
UK Chickpea Consumption Doubled from 2008/09–2018/19

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Population
2.2. Dietary Assessment Methodology
2.3. Classification of Chickpea and Bean Consumers
2.4. Dietary Variables
2.5. Covariates
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- EatWell. 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/742750/Eatwell_Guide_booklet_2018v4.pdf (accessed on 31 May 2023).
- Mullins, A.P.; Arjmandi, B.H. Health benefits of plant-based nutrition: Focus on beans in cardiometabolic diseases. Nutrients 2021, 13, 519. [Google Scholar] [CrossRef] [PubMed]
- Singh, N. Pulses: An overview. J. Food Sci. Technol. 2017, 54, 853–857. [Google Scholar] [CrossRef] [PubMed]
- NHS. 5 A Day Portion Sizes. 2023. Available online: https://www.nhs.uk/live-well/eat-well/5-a-day/portion-sizes/#:~:text=Pulses%20and%20beans,of%20your%205%20A%20Day (accessed on 31 May 2023).
- McCance; Public Health England. McCance and Widdowson’s The Composition of Foods Integrated Dataset 2021. 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/971021/McCance_and_Widdowsons_Composition_of_Fo (accessed on 31 May 2023).
- UK National Health Service. 5 A Day: What Counts? Available online: https://www.nhs.uk/live-well/eat-well/5-a-day/5-a-day-what-counts/ (accessed on 28 June 2023).
- British Nutrition Foundation. The Science of Fibre. Available online: https://www.nutrition.org.uk/healthy-sustainable-diets/starchy-foods-sugar-and-fibre/fibre/?level=Health%20professional#:~:text=Adults%20in%20the%20UK%20are,eating%20less%20fibre%20than%20recommended (accessed on 30 May 2023).
- SACN. SACN (2015) Carbohydrates and Health; Public Health England: Wellington House, UK, 2015.
- PHE. Public Health England (2019) National Diet and Nutrition Survey. 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/943114/NDNS_UK_Y9-11_report.pdf (accessed on 31 May 2023).
- Rehm, C.D.; Goltz, S.R.; Katcher, J.A.; Guarneiri, L.L.; Dicklin, M.R.; Maki, K.C. Trends and Patterns of Chickpea Consumption among United States Adults: Analyses of National Health and Nutrition Examination Survey Data. J. Nutr. 2023, 153, 1567–1576. [Google Scholar] [CrossRef]
- Reister, E.J.; Belote, L.N.; Leidy, H.J. The Benefits of Including Hummus and Hummus Ingredients into the American Diet to Promote Diet Quality and Health: A Comprehensive Review. Nutrients 2020, 12, 3678. [Google Scholar] [CrossRef] [PubMed]
- Cakir, Ö.; Ucarli, C.; Tarhanm, Ç.; Pekmez, M.; Turgut-Kara, N. Nutritional and health benefits of legumes and their distinctive genomic properties. Food Sci. Technol. 2019, 39, 1–12. [Google Scholar] [CrossRef]
- Begum, N.; Khan, Q.U.; Liu, L.G.; Li, W.; Liu, D.; Haq, I.U. Nutritional composition, health benefits and bio-active compounds of chickpea (Cicer arietinum L.). Front Nutr. 2023, 7, 1218468. [Google Scholar] [CrossRef] [PubMed]
- Polak, R.; Phillips, E.M.; Campbell, A. Legumes: Health benefits and culinary approaches to increase intake. Clin. Diabetes 2015, 33, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C.; Murray, R.; Zelman, K.M. The Nutritional Value and Health Benefits of Chickpeas and Hummus. Nutrients 2016, 8, 766. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Agency. National Diet and Nutrition Survey Years 9–11 (2016/17–2018/19) User Guide. Available online: https://doc.ukdataservice.ac.uk/doc/6533/mrdoc/pdf/6533_ndns_rp_yr9-11_user_guide_final_v2.pdf (accessed on 2 June 2023).
- Dikariyanto, V.; Berry, S.E.; Francis, L.; Smith, L.; Hall, W.L. Whole almond consumption is associated with better diet quality and cardiovascular disease risk factors in the UK adult population: National Diet and Nutrition Survey (NDNS) 2008–2017. Eur. J. Nutr. 2021, 60, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Darmadi-Blackberry, I.; Wahlqvist, M.L.; Kouris-Blazos, A.; Steen, B.; Lukito, W.; Horie, Y.; Horie, K. Legumes: The most important dietary predictor of survival in older people of different ethnicities. Asia Pac. J. Clin. Nutr. 2004, 13, 217–220. [Google Scholar] [PubMed]
- Jukanti, A.K.; Gaur, P.M.; Gowda, C.L.; Chibbar, R.N. Nutritional quality and health benefits of chickpea (Cicer arietinum L.): A review. Br. J. Nutr. 2012, 108 (Suppl. S1), S11–S26. [Google Scholar] [CrossRef] [PubMed]
- Yau, A.; Adams, J.; Monsivais, P. Time trends in adherence to UK dietary recommendations and associated sociodemographic inequalities, 1986–2012: A repeated cross-sectional analysis. Eur. J. Clin. Nutr. 2019, 73, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.G.; Scheelbeek, P.; Balmford, A.; Garnett, E.E. Discrepancies between Two Long-Term Dietary Datasets in the United Kingdom (UK). Wellcome Open Res. 2023, 6, 350. [Google Scholar] [CrossRef]
- Merga, B.; Haji, J. Economic importance of chickpea: Production, value, and world trade. Cogent Food Agric. 2019, 5, 1615718. [Google Scholar] [CrossRef]
- Mintel. Global New Products Database. Available online: https://www.gnpd.com/sinatra/analysis/chart_results/search/bOHy8rqxiU/?analysis_id=67c569a1-b92d-4535-8e92-295fb4e36b34¤t_tab=67c569a1-b92d-4535-8e92-295fb4e36b34 (accessed on 15 May 2023).
- Institute for Health Metrics and Evaluation. GBD Compare. Available online: https://vizhub.healthdata.org/gbd-compare/. (accessed on 10 June 2023).
- Mendes, V.; Niforou, A.; Kasdagli, M.I.; Ververis, E.; Naska, A. Intake of legumes and cardiovascular disease: A systematic review and dose–response meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 22–37. [Google Scholar] [CrossRef] [PubMed]
- Becerra-Tomás, N.; Papandreou, C.; Salas-Salvadó, J. Legume Consumption and Cardiometabolic Health. Adv. Nutr. 2019, 10, S437–S450. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; He, J.; Ogden, L.G.; Loria, C.; Vupputuri, S.; Myers, L.; Whelton, P.K. Legume consumption and risk of coronary heart disease in US men and women: NHANES I Epidemiologic Follow-up Study. Arch. Intern. Med. 2001, 161, 2573–2578. [Google Scholar] [CrossRef] [PubMed]
- Health effects of dietary risks in 195 countries, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012; Volume 40. [Google Scholar]

{kind=link}
| Chickpea Consumers, % (95% Confidence Interval) | ||||||
|---|---|---|---|---|---|---|
| 2008–2012 (n = 6828) | 2012–2014 (n = 2546) | 2014–2016 (n = 2723) | 2016–2019 (n = 3558) | p-Trend | p-Interaction | |
| Total | 6.1 (5.2, 7.0) | 8.2 (6.7, 9.8) | 11.7 (9.9, 13.5) | 12.3 (10.8, 13.8) | <0.001 | - |
| Age group, year | ||||||
| 1.5–3 | 5.7 (3.7, 7.7) | 4.8 (1.6, 8.0) 1 | 12.5 (8.5, 16.4) | 13.4 (9.9, 16.8) | <0.001 | 0.50 |
| 4–10 | 7.1 (5.4, 8.9) | 7.2 (4.4, 9.9) | 9.9 (6.8, 13.1) | 8.8 (6.3, 11.3) | 0.06 | |
| 11–18 | 4.4 (3.0, 5.9) | 2.8 (1.0, 4.5) 1 | 5.5 (3.2, 7.7) | 10.3 (7.4, 13.2) | <0.001 | |
| 19–64 | 7.1 (5.8, 8.5) | 10.1 (7.8, 12.4) | 14.7 (12.0, 17.4) | 14.4 (12.1, 16.6) | <0.001 | |
| ≥65 | 3.0 (1.5, 4.6) | 5.8 (2.7, 8.9) | 5.6 (2.5, 8.7) | 8.1 (5.2, 10.9) | <0.001 | |
| Sex | ||||||
| Male | 5.0 (3.8, 6.2) | 6.6 (4.4, 8.9) | 9.4 (7.0, 11.8) | 10.9 (8.8, 12.9) | <0.001 | 0.60 |
| Female | 7.2 (5.9, 8.6) | 9.8 (7.6, 11.9) | 14.0 (11.2, 16.8) | 13.7 (11.6, 15.8) | <0.001 | |
| Race/ethnicity | ||||||
| White | 4.8 (4.0, 5.7) | 6.7 (5.1, 8.2) | 10.3 (8.4, 12.1) | 11.3 (9.8, 12.9) | <0.001 | 0.002 |
| Other * | 15.9 (11.7, 20.1) | 19.9 (13.9, 25.8) | 19.4 (13.3, 25.4) | 18.5 (13.6, 23.4) | 0.26 | |
| Income Tertile ** | ||||||
| Low | 3.8 (2.4, 5.2) | 7.7 (4.8, 10.6) | 7.8 (5.0, 10.6) | 9.9 (7.2, 12.5) | <0.001 | 0.04 |
| Medium | 5.5 (3.9, 7.0) | 5.9 (3.2, 8.6) | 10.0 (6.5, 13.6) | 10.8 (8.2, 13.5) | <0.001 | |
| High | 9.4 (7.6, 11.3) | 10.7 (7.9, 13.6) | 15.8 (12.4, 19.1) | 16.9 (13.8, 20.0) | <0.001 | |
| Education (adults) *** | ||||||
| Low (≥16 years) | 3.1 (2.0, 4.1) | 4.7 (2.5, 6.9) | 4.8 (3.0, 6.6) | 6.6 (4.5, 8.7) | <0.001 | 0.44 |
| Medium (17–18 years) | 6.0 (3.8, 8.2) | 11.3 (6.6, 16.0) | 11.2 (7.1, 15.2) | 10.3 (7.1, 13.6) | 0.02 | |
| High (≥19 years) | 11.5 (8.7, 14.3) | 14.8 (10.8, 18.9) | 23.1 (18.1, 28.1) | 21.6 (17.8, 25.3) | <0.001 | |
| n | Chickpea Consumers, % (95% CI) | |
|---|---|---|
| Adults | 1844 | 11.6 (10.1, 13.0) |
| Body mass index, kg/m2 | ||
| Healthy weight: 18.5–24.9 | 584 | 15.7 (12.2, 19.2) |
| Overweight: 25–29.9 | 639 | 13.0 (10.0, 16.0) |
| Obese: ≥30 | 439 | 11.1 (7.8, 14.5) |
| Vegetarian-type dietary pattern a | ||
| No | 1720 | 10.9 (9.1, 12.7) |
| Yes | 120 | 37.8 (30.4, 45.2) |
| Cigarette smoking status | ||
| Current | 312 | 6.5 (4.3, 8.8) |
| Former | 443 | 8.5 (6.0, 11.0) |
| Never | 1061 | 16.3 (13.7, 19.0) |
| Self-reported overall health status | ||
| Very good | 608 | 16.7 (13.4, 20.0) |
| Good | 801 | 12.7 (10.1, 15.4) |
| Fair | 340 | 7.0 (4.1, 10.0) |
| Bad/very bad | 92 | 8.4 (7.7, 9.1) |
| Mean (95% CI) | |||
|---|---|---|---|
| Chickpea Consumers (n = 363) | Bean Consumers (n = 1708) | Non-Bean Consumers (n = 1487) | |
| Kcal/d | 1795 (1745, 1846) a | 1757 (1716, 1798) a | 1656 (1620, 1691) b |
| Protein, g/d | 71.5 (68.6, 74.4) a | 72.4 (70.7, 74.2) a | 67.0 (65.3, 68.8) b |
| Carbohydrate, g/d | 215 (208, 221) a | 216 (210, 221) a | 201 (196, 206) b |
| Free sugar, g/d | 45.4 (42.3, 48.5) | 48.8 (46.6, 50.1) | 47.6 (45.1, 50.2) |
| Dietary fibre, g/d | 23.1 (22.1, 24.2) a | 19.4 (18.7, 20.0) b | 15.8 (15.4, 16.2) c |
| Total fat, g/d | 71.3 (68.7, 74.0) a | 66.5 (64.7, 68.3) b | 63.8 (62.1, 65.5) c |
| Saturated fat, g/d | 24.7 (23.6, 25.9) | 24.5 (23.8, 25.3) | 24.2 (23.4, 24.9) |
| MUFA, g/d | 26.6 (25.4, 27.8) a | 24.4 (23.7, 25.1) b | 23.4 (22.7, 24.1) c |
| PUFA, g/d | 11.5 (10.9, 12.1) a | 9.5 (9.2, 9.8) b | 8.7 (8.4, 8.9) c |
| Potassium, mg/d | 2878 (2783, 2973) a | 2742 (2679, 2805) b | 2507 (2451, 2564) c |
| Vitamin D, μg/d | 6.3 (4.7, 7.9) | 5.5 (4.4, 6.6) | 5.0 (4.0, 6.0) |
| Iron, mg/d | 13.3 (11.1, 15.5) a | 11.8 (11.1, 12.5) a | 10.3 (9.5, 11.0) b |
| Magnesium, mg/d | 305.5 (291.2, 319.8) a | 265.0 (257.2, 271.9) b | 235.4 (228.4, 242.4) c |
| Sodium, mg/d | 1943 (1869, 2018) a | 2005 (1952, 2058) a | 1796 (1746, 1846) b |
| Calcium, mg/d | 849 (813, 885) a | 831 (807, 855) a | 787 (764, 810) b |
| Food Groups | |||
| Fruits and Vegetables, g/d | 361.6 (339.0, 384.6) a | 271.9 (260.1, 283.6) b | 235.6 (224.2, 247.0) c |
| Pulses and nuts, g/d | 42.8 (37.3, 48.4) a | 28.7 (25.1, 32.3) b | 3.5 (2.9, 4.2) c |
| Red and processed meat, g/d | 24.4 (20.4, 28.3) a | 45.4 (42.5, 48.3) b | 43.1 (40.4, 45.9) b |
| Fish, g/d | 19.3 (15.8, 22.9) | 19.4 (17.4, 21.3) | 19.2 (17.3, 21.2) |
| Oily fish, g/d | 9.1 (6.5, 11.8) | 8.2 (6.9, 9.4) | 6.6 (5.5, 7.7) |
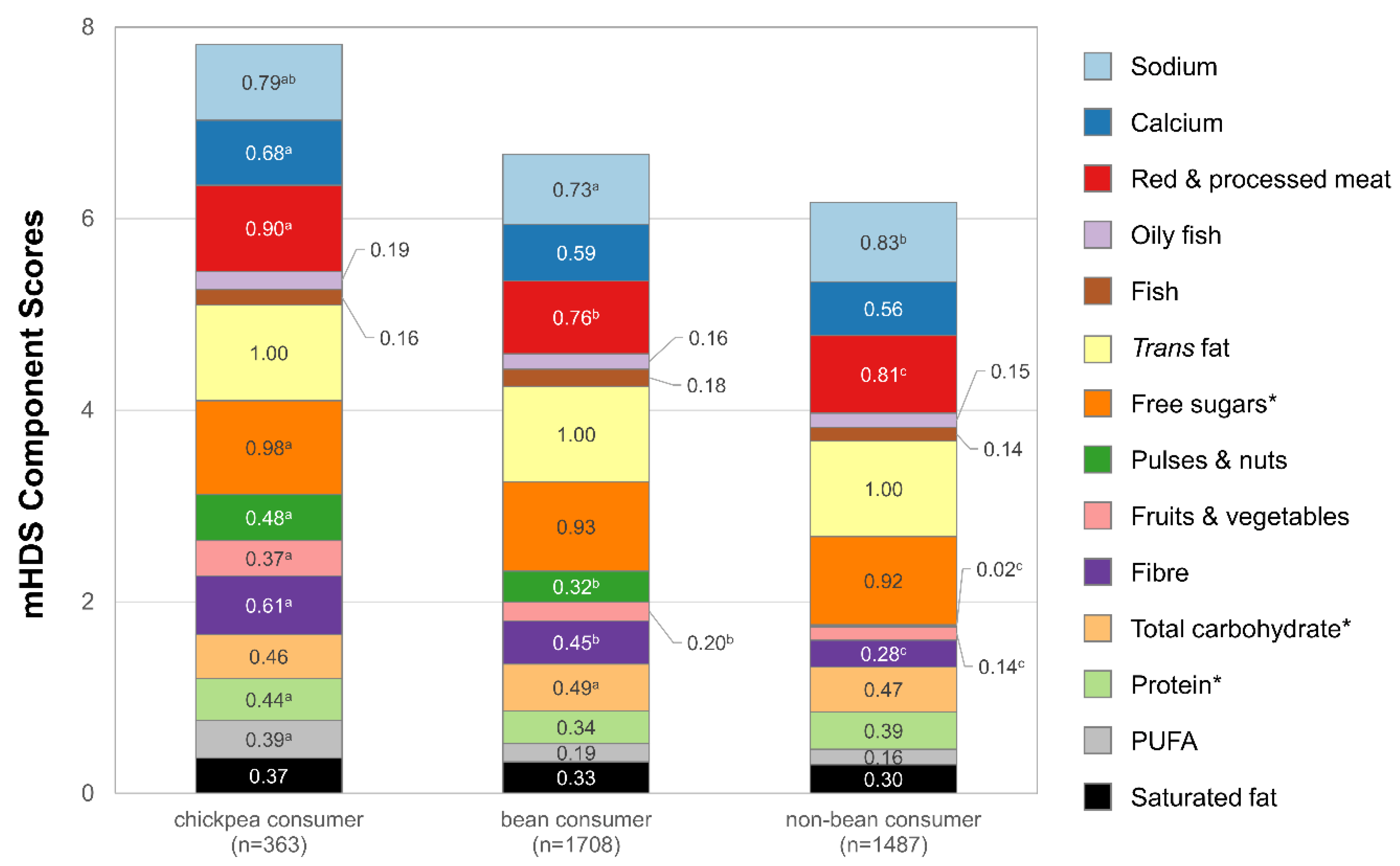
| Modified Healthy Dietary Score (range 0–14) | 7.8 (7.6, 8.0) a | 6.7 (6.6, 6.8) b | 6.2 (6.1, 6.3) c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutepova, I.; Rehm, C.D.; Friend, S.J. UK Chickpea Consumption Doubled from 2008/09–2018/19. Nutrients 2023, 15, 4784. https://doi.org/10.3390/nu15224784
Kutepova I, Rehm CD, Friend SJ. UK Chickpea Consumption Doubled from 2008/09–2018/19. Nutrients. 2023; 15(22):4784. https://doi.org/10.3390/nu15224784
Chicago/Turabian StyleKutepova, Inga, Colin D. Rehm, and Samara Joy Friend. 2023. "UK Chickpea Consumption Doubled from 2008/09–2018/19" Nutrients 15, no. 22: 4784. https://doi.org/10.3390/nu15224784
APA StyleKutepova, I., Rehm, C. D., & Friend, S. J. (2023). UK Chickpea Consumption Doubled from 2008/09–2018/19. Nutrients, 15(22), 4784. https://doi.org/10.3390/nu15224784