
L-Glutamine and Survival of Patients with Locally Advanced Head and Neck Cancer Receiving Chemoradiotherapy


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
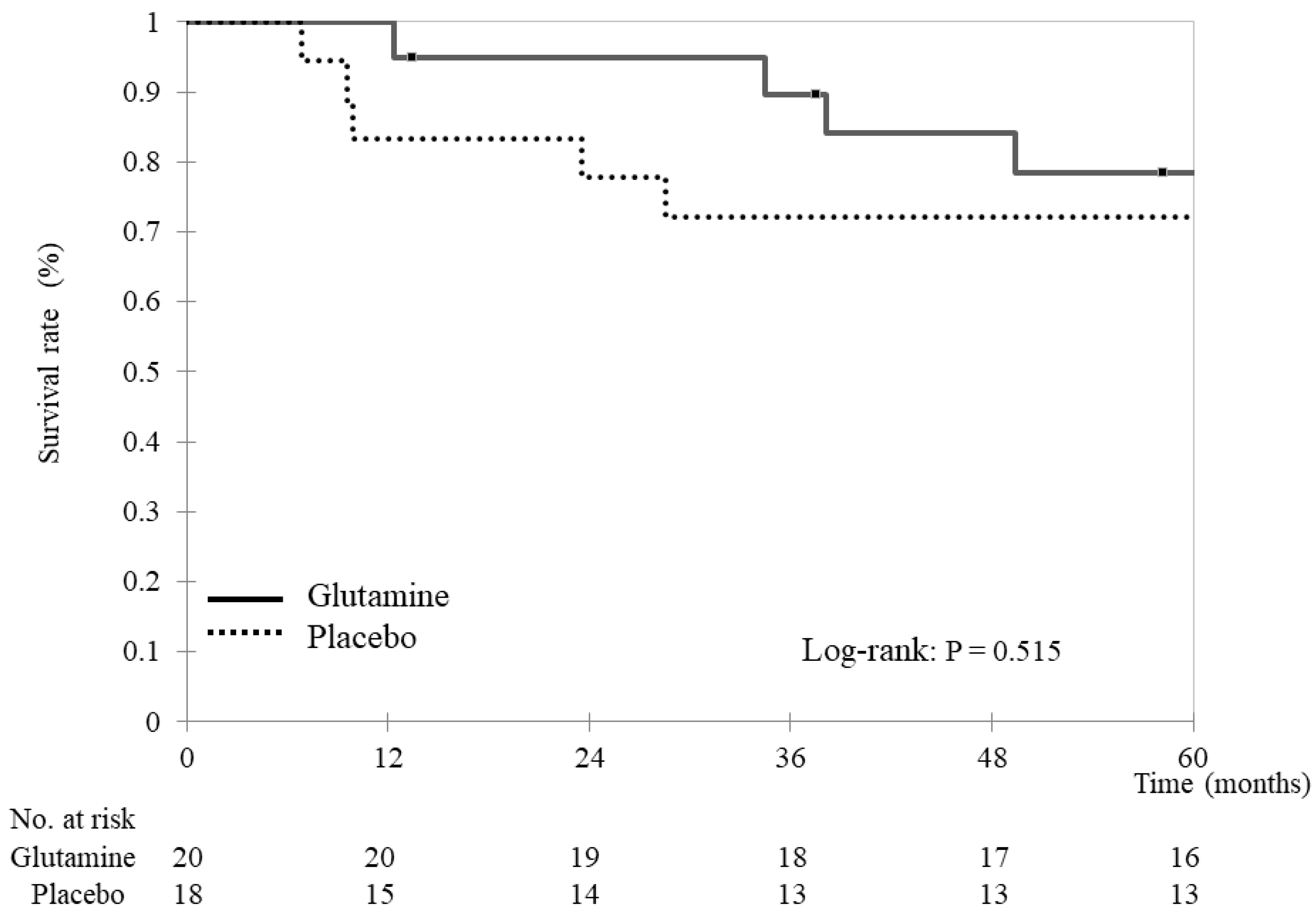
2.2. Survival
2.3. Statistical Analyses
3. Results
3.1. Overall Survival and Progression-Free Survival
3.2. Interruption and Salvage Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forastiere, A.A.; Trotti, A. Radiotherapy and concurrent chemotherapy: A strategy that improves locoregional control and survival in oropharyngeal cancer. J. Natl. Cancer Inst. 1999, 91, 2065–2066. [Google Scholar] [CrossRef]
- Groome, P.A.; O’Sullivan, B.; Mackillop, W.J.; Jackson, L.D.; Schulze, K.; Irish, J.C.; Warde, P.R.; Schneider, K.M.; Mackenzie, R.G.; Hodson, D.I.; et al. Compromised local control due to treatment interruptions and late treatment breaks in early glottic cancer: Population-based outcomes study supporting need for intensified treatment schedules. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 1002–1012. [Google Scholar] [CrossRef]
- Rosenthal, D.I.; Trotti, A. Strategies for managing radiation-induced mucositis in head and neck cancer. Semin. Radiat. Oncol. 2009, 19, 29–34. [Google Scholar] [CrossRef]
- Keefe, D.M.; Schubert, M.M.; Elting, L.S.; Sonis, S.T.; Epstein, J.B.; Raber-Durlacher, J.E.; Migliorati, C.A.; McGuire, D.B.; Hutchins, R.D.; Peterson, D.E.; et al. Updated clinical practice guidelines for the prevention and treatment of mucositis. Cancer 2007, 109, 820–831. [Google Scholar] [CrossRef]
- Quinn, B.; Potting, C.M.; Stone, R.; Blijlevens, N.M.; Fliedner, M.; Margulies, A.; Sharp, L. Guidelines for the assessment of oral mucositis in adult chemotherapy, radiotherapy and haematopoietic stem cell transplant patients. Eur. J. Cancer 2008, 44, 61–72. [Google Scholar] [CrossRef]
- Wasa, M.; Bode, B.P.; Abcouwer, S.F.; Collins, C.L.; Tanabe, K.K.; Souba, W.W. Glutamine as a regulator of DNA and protein biosynthesis in human solid tumor cell lines. Ann. Surg. 1996, 224, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Savarese, D.M.; Savy, G.; Vahdat, L.; Wischmeyer, P.E.; Corey, B. Prevention of chemotherapy and radiation toxicity with glutamine. Cancer Treat. Rev. 2003, 29, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Cerchietti, L.C.; Navigante, A.H.; Lutteral, M.A.; Castro, M.A.; Kirchuk, R.; Bonomi, M.; Cabalar, M.E.; Roth, B.; Negretti, G.; Sheinker, B.; et al. Double-blinded, placebo-controlled trial on intravenous L-alanyl-L-glutamine in the incidence of oral mucositis following chemoradiotherapy in patients with head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1330–1337. [Google Scholar] [CrossRef]
- Daniele, B.; Perrone, F.; Gallo, C.; Pignata, S.; De Martino, S.; De Vivo, R.; Barletta, E.; Tambaro, R.; Abbiati, R.; D’Agostino, L. Oral glutamine in the prevention of fluorouracil induced intestinal toxicity: A double blind, placebo controlled, randomised trial. Gut 2001, 48, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Topkan, E.; Yavuz, M.N.; Onal, C.; Yavuz, A.A. Prevention of acute radiation-induced esophagitis with glutamine in non-small cell lung cancer patients treated with radiotherapy: Evaluation of clinical and dosimetric parameters. Lung Cancer 2009, 63, 393–399. [Google Scholar] [CrossRef]
- Nose, S.; Wasa, M.; Tazuke, Y.; Owari, M.; Fukuzawa, M. Cisplatin upregulates glutamine transport in human intestinal epithelial cells: The protective mechanism of glutamine on intestinal mucosa after chemotherapy. JPEN J. Parenter. Enteral Nutr. 2010, 34, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, T.; Yamamoto, Y.; Wasa, M.; Takenaka, Y.; Nakahara, S.; Takagi, T.; Tsugane, M.; Hayashi, N.; Maeda, K.; Inohara, H.; et al. L-glutamine decreases the severity of mucositis induced by chemoradiotherapy in patients with locally advanced head and neck cancer: A double-blind, randomized, placebo-controlled trial. Oncol. Rep. 2015, 33, 33–39. [Google Scholar] [CrossRef]
- Pytlík, R.; Benes, P.; Patorková, M.; Chocenská, E.; Gregora, E.; Procházka, B.; Kozák, T. Standardized parenteral alanyl-glutamine dipeptide supplementation is not beneficial in autologous transplant patients: A randomized, double-blind, placebo controlled study. Bone Marrow Transpl. 2002, 30, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Kovacević, Z.; Morris, H.P. The role of glutamine in the oxidative metabolism of malignant cells. Cancer Res. 1972, 32, 326–333. [Google Scholar] [PubMed]
- Bode, B.P.; Kaminski, D.L.; Souba, W.W.; Li, A.P. Glutamine transport in isolated human hepatocytes and transformed liver cells. Hepatology 1995, 21, 511–520. [Google Scholar] [CrossRef]
- Fischer, C.P.; Bode, B.P.; Souba, W.W. Adaptive alterations in cellular metabolism with malignant transformation. Ann. Surg. 1998, 227, 627–634, discussion 634. [Google Scholar] [CrossRef]
- Knox, W.E.; Horowitz, M.L.; Friedell, G.H. The proportionality of glutaminase content to growth rate and morphology of rat neoplasms. Cancer Res. 1969, 29, 669–680. [Google Scholar]
- Klimberg, V.S.; Souba, W.W.; Salloum, R.M.; Plumley, D.A.; Cohen, F.S.; Dolson, D.J.; Bland, K.I.; Copeland, E.M. Glutamine-enriched diets support muscle glutamine metabolism without stimulating tumor growth. J. Surg. Res. 1990, 48, 319–323. [Google Scholar] [CrossRef]
- Topkan, E.; Parlak, C.; Topuk, S.; Pehlivan, B. Influence of oral glutamine supplementation on survival outcomes of patients treated with concurrent chemoradiotherapy for locally advanced non-small cell lung cancer. BMC Cancer 2012, 12, 502. [Google Scholar] [CrossRef]
- Li, Y.; Yu, Z.; Liu, F.; Tan, L.; Wu, B.; Li, J. Oral glutamine ameliorates chemotherapy-induced changes of intestinal permeability and does not interfere with the antitumor effect of chemotherapy in patients with breast cancer: A prospective randomized trial. Tumori 2006, 92, 396–401. [Google Scholar] [CrossRef]
- Gul, K.; Mehmet, K.; Meryem, A. The effects of oral glutamine on clinical and survival outcomes of non-small cell lung cancer patients treated with chemoradiotherapy. Clin. Nutr. 2017, 36, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Rubio, I.T.; Cao, Y.; Hutchins, L.F.; Westbrook, K.C.; Klimberg, V.S. Effect of glutamine on methotrexate efficacy and toxicity. Ann. Surg. 1998, 227, 772–778, discussion 778. [Google Scholar] [CrossRef] [PubMed]
- Rouse, K.; Nwokedi, E.; Woodliff, J.E.; Epstein, J.; Klimberg, V.S. Glutamine enhances selectivity of chemotherapy through changes in glutathione metabolism. Ann. Surg. 1995, 221, 420–426. [Google Scholar] [CrossRef]
- Salman, B.; Oguz, M.; Akmansu, M.; Bebitoglu, I.; Akca, G.; Sultan, N.; Emre, U.; Kerem, M.; Yilmaz, U. Effect of timing of glutamine-enriched enteral nutrition on intestinal damage caused by irradiation. Adv. Ther. 2007, 24, 648–661. [Google Scholar] [CrossRef]
- El Sharouni, S.Y.; Kal, H.B.; Battermann, J.J. Accelerated regrowth of non-small-cell lung tumours after induction chemotherapy. Br. J. Cancer 2003, 89, 2184–2189. [Google Scholar] [CrossRef]
- Koukourakis, M.; Hlouverakis, G.; Kosma, L.; Skarlatos, J.; Damilakis, J.; Giatromanolaki, A.; Yannakakis, D. The impact of overall treatment time on the results of radiotherapy for nonsmall cell lung carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 1996, 34, 315–322. [Google Scholar] [CrossRef]
- Diaz-Vivancos, P.; de Simone, A.; Kiddle, G.; Foyer, C.H. Glutathione-linking cell proliferation to oxidative stress. Free Radic. Biol. Med. 2015, 89, 1154–1164. [Google Scholar] [CrossRef]
- Ren, H.; Meng, Q.; Yepuri, N.; Du, X.; Sarpong, J.O.; Cooney, R.N. Protective effects of glutathione on oxidative injury induced by hydrogen peroxide in intestinal epithelial cells. J. Surg. Res. 2018, 222, 39–47. [Google Scholar] [CrossRef]
- Klimberg, V.S.; Pappas, A.A.; Nwokedi, E.; Jensen, J.C.; Broadwater, J.R.; Lang, N.P.; Westbrook, K.C. Effect of supplemental dietary glutamine on methotrexate concentrations in tumors. Arch. Surg. 1992, 127, 1317–1320. [Google Scholar] [CrossRef] [PubMed]
- Todorova, V.K.; Harms, S.A.; Kaufmann, Y.; Luo, S.; Luo, K.Q.; Babb, K.; Klimberg, V.S. Effect of dietary glutamine on tumor glutathione levels and apoptosis-related proteins in DMBA-induced breast cancer of rats. Breast. Cancer Res. Treat. 2004, 88, 247–256. [Google Scholar] [CrossRef]
- Leitão, R.F.; Ribeiro, R.A.; Lira, A.M.; Silva, L.R.; Bellaguarda, E.A.; Macedo, F.D.; Sousa, R.B.; Brito, G.A. Glutamine and alanyl-glutamine accelerate the recovery from 5-fluorouracil-induced experimental oral mucositis in hamster. Cancer Chemother. Pharmacol. 2008, 61, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Aquino, V.M.; Harvey, A.R.; Garvin, J.H.; Godder, K.T.; Nieder, M.L.; Adams, R.H.; Jackson, G.B.; Sandler, E.S. A double-blind randomized placebo-controlled study of oral glutamine in the prevention of mucositis in children undergoing hematopoietic stem cell transplantation: A pediatric blood and marrow transplant consortium study. Bone Marrow Transpl. 2005, 36, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Tao, K.M.; Li, X.Q.; Yang, L.Q.; Yu, W.F.; Lu, Z.J.; Sun, Y.M.; Wu, F.X. Glutamine supplementation for critically ill adults. Cochrane Database Syst. Rev. 2014, 2014, CD010050. [Google Scholar] [CrossRef]
- Wischmeyer, P.E. Glutamine in burn injury. Nutr. Clin. Pract. 2019, 34, 681–687. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsujimoto, T.; Wasa, M.; Inohara, H.; Ito, T. L-Glutamine and Survival of Patients with Locally Advanced Head and Neck Cancer Receiving Chemoradiotherapy. Nutrients 2023, 15, 4117. https://doi.org/10.3390/nu15194117
Tsujimoto T, Wasa M, Inohara H, Ito T. L-Glutamine and Survival of Patients with Locally Advanced Head and Neck Cancer Receiving Chemoradiotherapy. Nutrients. 2023; 15(19):4117. https://doi.org/10.3390/nu15194117
Chicago/Turabian StyleTsujimoto, Takae, Masafumi Wasa, Hidenori Inohara, and Toshinori Ito. 2023. "L-Glutamine and Survival of Patients with Locally Advanced Head and Neck Cancer Receiving Chemoradiotherapy" Nutrients 15, no. 19: 4117. https://doi.org/10.3390/nu15194117
APA StyleTsujimoto, T., Wasa, M., Inohara, H., & Ito, T. (2023). L-Glutamine and Survival of Patients with Locally Advanced Head and Neck Cancer Receiving Chemoradiotherapy. Nutrients, 15(19), 4117. https://doi.org/10.3390/nu15194117