
Marine n−3 Fatty Acids and Prevention of Cardiovascular Disease: A Novel Analysis of the VITAL Trial Using Win Ratio and Hierarchical Composite Outcomes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Intervention and Its Control
2.3. Data Collection
2.4. Ethical Considerations
2.5. Outcome Assessments
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the VITAL Participants
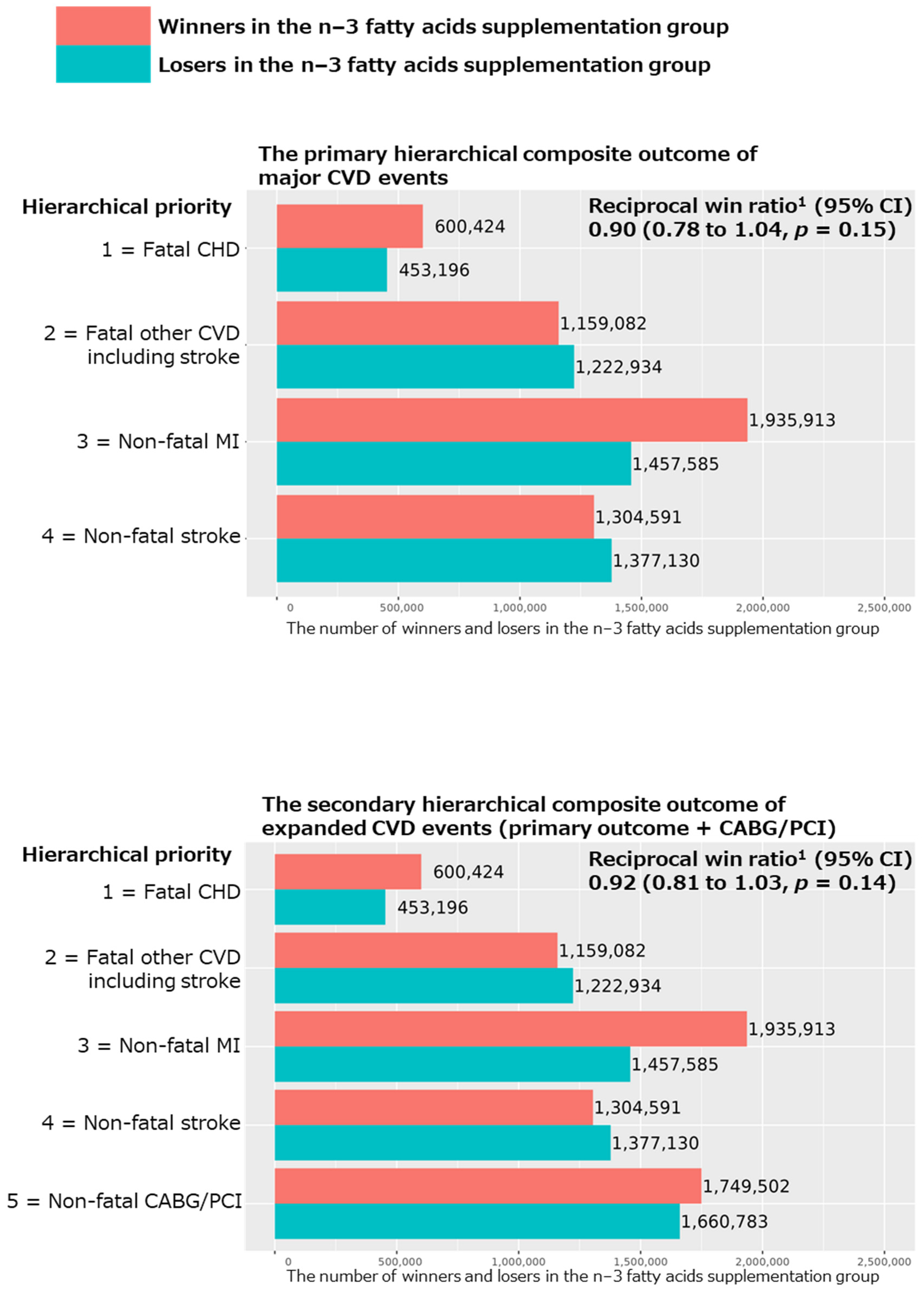
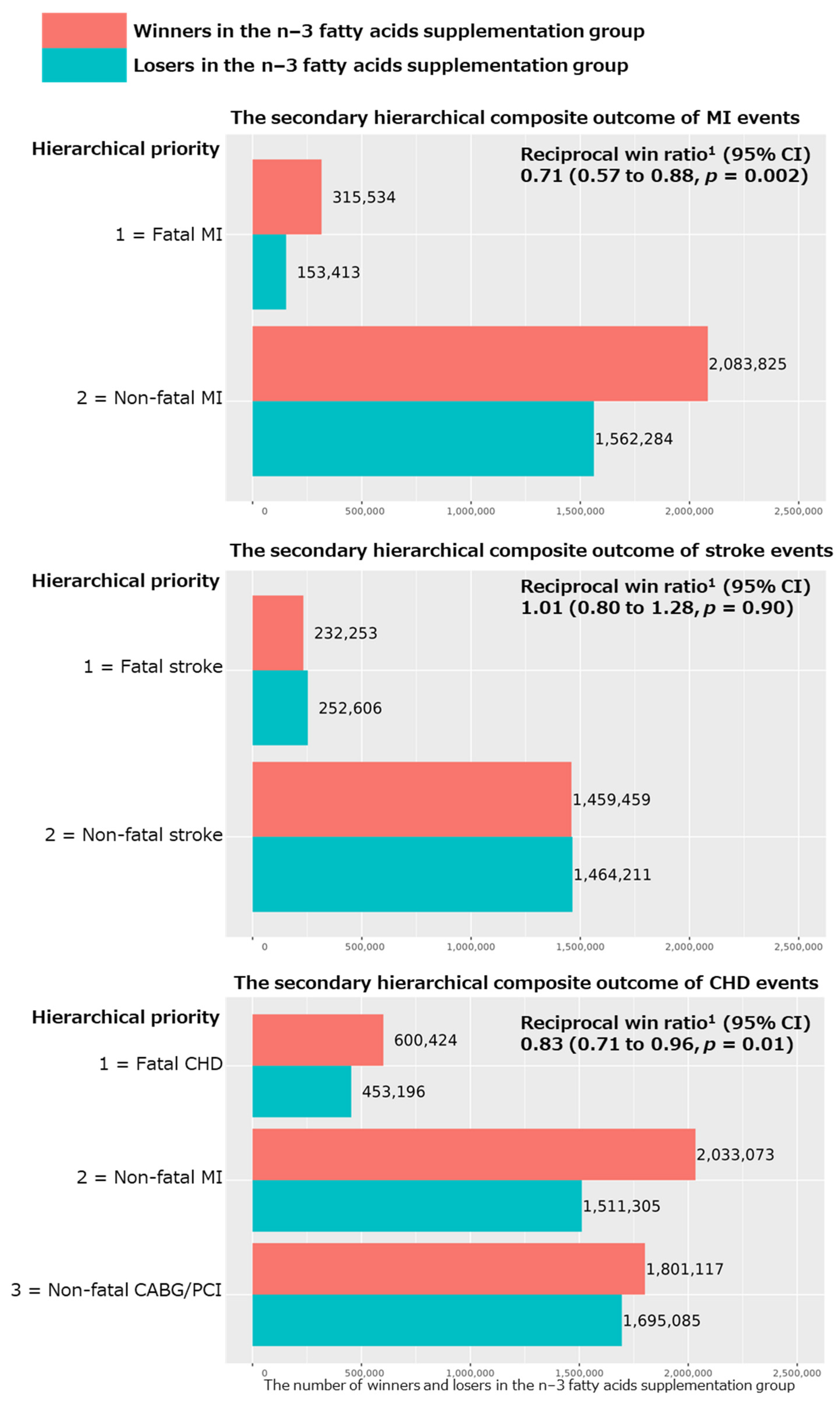
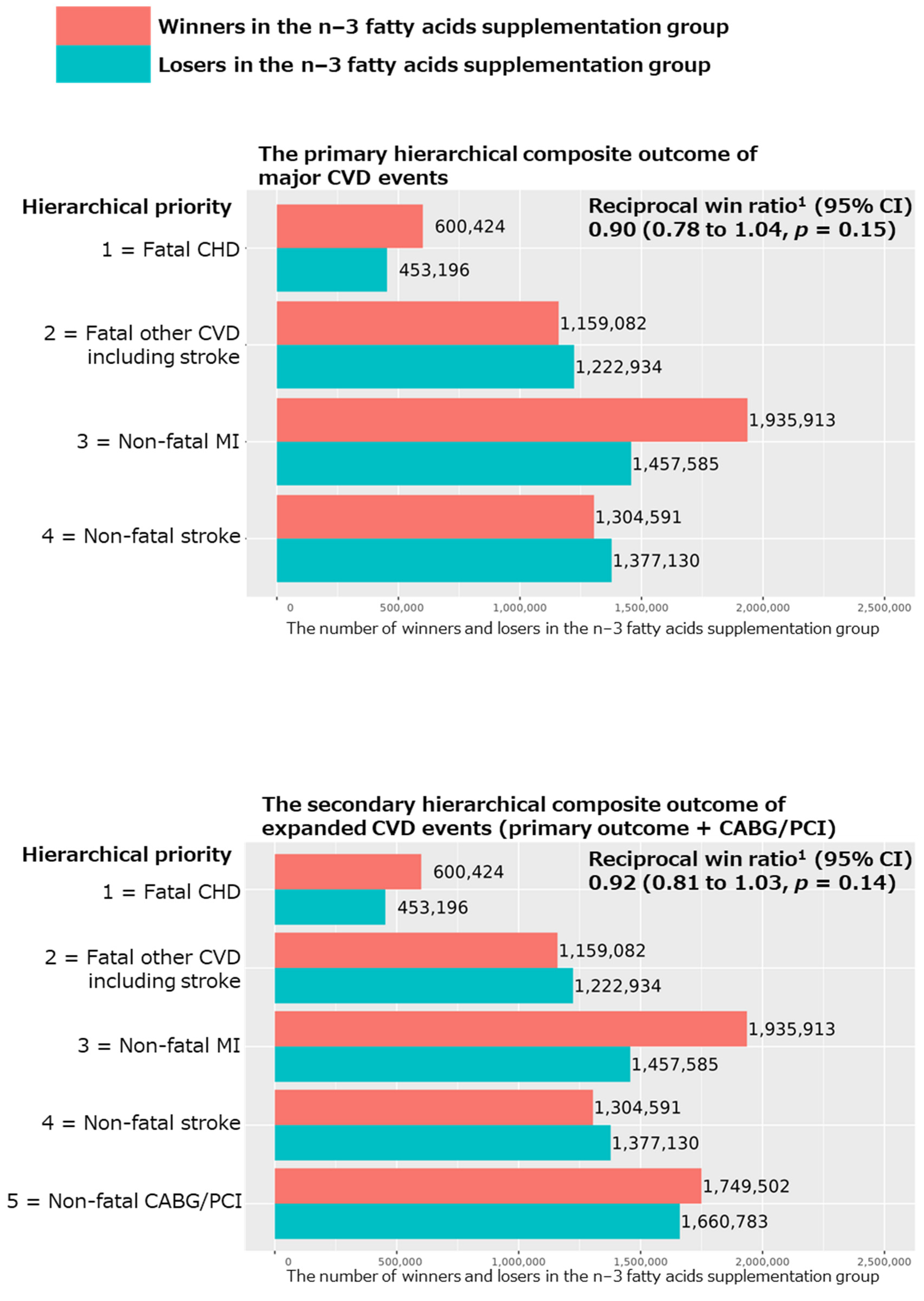
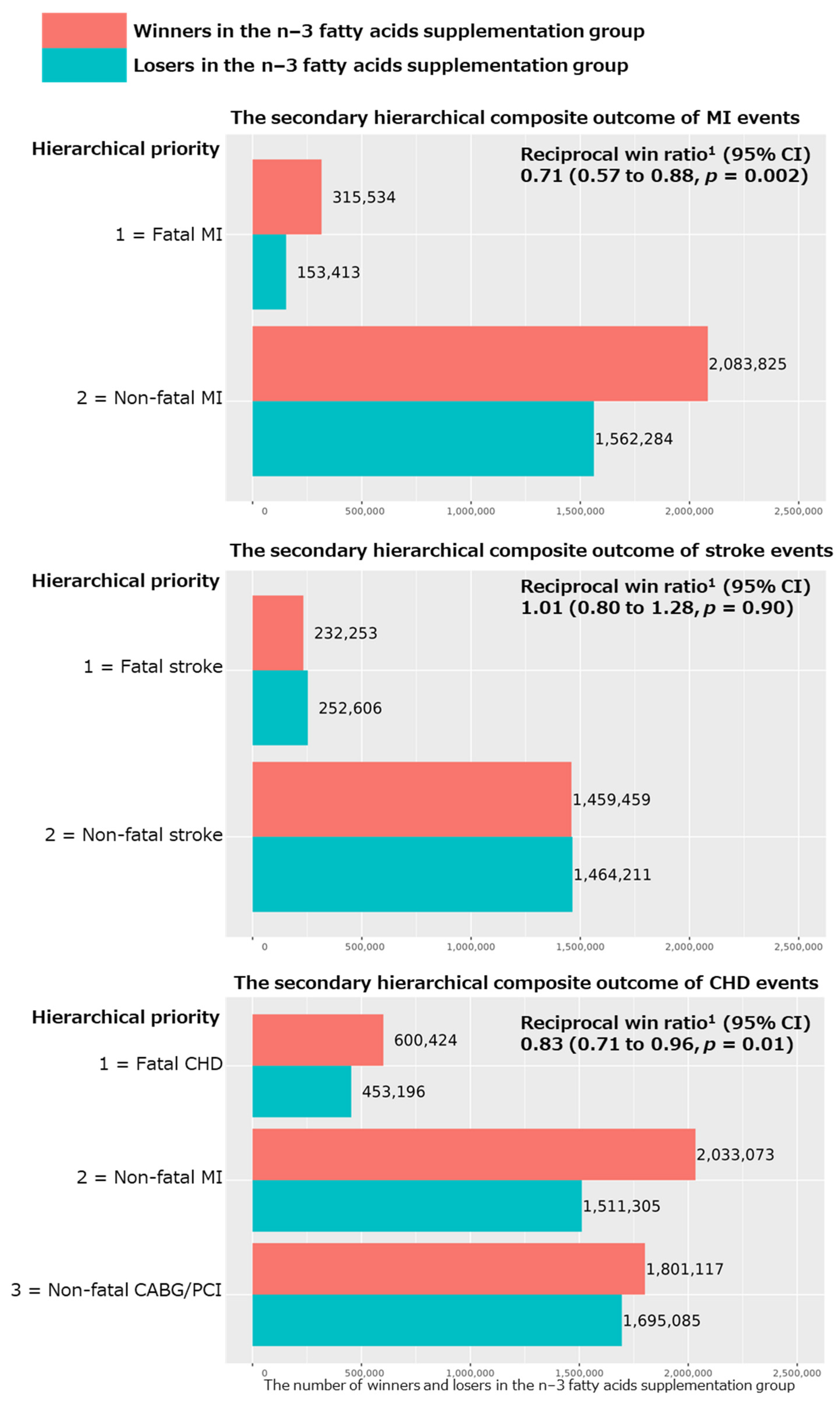
3.2. The Primary and Secondary Hierarchical Composite Outcomes in All Participants
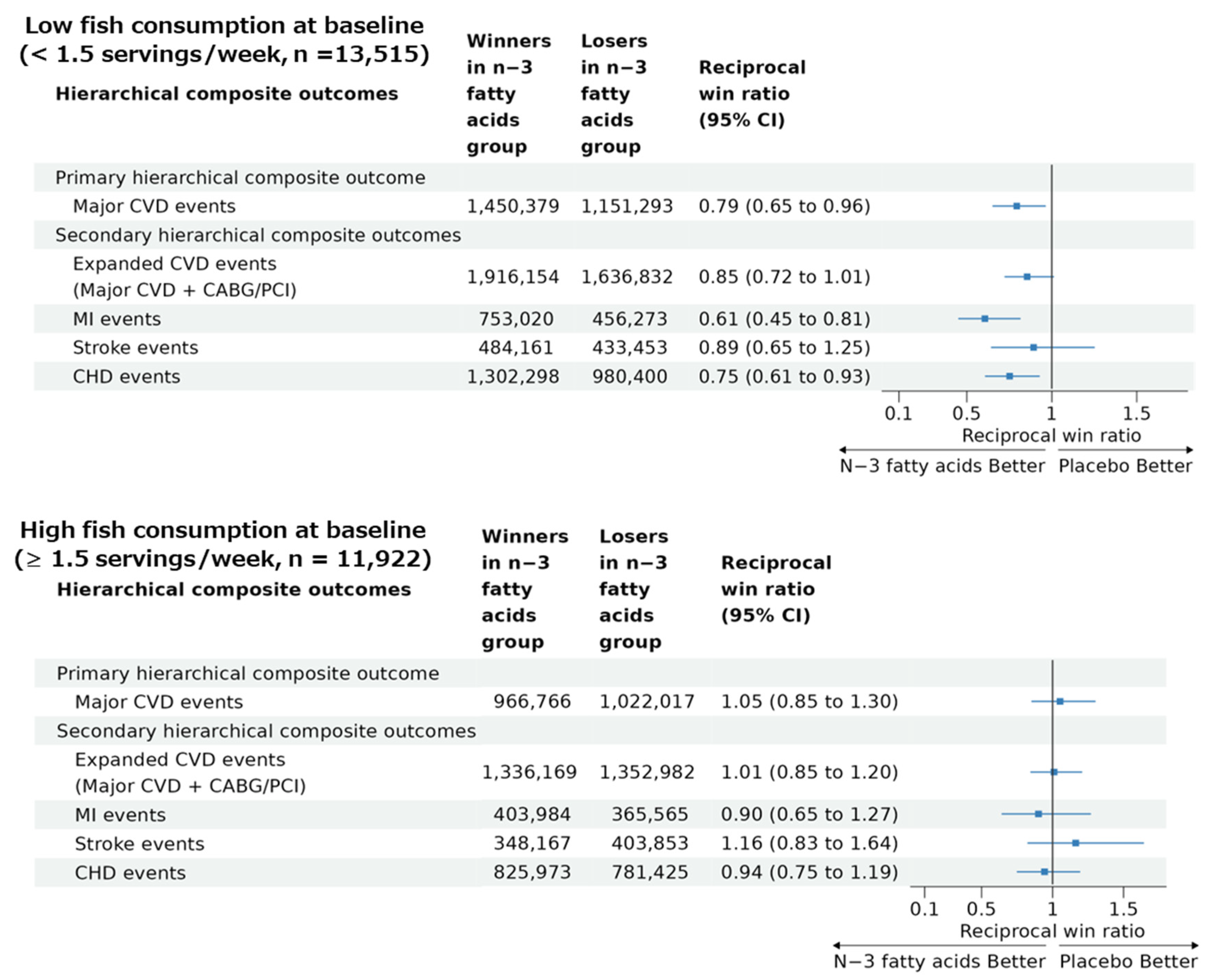
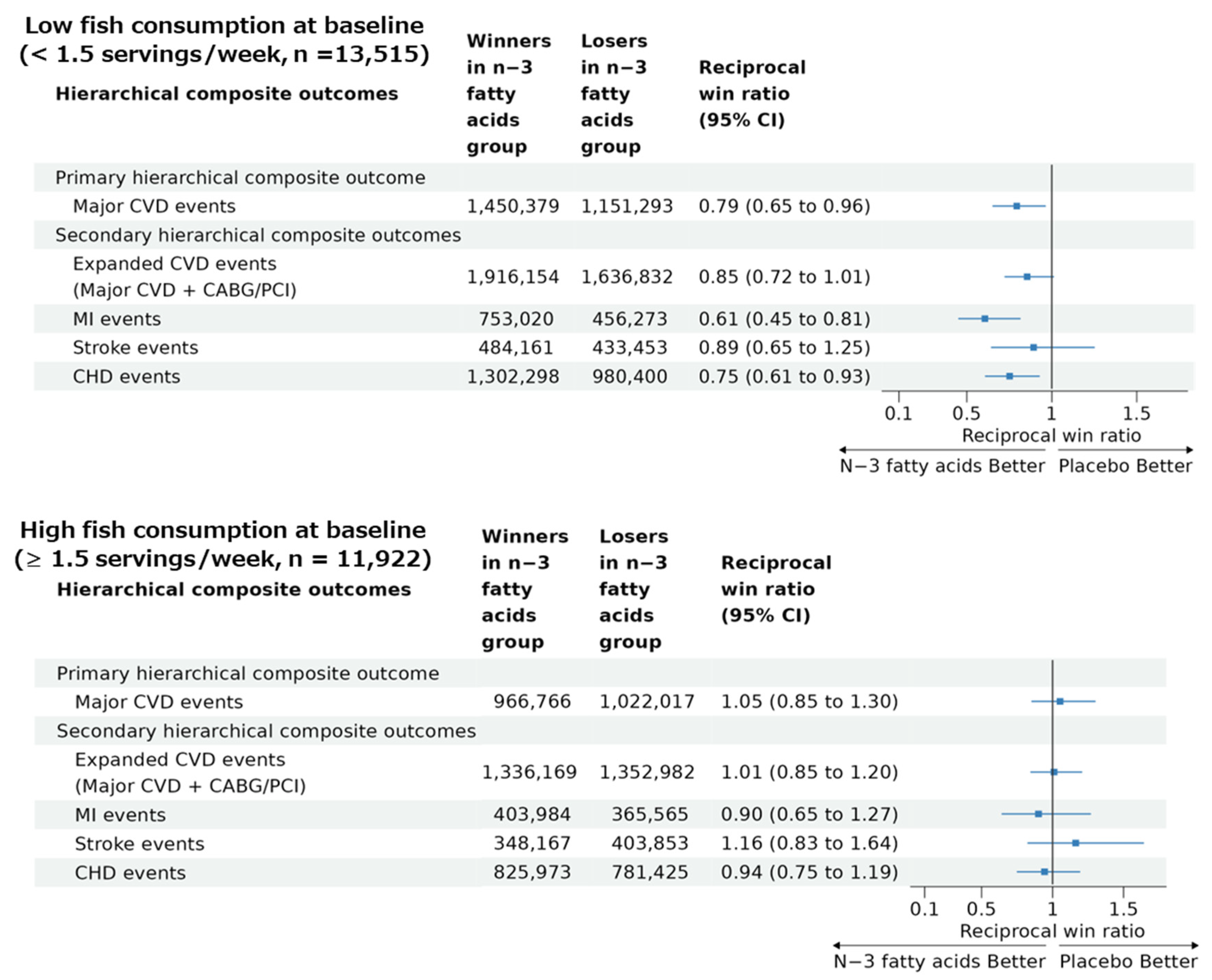
3.3. The Primary and Secondary Hierarchical Composite Outcomes in Subgroups with Low and High Fish Intake
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdelhamid, A.S.; Martin, N.; Bridges, C.; Brainard, J.S.; Wang, X.; Brown, T.J.; Hanson, S.; Jimoh, O.F.; Ajabnoor, S.M.; Deane, K.H.; et al. Polyunsaturated Fatty Acids for the Primary and Secondary Prevention of Cardiovascular Disease. Cochrane Database Syst. Rev. 2018, 11, CD012345. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.; Summerbell, C.D.; Worthington, H.V.; Song, F.; et al. Omega-3 Fatty Acids for the Primary and Secondary Prevention of Cardiovascular Disease. Cochrane Database Syst. Rev. 2020, 3, CD003177. [Google Scholar] [CrossRef]
- Lombardi, M.; Chiabrando, J.G.; Vescovo, G.M.; Bressi, E.; Del Buono, M.G.; Carbone, S.; Koenig, R.A.; Van Tassell, B.W.; Abbate, A.; Biondi-Zoccai, G.; et al. Impact of Different Doses of Omega-3 Fatty Acids on Cardiovascular Outcomes: A Pairwise and Network Meta-Analysis. Curr. Atheroscler. Rep. 2020, 22, 45. [Google Scholar] [CrossRef] [PubMed]
- Rizos, E.C.; Markozannes, G.; Tsapas, A.; Mantzoros, C.S.; Ntzani, E.E. Omega-3 Supplementation and Cardiovascular Disease: Formulation-Based Systematic Review and Meta-Analysis with Trial Sequential Analysis. Heart 2021, 107, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Markozannes, G.; Ntzani, E.E.; Tsapas, A.; Mantzoros, C.S.; Tsiara, S.; Xanthos, T.; Karpettas, N.; Patrikios, I.; Rizos, E.C. Dose-Related Meta-Analysis for Omega-3 Fatty Acids Supplementation on Major Adverse Cardiovascular Events. Clin. Nutr. 2022, 41, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.U.; Khan, M.U.; Riaz, H.; Valavoor, S.; Zhao, D.; Vaughan, L.; Okunrintemi, V.; Riaz, I.B.; Khan, M.S.; Kaluski, E.; et al. Effects of Nutritional Supplements and Dietary Interventions on Cardiovascular Outcomes: An Umbrella Review and Evidence Map. Ann. Intern. Med. 2019, 171, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Bernasconi, A.A.; Wiest, M.M.; Lavie, C.J.; Milani, R.V.; Laukkanen, J.A. Effect of Omega-3 Dosage on Cardiovascular Outcomes: An Updated Meta-Analysis and Meta-Regression of Interventional Trials. Mayo Clin. Proc. 2021, 96, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Cook, N.R.; Lee, I.-M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine N−3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Ariti, C.A.; Collier, T.J.; Wang, D. The Win Ratio: A New Approach to the Analysis of Composite Endpoints in Clinical Trials Based on Clinical Priorities. Eur. Heart J. 2012, 33, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Redfors, B.; Gregson, J.; Crowley, A.; Mcandrew, T.; Ben-Yehuda, O.; Stone, G.W.; Pocock, S.J. The Win Ratio Approach for Composite Endpoints: Practical Guidance Based on Previous Experience. Eur. Heart J. 2020, 41, 4391–4399. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Cook, N.R.; Lee, I.-M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico Dietary Supplementation with N-3 Polyunsaturated Fatty Acids and Vitamin E after Myocardial Infarction: Results of the GISSI-Prevenzione Trial. Gruppo Italiano per Lo Studio Della Sopravvivenza Nell’Infarto Miocardico. Lancet 1999, 354, 447–455. [Google Scholar]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J. Fish Consumption, Fish Oil, Omega-3 Fatty Acids, and Cardiovascular Disease. Circulation 2002, 106, 2747–2757. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Katus, H.A.; Lindahl, B.; Morrow, D.A.; Clemmensen, P.M.; et al. Third Universal Definition of Myocardial Infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P.J.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Duarte, K.; Ferreira, J.P. WinRatio: Win Ratio for Prioritized Outcomes and 95% Confidence Interval 2020. Available online: https://rdrr.io/cran/WinRatio/man/winratio.html(accessed on 12 September 2023).
- Jiang, L.; Wang, J.; Xiong, K.; Xu, L.; Zhang, B.; Ma, A. Intake of Fish and Marine N-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutrients 2021, 13, 2342. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Rimm, E.B. Fish Intake, Contaminants, and Human Health: Evaluating the Risks and the Benefits. JAMA 2006, 296, 1885–1899. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Song, Y.; Daviglus, M.L.; Liu, K.; Van Horn, L.; Dyer, A.R.; Greenland, P. Accumulated Evidence on Fish Consumption and Coronary Heart Disease Mortality: A Meta-Analysis of Cohort Studies. Circulation 2004, 109, 2705–2711. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| n−3 Fatty Acids | Placebo | |
|---|---|---|
| N | 12,933 | 12,938 |
| Age, mean (SD) | 67.1 (7.1) | 67.1 (7.1) |
| Female, n (%) | 6547 (50.6) | 6538 (50.5) |
| Race or ethnic group, N (%) | ||
| Non-Hispanic white | 9044 (71.5) | 9002 (71.2) |
| African American | 2549 (20.1) | 2557 (20.2) |
| Non-African American Hispanic | 491 (3.9) | 522 (4.1) |
| Asian | 200 (1.6) | 188 (1.5) |
| Native American | 120 (0.9) | 108 (0.9) |
| Other or unknown | 249 (2.0) | 274 (2.2) |
| BMI, mean (SD) | 28.1 (5.7) | 28.1 (5.8) |
| Dietary fish intake, servings/week, median (IQR) | 1.5 (0.9, 2.5) | 1.5 (0.9, 2.5) |
| Current smoking, N (%) | 920 (7.2) | 915 (7.2) |
| Medication use for hypertension | 6553 (51.0) | 6678 (52.0) |
| Medication use for diabetes | 1366 (10.6) | 1374 (10.6) |
| Medication use lowering cholesterol | 4800 (37.8) | 4742 (37.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogata, S.; Manson, J.E.; Kang, J.H.; Buring, J.E.; Lee, I.-M.; Nishimura, K.; Sakata, Y.; Danik, J.S.; D’Agostino, D.; Mora, S.; et al. Marine n−3 Fatty Acids and Prevention of Cardiovascular Disease: A Novel Analysis of the VITAL Trial Using Win Ratio and Hierarchical Composite Outcomes. Nutrients 2023, 15, 4235. https://doi.org/10.3390/nu15194235
Ogata S, Manson JE, Kang JH, Buring JE, Lee I-M, Nishimura K, Sakata Y, Danik JS, D’Agostino D, Mora S, et al. Marine n−3 Fatty Acids and Prevention of Cardiovascular Disease: A Novel Analysis of the VITAL Trial Using Win Ratio and Hierarchical Composite Outcomes. Nutrients. 2023; 15(19):4235. https://doi.org/10.3390/nu15194235
Chicago/Turabian StyleOgata, Soshiro, JoAnn E. Manson, Jae H. Kang, Julie E. Buring, I-Min Lee, Kunihiro Nishimura, Yasuhiko Sakata, Jacqueline Suk Danik, Denise D’Agostino, Samia Mora, and et al. 2023. "Marine n−3 Fatty Acids and Prevention of Cardiovascular Disease: A Novel Analysis of the VITAL Trial Using Win Ratio and Hierarchical Composite Outcomes" Nutrients 15, no. 19: 4235. https://doi.org/10.3390/nu15194235
APA StyleOgata, S., Manson, J. E., Kang, J. H., Buring, J. E., Lee, I.-M., Nishimura, K., Sakata, Y., Danik, J. S., D’Agostino, D., Mora, S., Albert, C. M., & Cook, N. R. (2023). Marine n−3 Fatty Acids and Prevention of Cardiovascular Disease: A Novel Analysis of the VITAL Trial Using Win Ratio and Hierarchical Composite Outcomes. Nutrients, 15(19), 4235. https://doi.org/10.3390/nu15194235