
Association between Malnutrition and Migraine Risk Assessed Using Objective Nutritional Indices

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
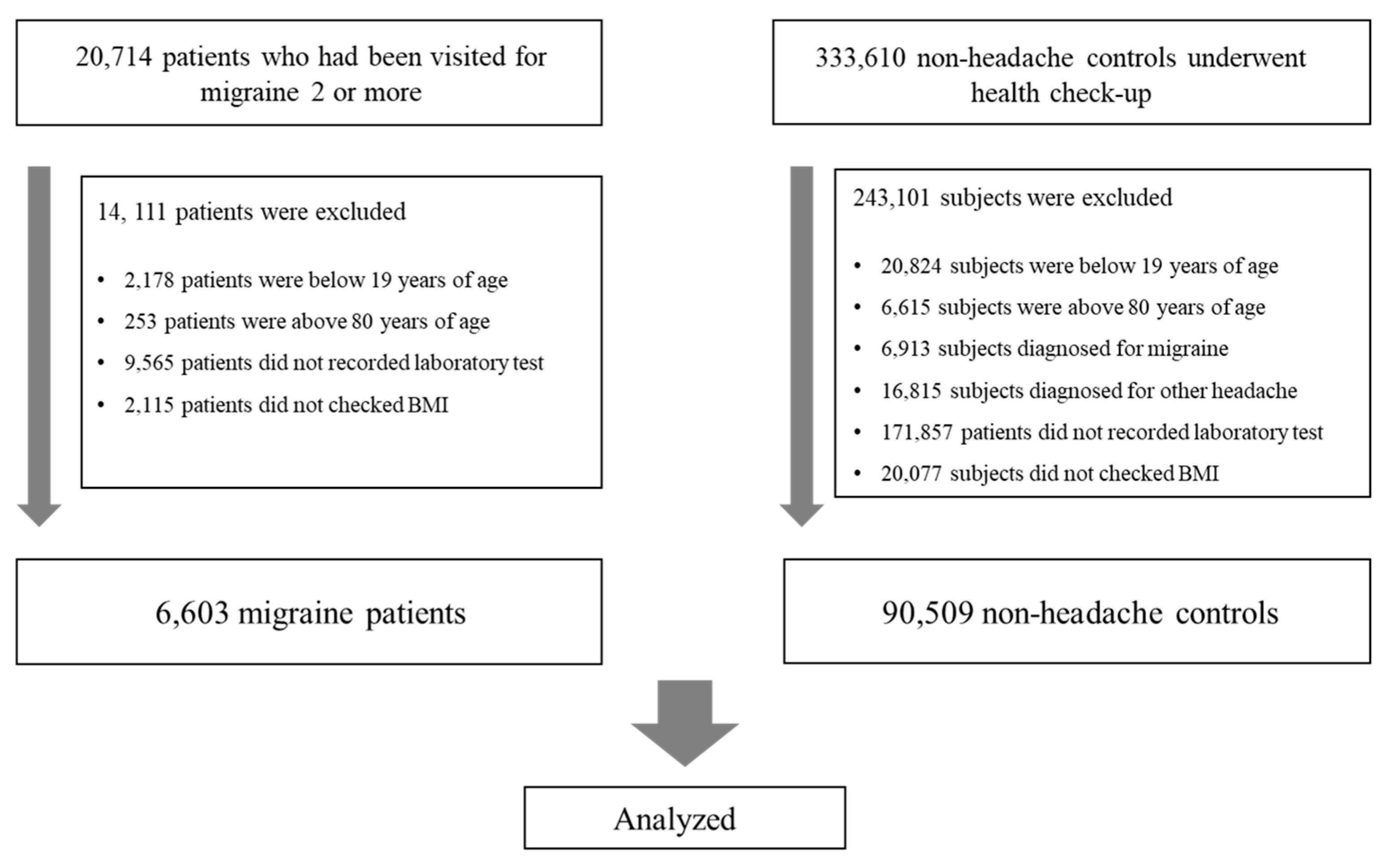
2.1. Subjects
2.2. Clinical Data Collection
2.3. Nutritional Status Assessments
2.4. Statistical Analyses
3. Results
3.1. Subject Characteristics
3.2. Comparison of Nutritional Status between Patient Groups
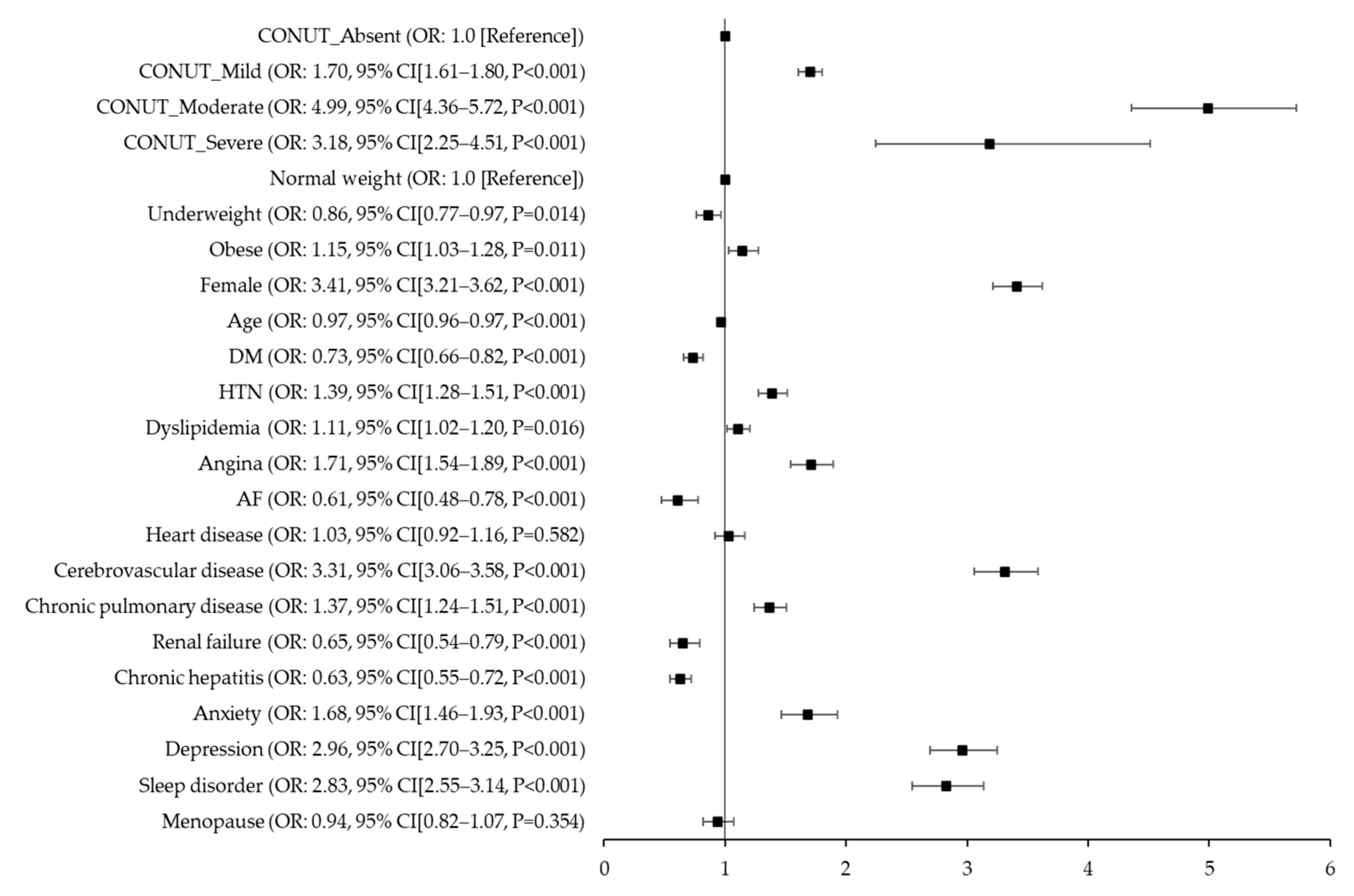
3.3. Association between Nutritional Status and Migraine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Nutritional Score | Risk of Malnutrition | |||
|---|---|---|---|---|
| Absent | Mild | Moderate | Severe | |
| CONUT (points) | 0–1 | 2–4 | 5–8 | 9–12 |
| Albumin (g/dL) | ≥3.5 | 3.0–3.4 | 2.5–2.9 | <2.5 |
| Score | 0 | 2 | 4 | 6 |
| Total cholesterol (mg/dL) | ≥180 | 140–179 | 100–139 | <100 |
| Score | 0 | 1 | 2 | 3 |
| Lymphocyte count (×109/L) | ≥1.60 | 1.20–1.59 | 0.80–1.19 | <0.80 |
| Score | 0 | 1 | 2 | 3 |
| PNI (points) | >38 | 35–38 | <35 | |
| Formula: 5 × lymphocyte count (109/L) + 10× serum albumin concentration (g/dL) | ||||
References
- Rockett, F.C.; de Oliveira, V.R.; Castro, K.; Chaves, M.L.; Perla Ada, S.; Perry, I.D. Dietary aspects of migraine trigger factors. Nutr. Rev. 2012, 70, 337–356. [Google Scholar] [CrossRef] [PubMed]
- Peroutka, S.J. What turns on a migraine? A systematic review of migraine precipitating factors. Curr. Pain Headache Rep. 2014, 18, 454. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Recober, A. Migraine and triggers: Post hoc ergo propter hoc? Curr. Pain Headache Rep. 2013, 17, 370. [Google Scholar] [CrossRef] [PubMed]
- Fukui, P.T.; Gonçalves, T.R.; Strabelli, C.G.; Lucchino, N.M.; Matos, F.C.; Santos, J.P.; Zukerman, E.; Zukerman-Guendler, V.; Mercante, J.P.; Masruha, M.R.; et al. Trigger factors in migraine patients. Arq. Neuropsiquiatr. 2008, 66, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Quintana, S.; Russo, M.; Torelli, P. Nutraceuticals and migraine: Further strategy for the treatment of specific conditions. Neurol. Sci. 2022, 43, 6565–6567. [Google Scholar] [CrossRef] [PubMed]
- Ramsden, C.E.; Zamora, D.; Faurot, K.R.; MacIntosh, B.; Horowitz, M.; Keyes, G.S.; Yuan, Z.X.; Miller, V.; Lynch, C.; Honvoh, G.; et al. Dietary alteration of n-3 and n-6 fatty acids for headache reduction in adults with migraine: Randomized controlled trial. BMJ 2021, 374, n1448. [Google Scholar] [CrossRef] [PubMed]
- Ramsden, C.E.; Faurot, K.R.; Zamora, D.; Palsson, O.S.; MacIntosh, B.A.; Gaylord, S.; Taha, A.Y.; Rapoport, S.I.; Hibbeln, J.R.; Davis, J.M.; et al. Targeted alterations in dietary n-3 and n-6 fatty acids improve life functioning and reduce psychological distress among patients with chronic headache: A secondary analysis of a randomized trial. J. Pain 2015, 156, 587–596. [Google Scholar] [CrossRef]
- Lovati, C.; d’Alessandro, C.M.; Ventura, S.D.; Muzio, F.; Pantoni, L. Ketogenic diet in refractory migraine: Possible efficacy and role of ketone bodies-a pilot experience. Neurol. Sci. 2022, 43, 6479–6485. [Google Scholar] [CrossRef]
- Finsterer, J.; Frank, M. Low-Glycemic-Index Diet Relieving Migraine but Inducing Muscle Cramps. J. Neurosci. Rural. Pract. 2019, 10, 552–554. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Pinto, A.; Ienca, R.; Coppola, G.; Sirianni, G.; Di Lorenzo, G.; Parisi, V.; Serrao, M.; Spagnoli, A.; Vestri, A.; et al. A Randomized Double-Blind, Cross-Over Trial of very Low-Calorie Diet in Overweight Migraine Patients: A Possible Role for Ketones? Nutrients 2019, 11, 1742. [Google Scholar] [CrossRef]
- Barbanti, P.; Fofi, L.; Aurilia, C.; Egeo, G.; Caprio, M. Ketogenic diet in migraine: Rationale, findings and perspectives. Neurol. Sci. 2017, 38, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Bakırhan, H.; Yıldıran, H.; Uyar Cankay, T. Associations between diet quality, DASH and Mediterranean dietary patterns and migraine characteristics. Nutr. Neurosci. 2022, 25, 2324–2334. [Google Scholar] [CrossRef] [PubMed]
- Arab, A.; Khorvash, F.; Karimi, E.; Hadi, A.; Askari, G. Associations between adherence to Mediterranean dietary pattern and frequency, duration, and severity of migraine headache: A cross-sectional study. Nutr. Neurosci. 2023, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Altamura, C.; Cecchi, G.; Bravo, M.; Brunelli, N.; Laudisio, A.; Caprio, P.D.; Botti, G.; Paolucci, M.; Khazrai, Y.M.; Vernieri, F. The Healthy Eating Plate Advice for Migraine Prevention: An Interventional Study. Nutrients 2020, 12, 1579. [Google Scholar] [CrossRef] [PubMed]
- Altamura, C.; Botti, G.; Paolucci, M.; Brunelli, N.; Cecchi, G.; Khazrai, M.; Vernieri, F. Promoting healthy eating can help preventing migraine: A real-life preliminary study. Neurol. Sci. 2018, 39, 155–156. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.T.; Vij, B. Diet and Headache: Part 2. Headache J. Head Face Pain 2016, 56, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Edvinsson, L.; Ekman, R. Release of vasoactive peptides in the extracerebral circulation of humans and the cat during activation of the trigeminovascular system. Ann. Neurol. 1988, 23, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Fila, M.; Chojnacki, J.; Sobczuk, P.; Chojnacki, C.; Blasiak, J. Nutrition and Calcitonin Gene Related Peptide (CGRP) in Migraine. Nutrients 2023, 15, 289. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Cai, J.; Li, Y.; Rong, X.; Li, Y.; He, L.; Li, H.; Liang, Y.; Huang, H.; Xu, Y.; et al. Baseline Objective Malnutritional Indices as Immune-Nutritional Predictors of Long-Term Recurrence in Patients with Acute Ischemic Stroke. Nutrients 2022, 14, 1337. [Google Scholar] [CrossRef]
- Akkuzu, M.Z.; Altıntaş, E.; Yaraş, S.; Sezgin, O.; Ateş, F.; Üçbilek, E.; Özdoğan, O. Controlling Nutritional Status (CONUT) Score and Prognostic Nutritional Index (PNI) Are Good Candidates for Prognostic Markers for Acute Pancreatitis. Medicina 2022, 59, 70. [Google Scholar] [CrossRef]
- Di Vincenzo, O.; Luisi, M.L.E.; Alicante, P.; Ballarin, G.; Biffi, B.; Gheri, C.F.; Scalfi, L. The Assessment of the Risk of Malnutrition (Undernutrition) in Stroke Patients. Nutrients 2023, 15, 683. [Google Scholar] [CrossRef] [PubMed]
- Serón-Arbeloa, C.; Labarta-Monzón, L.; Puzo-Foncillas, J.; Mallor-Bonet, T.; Lafita-López, A.; Bueno-Vidales, N.; Montoro-Huguet, M. Malnutrition Screening and Assessment. Nutrients 2022, 14, 2392. [Google Scholar] [CrossRef] [PubMed]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic nutritional index in gastrointestinal surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Iwakami, N.; Nagai, T.; Furukawa, T.A.; Sugano, Y.; Honda, S.; Okada, A.; Asaumi, Y.; Aiba, T.; Noguchi, T.; Kusano, K.; et al. Prognostic value of malnutrition assessed by Controlling Nutritional Status score for long-term mortality in patients with acute heart failure. Int. J. Cardiol. 2017, 230, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Iseki, Y.; Shibutani, M.; Maeda, K.; Nagahara, H.; Ohtani, H.; Sugano, K.; Ikeya, T.; Muguruma, K.; Tanaka, H.; Toyokawa, T.; et al. Impact of the Preoperative Controlling Nutritional Status (CONUT) Score on the Survival after Curative Surgery for Colorectal Cancer. PLoS ONE 2015, 10, e0132488. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.L.; Sung, S.H.; Cheng, H.M.; Hsu, P.F.; Guo, C.Y.; Yu, W.C.; Chen, C.H. Prognostic Nutritional Index and the Risk of Mortality in Patients with Acute Heart Failure. J. Am. Heart Assoc. 2017, 6, e004876. [Google Scholar] [CrossRef]
- Chen, Q.J.; Qu, H.J.; Li, D.Z.; Li, X.M.; Zhu, J.J.; Xiang, Y.; Li, L.; Ma, Y.T.; Yang, Y.N. Prognostic nutritional index predicts clinical outcome in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Sci. Rep. 2017, 7, 3285. [Google Scholar] [CrossRef]
- Pinato, D.J.; North, B.V.; Sharma, R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: The prognostic nutritional index (PNI). Br. J. Cancer 2012, 106, 1439–1445. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Lowe, E.F.; Stein, M.; Woolley, T.; Waycaster, M.; Scroggins, B.; Acuff, R.; Smith, J.T.; Lefemine, A.A. Prognostic Nutritional Index: Its usefulness as a predictor of clinical course. J. Am. Coll. Nutr. 1983, 2, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ma, L.; Zhao, L.; Sheng, J.; Xu, Y.; Chen, J.; Yu, L.; Sun, Q.; Zhou, H.; Zhu, S.; et al. Association Between the Prognostic Nutritional Index and Cognitive Function Among Older Adults in the United States: A Population-Based Study. J. Alzheimers Dis. JAD 2021, 83, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Liu, K.; Li, S.; Gao, Y.; Zhao, L.; Liu, H.; Fang, H.; Wu, J.; Sun, S.; Li, Y.; et al. Prognostic nutritional index predicts clinical outcomes in patients with cerebral venous sinus thrombosis. BMC Neurol. 2021, 21, 404. [Google Scholar] [CrossRef] [PubMed]
- Xiang, W.; Chen, X.; Ye, W.; Li, J.; Zhang, X.; Xie, D. Prognostic Nutritional Index for Predicting 3-Month Outcomes in Ischemic Stroke Patients Undergoing Thrombolysis. Front. Neurol. 2020, 11, 599. [Google Scholar] [CrossRef] [PubMed]
- Naito, H.; Nezu, T.; Hosomi, N.; Aoki, S.; Kinoshita, N.; Kuga, J.; Shimomura, R.; Araki, M.; Ueno, H.; Ochi, K.; et al. Controlling nutritional status score for predicting 3-mo functional outcome in acute ischemic stroke. Nutrition 2018, 55, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Gao, L.; Wu, K.; Jiang, X.; Chen, X.; Li, C.; Ge, W.; He, L.; Chen, N. Association between the prognostic nutritional index and severe headache or migraine: A population-based study. Nutr. Neurosci. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, X.; Kadasah, S.; Peng, C. Clinical Value of the Prognostic Nutrition Index in the Assessment of Prognosis in Critically Ill Patients with Stroke: A Retrospective Analysis. Comput. Math. Methods Med. 2022, 2022, 4889920. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, M.; Mo, H.J.; Kim, C.; Sohn, J.H.; Yu, K.H.; Lee, S.H. The association between malnutrition status and hemorrhagic transformation in patients with acute ischemic stroke receiving intravenous thrombolysis. BMC Neurol. 2023, 23, 106. [Google Scholar] [CrossRef]
- Soeters, P.; Bozzetti, F.; Cynober, L.; Forbes, A.; Shenkin, A.; Sobotka, L. Defining malnutrition: A plea to rethink. Clin. Nutr. 2017, 36, 896–901. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Leij-Halfwerk, S.; Verwijs, M.H.; van Houdt, S.; Borkent, J.W.; Guaitoli, P.R.; Pelgrim, T.; Heymans, M.W.; Power, L.; Visser, M.; Corish, C.A.; et al. Prevalence of protein-energy malnutrition risk in European older adults in community, residential and hospital settings, according to 22 malnutrition screening tools validated for use in adults ≥ 65 years: A systematic review and meta-analysis. Maturitas 2019, 126, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M.; Buse, D.C.; Ashina, H.; Pozo-Rosich, P.; Peres, M.F.P.; Lee, M.J.; Terwindt, G.M.; Halker Singh, R.; Tassorelli, C.; Do, T.P.; et al. Migraine: Integrated approaches to clinical management and emerging treatments. Lancet 2021, 397, 1505–1518. [Google Scholar] [CrossRef] [PubMed]
- Hindiyeh, N.A.; Zhang, N.; Farrar, M.; Banerjee, P.; Lombard, L.; Aurora, S.K. The Role of Diet and Nutrition in Migraine Triggers and Treatment: A Systematic Literature Review. Headache J. Head Face Pain 2020, 60, 1300–1316. [Google Scholar] [CrossRef]
- Gazerani, P. A Bidirectional View of Migraine and Diet Relationship. Neuropsychiatr. Dis. Treat. 2021, 17, 435–451. [Google Scholar] [CrossRef] [PubMed]
- Gazerani, P. Migraine and Diet. Nutrients 2020, 12, 1658. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Holland, P.R.; Martins-Oliveira, M.; Hoffmann, J.; Schankin, C.; Akerman, S. Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiol. Rev. 2017, 97, 553–622. [Google Scholar] [CrossRef] [PubMed]
- Fila, M.; Chojnacki, C.; Chojnacki, J.; Blasiak, J. Nutrients to Improve Mitochondrial Function to Reduce Brain Energy Deficit and Oxidative Stress in Migraine. Nutrients 2021, 13, 4433. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.F. CGRP-based Migraine Therapeutics: How Might They Work, Why So Safe, and What Next? ACS Pharm. Transl. Sci. 2019, 2, 2–8. [Google Scholar] [CrossRef]

| Migraine | Control | ASD | |
|---|---|---|---|
| (n = 6603) | (n = 90,509) | ||
| Median age, years (IQR) | 46 (36, 57) | 49 (39, 59) | 0.22 |
| Female, n (%) | 4888 (74.0%) | 40,528 (44.8%) | 0.59 |
| BMI categories, (n, %) | 0.03 | ||
| Underweight (<18.5) | 376 (5.7%) | 3570 (3.9%) | |
| Normal (18.5–29.9) | 5777 (87.5%) | 81,656 (90.2%) | |
| Obese (≥30) | 450 (6.8%) | 5283 (5.8%) | |
| Diabetes mellitus, n (%) | 535 (8.1%) | 7977 (8.8%) | 0.03 |
| Hypertension, n (%) | 1163 (17.6%) | 11,443 (12.6%) | 0.15 |
| Dyslipidemia, n (%) | 987 (14.9%) | 11,971 (13.2%) | 0.05 |
| Angina, n (%) | 635 (9.6%) | 5281 (5.8%) | 0.16 |
| AF, n (%) | 87 (1.3%) | 1413 (1.6%) | 0.02 |
| Heart disease, n (%) | 469 (7.1%) | 4760 (5.3%) | 0.08 |
| Cerebrovascular disease, n (%) | 1241 (18.8%) | 6534 (7.2%) | 0.43 |
| Chronic pulmonary disease, n (%) | 630 (9.5%) | 5610 (6.2%) | 0.14 |
| Renal failure, n (%) | 153 (2.3%) | 2258 (2.5%) | 0.01 |
| Chronic hepatitis, n (%) | 257 (3.9%) | 5353 (5.9%) | 0.09 |
| Anxiety disorder, n (%) | 368 (5.6%) | 1311 (1.4%) | 0.32 |
| Depression, n (%) | 953 (14.4%) | 2864 (3.2%) | 0.59 |
| Sleep disorder, n (%) | 690 (10.4%) | 2420 (2.7%) | 0.44 |
| Menopause, n (%) | 317 (4.8%) | 2613 (2.9%) | 0.11 |
| Migraine | Control | p | |
|---|---|---|---|
| (n = 6603) | (n = 90,509) | ||
| Median CONUT (IQR) | 1 (0, 2) | 1 (0, 2) | <0.001 |
| CONUT categories, (n, %) | <0.001 | ||
| Absent (0–1) | 3750 (56.8%) | 65,663 (72.5%) | |
| Mild (2–4) | 2455 (37.2%) | 23,009 (25.4%) | |
| Moderate (5–8) | 355 (5.4%) | 1502 (1.7%) | |
| Severe (9–12) | 43 (0.7%) | 335 (0.4%) | |
| Median PNI (IQR) | 52.1 (47.2, 56.3) | 54.7 (51.5, 57.8) | <0.001 |
| PNI categories by original scoring system, n (%) | <0.001 | ||
| Absent (>38) | 6356 (96.3%) | 89,408 (98.8%) | |
| Moderate (35–38) | 128 (1.9%) | 475 (0.5%) | |
| Severe (<35) | 119 (1.8%) | 626 (0.7%) | |
| PNI categories by tertiles, n (%) | <0.001 | ||
| Tertile 1 (<52.55) | 3519 (53.3%) | 28,844 (31.9%) | |
| Tertile 2 (52.55–56.59) | 1526 (23.1%) | 30,844 (34.1%) | |
| Tertile 3 (>56.59) | 1558 (23.6%) | 30,821 (34.1%) | |
| Unadjusted | p | Fully Adjusted | p | Backward Elimination | p | |
|---|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | ||||
| CONUT categories | ||||||
| Absent (0–1) | 1.0 [Reference] | 1.0 [Reference] | 1.0 [Reference] | |||
| Mild (2–4) | 1.87 (1.77–1.97) | <0.001 | 1.70 (1.61–1.80) | <0.001 | 1.70 (1.61–1.80) | <0.001 |
| Moderate (5–8) | 4.14 (3.67–4.67) | <0.001 | 4.99 (4.36–5.72) | <0.001 | 5.00 (4.37–5.74) | <0.001 |
| Severe (9–12) | 2.25 (1.63–3.09) | <0.001 | 3.18 (2.25–4.51) | <0.001 | 3.21 (2.26–4.54) | <0.001 |
| CONUT per 1-point increase | 1.26 (1.25–1.28) | <0.001 | 1.29 (1.27–1.31) | <0.001 | 1.29 (1.27–1.31) | <0.001 |
| PNI categories | ||||||
| By original scoring system | ||||||
| Absent (>38) | 1.0 [Reference] | 1.0 [Reference] | 1.0 [Reference] | |||
| Moderate (35–38) | 3.79 (3.11–4.62) | <0.001 | 4.76 (3.82–5.94) | <0.001 | 4.72 (3.79–5.89) | <0.001 |
| Severe (<35) | 2.67 (2.19–3.26) | <0.001 | 3.88 (3.11–4.84) | <0.001 | 3.87 (3.10–4.82) | <0.001 |
| By tertiles | ||||||
| Tertile 1 (<52.55) | 1.0 [Reference] | 1.0 [Reference] | 1.0 [Reference] | |||
| Tertile 2 (52.55–56.59) | 0.41 (0.38–0.43) | <0.001 | 0.43 (0.40–0.46) | <0.001 | 0.43 (0.40–0.46) | <0.001 |
| Tertile 3 (>56.59) | 0.41 (0.39–0.44) | <0.001 | 0.49 (0.46–0.53) | <0.001 | 0.49 (0.46–0.53) | <0.001 |
| PNI per 1-point increase | 0.93 (0.92–0.93) | <0.001 | 0.92 (0.92–0.93) | <0.001 | 0.92 (0.92–0.93) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Kwon, Y.-S.; Lee, J.J.; Lee, S.-H.; Sohn, J.-H. Association between Malnutrition and Migraine Risk Assessed Using Objective Nutritional Indices. Nutrients 2023, 15, 3828. https://doi.org/10.3390/nu15173828
Kim J-H, Kwon Y-S, Lee JJ, Lee S-H, Sohn J-H. Association between Malnutrition and Migraine Risk Assessed Using Objective Nutritional Indices. Nutrients. 2023; 15(17):3828. https://doi.org/10.3390/nu15173828
Chicago/Turabian StyleKim, Jong-Ho, Young-Suk Kwon, Jae Jun Lee, Sang-Hwa Lee, and Jong-Hee Sohn. 2023. "Association between Malnutrition and Migraine Risk Assessed Using Objective Nutritional Indices" Nutrients 15, no. 17: 3828. https://doi.org/10.3390/nu15173828
APA StyleKim, J.-H., Kwon, Y.-S., Lee, J. J., Lee, S.-H., & Sohn, J.-H. (2023). Association between Malnutrition and Migraine Risk Assessed Using Objective Nutritional Indices. Nutrients, 15(17), 3828. https://doi.org/10.3390/nu15173828