

Nutritional Status Indices and Monoclonal Gammopathy of Undetermined Significance Risk in the Elderly Population: Findings from the National Health and Nutrition Examination Survey



Abstract
:
1. Introduction
2. Methods
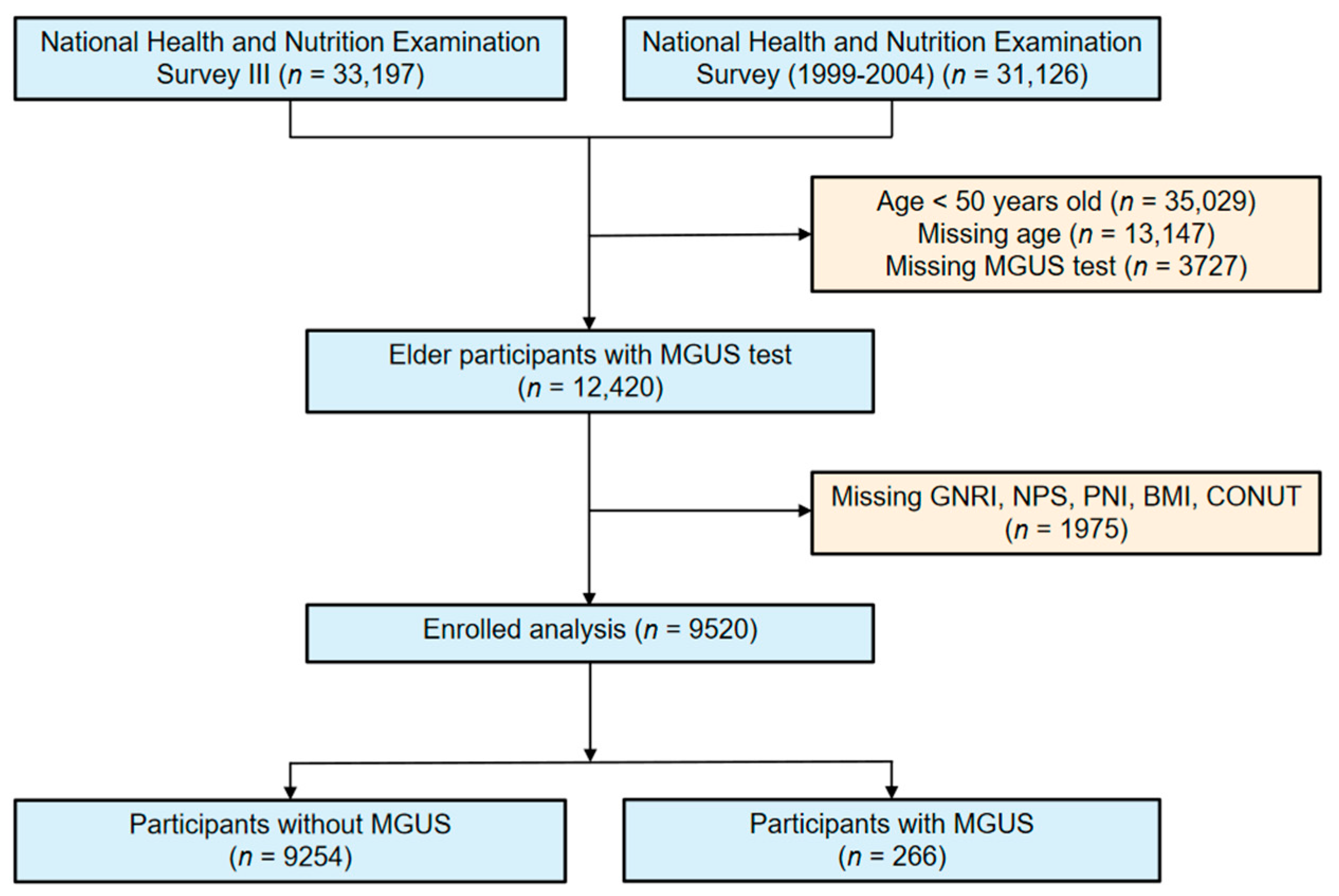
2.1. Study Design and Population
2.2. Assessment of MGUS
2.3. Analytic Samples
2.4. Assessments of Nutritional Status
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
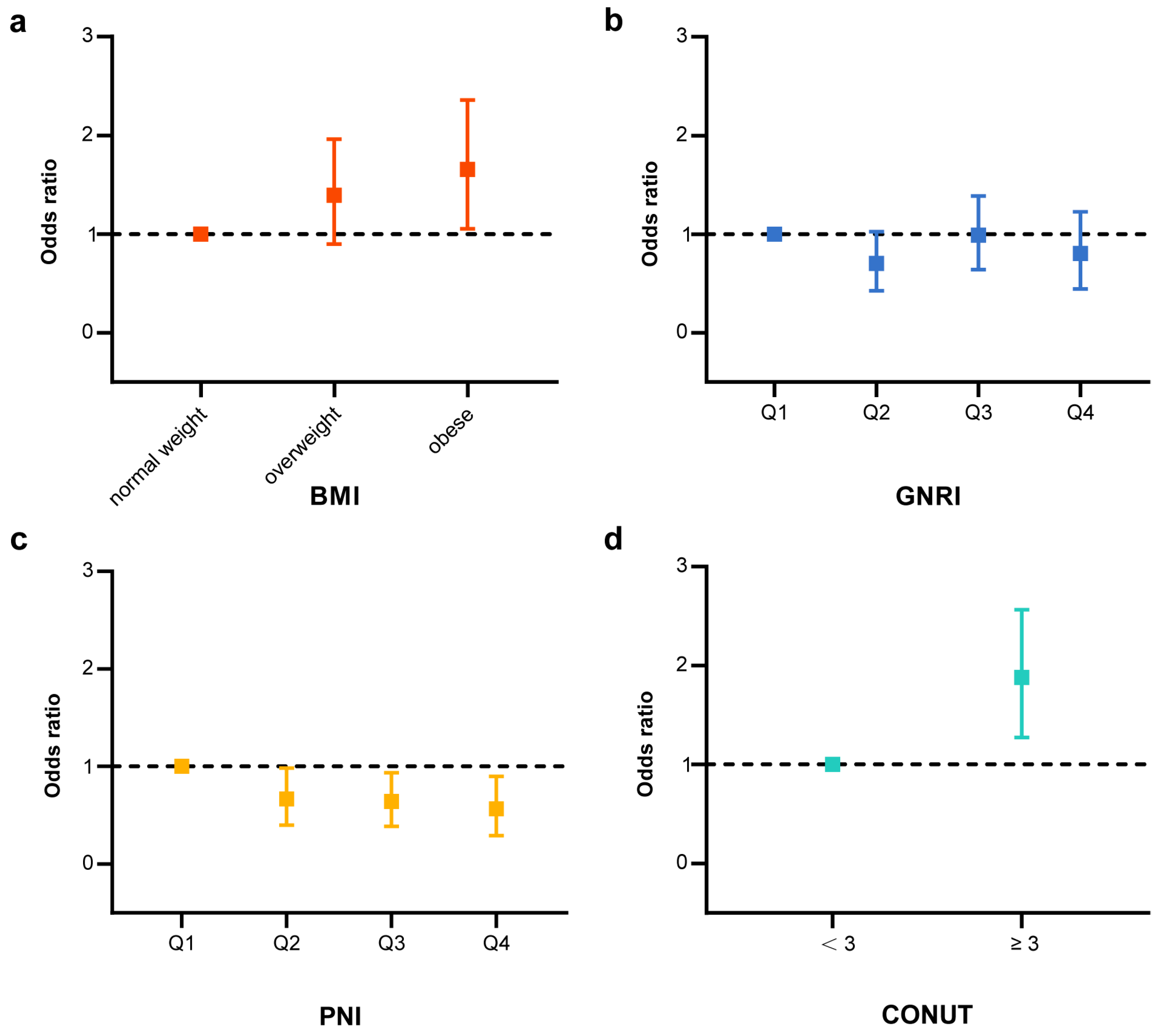
3.2. Association of Nutritional Indices and Prevalence of MGUS
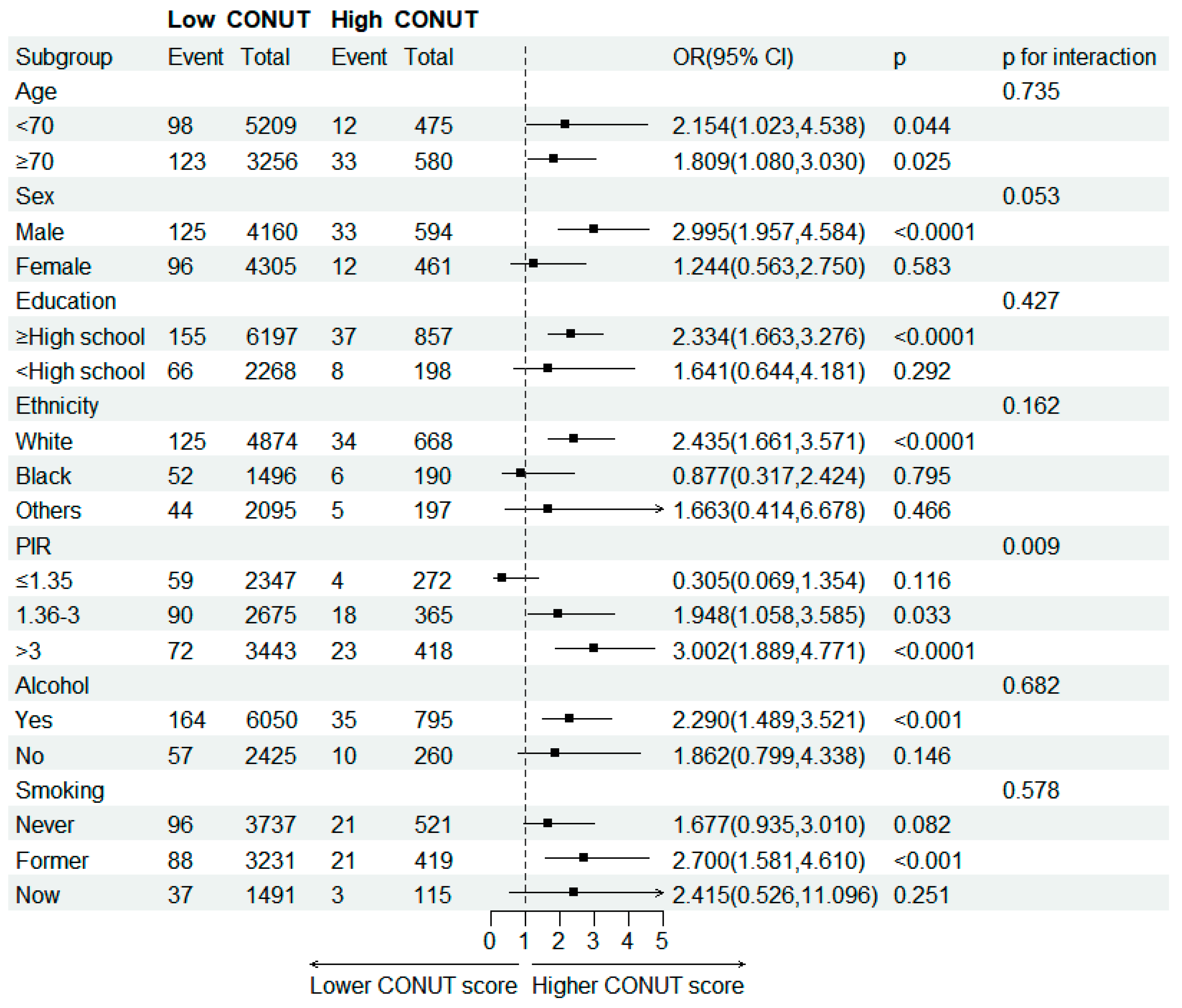
3.3. Subgroup Analysis of MGUS Participants Based on Nutritional Indices
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kyle, R.A.; Therneau, T.M.; Rajkumar, S.V.; Larson, D.R.; Plevak, M.F.; Offord, J.R.; Dispenzieri, A.; Katzmann, J.A.; Melton, L.J., 3rd. Prevalence of Monoclonal Gammopathy of Undetermined Significance. N. Engl. J. Med. 2006, 354, 1362–1369. [Google Scholar] [CrossRef] [PubMed]
- Atkin, C.; Reddy-Kolanu, V.; Drayson, M.T.; Sapey, E.; Richter, A.G. The Prevalence and Significance of Monoclonal Gammopathy of Undetermined Significance in Acute Medical Admissions. Br. J. Haematol. 2020, 189, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Kyle, R.A.; Pfeiffer, R.M.; Katzmann, J.A.; Caporaso, N.E.; Hayes, R.B.; Dispenzieri, A.; Kumar, S.; Clark, R.J.; Baris, D.; et al. Monoclonal Gammopathy of Undetermined Significance (MGUS) Consistently Precedes Multiple Myeloma: A Prospective Study. Blood 2009, 113, 5412–5417. [Google Scholar] [CrossRef]
- Landgren, O.; Graubard, B.I.; Katzmann, J.A.; Kyle, R.A.; Ahmadizadeh, I.; Clark, R.; Kumar, S.K.; Dispenzieri, A.; Greenberg, A.J.; Therneau, T.M.; et al. Racial Disparities in the Prevalence of Monoclonal Gammopathies: A Population-Based Study of 12,482 Persons from the National Health and Nutritional Examination Survey. Leukemia 2014, 28, 1537–1542. [Google Scholar] [CrossRef]
- Waxman, A.J.; Mink, P.J.; Devesa, S.S.; Anderson, W.F.; Weiss, B.M.; Kristinsson, S.Y.; McGlynn, K.A.; Landgren, O. Racial Disparities in Incidence and Outcome in Multiple Myeloma: A Population-Based Study. Blood 2010, 116, 5501–5506. [Google Scholar] [CrossRef] [PubMed]
- Recalde, M.; Davila-Batista, V.; Díaz, Y.; Leitzmann, M.; Romieu, I.; Freisling, H.; Duarte-Salles, T. Body Mass Index and Waist Circumference in Relation to the Risk of 26 Types of Cancer: A Prospective Cohort Study of 3.5 Million Adults in Spain. BMC Med. 2021, 19, 10. [Google Scholar] [CrossRef]
- Hofmann, J.N.; Moore, S.C.; Lim, U.; Park, Y.; Baris, D.; Hollenbeck, A.R.; Matthews, C.E.; Gibson, T.M.; Hartge, P.; Purdue, M.P. Body Mass Index and Physical Activity at Different Ages and Risk of Multiple Myeloma in the NIH-AARP Diet and Health Study. Am. J. Epidemiol. 2013, 177, 776–786. [Google Scholar] [CrossRef]
- Carson, K.R.; Bates, M.L.; Tomasson, M.H. The Skinny on Obesity and Plasma Cell Myeloma: A Review of the Literature. Bone Marrow Transpl. 2014, 49, 1009–1015. [Google Scholar] [CrossRef]
- Kleinstern, G.; Larson, D.R.; Allmer, C.; Norman, A.D.; Muntifering, G.; Sinnwell, J.; Visram, A.; Rajkumar, V.; Dispenzieri, A.; Kyle, R.A.; et al. Body Mass Index Associated with Monoclonal Gammopathy of Undetermined Significance (MGUS) Progression in Olmsted County, Minnesota. Blood Cancer J. 2022, 12, 67. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.P.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A Tool for Controlling Nutritional Status. First Validation in a Hospital Population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic Nutritional Index in Gastrointestinal Surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A New Index for Evaluating at-Risk Elderly Medical Patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Arero, G.; Arero, A.G.; Mohammed, S.H.; Vasheghani-Farahani, A. Prognostic Potential of the Controlling Nutritional Status (CONUT) Score in Predicting All-Cause Mortality and Major Adverse Cardiovascular Events in Patients with Coronary Artery Disease: A Meta-Analysis. Front. Nutr. 2022, 9, 850641. [Google Scholar] [CrossRef]
- Chen, M.-Y.; Wen, J.-X.; Lu, M.-T.; Jian, X.-Y.; Wan, X.-L.; Xu, Z.-W.; Liang, J.-Q.; Wu, J.-D. Association Between Prognostic Nutritional Index and Prognosis in Patients with Heart Failure: A Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 918566. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.S.; Yoo, J.; Jung, S.M.; Song, J.J.; Park, Y.-B.; Lee, S.-W. Comparison of the Clinical Implications among Five Different Nutritional Indices in Patients with Lupus Nephritis. Nutrients 2019, 11, 1456. [Google Scholar] [CrossRef]
- Correa-Rodríguez, M.; Pocovi-Gerardino, G.; Callejas-Rubio, J.-L.; Fernández, R.R.; Martín-Amada, M.; Cruz-Caparros, M.-G.; Ortego-Centeno, N.; Rueda-Medina, B. The Prognostic Nutritional Index and Nutritional Risk Index Are Associated with Disease Activity in Patients with Systemic Lupus Erythematosus. Nutrients 2019, 11, 638. [Google Scholar] [CrossRef]
- Kim, H.; Shin, D.-M.; Lee, J.-H.; Cho, E.-S.; Lee, H.S.; Shin, S.-J.; Park, E.J.; Baik, S.H.; Lee, K.Y.; Kang, J. Combining Prognostic Nutritional Index (PNI) and Controlling Nutritional Status (CONUT) Score as a Valuable Prognostic Factor for Overall Survival in Patients with Stage I-III Colorectal Cancer. Front. Oncol. 2023, 13, 1026824. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. The Challenge of Reforming Nutritional Epidemiologic Research. JAMA 2018, 320, 969–970. [Google Scholar] [CrossRef]
- Key, T.J.; Bradbury, K.E.; Perez-Cornago, A.; Sinha, R.; Tsilidis, K.K.; Tsugane, S. Diet, Nutrition, and Cancer Risk: What Do We Know and What Is the Way Forward? BMJ 2020, 368, m511. [Google Scholar] [CrossRef]
- Ezzati, T.M.; Massey, J.T.; Waksberg, J.; Chu, A.; Maurer, K.R. Sample Design: Third National Health and Nutrition Examination Survey; Vital and Health Statistics, Series 2; National Center for Health Statistics: Hyattsville, MD, USA, 1992; pp. 1–35. [Google Scholar]
- Curtin, L.R.; Mohadjer, L.K.; Dohrmann, S.M.; Montaquila, J.M.; Kruszan-Moran, D.; Mirel, L.B.; Carroll, M.D.; Hirsch, R.; Schober, S.; Johnson, C.L. The National Health and Nutrition Examination Survey: Sample Design, 1999–2006; Vital and Health Statistics, Series 2; National Center for Health Statistics: Hyattsville, MD, USA, 2012; pp. 1–39. [Google Scholar]
- Zhao, X.-H.; Shen, W.-B.; Wang, D.; Wang, H.-S.; Song, C.-Y.; Deng, W.-Z. The Prognosis Value of CONUT and SIS Score for Recurrent or Metastatic Esophageal Squamous Cell Carcinoma Patients Treated with Second-Line Immunotherapy. Front. Oncol. 2023, 13, 1167625. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, C.; Ji, R.; Lu, H.; Zhang, W.; Li, L.-L.; Liu, R.; Qian, H.; He, A. Prognostic Significance of the Controlling Nutritional Status (CONUT) Score in Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2020, 30, 74–82. [Google Scholar] [CrossRef]
- Zhang, G.; Zhang, Y.; He, F.; Wu, H.; Wang, C.; Fu, C. Preoperative Controlling Nutritional Status (CONUT) Score Is a Prognostic Factor for Early-Stage Cervical Cancer Patients with High-Risk Factors. Gynecol. Oncol. 2021, 162, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Toyokawa, T.; Kubo, N.; Tamura, T.; Sakurai, K.; Amano, R.; Tanaka, H.; Muguruma, K.; Yashiro, M.; Hirakawa, K.; Ohira, M. The Pretreatment Controlling Nutritional Status (CONUT) Score Is an Independent Prognostic Factor in Patients with Resectable Thoracic Esophageal Squamous Cell Carcinoma: Results from a Retrospective Study. BMC Cancer 2016, 16, 722. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E. Regression Modeling Strategies; Springer International Publishing: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Landgren, O.; Rajkumar, S.V.; Pfeiffer, R.M.; Kyle, R.A.; Katzmann, J.A.; Dispenzieri, A.; Cai, Q.; Goldin, L.R.; Caporaso, N.E.; Fraumeni, J.F.; et al. Obesity Is Associated with an Increased Risk of Monoclonal Gammopathy of Undetermined Significance among Black and White Women. Blood 2010, 116, 1056–1059. [Google Scholar] [CrossRef] [PubMed]
- Britton, J.A.; Khan, A.E.; Rohrmann, S.; Becker, N.; Linseisen, J.; Nieters, A.; Kaaks, R.; Tjønneland, A.; Halkjaer, J.; Severinsen, M.T.; et al. Anthropometric Characteristics and Non-Hodgkin’s Lymphoma and Multiple Myeloma Risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). Haematologica 2008, 93, 1666–1677. [Google Scholar] [CrossRef]
- Blair, C.K.; Cerhan, J.R.; Folsom, A.R.; Ross, J.A. Anthropometric Characteristics and Risk of Multiple Myeloma. Epidemiology 2005, 16, 691–694. [Google Scholar] [CrossRef]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-Mass Index and Incidence of Cancer: A Systematic Review and Meta-Analysis of Prospective Observational Studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Lin, J.-X.; Lin, L.-Z.; Tang, Y.-H.; Wang, J.-B.; Lu, J.; Chen, Q.-Y.; Cao, L.-L.; Lin, M.; Tu, R.-H.; Huang, C.-M.; et al. Which Nutritional Scoring System Is More Suitable for Evaluating the Short- or Long-Term Prognosis of Patients with Gastric Cancer Who Underwent Radical Gastrectomy? J. Gastrointest. Surg. 2020, 24, 1969–1977. [Google Scholar] [CrossRef]
- Mao, Y.-S.; Hao, S.-J.; Zou, C.-F.; Xie, Z.-B.; Fu, D.-L. Controlling Nutritional Status Score Is Superior to Prognostic Nutritional Index Score in Predicting Survival and Complications in Pancreatic Ductal Adenocarcinoma: A Chinese Propensity Score Matching Study. Br. J. Nutr. 2020, 124, 1190–1197. [Google Scholar] [CrossRef]
- Yoon, J.-P.; Nam, J.-S.; Abidin, M.F.B.Z.; Kim, S.-O.; Lee, E.-H.; Choi, I.-C.; Chin, J.-H. Comparison of Preoperative Nutritional Indexes for Outcomes after Primary Esophageal Surgery for Esophageal Squamous Cell Carcinoma. Nutrients 2021, 13, 4086. [Google Scholar] [CrossRef]
- Matsukawa, T.; Suto, K.; Kanaya, M.; Izumiyama, K.; Minauchi, K.; Yoshida, S.; Oda, H.; Miyagishima, T.; Mori, A.; Ota, S.; et al. Validation and Comparison of Prognostic Values of GNRI, PNI, and CONUT in Newly Diagnosed Diffuse Large B Cell Lymphoma. Ann. Hematol. 2020, 99, 2859–2868. [Google Scholar] [CrossRef]
- Yang, Z.; Zheng, Y.; Wu, Z.; Wen, Y.; Wang, G.; Chen, S.; Tan, F.; Li, J.; Wu, S.; Dai, M.; et al. Association between Pre-Diagnostic Serum Albumin and Cancer Risk: Results from a Prospective Population-Based Study. Cancer Med. 2021, 10, 4054–4065. [Google Scholar] [CrossRef] [PubMed]
- He, M.-M.; Fang, Z.; Hang, D.; Wang, F.; Polychronidis, G.; Wang, L.; Lo, C.-H.; Wang, K.; Zhong, R.; Knudsen, M.D.; et al. Circulating Liver Function Markers and Colorectal Cancer Risk: A Prospective Cohort Study in the UK Biobank. Int. J. Cancer 2021, 148, 1867–1878. [Google Scholar] [CrossRef]
- Kühn, T.; Sookthai, D.; Graf, M.E.; Schübel, R.; Freisling, H.; Johnson, T.; Katzke, V.; Kaaks, R. Albumin, Bilirubin, Uric Acid and Cancer Risk: Results from a Prospective Population-Based Study. Br. J. Cancer 2017, 117, 1572–1579. [Google Scholar] [CrossRef]
- Greipp, P.R.; San Miguel, J.; Durie, B.G.M.; Crowley, J.J.; Barlogie, B.; Bladé, J.; Boccadoro, M.; Child, J.A.; Avet-Loiseau, H.; Kyle, R.A.; et al. International Staging System for Multiple Myeloma. J. Clin. Oncol. 2005, 23, 3412–3420. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Avet-Loiseau, H.; Oliva, S.; Lokhorst, H.M.; Goldschmidt, H.; Rosinol, L.; Richardson, P.; Caltagirone, S.; Lahuerta, J.J.; Facon, T.; et al. Revised International Staging System for Multiple Myeloma: A Report from International Myeloma Working Group. J. Clin. Oncol. 2015, 33, 2863–2869. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, M.; Cairns, D.A.; Lahuerta, J.J.; Wester, R.; Bertsch, U.; Waage, A.; Zamagni, E.; Mateos, M.-V.; Dall’Olio, D.; van de Donk, N.W.C.J.; et al. Second Revision of the International Staging System (R2-ISS) for Overall Survival in Multiple Myeloma: A European Myeloma Network (EMN) Report Within the HARMONY Project. J. Clin. Oncol. 2022, 40, 3406–3418. [Google Scholar] [CrossRef] [PubMed]
- Kyle, R.A.; Therneau, T.M.; Rajkumar, S.V.; Remstein, E.D.; Offord, J.R.; Larson, D.R.; Plevak, M.F.; Melton, L.J., 3rd. Long-Term Follow-up of IgM Monoclonal Gammopathy of Undetermined Significance. Blood 2003, 102, 3759–3764. [Google Scholar] [CrossRef]
- Kadakia, K.C.; Symanowski, J.T.; Aktas, A.; Szafranski, M.L.; Salo, J.C.; Meadors, P.L.; Walsh, D. Malnutrition Risk at Solid Tumor Diagnosis: The Malnutrition Screening Tool in a Large US Cancer Institute. Support Care Cancer 2022, 30, 2237–2244. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B. Albumin--an Important Extracellular Antioxidant? Biochem. Pharmacol. 1988, 37, 569–571. [Google Scholar] [CrossRef]
- de Mutsert, R.; Grootendorst, D.C.; Indemans, F.; Boeschoten, E.W.; Krediet, R.T.; Dekker, F.W. Netherlands Cooperative Study on the Adequacy of Dialysis-II Study Group Association between Serum Albumin and Mortality in Dialysis Patients Is Partly Explained by Inflammation, and Not by Malnutrition. J. Ren. Nutr. 2009, 19, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Tian, S.; Ning, B.; Huang, T.; Li, Y.; Wei, Y. Stress and Cancer: The Mechanisms of Immune Dysregulation and Management. Front. Immunol. 2022, 13, 1032294. [Google Scholar] [CrossRef] [PubMed]
- Tienhaara, A.; Pelliniemi, T.T. Peripheral Blood Lymphocyte Subsets in Multiple Myeloma and Monoclonal Gammopathy of Undetermined Significance. Clin. Lab. Haematol. 1994, 16, 213–223. [Google Scholar] [CrossRef]
- Prabhala, R.H.; Neri, P.; Bae, J.E.; Tassone, P.; Shammas, M.A.; Allam, C.K.; Daley, J.F.; Chauhan, D.; Blanchard, E.; Thatte, H.S.; et al. Dysfunctional T Regulatory Cells in Multiple Myeloma. Blood 2006, 107, 301–304. [Google Scholar] [CrossRef]
- Pedersen, K.M.; Çolak, Y.; Bojesen, S.E.; Nordestgaard, B.G. Low High-Density Lipoprotein and Increased Risk of Several Cancers: 2 Population-Based Cohort Studies Including 116,728 Individuals. J. Hematol. Oncol. 2020, 13, 129. [Google Scholar] [CrossRef] [PubMed]
- Choi, T.; Choi, I.Y.; Han, K.; Jeong, S.-M.; Yoo, J.E.; Rhee, S.Y.; Park, Y.-G.; Shin, D.W. Lipid Level, Lipid Variability, and Risk of Multiple Myeloma: A Nationwide Population-Based Study of 3,527,776 Subjects. Cancers 2021, 13, 540. [Google Scholar] [CrossRef]
- Landgren, O.; Graubard, B.I.; Kumar, S.; Kyle, R.A.; Katzmann, J.A.; Murata, K.; Costello, R.; Dispenzieri, A.; Caporaso, N.; Mailankody, S.; et al. Prevalence of Myeloma Precursor State Monoclonal Gammopathy of Undetermined Significance in 12372 Individuals 10-49 Years Old: A Population-Based Study from the National Health and Nutrition Examination Survey. Blood Cancer J. 2017, 7, e618. [Google Scholar] [CrossRef]
- Wang, Y.-Z.; Wu, Q.-J.; Zhu, J.; Wu, L. Fish Consumption and Risk of Myeloma: A Meta-Analysis of Epidemiological Studies. Cancer Causes Control 2015, 26, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Thordardottir, M.; Lindqvist, E.K.; Lund, S.H.; Costello, R.; Burton, D.; Steingrimsdottir, L.; Korde, N.; Mailankody, S.; Eiriksdottir, G.; Launer, L.J.; et al. Dietary Intake Is Associated with Risk of Multiple Myeloma and Its Precursor Disease. PLoS ONE 2018, 13, e0206047. [Google Scholar] [CrossRef]
- Hosgood, H.D., 3rd; Baris, D.; Zahm, S.H.; Zheng, T.; Cross, A.J. Diet and Risk of Multiple Myeloma in Connecticut Women. Cancer Causes Control 2007, 18, 1065–1076. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Abbreviation | Calculation Formula | Reference |
|---|---|---|---|
| Body Mass Index | BMI | weight(kg)/(height(m))2 | |
| Prognostic Nutritional Index | PNI | (10 × serum albumin (g/dL)) + (0.005 × lymphocytes/μL) | [10] |
| Controlling Nutritional Status | CONUT | Serum albumin score + total lymphocyte count score + total cholesterol score. For serum albumin levels >3.5, between 3.0 and 3.49, between 2.5 and 2.99 and <2.5 g/dL, 0, 2, 4, and 6 points were assigned, respectively. For serum total cholesterol levels >180, between 140 and 179, between 100 and 139 and <100 mg/dL, 0, 1, 2, and 3 points were assigned, respectively. For serum total lymphocyte count >1600, between 1200 and 1599, between 800 and 1199 and <800/mm3, 0, 1, 2, and 3 points were assigned, respectively. Their sum ranges from <3 to ≥3. | [11] |
| Geriatric Nutritional Risk Index | GNRI | (1.489 × serum albumin (g/L) + 41.7 × (present weight/ideal body weight) ideal body weight = height(cm)—100—(height(cm)—150)/(4(male), 2.5(female)) | [12] |
| Variables | Non-MGUS | MGUS | p-Values |
|---|---|---|---|
| (n = 9254) | (n = 266) | ||
| Age—yrs, median | 63.63 (63.30, 64.16) | 68.83 (67.16, 70.50) | <0.001 ***,b |
| Sex | 0.08 | ||
| Female | 53.68 | 46.44 | |
| Male | 46.32 | 53.56 | |
| Dairy intake—kcal, median (IQR) | 1784.79 (1336.00, 2348.00) | 1730.76 (1277.00, 2315.00) | 0.32 a |
| Laboratory tests | |||
| Albumin—g/L | 41.97 (41.75, 42.18) | 40.36 (39.62, 41.11) | <0.001 ***,b |
| Total cholesterol—mg/dL | 216.84 (215.28, 218.40) | 208.65 (200.98, 216.32) | 0.04 *,b |
| Triglycerides—mmol/L | 1.77 (1.73, 1.81) | 1.81 (1.65, 1.97) | 0.63 b |
| Lymphocyte—×109/L | 2.13 (2.09, 2.16) | 2.10 (1.95, 2.25) | 0.75 b |
| BMI—kg/m2, median (IQR) | 27.14 (24.10, 30.88) | 27.90 (24.70, 31.47) | 0.39 a |
| PNI—point, median (IQR) | 52.00 (49.00, 55.50) | 50.50 (46.50, 53.75) | <0.001 ***,a |
| GNRI—point, median (IQR) | 114.28 (107.85, 121.91) | 113.35 (104.88, 120.46) | 0.048 *,a |
| BMI—kg/m2 | 0.24 | ||
| normal weight | 32.00 | 26.34 | |
| overweight | 38.47 | 41.51 | |
| obese | 29.52 | 32.14 | |
| CONUT strata | <0.001 *** | ||
| <3 | 90.72 | 81.73 | |
| ≥3 | 9.28 | 18.27 | |
| Race | 0.20 | ||
| Whites | 82.20 | 79.92 | |
| Blacks | 7.68 | 11.04 | |
| Others | 10.13 | 9.05 | |
| Education status | 0.29 | ||
| <high school | 17.78 | 20.72 | |
| ≥high school | 82.22 | 79.28 | |
| Smoking | 0.30 | ||
| Never smoked | 43.42 | 42.31 | |
| Former smoker | 38.80 | 43.77 | |
| Current smoker | 17.78 | 13.92 | |
| Drinking | 0.94 | ||
| No | 26.88 | 26.60 | |
| Yes | 73.12 | 73.40 | |
| Poverty | 0.01 * | ||
| ≤1.35 | 18.46 | 14.11 | |
| 1.36–3 | 28.97 | 38.94 | |
| >3 | 52.56 | 46.95 |
| Nutritional Indices | Model 1 a | Model 2 b | Model 3 c | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cases (n = 266) | Non-Cases (n = 9254) | Unadjusted or (95% CI) | p-Values | Multivariable Adjusted or (95% CI) | p-Values | Multivariable Adjusted or (95% CI) | p-Values | Multivariable Adjusted or (95% CI) | p-Values | |
| BMI | ||||||||||
| normal weight | 80 (30.07%) | 2878 (31.10%) | [Ref] | [Ref] | [Ref] | [Ref] | ||||
| overweight | 109 (40.98%) | 3699 (39.97%) | 1.311 (0.900–1.910) | 0.155 | 1.331 (0.918–1.929) | 0.128 | 1.322 (0.911–1.918) | 0.138 | 1.327 (0.897–1.961) | 0.152 |
| obese | 77 (28.95%) | 2677 (28.93%) | 1.323 (0.887–1.971) | 0.165 | 1.567 (1.051–2.335) | 0.028 * | 1.547 (1.024–2.336) | 0.039 | 1.553 (1.023–2.358) | 0.039 * |
| p for trend | 0.155 | 0.026 * | 0.034 * | 0.036 * | ||||||
| PNI | ||||||||||
| Q1 | 112 (42.11%) | 2519 (27.22%) | [Ref] | [Ref] | [Ref] | [Ref] | ||||
| Q2 | 67 (25.19%) | 2365 (25.56%) | 0.556 (0.362–0.855) | 0.009 ** | 0.613 (0.391–0.960) | 0.033 * | 0.623 (0.397–0.979) | 0.041 * | 0.623 (0.396–0.979) | 0.04 * |
| Q3 | 46 (17.29%) | 2090 (22.58%) | 0.511 (0.335–0.780) | 0.003 ** | 0.586 (0.379–0.906) | 0.017 * | 0.602 (0.388–0.934) | 0.025 * | 0.600 (0.386–0.934) | 0.025 * |
| Q4 | 41 (15.41%) | 2280 (24.64%) | 0.407 (0.236–0.703) | 0.002 ** | 0.498 (0.286–0.867) | 0.015 * | 0.510 (0.289–0.902) | 0.022 * | 0.509 (0.290–0.896) | 0.02 * |
| p for trend | <0.001 *** | 0.005 ** | 0.008 ** | 0.008 ** | ||||||
| GNRI | ||||||||||
| Q1 | 88 (33.08%) | 2292 (24.77%) | [Ref] | [Ref] | [Ref] | [Ref] | ||||
| Q2 | 59 (22.19%) | 2321 (25.08%) | 0.611 (0.395–0.945) | 0.028 * | 0.656 (0.429–1.004) | 0.052 | 0.663 (0.432–1.018) | 0.06 | 0.660 (0.424–1.026) | 0.064 |
| Q3 | 63 (23.68%) | 2317 (25.04%) | 0.845 (0.574–1.244) | 0.386 | 0.947 (0.648–1.382) | 0.771 | 0.951 (0.646–1.400) | 0.795 | 0.942 (0.639–1.388) | 0.756 |
| Q4 | 56 (21.05%) | 2324 (25.11%) | 0.577 (0.358–0.930) | 0.025 * | 0.742 (0.455–1.211) | 0.226 | 0.746 (0.452–1.232) | 0.245 | 0.737 (0.443–1.227) | 0.233 |
| p for trend | 0.043 * | 0.378 | 0.409 | 0.377 | ||||||
| CONUT | ||||||||||
| <3 | 221 (83.08%) | 8244 (89.09%) | [Ref] | [Ref] | [Ref] | [Ref] | ||||
| ≥3 | 45 (16.92%) | 1010 (10.01%) | 2.186 (1.556, 3.073) | <0.001 *** | 1.814 (1.274, 2.582) | 0.001 *** | 1.799 (1.264, 2.561) | 0.002 ** | 1.805 (1.271, 2.564) | 0.002 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Wu, M.; Yu, Z.; Niu, T. Nutritional Status Indices and Monoclonal Gammopathy of Undetermined Significance Risk in the Elderly Population: Findings from the National Health and Nutrition Examination Survey. Nutrients 2023, 15, 4210. https://doi.org/10.3390/nu15194210
Li L, Wu M, Yu Z, Niu T. Nutritional Status Indices and Monoclonal Gammopathy of Undetermined Significance Risk in the Elderly Population: Findings from the National Health and Nutrition Examination Survey. Nutrients. 2023; 15(19):4210. https://doi.org/10.3390/nu15194210
Chicago/Turabian StyleLi, Linfeng, Mengrui Wu, Zhengyu Yu, and Ting Niu. 2023. "Nutritional Status Indices and Monoclonal Gammopathy of Undetermined Significance Risk in the Elderly Population: Findings from the National Health and Nutrition Examination Survey" Nutrients 15, no. 19: 4210. https://doi.org/10.3390/nu15194210
APA StyleLi, L., Wu, M., Yu, Z., & Niu, T. (2023). Nutritional Status Indices and Monoclonal Gammopathy of Undetermined Significance Risk in the Elderly Population: Findings from the National Health and Nutrition Examination Survey. Nutrients, 15(19), 4210. https://doi.org/10.3390/nu15194210