
Survivors Overcoming and Achieving Resiliency (SOAR): Mindful Eating Practice for Breast Cancer Survivors in a Virtual Teaching Kitchen
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. SOAR Intervention
2.3.1. Overview
2.3.2. Professional Team
2.3.3. Structure and Topics
2.4. Outcome Measures
Mindful Eating Questionnaire (MEQ) [37]
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute, N.C. Office of Cancer Survivorship Statistics and Graphs. Available online: https://cancercontrol.cancer.gov/ocs/statistics (accessed on 15 February 2023).
- Castro-Espin, C.; Agudo, A. The Role of Diet in Prognosis among Cancer Survivors: A Systematic Review and Meta-Analysis of Dietary Patterns and Diet Interventions. Nutrients 2022, 14, 348. [Google Scholar] [CrossRef] [PubMed]
- Ergas, I.J.; Cespedes Feliciano, E.M.; Bradshaw, P.T.; Roh, J.M.; Kwan, M.L.; Cadenhead, J.; Santiago-Torres, M.; Troeschel, A.N.; Laraia, B.; Madsen, K.; et al. Diet Quality and Breast Cancer Recurrence and Survival: The Pathways Study. JNCI Cancer Spectr. 2021, 5, pkab019. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Sarwer, D.B.; Troxel, A.B.; Sturgeon, K.; DeMichele, A.M.; Denlinger, C.S.; Schmitz, K.H. A randomized trial of exercise and diet on health-related quality of life in survivors of breast cancer with overweight or obesity. Cancer 2021, 127, 3856–3864. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, H.; Bradhurst, P.; Ma, L.X.; Tan, S.Y.C.; Egger, S.J.; Vardy, J.L. Body weight management in overweight and obese breast cancer survivors. Cochrane Database Syst. Rev. 2020, 12, CD012110. [Google Scholar] [CrossRef] [PubMed]
- Scott, E.; Daley, A.J.; Doll, H.; Woodroofe, N.; Coleman, R.E.; Mutrie, N.; Crank, H.; Powers, H.J.; Saxton, J.M. Effects of an exercise and hypocaloric healthy eating program on biomarkers associated with long-term prognosis after early-stage breast cancer: A randomized controlled trial. Cancer Causes Control 2013, 24, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Porciello, G.; Montagnese, C.; Crispo, A.; Grimaldi, M.; Libra, M.; Vitale, S.; Palumbo, E.; Pica, R.; Calabrese, I.; Cubisino, S.; et al. Mediterranean diet and quality of life in women treated for breast cancer: A baseline analysis of DEDiCa multicentre trial. PLoS ONE 2020, 15, e0239803. [Google Scholar] [CrossRef]
- Coro, D.G.; Hutchinson, A.D.; Banks, S.; Coates, A.M. Diet and cognitive function in cancer survivors with cancer-related cognitive impairment: A qualitative study. Eur. J. Cancer Care 2020, 29, e13303. [Google Scholar] [CrossRef]
- Zick, S.M.; Colacino, J.; Cornellier, M.; Khabir, T.; Surnow, K.; Djuric, Z. Fatigue reduction diet in breast cancer survivors: A pilot randomized clinical trial. Breast Cancer Res. Treat. 2017, 161, 299–310. [Google Scholar] [CrossRef]
- Anyene, I.C.; Ergas, I.J.; Kwan, M.L.; Roh, J.M.; Ambrosone, C.B.; Kushi, L.H.; Cespedes Feliciano, E.M. Plant-Based Dietary Patterns and Breast Cancer Recurrence and Survival in the Pathways Study. Nutrients 2021, 13, 3374. [Google Scholar] [CrossRef]
- Rock, C.L.; Flatt, S.W.; Natarajan, L.; Thomson, C.A.; Bardwell, W.A.; Newman, V.A.; Hollenbach, K.A.; Jones, L.; Caan, B.J.; Pierce, J.P. Plasma carotenoids and recurrence-free survival in women with a history of breast cancer. J. Clin. Oncol. 2005, 23, 6631–6638. [Google Scholar] [CrossRef]
- Rock, C.L.; Natarajan, L.; Pu, M.; Thomson, C.A.; Flatt, S.W.; Caan, B.J.; Gold, E.B.; Al-Delaimy, W.K.; Newman, V.A.; Hajek, R.A.; et al. Longitudinal biological exposure to carotenoids is associated with breast cancer-free survival in the Women’s Healthy Eating and Living Study. Cancer Epidemiol. Biomark. Prev. 2009, 18, 486–494. [Google Scholar] [CrossRef]
- Lee, E.; Levine, E.A.; Franco, V.I.; Allen, G.O.; Gong, F.; Zhang, Y.; Hu, J.J. Combined genetic and nutritional risk models of triple negative breast cancer. Nutr. Cancer 2014, 66, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Busch, C.; Burkard, M.; Leischner, C.; Lauer, U.M.; Frank, J.; Venturelli, S. Epigenetic activities of flavonoids in the prevention and treatment of cancer. Clin. Epigenetics 2015, 7, 64. [Google Scholar] [CrossRef] [PubMed]
- Arora, I.; Sharma, M.; Tollefsbol, T.O. Combinatorial Epigenetics Impact of Polyphenols and Phytochemicals in Cancer Prevention and Therapy. Int. J. Mol. Sci. 2019, 20, 4567. [Google Scholar] [CrossRef] [PubMed]
- Clinton, S.K.; Giovannucci, E.L.; Hursting, S.D. The World Cancer Research Fund/American Institute for Cancer Research Third Expert Report on Diet, Nutrition, Physical Activity, and Cancer: Impact and Future Directions. J. Nutr. 2020, 150, 663–671. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Healthy Diet. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 18 September 2023).
- Schmidt, F.M.; Weschenfelder, J.; Sander, C.; Minkwitz, J.; Thormann, J.; Chittka, T.; Mergl, R.; Kirkby, K.C.; Fasshauer, M.; Stumvoll, M.; et al. Inflammatory cytokines in general and central obesity and modulating effects of physical activity. PLoS ONE 2015, 10, e0121971. [Google Scholar] [CrossRef]
- Harris, B.H.L.; Macaulay, V.M.; Harris, D.A.; Klenerman, P.; Karpe, F.; Lord, S.R.; Harris, A.L.; Buffa, F.M. Obesity: A perfect storm for carcinogenesis. Cancer Metastasis Rev. 2022, 41, 491–515. [Google Scholar] [CrossRef]
- Wahl, S.; Drong, A.; Lehne, B.; Loh, M.; Scott, W.R.; Kunze, S.; Tsai, P.C.; Ried, J.S.; Zhang, W.; Yang, Y.; et al. Epigenome-wide association study of body mass index, and the adverse outcomes of adiposity. Nature 2017, 541, 81–86. [Google Scholar] [CrossRef]
- Vance, V.; Mourtzakis, M.; McCargar, L.; Hanning, R. Weight gain in breast cancer survivors: Prevalence, pattern and health consequences. Obes. Rev. 2011, 12, 282–294. [Google Scholar] [CrossRef]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef]
- Jarvandi, S.; Perez, M.; Margenthaler, J.; Colditz, G.A.; Kreuter, M.W.; Jeffe, D.B. Improving Lifestyle Behaviors after Breast Cancer Treatment among African American Women with and without Diabetes: Role of Health Care Professionals. Ann. Behav. Med. 2021, 55, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Johnston, E.A.; van der Pols, J.C.; Ekberg, S. Needs, preferences, and experiences of adult cancer survivors in accessing dietary information post-treatment: A scoping review. Eur. J. Cancer Care 2021, 30, e13381. [Google Scholar] [CrossRef] [PubMed]
- Redwine, L.S.; Schwartz, E.R.; Garland, E.L. Mindfulness Promotes Positive Health Behaviors by Enhancing Self-Regulation, Motivation, and Learning: Perspectives from Research and Clinical Care. J. Integr. Complement. Med. 2022, 28, 847–850. [Google Scholar] [CrossRef]
- Holzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How Does Mindfulness Meditation Work? Proposing Mechanisms of Action From a Conceptual and Neural Perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef] [PubMed]
- Schuman-Olivier, Z.; Trombka, M.; Lovas, D.A.; Brewer, J.A.; Vago, D.R.; Gawande, R.; Dunne, J.P.; Lazar, S.W.; Loucks, E.B.; Fulwiler, C. Mindfulness and Behavior Change. Harv. Rev. Psychiatry 2020, 28, 371–394. [Google Scholar] [CrossRef]
- Creswell, J.D.; Lindsay, E.K.; Villalba, D.K.; Chin, B. Mindfulness Training and Physical Health: Mechanisms and Outcomes. Psychosom. Med. 2019, 81, 224–232. [Google Scholar] [CrossRef] [PubMed]
- The Center for Mindful Eating. Mindful Eating. Available online: thecenterformindfuleating.org (accessed on 15 February 2023).
- Warren, J.M.; Smith, N.; Ashwell, M. A structured literature review on the role of mindfulness, mindful eating and intuitive eating in changing eating behaviours: Effectiveness and associated potential mechanisms. Nutr. Res. Rev. 2017, 30, 272–283. [Google Scholar] [CrossRef]
- Chung, S.; Zhu, S.; Friedmann, E.; Kelleher, C.; Kozlovsky, A.; Macfarlane, K.W.; Tkaczuk, K.H.; Ryan, A.S.; Griffith, K.A. Weight loss with mindful eating in African American women following treatment for breast cancer: A longitudinal study. Support. Care Cancer 2016, 24, 1875–1881. [Google Scholar] [CrossRef]
- Sattler, E.L.P.; Washington, A.M.; Young, H.N.; Cobran, E.; Hartzell, D.; Dunagan, K.A.; Davis, M. Effect of a Mindful Eating Intervention on Cardiometabolic Markers in Overweight and Obese Postmenopausal Breast Cancer Survivors—A Pilot Study. Fed. Am. Soc. Exp. Biol. 2017, 31, 790-31. [Google Scholar]
- Monlezun, D.J.; Kasprowicz, E.; Tosh, K.W.; Nix, J.; Urday, P.; Tice, D.; Sarris, L.; Harlan, T.S. Medical school-based teaching kitchen improves HbA1c, blood pressure, and cholesterol for patients with type 2 diabetes: Results from a novel randomized controlled trial. Diabetes Res. Clin. Pract. 2015, 109, 420–426. [Google Scholar] [CrossRef]
- Eisenberg, D.M.; Righter, A.C.; Matthews, B.; Zhang, W.; Willett, W.C.; Massa, J. Feasibility Pilot Study of a Teaching Kitchen and Self-Care Curriculum in a Workplace Setting. Am. J. Lifestyle Med. 2019, 13, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Collaborative, T.K. What Are Teaching Kitchens? Available online: https://teachingkitchens.org/what-are-teaching-kitchens/ (accessed on 15 August 2023).
- Eisenberg, D.M.; Pacheco, L.S.; McClure, A.C.; McWhorter, J.W.; Janisch, K.; Massa, J. Perspective: Teaching Kitchens: Conceptual Origins, Applications and Potential for Impact within Food Is Medicine Research. Nutrients 2023, 15, 2859. [Google Scholar] [CrossRef] [PubMed]
- Framson, C.; Kristal, A.R.; Schenk, J.M.; Littman, A.J.; Zeliadt, S.; Benitez, D. Development and validation of the mindful eating questionnaire. J. Am. Diet. Assoc. 2009, 109, 1439–1444. [Google Scholar] [CrossRef] [PubMed]
- Erinosho, T.O.; Pinard, C.A.; Nebeling, L.C.; Moser, R.P.; Shaikh, A.R.; Resnicow, K.; Oh, A.Y.; Yaroch, A.L. Development and implementation of the National Cancer Institute’s Food Attitudes and Behaviors Survey to assess correlates of fruit and vegetable intake in adults. PLoS ONE 2015, 10, e0115017. [Google Scholar] [CrossRef]
- Xunlin, N.G.; Lau, Y.; Klainin-Yobas, P. The effectiveness of mindfulness-based interventions among cancer patients and survivors: A systematic review and meta-analysis. Support. Care Cancer 2020, 28, 1563–1578. [Google Scholar] [CrossRef]
- Bower, J.E.; Partridge, A.H.; Wolff, A.C.; Thorner, E.D.; Irwin, M.R.; Joffe, H.; Petersen, L.; Crespi, C.M.; Ganz, P.A. Targeting Depressive Symptoms in Younger Breast Cancer Survivors: The Pathways to Wellness Randomized Controlled Trial of Mindfulness Meditation and Survivorship Education. J. Clin. Oncol. 2021, 39, 3473–3484. [Google Scholar] [CrossRef]
- Thomas, E.A.; Mijangos, J.L.; Hansen, P.A.; White, S.; Walker, D.; Reimers, C.; Beck, A.C.; Garland, E.L. Mindfulness-Oriented Recovery Enhancement Restructures Reward Processing and Promotes Interoceptive Awareness in Overweight Cancer Survivors: Mechanistic Results From a Stage 1 Randomized Controlled Trial. Integr. Cancer Ther. 2019, 18, 1534735419855138. [Google Scholar] [CrossRef]
- Miller, M.F.; Li, Z.; Habedank, M. A Randomized Controlled Trial Testing the Effectiveness of Coping with Cancer in the Kitchen, a Nutrition Education Program for Cancer Survivors. Nutrients 2020, 12, 3144. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on an Evidence Framework for Obesity Prevention Decision Making. An in-depth look at study designs and methodologies. In Bridging the Evidence Gap in Obesity Prevention: A Framework to Inform Decision Making; Kumanyika, S.K., Lynn, P., Sim, L.J., Eds.; National Academic Press (US): Washington, DC, USA, 2010. [Google Scholar]
- Bower, J.E.; Crosswell, A.D.; Stanton, A.L.; Crespi, C.M.; Winston, D.; Arevalo, J.; Ma, J.; Cole, S.W.; Ganz, P.A. Mindfulness meditation for younger breast cancer survivors: A randomized controlled trial. Cancer 2015, 121, 1231–1240. [Google Scholar] [CrossRef]
- Stanszus, L.S.; Frank, P.; Geiger, S.M. Healthy eating and sustainable nutrition through mindfulness? Mixed method results of a controlled intervention study. Appetite 2019, 141, 104325. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Variable | N Participants Indicating Response | Total N | |
|---|---|---|---|
| Cohort: | 2020F | 17 (16.7%) | 102 |
| 2021F | 15 (14.7%) | ||
| 2021S | 12 (11.8%) | ||
| 2022F | 18 (17.6%) | ||
| 2022S | 15 (14.7%) | ||
| 2023S | (24.5%) | ||
| BMI Group: | gte30 | 49 (48.0%) | 102 |
| lt30 | (50.0%) | ||
| “Missing” | (1.96%) | ||
| Pregnant: | Yes | 0 (0.00%) | 102 |
| No | 99 (97.1%) | ||
| “Missing” | 3 (2.94%) | ||
| Gender: | Female | 100 (98.0%) | 102 |
| Other | 2 (1.96%) | ||
| “Missing” | 0 (0.00%) | ||
| Age: | 18–34 years | 0 (0.00%) | 102 |
| 35–54 years | 29 (28.4%) | ||
| 55 or older | 69 (67.6%) | ||
| “Missing” | 4 (3.92%) | ||
| Hispanic: | Yes | 7 (6.86%) | 102 |
| No | 92 (90.2%) | ||
| “Missing” | 3 (2.94%) | ||
| Race: | Black | 13 (12.7%) | 102 |
| Other | 4 (3.92%) | ||
| White | 83 (81.4%) | ||
| “Missing” | 2 (1.96%) | ||
| Education: | College degree | 66 (64.7%) | 102 |
| HS degree | 7 (6.86%) | ||
| Some college | 26 (25.5%) | ||
| “Missing” | 3 (2.94%) | ||
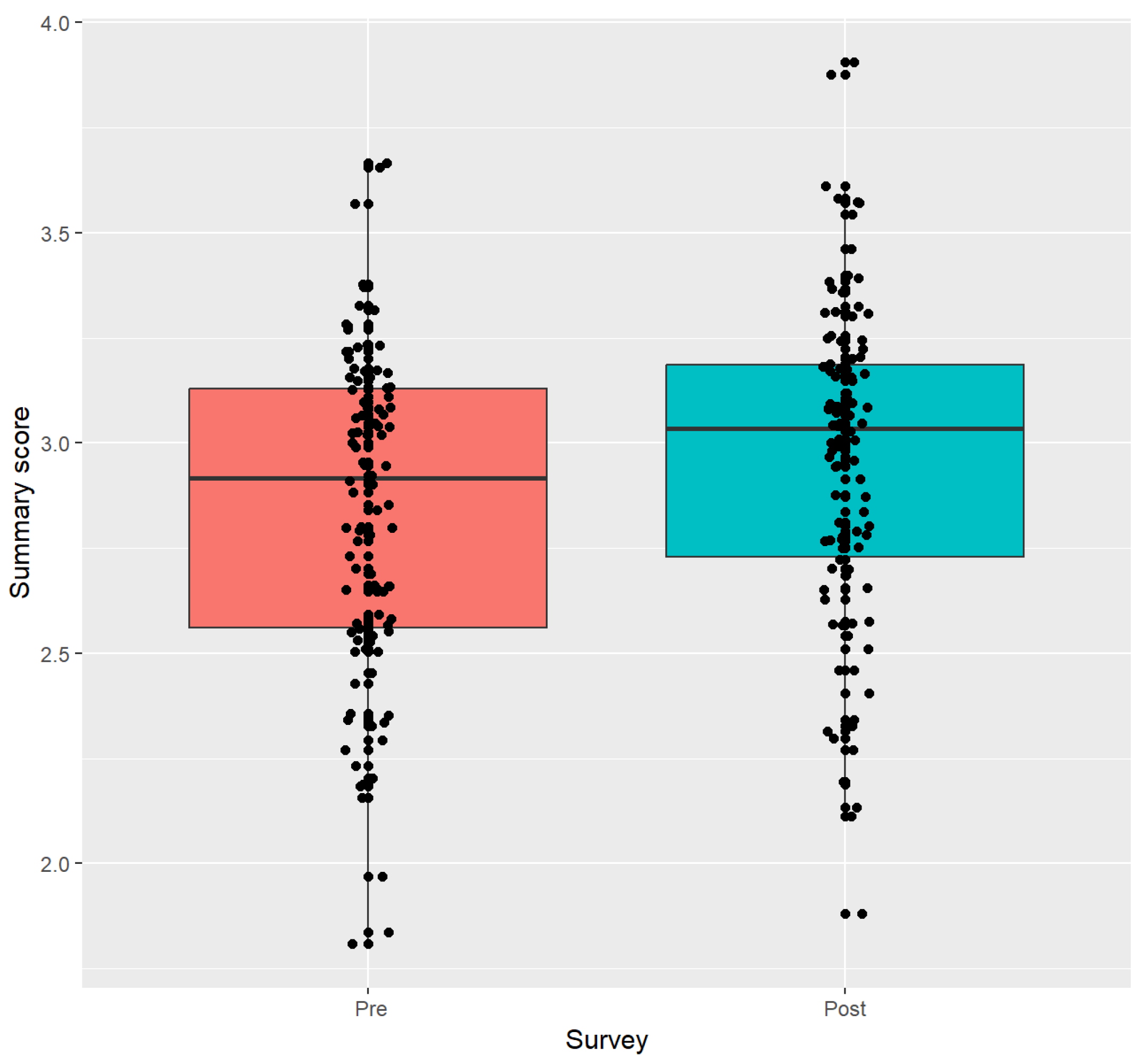
| Scale | Pre-SOAR Mean (Sd) | Post-SOAR Mean (Sd) | Mean Change (Sd) | p-Value |
|---|---|---|---|---|
| Summary Score | 2.84 (0.38) | 2.96 (0.39) | 0.12 (0.30) | 0.0003 |
| Awareness | 2.58 (0.59) | 2.73 (0.61) | 0.15 (0.49) | 0.0023 |
| Distraction | 3 (0.56) | 3.01 (0.52) | 0.01 (0.54) | 0.6718 |
| Disinhibition | 3.06 (0.63) | 3.18 (0.59) | 0.12 (0.4) | 0.0040 |
| Emotional Cues | 2.99 (0.77) | 3.16 (0.67) | 0.17 (0.54) | 0.0034 |
| External | 2.56 (0.59) | 2.7 (0.58) | 0.15 (0.50) | 0.0022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.; Riccardi, D.; Pflanzer, S.; Redwine, L.S.; Gray, H.L.; Carson, T.L.; McDowell, M.; Thompson, Z.; Hubbard, J.J.; Pabbathi, S. Survivors Overcoming and Achieving Resiliency (SOAR): Mindful Eating Practice for Breast Cancer Survivors in a Virtual Teaching Kitchen. Nutrients 2023, 15, 4205. https://doi.org/10.3390/nu15194205
Huang S, Riccardi D, Pflanzer S, Redwine LS, Gray HL, Carson TL, McDowell M, Thompson Z, Hubbard JJ, Pabbathi S. Survivors Overcoming and Achieving Resiliency (SOAR): Mindful Eating Practice for Breast Cancer Survivors in a Virtual Teaching Kitchen. Nutrients. 2023; 15(19):4205. https://doi.org/10.3390/nu15194205
Chicago/Turabian StyleHuang, Sherri, Diane Riccardi, Sonya Pflanzer, Laura S. Redwine, Heewon L. Gray, Tiffany L. Carson, Marc McDowell, Zachary Thompson, Jesse J. Hubbard, and Smitha Pabbathi. 2023. "Survivors Overcoming and Achieving Resiliency (SOAR): Mindful Eating Practice for Breast Cancer Survivors in a Virtual Teaching Kitchen" Nutrients 15, no. 19: 4205. https://doi.org/10.3390/nu15194205
APA StyleHuang, S., Riccardi, D., Pflanzer, S., Redwine, L. S., Gray, H. L., Carson, T. L., McDowell, M., Thompson, Z., Hubbard, J. J., & Pabbathi, S. (2023). Survivors Overcoming and Achieving Resiliency (SOAR): Mindful Eating Practice for Breast Cancer Survivors in a Virtual Teaching Kitchen. Nutrients, 15(19), 4205. https://doi.org/10.3390/nu15194205