Reson. Imaging 2022, 56, 1621–1649. [Google Scholar] [CrossRef]
- Calcaterra, V.; Verduci, E.; Cena, H.; Magenes, V.C.; Todisco, C.F.; Tenuta, E.; Gregorio, C.; De Giuseppe, R.; Bosetti, A.; Di Profio, E.; et al. Polycystic Ovary Syndrome in Insulin-Resistant Adolescents with Obesity: The Role of Nutrition Therapy and Food Supplements as a Strategy to Protect Fertility. Nutrients 2021, 13, 1848. [Google Scholar] [CrossRef]
- Chen, T.; Yu, Y.; Jia, F.; Luan, P.; Liu, X. The relationship between polycystic ovary syndrome and insulin resistance from 1983 to 2022: A bibliometric analysis. Front. Public Health 2022, 10, 960965. [Google Scholar] [CrossRef] [PubMed]
- Bellou, V.; Belbasis, L.; Tzoulaki, I.; Evangelou, E. Risk factors for type 2 diabetes mellitus: An exposure-wide umbrella review of meta-analyses. PLoS ONE 2018, 13, e0194127. [Google Scholar] [CrossRef] [PubMed]
- Koren, D.; Taveras, E.M. Association of sleep disturbances with obesity, insulin resistance and the metabolic syndrome. Metabolism 2018, 84, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Park, S.Y.; Choi, C.S. Insulin Resistance: From Mechanisms to Therapeutic Strategies. Diabetes Metab. J. 2022, 46, 15–37. [Google Scholar] [CrossRef]
- Gasmi, A.; Noor, S.; Menzel, A.; Doşa, A.; Pivina, L.; Bjørklund, G. Obesity and Insulin Resistance: Associations with Chronic Inflammation, Genetic and Epigenetic Factors. Curr. Med. Chem. 2021, 28, 800–826. [Google Scholar] [CrossRef]
- Sampath Kumar, A.; Maiya, A.G.; Shastry, B.A.; Vaishali, K.; Ravishankar, N.; Hazari, A.; Gundmi, S.; Jadhav, R. Exercise and insulin resistance in type 2 diabetes mellitus: A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2019, 62, 98–103. [Google Scholar] [CrossRef]
- Prana, V.; Tieri, P.; Palumbo, M.C.; Mancini, E.; Castiglione, F. Modeling the Effect of High Calorie Diet on the Interplay between Adipose Tissue, Inflammation, and Diabetes. Comput. Math Methods Med. 2019, 2019, 7525834. [Google Scholar] [CrossRef]
- Ahmed, B.; Sultana, R.; Greene, M.W. Adipose tissue and insulin resistance in obese. Biomed. Pharmacother. 2021, 137, 111315. [Google Scholar] [CrossRef]
- Borel, A.L. Sleep Apnea and Sleep Habits: Relationships with Metabolic Syndrome. Nutrients 2019, 11, 2628. [Google Scholar] [CrossRef]
- Gil Llinás, M.; Estades Janer, M.P.; Rosselló Janer, M.E.; Ragosin Sepúlveda, M.C. Role of occupational nursing in the early detection of people at high risk of insulin resistance. Acad. J. Health Sci. 2022, 37, 107–114. [Google Scholar] [CrossRef]
- Napoleão, A.; Fernandes, L.; Miranda, C.; Marum, A.P. Effects of Calorie Restriction on Health Span and Insulin Resistance: Classic Calorie Restriction Diet vs. Ketosis-Inducing Diet. Nutrients 2021, 13, 1302. [Google Scholar] [CrossRef] [PubMed]
- Mikusova, V.; Mikus, J.; Grilusova, K.; Roncakova, M.; Benko, J.; Martinka, E. Insulin resistance and need for a lifestyle change to eliminate it. Bratisl. Lek. Listy. 2021, 122, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Hansen, D.; De Strijcker, D.; Calders, P. Impact of Endurance Exercise Training in the Fasted State on Muscle Biochemistry and Metabolism in Healthy Subjects: Can These Effects be of Particular Clinical Benefit to Type 2 Diabetes Mellitus and Insulin-Resistant Patients? Sports Med. 2017, 47, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Battista, F.; Ermolao, A.; van Baak, M.A.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraça, E.V.; Encantado, J.; Dicker, D.; Farpour-Lambert, N.; et al. Effect of exercise on cardiometabolic health of adults with overweight or obesity: Focus on blood pressure, insulin resistance, and intrahepatic fat-A systematic review and meta-analysis. Obes. Rev. 2021, 22 (Suppl. S4), e13269. [Google Scholar] [CrossRef] [PubMed]
- Francesconi, C.; Niebauer, J.; Haber, P.; Weitgasser, R.; Lackinger, C. Lebensstil: Körperliche Aktivität und Training in der Prävention und Therapie des Typ 2 Diabetes mellitus (Update 2019) [Lifestyle: Physical activity and training as prevetion and therapy of type 2 diabetes mellitus (Update 2019)]. Wien. Klin. Wochenschr. 2019, 131 (Suppl. S1), 61–66. (In German) [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, E.; Oikonomou, C.; Nychas, G.; Dimitriadis, G.D. Effects of Diet, Lifestyle, Chrononutrition and Alternative Dietary Interventions on Postprandial Glycemia and Insulin Resistance. Nutrients 2022, 14, 823. [Google Scholar] [CrossRef] [PubMed]
- Celik, O.; Yildiz, B.O. Obesity and physical exercise. Minerva Endocrinol. 2021, 46, 131–144. [Google Scholar] [CrossRef]
- Mastrototaro, L.; Roden, M. Insulin resistance and insulin sensitizing agents. Metabolism 2021, 125, 154892. [Google Scholar] [CrossRef]
- Aaseth, J.; Ellefsen, S.; Alehagen, U.; Sundfør, T.M.; Alexander, J. Diets and drugs for weight loss and health in obesity—An update. Biomed. Pharmacother. 2021, 140, 111789. [Google Scholar] [CrossRef]
- Mirabelli, M.; Chiefari, E.; Arcidiacono, B.; Corigliano, D.M.; Brunetti, F.S.; Maggisano, V.; Russo, D.; Foti, D.P.; Brunetti, A. Mediterranean Diet Nutrients to Turn the Tide against Insulin Resistance and Related Diseases. Nutrients 2020, 12, 1066. [Google Scholar] [CrossRef]
- Podlipskyte, A.; Kazukauskiene, N.; Varoneckas, G.; Mickuviene, N. Association of Insulin Resistance with Cardiovascular Risk Factors and Sleep Complaints: A 10-Year Follow-Up. Front. Public Health 2022, 10, 848284. [Google Scholar] [CrossRef] [PubMed]
- Adeva-Andany, M.M.; Martínez-Rodríguez, J.; González-Lucán, M.; Fernández-Fernández, C.; Castro-Quintela, E. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab. Syndr. 2019, 13, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Saotome, M.; Ikoma, T.; Hasan, P.; Maekawa, Y. Cardiac Insulin Resistance in Heart Failure: The Role of Mitochondrial Dynamics. Int. J. Mol. Sci. 2019, 20, 3552. [Google Scholar] [CrossRef] [PubMed]
- Ding, P.F.; Zhang, H.S.; Wang, J.; Gao, Y.Y.; Mao, J.N.; Hang, C.H.; Li, W. Insulin resistance in ischemic stroke: Mechanisms and therapeutic approaches. Front. Endocrinol. 2022, 13, 1092431. [Google Scholar] [CrossRef] [PubMed]
- McCracken, E.; Monaghan, M.; Sreenivasan, S. Pathophysiology of the metabolic syndrome. Clin. Dermatol. 2018, 36, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Papachristoforou, E.; Lambadiari, V.; Maratou, E.; Makrilakis, K. Association of Glycemic Indices (Hyperglycemia, Glucose Variability, and Hypoglycemia) with Oxidative Stress and Diabetic Complications. J. Diabetes Res. 2020, 2020, 7489795. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Manent, J.I.; Jover, A.M.; Martinez, C.S.; Tomás-Gil, P.; Martí-Lliteras, P.; López-González, Á.A. Waist Circumference Is an Essential Factor in Predicting Insulin Resistance and Early Detection of Metabolic Syndrome in Adults. Nutrients 2023, 15, 257. [Google Scholar] [CrossRef]
- Wang, J.; Yan, S.; Cui, Y.; Chen, F.; Piao, M.; Cui, W. The Diagnostic and Prognostic Value of the Triglyceride-Glucose Index in Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD): A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4969. [Google Scholar] [CrossRef]
- Kim, B.; Kim, G.; Lee, Y.; Taniguchi, K.; Isobe, T.; Oh, S. Triglyceride-Glucose Index as a Potential Indicator of Sarcopenic Obesity in Older People. Nutrients 2023, 15, 555. [Google Scholar] [CrossRef]
- Zheng, Y.; Yin, G.; Chen, F.; Lin, L.; Chen, Y. Evaluation of Triglyceride Glucose Index and Homeostasis Model of Insulin Resistance in Patients with Polycystic Ovary Syndrome. Int. J. Womens Health 2022, 14, 1821–1829. [Google Scholar] [CrossRef]
- Manzanero, R.B.; López-González, A.A.; Tomás-Gil, P.; Paublini, H.; Martínez-Jover, A. Ramírez-Manent JIEstimation of cardiometabolic risk in 25.030 Spanish kitchen workers. Acad. J. Health Sci. 2023, 38, 101–110. [Google Scholar] [CrossRef]
- Paublini, H.; López González, A.A.; Busquets-Cortés, C.; Tomas-Gil, P.; Riutord-Sbert, P.; Ramírez-Manent, J.I. Relationship between Atherogenic Dyslipidaemia and Lipid Triad and Scales That Assess Insulin Resistance. Nutrients 2023, 15, 2105. [Google Scholar] [CrossRef] [PubMed]
- Aguiló, M.C.; Ramírez-Manent, J.I.; tomás-Gil, P.; Paublini, H.; Tárraga-López, P.J.; López-González, A.A. Influence of tobacco consumption on the values of different overweight and obesity scales in 418,343 spanish people. Acad. J. Health Sci. 2023, 38, 111–117. [Google Scholar] [CrossRef]
- Riutord-Sbert, P.; Riutord-Fe, B.; Riutord-Fe, N.; Arroyo-Bote, S.; López González, A.A.; Ramírez-Manent, J.I. Influence of physical activity and mediterranean diet on the values of different scales of overweight and obesity. Acad. J. Health Sci. 2022, 37, 21–28. [Google Scholar] [CrossRef]
- Tessari, S.; Casazza, M.; De Boni, G.; Bertoncello, C.; Fonzo, M.; Di Pieri, M.; Russo, F. Promoting health and preventing non-communicable diseases: Evaluation of the adherence of the Italian population to the Mediterranean Diet by using the PREDIMED questionnaire. Ann. Ig. 2021, 33, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Trovato, B.; Godos, J.; Varrasi, S.; Roggio, F.; Castellano, S.; Musumeci, G. Physical Activity, Sun Exposure, Vitamin D Intake and Perceived Stress in Italian Adults. Nutrients 2023, 15, 2301. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Schunkert, H.; Moebus, S.; Hanisch, J.; Bramlage, P.; Steinhagen-Thiessen, E.; Hauner, H.; Weil, J.; Wasem, J.; Jöckel, K.H. The correlation between waist circumference and ESC cardiovascular risk score: Data from the German metabolic and cardiovascular risk project (GEMCAS). Clin. Res. Cardiol. 2008, 97, 827–835. [Google Scholar] [CrossRef]
- Mancia, G.; Bombelli, M.; Facchetti, R.; Casati, A.; Ronchi, I.; Quarti-Trevano, F.; Arenare, F.; Grassi, G.; Sega, R. Impact of different definitions of the metabolic syndrome on the prevalence of organ damage, cardiometabolic risk and cardiovascular events. J. Hypertens. 2010, 28, 999–1006. [Google Scholar] [CrossRef]
- Gallois, Y.; Vol, S.; Cacès, E.; Balkau, B. Distribution of fasting serum insulin measured by enzyme immunoassay in an unselected population of 4,032 individuals. Reference values according to age and sex. D.E.S.I.R. Study Group. Données Epidémiologiques sur le Syndrome d’Insulino-Résistance. Diabetes Metab. 1996, 22, 427–431. [Google Scholar]
- Geer, E.B.; Shen, W. Gender differences in insulin resistance, body composition, and energy balance. Gend. Med. 2009, 6 (Suppl. S1), 60–75. [Google Scholar] [CrossRef] [PubMed]
- Vigna, L.; Tirelli, A.S.; Gaggini, M.; Di Piazza, S.; Tomaino, L.; Turolo, S.; Moroncini, G.; Chatzianagnostou, K.; Bamonti, F.; Vassalle, C. Insulin resistance and cardiometabolic indexes: Comparison of concordance in working-age subjects with overweight and obesity. Endocrine 2022, 77, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Determinantes de Salud (Consumo de Tabaco, Exposición Pasiva al Humo de Tabaco, Alcohol, Problemas Medioambientales en la Vivienda). Available online: https://www.ine.es/ss/Satellite?L=es_ES&c=INESeccion_C&cid=1259926698156&p=1254735110672&pagename=ProductosYServicios/PYSLayout (accessed on 27 September 2023).
- Encuesta 2019/2020 Sobre Consumo de Sustancias Psicoactivas en el Ámbito Laboral en España. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/pdf/2021_OEDA_InformeLaboral_2019_2020.pdf (accessed on 10 October 2023).
- Cambron, C.; Lam, C.Y.; Cinciripini, P.; Li, L.; Wetter, D.W. Socioeconomic Status, Social Context, and Smoking Lapse during a Quit Attempt: An Ecological Momentary Assessment Study. Ann. Behav. Med. 2020, 54, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Martín Álvarez, J.M.; Barrientos Marín, J.; Millán, J.M. The relationship between the socio-economic gradient and cigarette consumption in Spain. Adicciones 2022, 34, 94–109, (In Spanish with English Abstract). [Google Scholar] [CrossRef] [PubMed]
- Ruokolainen, O.; Härkänen, T.; Lahti, J.; Haukkala, A.; Heliövaara, M.; Rahkonen, O. Association between educational level and smoking cessation in an 11-year follow-up study of a national health survey. Scand. J. Public Health 2021, 49, 951–960. [Google Scholar] [CrossRef]
- Sandoval, J.L.; Leão, T.; Cullati, S.; Theler, J.M.; Joost, S.; Humair, J.P.; Gaspoz, J.M.; Guessous, I. Public smoking ban and socioeconomic inequalities in smoking prevalence and cessation: A cross-sectional population-based study in Geneva, Switzerland (1995-2014). Tob. Control. 2018, 27, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Rehman, K.; Haider, K.; Akash, M.S.H. Cigarette smoking and nicotine exposure contributes for aberrant insulin signaling and cardiometabolic disorders. Eur. J. Pharmacol. 2021, 909, 174410. [Google Scholar] [CrossRef] [PubMed]
- Ejercicio Físico Regular y Sedentarismo en el Tiempo Libre. Available online: https://www.ine.es/ss/Satellite?param1=PYSDetalleFichaIndicador&c=INESeccion_C¶m3=1259947308577&p=1254735110672&pagename=ProductosYServicios%2FPYSLayout&rendermode=pr+eviewnoinsite&cid=1259944495973&L=0#:~:text=En%20relaci%C3%B3n%20a%20la%20variable,%2C9%25%20para%20las%20mujeres (accessed on 27 September 2023).
- Salas-Salvadó, J.; Díaz-López, A.; Ruiz-Canela, M.; Basora, J.; Fitó, M.; Corella, D.; Serra-Majem, L.; Wärnberg, J.; Romaguera, D.; PREDIMED-Plus Investigators; et al. Effect of a Lifestyle Intervention Program with Energy-Restricted Mediterranean Diet and Exercise on Weight Loss and Cardiovascular Risk Factors: One-Year Results of the PREDIMED-Plus Trial. Diabetes Care. 2019, 42, 777–788. [Google Scholar] [CrossRef]
- Gołąbek, K.D.; Regulska-Ilow, B. Dietary support in insulin resistance: An overview of current scientific reports. Adv Clin Exp Med. 2019, 28, 1577–1585. [Google Scholar] [CrossRef]
- Cena, H.; Calder, P.C. Defining a Healthy Diet: Evidence for The Role of Contemporary Dietary Patterns in Health and Disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef]
- Hsiao, F.Y.; Chen, L.K. What constitutes healthy diet in healthy longevity. Arch. Gerontol. Geriatr. 2022, 102, 104761. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lin, X.; Bloomgarden, Z.T.; Ning, G. The Jiangnan diet, a healthy diet pattern for Chinese. J. Diabetes. 2020, 12, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Ramírez Manent, J.I.; Altisench Jané, B.; Sanchís Cortés, P.; Busquets-Cortés, C.; Arroyo Bote, S.; Masmiquel Comas, L.; López González, Á.A. Impact of COVID-19 Lockdown on Anthropometric Variables, Blood Pressure, and Glucose and Lipid Profile in Healthy Adults: A before and after Pandemic Lockdown Longitudinal Study. Nutrients 2022, 14, 1237. [Google Scholar] [CrossRef] [PubMed]
- Beslay, M.; Srour, B.; Méjean, C.; Allès, B.; Fiolet, T.; Debras, C.; Chazelas, E.; Deschasaux, M.; Wendeu-Foyet, M.G.; Hercberg, S.; et al. Ultra-processed food intake in association with BMI change and risk of overweight and obesity: A prospective analysis of the French NutriNet-Santé cohort. PLoS Med. 2020, 17, e1003256. [Google Scholar] [CrossRef] [PubMed]
- Gantenbein, K.V.; Kanaka-Gantenbein, C. Mediterranean Diet as an Antioxidant: The Impact on Metabolic Health and Overall Wellbeing. Nutrients 2021, 13, 1951. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Herrero, M.T.; Ramírez-Iñiguez de la Torre, M.V.; Capdevila García, L.; Partida-Hanon, A.; Reinoso-Barbero, L.; López González, A.A. Lifestyle, overweight and obesity in spanish workers: Related variables. Acad. J. Health Sci. 2022, 37, 135–143. [Google Scholar] [CrossRef]
- Mazza, E.; Ferro, Y.; Pujia, R.; Mare, R.; Maurotti, S.; Montalcini, T.; Pujia, A. Mediterranean Diet in Healthy Aging. J. Nutr. Health Aging 2021, 25, 1076–1083. [Google Scholar] [CrossRef]
- Dziegielewska-Gesiak, S. Metabolic Syndrome in an Aging Society—Role of Oxidant-Antioxidant Imbalance and Inflammation Markers in Disentangling Atherosclerosis. Clin. Interv. Aging 2021, 16, 1057–1070. [Google Scholar] [CrossRef]
- Harman, D. Free radicals in aging. Mol. Cell Biochem. 1988, 84, 155–161. [Google Scholar] [CrossRef]
- Hernáez, Á.; Soria-Florido, M.T.; Schröder, H.; Ros, E.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Arós, F.; Serra-Majem, L.; et al. Role of HDL function and LDL atherogenicity on cardiovascular risk: A comprehensive examination. PLoS ONE 2019, 14, e0218533. [Google Scholar] [CrossRef]
- Sottero, B.; Gargiulo, S.; Russo, I.; Barale, C.; Poli, G.; Cavalot, F. Postprandial Dysmetabolism and Oxidative Stress in Type 2 Diabetes: Pathogenetic Mechanisms and Therapeutic Strategies. Med. Res. Rev. 2015, 35, 968–1031. [Google Scholar] [CrossRef] [PubMed]
- Malczyk, E.; Dzięgielewska-Gęsiak, S.; Fatyga, E.; Ziółko, E.; Kokot, T.; Muc-Wierzgon, M. Body composition in healthy older persons: Role of the ratio of extracellular/total body water. J. Biol. Regul. Homeost Agents 2016, 30, 767–772. [Google Scholar] [PubMed]
- Potes, Y.; de Luxán-Delgado, B.; Rodriguez-González, S.; Guimarães, M.R.M.; Solano, J.J.; Fernández-Fernández, M.; Bermúdez, M.; Boga, J.A.; Vega-Naredo, I.; Coto-Montes, A. Overweight in elderly people induces impaired autophagy in skeletal muscle. Free Radic. Biol. Med. 2017, 110, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Stephens, C.R.; Easton, J.F.; Robles-Cabrera, A.; Fossion, R.; de la Cruz, L.; Martínez-Tapia, R.; Barajas-Martínez, A.; Hernández-Chávez, A.; López-Rivera, J.A.; Rivera, A.L. The Impact of Education and Age on Metabolic Disorders. Front. Public Health 2020, 8, 180. [Google Scholar] [CrossRef] [PubMed]
- Jurkovičová, J.; Hirošová, K.; Vondrová, D.; Samohýl, M.; Štefániková, Z.; Filová, A.; Kachútová, I.; Babjaková, J.; Argalášová, Ľ. The Prevalence of Insulin Resistance and the Associated Risk Factors in a Sample of 14–18-Year-Old Slovak Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 909. [Google Scholar] [CrossRef] [PubMed]
- Lepe, A.; de Kroon, M.L.A.; Reijneveld, S.A.; de Winter, A.F. Socioeconomic inequalities in paediatric metabolic syndrome: Mediation by parental health literacy. Eur. J. Public Health 2023, 33, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, D.; Wu, J.; Zou, P.; Cui, N.; Li, D.; Shao, J.; Tang, L.; Xue, E.; Ye, Z.; et al. Heterogenous subtypes of health literacy among individuals with Metabolic syndrome: A latent class analysis. Ann. Med. 2023, 55, 2268109. [Google Scholar] [CrossRef]
- Stringhini, S.; Carmeli, C.; Jokela, M.; Avendaño, M.; Muennig, P.; Guida, F.; Ricceri, F.; d’Errico, A.; Barros, H.; LIFEPATH consortium; et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: A multicohort study and meta-analysis of 1·7 million men and women. Lancet 2017, 389, 1229–1237. [Google Scholar] [CrossRef]
- Blanquet, M.; Legrand, A.; Pélissier, A.; Mourgues, C. Socio-economics status and metabolic syndrome: A meta-analysis. Diabetes Metab. Syndr. 2019, 13, 1805–1812. [Google Scholar] [CrossRef]
- Escribano, H.E.; Pérez-Lema, M.; Recatalá Gimeno, M.J.; Tosoratto, J.L.; Carriedo, B.; López González, A.A. Classification of blood pressure with JNC-7 criteria in spanish working population: Influence of age, sex, social class and tobacco consumption. Acad. J. Health Sci. 2022, 37, 28–32. [Google Scholar] [CrossRef]
- Cardel, M.I.; Guo, Y.; Sims, M.; Dulin, A.; Miller, D.; Chi, X.; Pavela, G.; DeBoer, M.D.; Gurka, M.J. Objective and subjective socioeconomic status associated with metabolic syndrome severity among African American adults in Jackson Heart Study. Psychoneuroendocrinology 2020, 117, 104686. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jaramillo, P.; Gomez-Arbelaez, D.; Martinez-Bello, D.; Abat, M.E.M.; Alhabib, K.F.; Avezum, Á.; Barbarash, O.; Chifamba, J.; Diaz, M.L.; Gulec, S.; et al. Association of the triglyceride glucose index as a measure of insulin resistance with mortality and cardiovascular disease in populations from five continents (PURE study): A prospective cohort study. Lancet Healthy Longev. 2023, 4, e23–e33. [Google Scholar] [CrossRef] [PubMed]
- Letellier, N.; Yang, J.A.; Cavaillès, C.; Casey, J.A.; Carrasco-Escobar, G.; Zamora, S.; Jankowska, M.M.; Benmarhnia, T. Aircraft and road traffic noise, insulin resistance, and diabetes: The role of neighborhood socioeconomic status in San Diego County. Environ. Pollut. 2023, 335, 122277. [Google Scholar] [CrossRef] [PubMed]
- Poverty and Social Exclusion in Britain. Available online: https://www.bristol.ac.uk/poverty/pse/Poverty%20and%20Social%20Exclusion%20in%20Britain%20JRF%20Report.pdf (accessed on 8 December 2023).
- Gordon, D.; Lloyd, L.; Heslop, P. Jersey Health Survey. Available online: https://www.bristol.ac.uk/poverty/downloads/healthinequalities/JHS01_v3.pdf (accessed on 8 December 2023).
- Gordon, D.; Irving, M.; Nandy, S. Multidimensional Measures of Child Poverty. Available online: https://ipcig.org/conference/md-poverty/papers/Dave%20Gordon.pdf (accessed on 8 December 2023).

{kind=link}
| Men n = 232,814 | Women n = 154,110 | ||
|---|---|---|---|
| Mean (SD) | Mean (SD) | p-Value | |
| Age (years) | 39.8 (10.3) | 39.2 (10.2) | <0.001 |
| Height (cm) | 173.9 (7.0) | 161.2 (6.6) | <0.001 |
| Weight (kg) | 81.1 (13.9) | 65.3 (13.2) | <0.001 |
| Waist circumference (cm) | 87.7 (9.1) | 73.9 (7.9) | <0.001 |
| Hip circumference (cm) | 100.0 (8.4) | 97.2 (8.9) | <0.001 |
| Systolic blood pressure (mmHg) | 124.4 (15.1) | 114.4 (14.8) | <0.001 |
| Diastolic blood pressure (mmHg) | 75.4 (10.6) | 69.7 (10.3) | <0.001 |
| Total cholesterol (mg/dL) | 195.9 (38.9) | 193.6 (36.4) | <0.001 |
| HDL-c (mg/dL) | 51.0 (7.0) | 53.7 (7.6) | <0.001 |
| LDL-c (mg/dL) | 120.5 (37.6) | 122.3 (37.0) | <0.001 |
| Triglycerides (mg/dL) | 123.8 (88.0) | 88.1 (46.2) | <0.001 |
| Glycaemia (mg/dL) | 88.1 (12.9) | 84.1 (11.5) | <0.001 |
| % | % | p-value | |
| 20–29 years | 17.9 | 19.5 | <0.001 |
| 30–39 years | 33.1 | 33.3 | |
| 40–49 years | 29.7 | 29.4 | |
| 50–59 years | 16.3 | 15.3 | |
| 60–69 years | 3.0 | 2.5 | |
| Primary school | 61.2 | 51.8 | <0.001 |
| Secondary school | 34.0 | 40.7 | |
| University | 4.8 | 7.5 | |
| Social class I | 5.3 | 7.2 | <0.001 |
| Social class II | 17.4 | 33.2 | |
| Social class III | 77.3 | 59.8 | |
| Non-physical activity | 54.5 | 47.8 | <0.001 |
| Yes, physical activity | 45.5 | 52.2 | |
| Non-healthy food | 59.0 | 48.6 | <0.001 |
| Healthy food | 41.0 | 51.4 | |
| Non-smokers | 62.9 | 67.0 | <0.001 |
| Smokers | 37.1 | 33.0 |
| Men | Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| TyG Index | TyG-BMI | METS-IR | TG/HDL-c | TyG Index | TyG-BMI | METS-IR | TG/HDL-c | |||
| n | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | n | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| 20–29 years | 41,742 | 8.1 (0.5) | 204.3 (40.3) | 34.9 (6.8) | 1.8 (1.4) | 29,978 | 8.0 (0.5) | 190.5 (42.3) | 32.5 (7.2) | 1.4 (0.8) |
| 30–39 years | 76,960 | 8.4 (0.6) | 222.2 (42.0) | 38.0 (7.1) | 2.4 (2.1) | 51,392 | 8.0 (0.5) | 197.9 (45.1) | 34.0 (7.7) | 1.5 (0.9) |
| 40–49 years | 69,068 | 8.5 (0.6) | 235.0 (43.1) | 40.3 (7.4) | 2.9 (2.5) | 45,296 | 8.1 (0.5) | 209.9 (45.6) | 36.2 (7.7) | 1.8 (1.0) |
| 50–59 years | 38,028 | 8.6 (0.6) | 241.3 (41.8) | 42.0 (7.3) | 3.1 (2.4) | 23,516 | 8.3 (0.5) | 222.9 (46.0) | 38.5 (7.7) | 2.1 (1.3) |
| 60–69 years | 7016 | 8.6 (0.5) | 245.0 (39.4) | 42.9 (7.0) | 3.1 (2.0) | 3928 | 8.4 (0.5) | 231.2 (43.7) | 39.9 (7.3) | 2.2 (1.1) |
| Primary school | 142,494 | 8.4 (0.6) | 226.8 (44.7) | 39.0 (7.7) | 2.6 (2.9) | 79,810 | 8.1 (0.5) | 211.3 (48.2) | 36.4 (8.2) | 1.7 (1.0) |
| Secondary school | 79,226 | 8.4 (0.6) | 226.4 (42.8) | 38.8 (7.4) | 2.5 (2.1) | 62,690 | 8.1 (0.5) | 198.4 (43.2) | 34.0 (7.3) | 1.6 (1.0) |
| University | 11,094 | 8.3 (0.5) | 224.0 (39.4) | 38.5 (6.9) | 2.5 (2.3) | 11,610 | 8.0 (0.5) | 193.0 (41.1) | 33.1 (7.0) | 1.6 (0.8) |
| Social class I | 12,262 | 8.3 (0.5) | 224.6 (40.2) | 38.6 (7.0) | 2.5 (2.2) | 10,744 | 8.0 (0.5) | 192.6 (40.5) | 33.0 (6.9) | 1.6 (0.8) |
| Social class II | 40,650 | 8.4 (0.6) | 225.5 (42.0) | 38.6 (7.3) | 2.5 (2.1) | 51,230 | 8.1 (0.5) | 195.5 (41.8) | 33.6 (7.1) | 1.6 (1.0) |
| Social class III | 179,902 | 8.4 (0.6) | 226.9 (44.4) | 39.0 (7.7) | 2.6 (2.2) | 92,136 | 8.1 (0.5) | 211.1 (48.1) | 36.3 (8.2) | 1.7 (1.0) |
| Non-physical activity | 126,808 | 8.7 (0.6) | 253.3 (39.5) | 43.5 (6.9) | 3.4 (2.7) | 73,684 | 8.3 (0.5) | 235.9 (46.3) | 40.6 (7.8) | 2.2 (1.2) |
| Yes, physical activity | 106,006 | 8.1 (0.4) | 194.5 (21.6) | 33.4 (3.6) | 1.6 (0.6) | 80,426 | 7.9 (0.4) | 176.0 (20.5) | 30.2 (3.5) | 1.3 (0.4) |
| Non-Mediterranean diet | 137,464 | 8.7 (0.6) | 249.0 (41.2) | 42.7 (7.3) | 3.3 (2.6) | 74,828 | 8.3 (0.5) | 233.2 (48.2) | 40.0 (8.2) | 2.1 (1.2) |
| Yes, Mediterranean diet | 95,350 | 8.1 (0.4) | 194.2 (21.7) | 33.4 (3.6) | 1.6 (0.6) | 79,282 | 7.9 (0.4) | 177.7 (21.7) | 30.6 (3.7) | 1.3 (0.5) |
| Non-smokers | 146,480 | 8.4 (0.6) | 228.7 (43.0) | 39.2 (7.3) | 2.4 (1.8) | 103,300 | 8.1 (0.5) | 207.2 (46.9) | 35.6 (8.0) | 1.7 (1.0) |
| Smokers | 86,334 | 8.5 (0.6) | 223.0 (44.9) | 39.4 (8.0) | 2.9 (2.7) | 50,810 | 8.1 (0.5) | 209.5 (44.5) | 36.2 (7.5) | 1.8 (1.1) |
| Men | Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| TyG Index High | TyG-BMI High | METS-IR High | TG/HDL-c High | TyG Index High | TyG-BMI High | METS-IR High | TG/HDL-c High | |||
| n | % | % | % | % | n | % | % | % | % | |
| 20–29 years | 41,742 | 10.7 | 10.7 | 3.6 | 9.7 | 29,978 | 5.9 | 8.2 | 3.3 | 12.8 |
| 30–39 years | 76,960 | 20.3 | 18.6 | 6.6 | 18.7 | 51,392 | 7.4 | 11.0 | 4.5 | 15.4 |
| 40–49 years | 69,068 | 30.6 | 28.0 | 10.0 | 28.4 | 45,296 | 12.3 | 14.8 | 6.4 | 22.2 |
| 50–59 years | 38,028 | 35.0 | 33.3 | 13.3 | 34.1 | 23,516 | 20.3 | 20.5 | 8.2 | 32.3 |
| 60–69 years | 7016 | 36.6 | 36.7 | 14.5 | 34.1 | 3928 | 26.1 | 25.7 | 10.4 | 41.1 |
| Primary school | 142,494 | 25.2 | 23.5 | 8.9 | 23.5 | 79,810 | 12.7 | 16.7 | 6.9 | 22.2 |
| Secondary school | 79,226 | 23.8 | 22.2 | 7.8 | 22.2 | 62,690 | 9.5 | 10.2 | 4.2 | 18.2 |
| University | 11,094 | 20.9 | 19.9 | 6.6 | 20.6 | 11,610 | 7.8 | 7.7 | 3.2 | 16.4 |
| Social class I | 12,262 | 21.3 | 20.9 | 7.0 | 20.4 | 10,744 | 7.5 | 7.6 | 3.1 | 15.9 |
| Social class II | 40,650 | 23.7 | 21.4 | 7.3 | 22.4 | 51,230 | 9.3 | 9.0 | 3.7 | 18.3 |
| Social class III | 179,902 | 24.9 | 23.4 | 8.8 | 23.2 | 92,136 | 12.3 | 16.5 | 6.8 | 21.6 |
| Non-physical activity | 126,808 | 43.3 | 42.0 | 15.4 | 41.3 | 73,684 | 22.5 | 28.0 | 11.6 | 38.2 |
| Yes, physical activity | 106,006 | 2.0 | 0.3 | 2.4 | 0.9 | 80,426 | 0.4 | 0.3 | 0.2 | 3.5 |
| Non-Mediterranean diet | 137,464 | 39.8 | 38.8 | 14.2 | 37.8 | 74,828 | 21.2 | 27.6 | 11.4 | 34.5 |
| Yes, Mediterranean diet | 95,350 | 2.4 | 0.1 | 0.3 | 1.5 | 79,282 | 1.3 | 0.1 | 0.1 | 6.5 |
| Non-smokers | 146,480 | 22.6 | 23.8 | 8.2 | 20.9 | 103,300 | 10.6 | 14.6 | 6.1 | 19.4 |
| Smokers | 86,334 | 27.7 | 24.4 | 8.8 | 26.5 | 50,810 | 11.8 | 15.0 | 6.4 | 21.6 |
| METS-IR High | TG/HDL High | TyG Index High | TyG-BMI Index High | |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Female | 1 | 1 | 1 | 1 |
| Male | 1.25 (1.22–1.29) | 1.01 (1.00–1.03) | 2.57 (2.52–2.63) | 1.67 (1.63–1.70) |
| 20–29 years | 1 | 1 | 1 | 1 |
| 30–39 years | 1.11 (1.04–1.18) | 1.11 (1.06–1.16) | 1.14 (1.09–1.20) | 1.14 (1.08–1.19) |
| 40–49 years | 1.21 (1.13–1.28) | 1.30 (1.24–1.36) | 1.28 (1.22–1.34) | 1.17 (1.12–1.23) |
| 50–59 years | 1.33 (1.25–1.42) | 1.64 (1.57–1.72) | 1.66 (1.58–1.74) | 1.31 (1.25–1.38) |
| 60–69 years | 1.54 (1.44–1.66) | 2.08 (1.98–2.19) | 2.22 (2.11–2.34) | 1.48 (1.40–1.56) |
| Social class I | 1 | 1 | 1 | 1 |
| Social class II | 1.19 (1.13–1.24) | 1.04 (1.00–1.08) | 1.08 (1.04–1.14) | 1.20 (1.16–1.24) |
| Social class III | 1.25 (1.17–1.33) | 1.18 (1.16–1.20) | 1.09 (1.06–1.11) | 1.22 (1.16–1.27) |
| Yes, physical activity | 1 | 1 | 1 | 1 |
| Non-physical activity | 21.10 (12.91–34.42) | 31.32 (29.80–32.92) | 22.58 (21.31–23.91) | 78.77 (69.73–90.53) |
| Yes, Mediterranean diet | 1 | 1 | 1 | 1 |
| Non-Mediterranean diet | 16.61 (8.32–33.34) | 11.17 (10.80–13.58) | 1.86 (1.77–1.96) | 37.28 (22.55–54.88) |
| Non-smokers | 1 | 1 | 1 | 1 |
| Smokers | 1.06 (1.03–1.09) | 1.63 (1.60–1.66) | 1.56 (1.53–1.59) | 1.09 (1.07–1.11) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mestre Font, M.; Busquets-Cortés, C.; Ramírez-Manent, J.I.; Tomás-Gil, P.; Paublini, H.; López-González, Á.A. Influence of Sociodemographic Variables and Healthy Habits on the Values of Insulin Resistance Indicators in 386,924 Spanish Workers. Nutrients 2023, 15, 5122. https://doi.org/10.3390/nu15245122
Mestre Font M, Busquets-Cortés C, Ramírez-Manent JI, Tomás-Gil P, Paublini H, López-González ÁA. Influence of Sociodemographic Variables and Healthy Habits on the Values of Insulin Resistance Indicators in 386,924 Spanish Workers. Nutrients. 2023; 15(24):5122. https://doi.org/10.3390/nu15245122
Chicago/Turabian StyleMestre Font, Miguel, Carla Busquets-Cortés, José Ignacio Ramírez-Manent, Pilar Tomás-Gil, Hernán Paublini, and Ángel Arturo López-González. 2023. "Influence of Sociodemographic Variables and Healthy Habits on the Values of Insulin Resistance Indicators in 386,924 Spanish Workers" Nutrients 15, no. 24: 5122. https://doi.org/10.3390/nu15245122
APA StyleMestre Font, M., Busquets-Cortés, C., Ramírez-Manent, J. I., Tomás-Gil, P., Paublini, H., & López-González, Á. A. (2023). Influence of Sociodemographic Variables and Healthy Habits on the Values of Insulin Resistance Indicators in 386,924 Spanish Workers. Nutrients, 15(24), 5122. https://doi.org/10.3390/nu15245122