
Impact of Vitamin D Deficiency on Tumor Aggressiveness in Neuroendocrine Neoplasms


 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Subjects and Methods
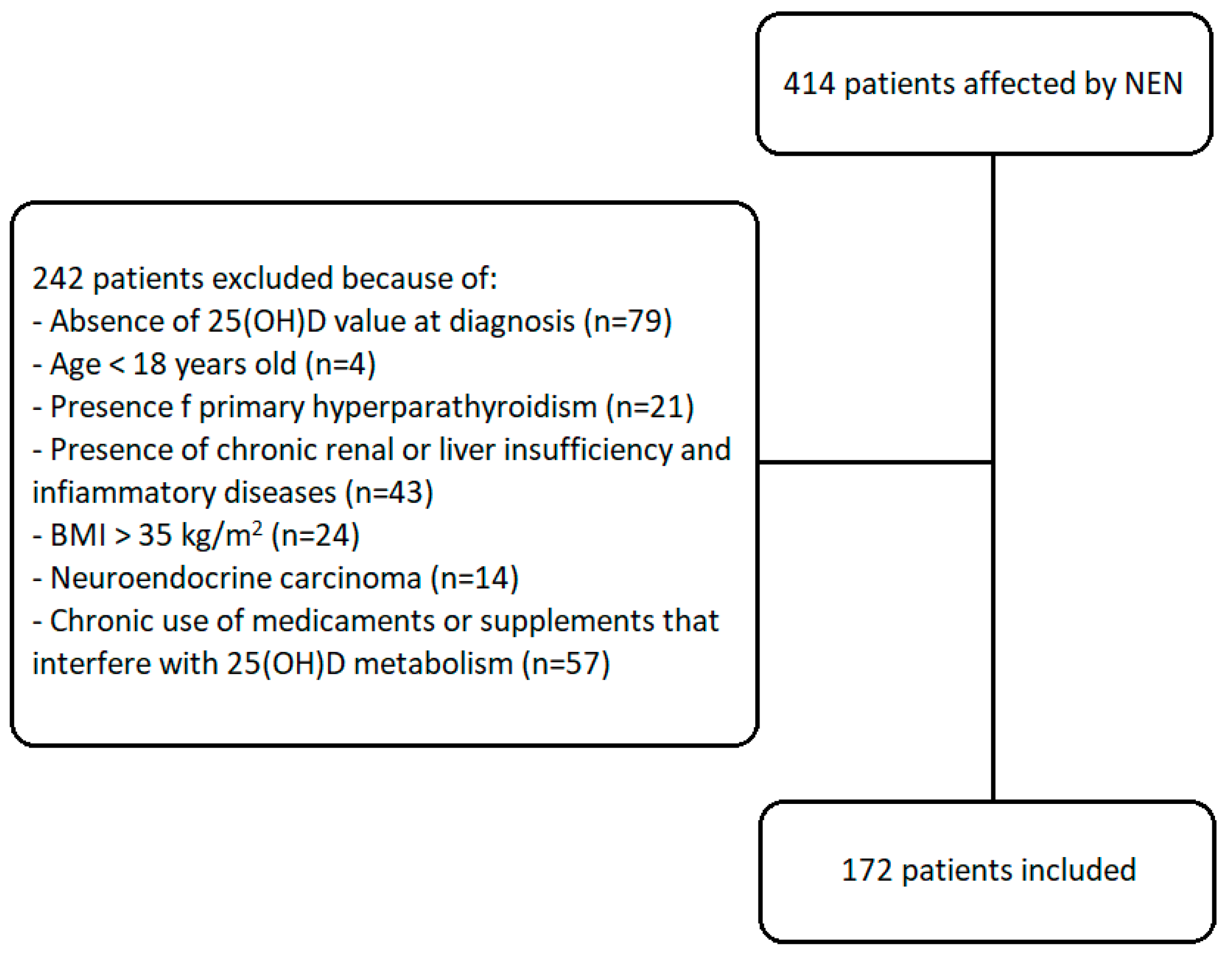
2.1. Study Design and Population
- -
- Presence of 25(OH)D value at diagnosis;
- -
- Age > 18 years old;
- -
- Absence of primary hyperparathyroidism (PTH levels above the upper limit due to dysregulated production by one or more hyperplastic parathyroids);
- -
- Absence of chronic renal or liver insufficiency and inflammatory diseases;
- -
- BMI < 35 kg/m2;
- -
- Well differentiation at cytological/histologic examination;
- -
- Absence of chronic use of medicaments or supplements known to interfere with 25(OH)D metabolism (including cinacalcet, calcium, bone antiresorptive therapies, sex-hormones and anti-inflammatories).
2.2. Laboratory Assessment
2.3. Statistical Analysis
3. Results
3.1. Clinical and Pathological Features
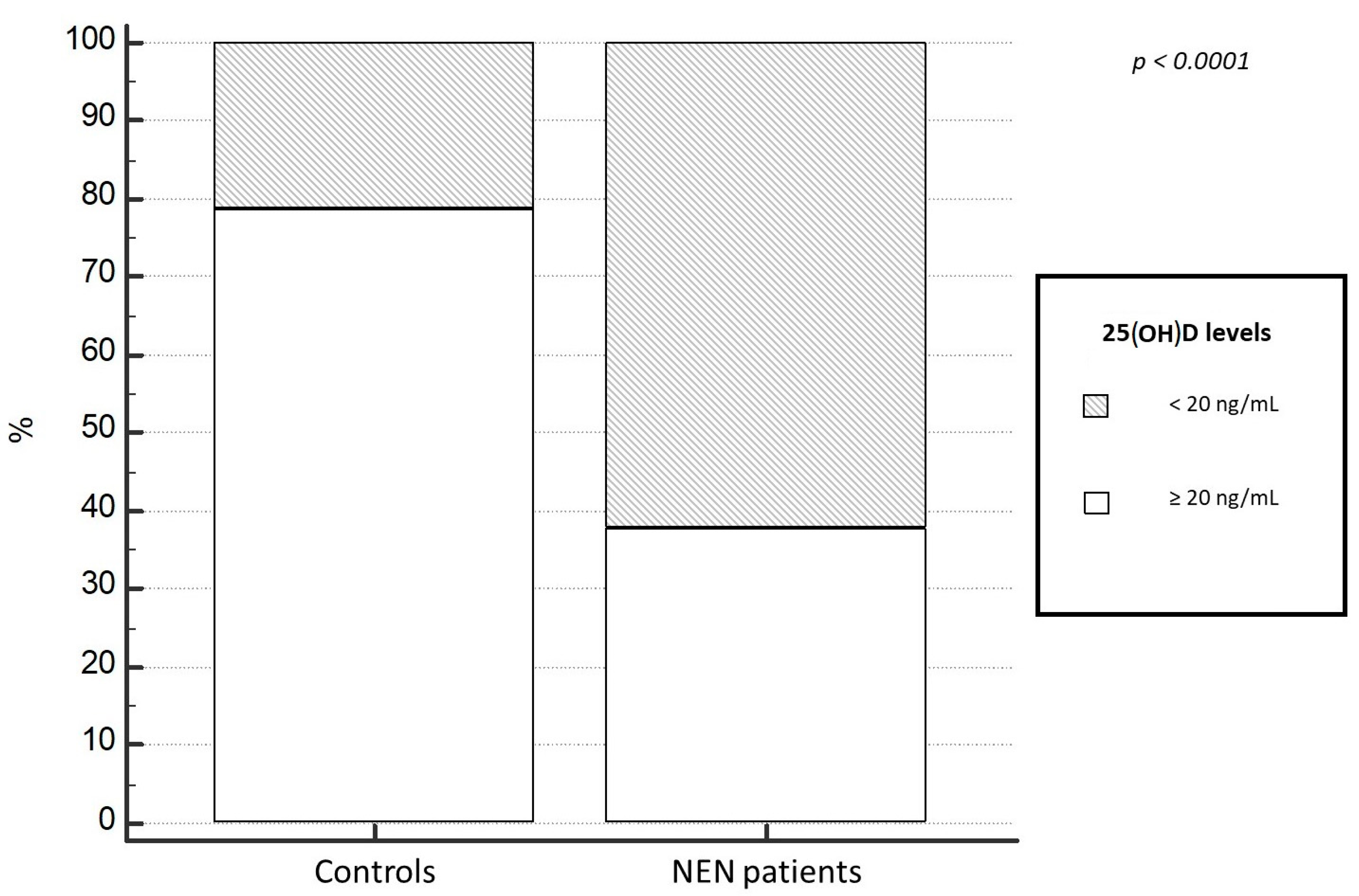
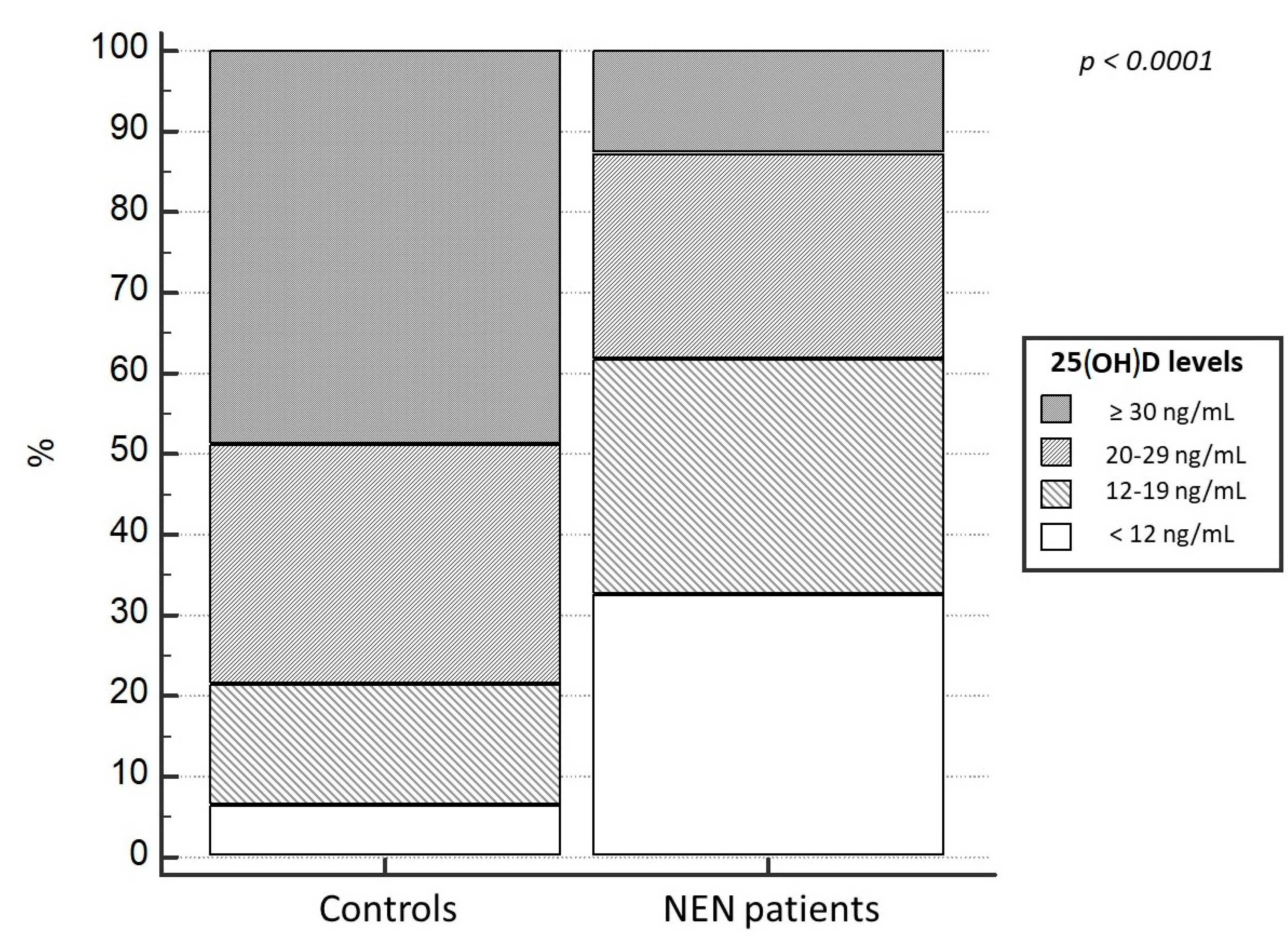
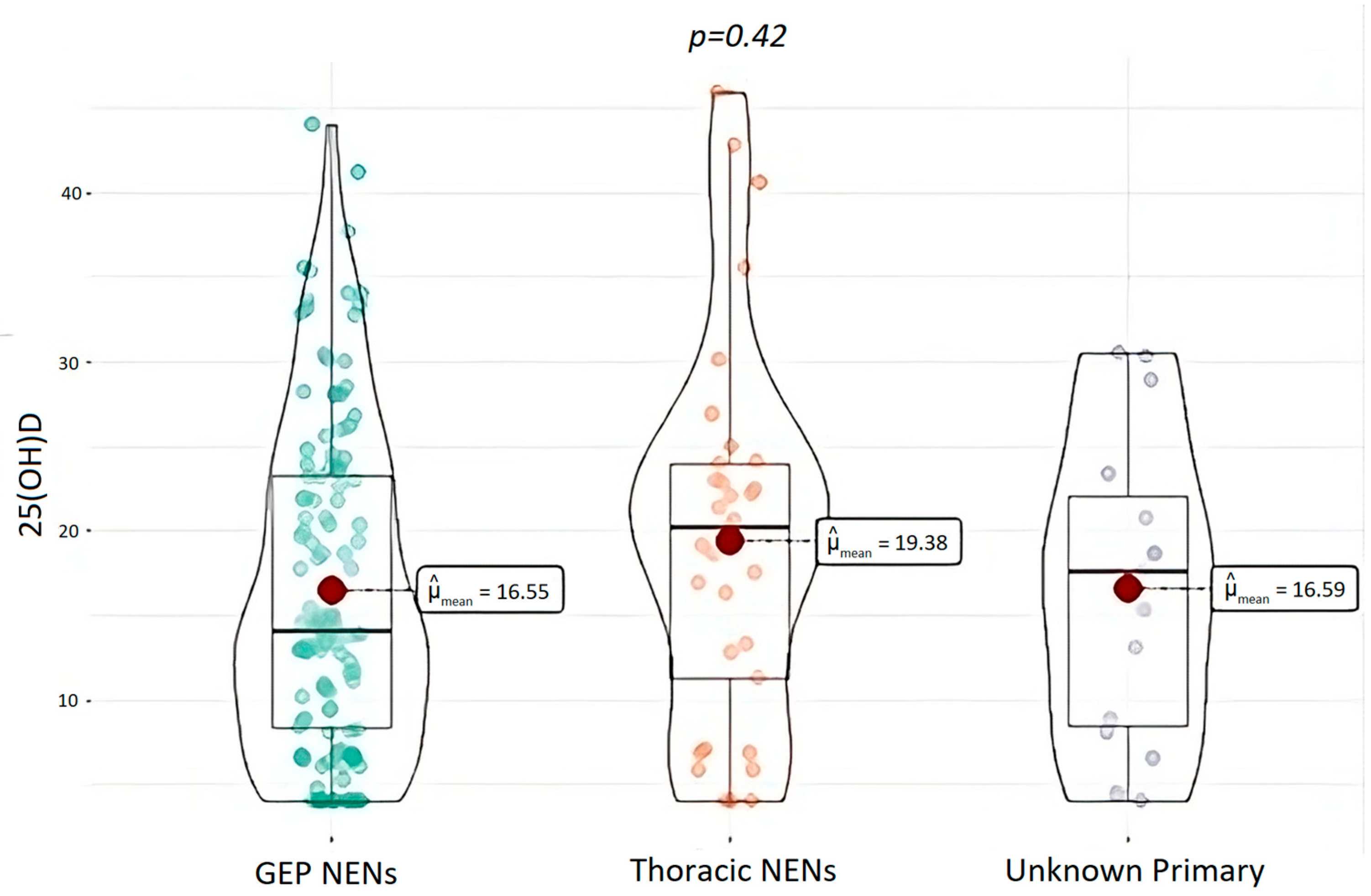
3.2. Levels of 25(OH)D
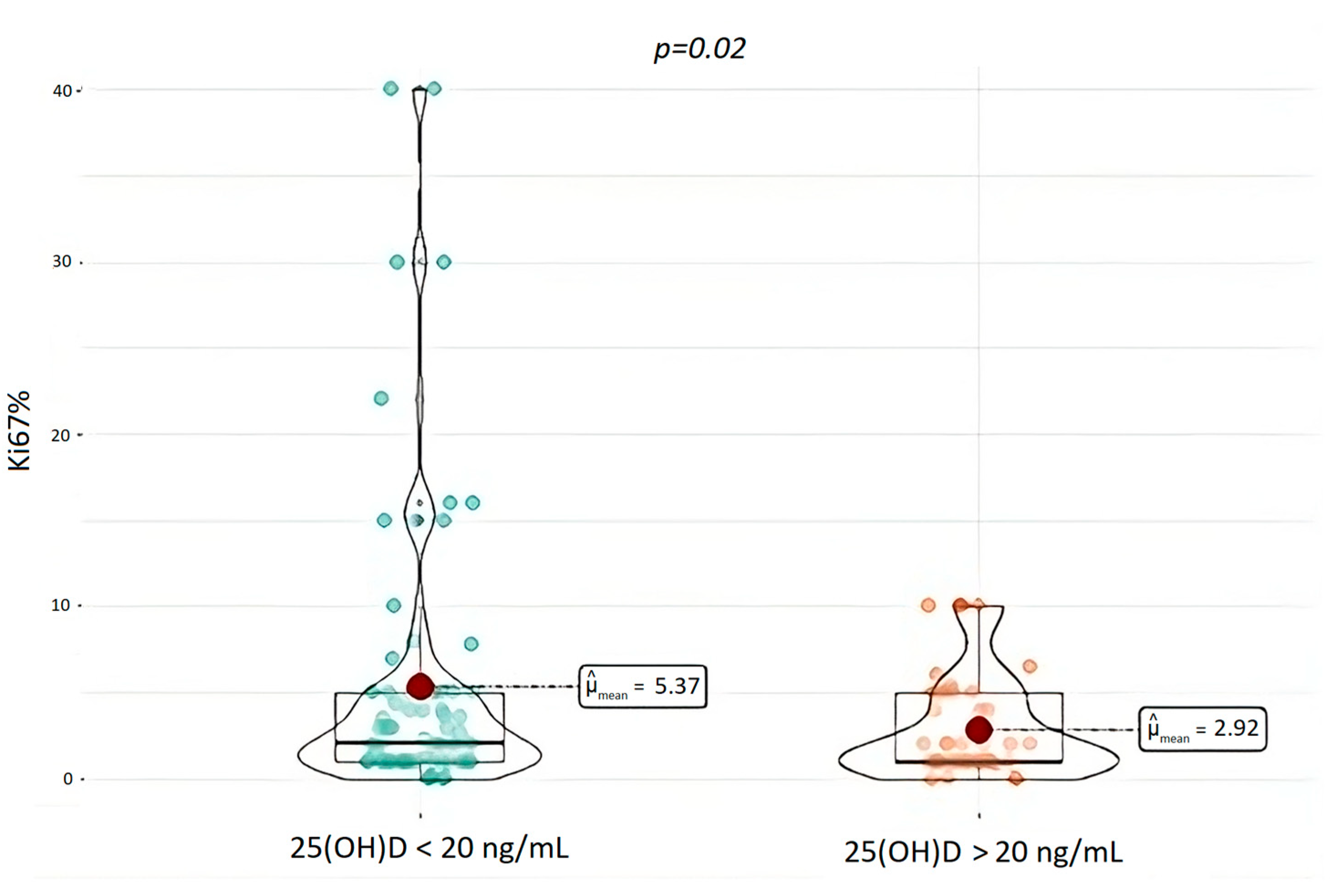
3.3. Tumor Aggressiveness and 25(OH)D Levels
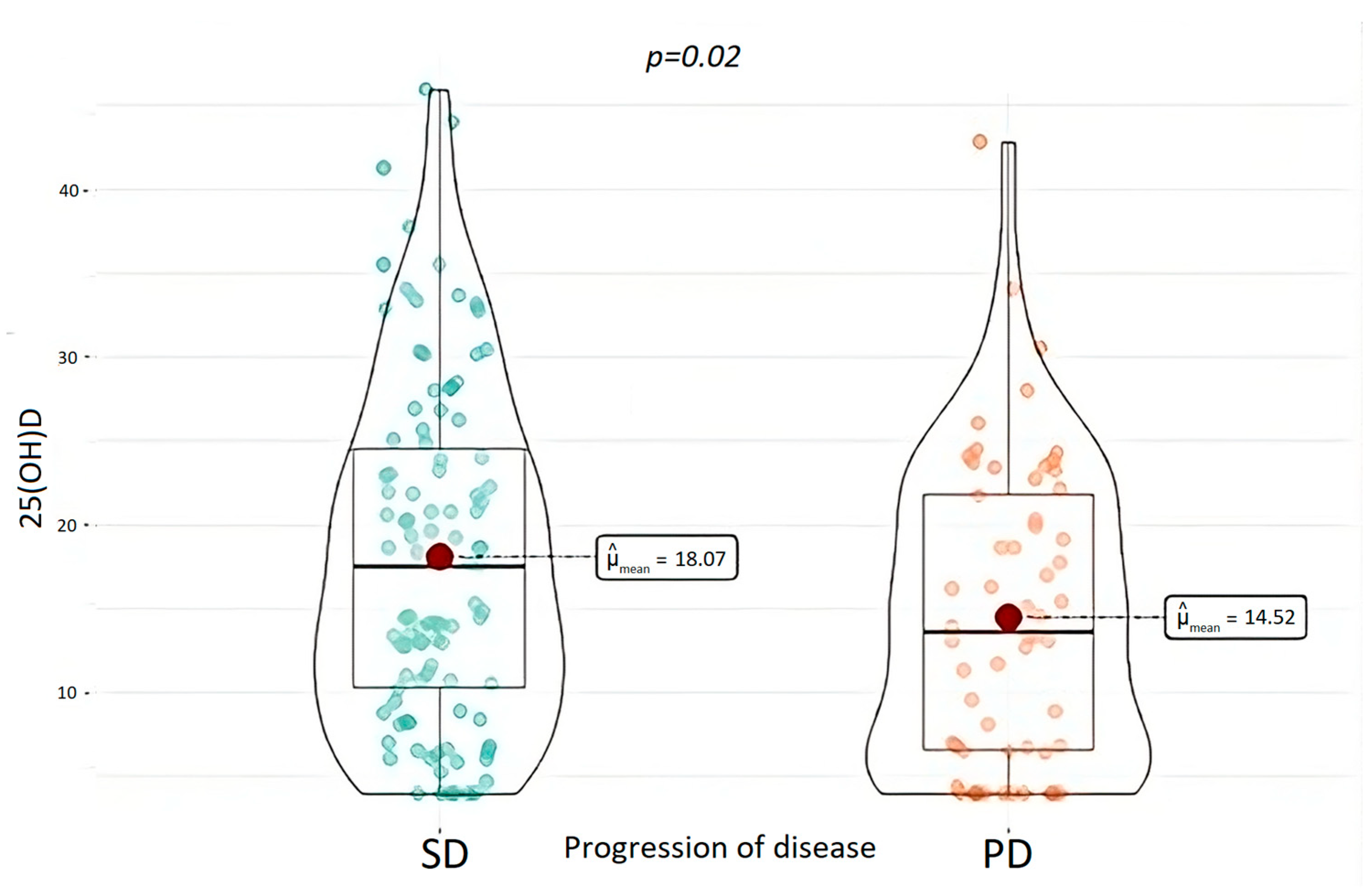
3.4. Clinical Outcomes and 25(OH)D Levels
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Oberndorfer, S. Karzinoide tumoren des Dünndarms. Frankf. Z. Pathol. 1907, 1, 425–432. [Google Scholar]
- Gosset, A.M.P. Tumeurs endocrines de l’appendice. Press. Med. 1914, 25, 237–240. [Google Scholar]
- Rizen, E.N.; Phan, A.T. Neuroendocrine Tumors: A Relevant Clinical Update. Curr. Oncol. Rep. 2022, 24, 703–714. [Google Scholar] [CrossRef]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- WHO Classification of Tumors Editorial Board. WHO Classification of Endocrine and Neuroendocrine Tumours; IARC: Lyon, France, 2022. [Google Scholar]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing but NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef] [PubMed]
- Öberg, K. The Genesis of the Neuroendocrine Tumors Concept: From Oberndorfer to 2018. Endocrinol. Metab. Clin. N. Am. 2018, 47, 711–731. [Google Scholar] [CrossRef] [PubMed]
- Marx, S.J. Molecular genetics of multiple endocrine neoplasia types 1 and 2. Nat. Rev. Cancer 2005, 5, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Donis-keller, H.; Dou, S.; Chi, D.; Carlson, K.M.; Toshima, K.; Lairmore, T.C.; Howe, J.R.; Moley, J.F.; Goodfellow, P.; Wells, S.A., Jr. Mutations in the RET proto-oncogene are associated with MEN 2a and FMTC. Hum. Mol. Genet. 1993, 2, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Varshney, N.; Kebede, A.A.; Owusu-Dapaah, H.; Lather, J.; Kaushik, M.; Bhullar, J.S. A Review of Von Hippel-Lindau Syndrome. J. Kidney Cancer VHL 2017, 4, 20–29. [Google Scholar] [CrossRef]
- Larson, A.M.; Hedgire, S.S.; Deshpande, V.; Stemmer-Rachamimov, A.O.; Harisinghani, M.G.; Ferrone, C.R.; Shah, U.; Thiele, E.A. Pancreatic neuroendocrine tumors in patients with tuberous sclerosis complex. Clin. Genet. 2012, 82, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Ferner, R.E.; Huson, S.M.; Thomas, N.; Moss, C.; Willshaw, H.; Evans, D.G.; Upadhyaya, M.; Towers, R.; Gleeson, M.; Steiger, C.; et al. Guidelines for the diagnosis and management of individuals with neurofibromatosis. J. Med. Genet. 2007, 44, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Pastorino, L.; Grillo, F.; Albertelli, M.; Ghiorzo, P.; Bruno, W. Insights into mechanisms of tumorigenesis in neuroendocrine neoplasms. Int. J. Mol. Sci. 2021, 22, 10328. [Google Scholar] [CrossRef]
- Kaderli, R.M.; Spanjol, M.; Kollár, A.; Bütikofer, L.; Gloy, V.; Dumont, R.A.; Seiler, C.A.; Christ, E.R.; Radojewski, P.; Briel, M.; et al. Therapeutic Options for Neuroendocrine Tumors: A Systematic Review and Network Meta-analysis. JAMA Oncol. 2019, 5, 480–489. [Google Scholar] [CrossRef]
- Marino, R.; Misra, M. Extra-skeletal effects of vitamin D. Nutrients 2019, 11, 1460. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Holick, M.F. Immunologic effects of vitamin d on human health and disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]
- Latic, N.; Erben, R.G. Vitamin D and cardiovascular disease, with emphasis on hypertension, atherosclerosis, and heart failure. Int. J. Mol. Sci. 2020, 21, 6483. [Google Scholar] [CrossRef]
- Grant, W.B. Review of recent advances in understanding the role of Vitamin D in reducing cancer risk: Breast, colorectal, prostate, and overall cancer. Anticancer Res. 2020, 40, 491–499. [Google Scholar] [CrossRef]
- Muñoz, A.; Grant, W.B. Vitamin D and Cancer: An Historical Overview of the Epidemiology and Mechanisms. Nutrients 2022, 14, 1448. [Google Scholar] [CrossRef]
- Cutolo, M.; Paolino, S.; Sulli, A.; Smith, V.; Pizzorni, C.; Seriolo, B. Vitamin D, steroid hormones, and autoimmunity. Ann. N. Y. Acad. Sci. 2014, 1317, 39–46. [Google Scholar] [CrossRef]
- Leyssens, C.; Verlinden, L.; Verstuy, A. Antineoplastic effects of 1,25(OH)2D3 and its analogs in breast, prostate and colorectal cancer. Endocr. Relat. Cancer 2013, 20, R31–R47. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar] [CrossRef] [PubMed]
- Swami, S.; Raghavachari, N.; Muller, U.R.; Bao, Y.P.; Feldman, D. Vitamin D growth inhibition of breast cancer cells: Gene expression patterns assessed by cDNA microarray. Breast Cancer Res. Treat. 2003, 80, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Vasilovici, A.F.; Grigore, L.E.; Ungureanu, L.; Fechete, O.; Candrea, E.; Trifa, A.P.; Vișan, S.; Șenilă, S.; Cosgarea, R. Vitamin D receptor polymorphisms and melanoma (Review). Oncol. Lett. 2019, 17, 4162–4169. [Google Scholar] [CrossRef] [PubMed]
- Oades, G.M.; Dredge, K.; Kirby, R.S.; Colston, K.W. Vitamin D receptor-dependent antitumour effects of 1,25-dihydroxyvitamin D3 and two synthetic analogues in three in vivo models of prostate cancer. BJU Int. 2002, 90, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Erin, L.M.; Zhanga, X.; Flaskb, C.; Duerkb, J.; MacDonald, P.N.; Keri, R.A. EB1089, a vitamin D receptor agonist, reduces proliferation and decreases tumor growth rate in a mouse model of hormone-induced mammary cancer. Cancer Lett. 2005, 229, 205–215. [Google Scholar]
- Keum, N.; Lee, D.H.; Greenwood, D.C.; Manson, J.E.; Giovannucci, E. Vitamin D supplementation and total cancer incidence and mortality: A meta-Analysis of randomized controlled trials. Ann. Oncol. 2019, 30, 733–743. [Google Scholar] [CrossRef]
- Grant, W.B.; Al Anouti, F.; Moukayed, M. Targeted 25-hydroxyvitamin D concentration measurements and vitamin D3 supplementation can have important patient and public health benefits. Eur. J. Clin. Nutr. 2020, 74, 366–376. [Google Scholar] [CrossRef]
- Kopustinskiene, D.M.; Jakstas, V.; Savickas, A.; Bernatoniene, J. Flavonoids as Anticancer Agents. Nutrients 2020, 12, 457. [Google Scholar] [CrossRef]
- Lind, A.; Wängberg, B.; Ellegård, L. Vitamin D and vitamin B12 deficiencies are common in patients with midgut carcinoid (SI-NET). Eur. J. Clin. Nutr. 2016, 70, 990–994. [Google Scholar] [CrossRef]
- Massironi, S.; Zilli, A.; Bernasconi, S.; Fanetti, I.; Cavalcoli, F.; Ciafardini, C.; Felicetta, I.; Conte, D. A role for vitamin D in the Gastro-entero-pancreatic Neuroendocrine Neoplasms outcome: Report on a Series from a Single Institute. Neuroendocrinology 2017, 105, 403–411. [Google Scholar] [CrossRef]
- Barrea, L.; Altieri, B.; Muscogiuri, G.; Laudisio, D.; Annunziata, G.; Colao, A.; Faggiano, A.; Savastano, S. Impact of nutritional status on gastroenteropancreatic neuroendocrine tumors (GEP-NET) aggressiveness. Nutrients 2018, 10, 1854. [Google Scholar] [CrossRef]
- Altieri, B.; Barrea, L.; Modica, R.; Bottiglieri, F.; de Cicco, F.; Muscogiuri, G.; Circelli, L.; Savarese, G.; Di Somma, C.; Savastano, S.; et al. Vitamin D deficiency and tumor aggressiveness in gastroenteropancreatic neuroendocrine tumors. Endocrine 2022, 75, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Altieri, B.; Di Dato, C.; Modica, R.; Bottiglieri, F.; Di Sarno, A.; Pittaway, J.F.H.; Martini, C.; Faggiano, A.; Colao, A. Bone Metabolism and Vitamin D Implication in Gastroenteropancreatic Neuroendocrine Tumors. Nutrients 2020, 12, 1021. [Google Scholar] [CrossRef]
- Motylewska, E.; Gawronska, J.; Niedziela, A.; Melen-Mucha, G.; Lawnicka, H.; Komorowski, J.; Swietoslawski, J.; Stepien, H. Somatostatin Analogs and Tumor Localization Do Not Influence Vitamin D Concentration in Patients with Neuroendocrine Tumors. Nutr. Cancer 2016, 68, 428–434. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.; Cashman, K.; Key, T.; Lanham-New, S.; McArdle, H.; Walsh, S.; Williams, A.; Young, I. Vitamin D and Health 2016; Scientific Advisory Committee on Nutrition: 2016; pp. 56–116. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/537616/SACN_Vitamin_D_and_Health_report.pdf (accessed on 13 July 2023).
- Patil, I. Visualizations with statistical details: The “ggstatsplot” approach. J. Open Source Softw. 2021, 6, 3167. [Google Scholar] [CrossRef]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000. [Google Scholar]
- Meyer, D.; Zeileis, A.; Hornik, K.; Gerber, F. vcd: Visualizing Categorical Data; R Package 1.4-11. 2023. Available online: https://cran.r-project.org/web/packages/vcd/citation.html (accessed on 13 July 2023).
- Aytekin, A. Comparison of Vitamin D Levels between Healthy Individuals and Cancer Patients. Eurasian J. Med. Investig. 2020, 4, 259–264. [Google Scholar] [CrossRef]
- Clement, D.S.V.M.; Tesselaar, M.E.T.; Van Leerdam, M.E.; Srirajaskanthan, R.; Ramage, J.K. Nutritional and vitamin status in patients with neuroendocrine neoplasms. World J. Gastroenterol. 2019, 25, 1171–1184. [Google Scholar] [CrossRef]
- Chowdhury, R.; Kunutsor, S.; Vitezova, A.; Oliver-Williams, C.; Chowdhury, S.; Kiefte-De-Jong, J.C.; Khan, H.; Baena, C.P.; Prabhakaran, D.; Hoshen, M.B.; et al. Vitamin D and risk of cause specific death: Systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ 2014, 348, g1903. [Google Scholar] [CrossRef]
- Giovannucci, E. The epidemiology of vitamin D and cancer incidence and mortality: A review (United States). Cancer Causes Control 2005, 16, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Arayici, M.E.; Basbinar, Y.; Ellidokuz, H. Vitamin D Intake, Serum 25-Hydroxyvitamin-D (25(OH)D) Levels, and Cancer Risk: A Comprehensive Meta-Meta-Analysis Including Meta-Analyses of Randomized Controlled Trials and Observational Epidemiological Studies. Nutrients 2023, 15, 2722. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Alonso, P.; Boughanem, H.; Canudas, S.; Becerra-Tomás, N.; Fernández de la Puente, M.; Babio, N.; Macias-Gonzalez, M.; Salas-Salvadó, J. Circulating vitamin D levels and colorectal cancer risk: A meta-analysis and systematic review of case-control and prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2023, 63, 1–17. [Google Scholar] [CrossRef]
- Lopez-Caleya, J.F.; Ortega-Valín, L.; Fernández-Villa, T.; Delgado-Rodríguez, M.; Martín-Sánchez, V.; Molina, A.J. The role of calcium and vitamin D dietary intake on risk of colorectal cancer: Systematic review and meta-analysis of case–control studies. Cancer Causes Control 2022, 33, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Olumi, A.F. Commentary on “Randomized clinical trial of vitamin D3 doses on prostatic vitamin D metabolite levels and Ki67 labeling in prostate cancer patients.” Wagner D, Trudel D, Van der Kwast T, Nonn L, Giangreco AA, Li D, Dias A, Cardoza M, Laszlo S, Hersey K, Klotz L, Finelli A, Fleshner N, Vieth R, Department of Nutritional Sciences, University of Toronto, Ontario, Canada.: J. Clin. Endocrinol. Metab. 2013;98(4):1498–507 [Epub 2013 Mar 5]. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 210. [Google Scholar] [CrossRef]
- Shirazi, L.; Almquist, M.; Borgquist, S.; Malm, J.; Manjer, J. Serum vitamin D (25OHD3) levels and the risk of different subtypes of breast cancer: A nested case-control study. Breast 2016, 28, 184–190. [Google Scholar] [CrossRef]
- Wagner, D.; Trudel, D.; Van Der Kwast, T.; Nonn, L.; Giangreco, A.A.; Li, D.; Dias, A.; Cardoza, M.; Laszlo, S.; Hersey, K.; et al. Randomized clinical trial of Vitamin D3 doses on prostatic Vitamin D metabolite levels and Ki67 labeling in prostate cancer patients. J. Clin. Endocrinol. Metab. 2013, 98, 1498–1507. [Google Scholar] [CrossRef]
- WHO Classification of Tumors Editorial Board. WHO Classification of Thoracic Tumours; IARC: Lyon, France, 2021. [Google Scholar]
- Ingraham, B.A.; Bragdon, B.; Nohe, A. Molecular basis of the potential of vitamin D to prevent cancer. Curr. Med. Res. Opin. 2008, 24, 139–149. [Google Scholar] [CrossRef]
- Pálmer, H.G.; González-Sancho, J.M.; Espada, J.; Berciano, M.T.; Puig, I.; Baulida, J.; Quintanilla, M.; Cano, A.; de Herreros, A.G.; Lafarga, M.; et al. Vitamin D3 promotes the differentiation of colon carcinoma cells by the induction of E-cadherin and the inhibition of β-catenin signaling. J. Cell Biol. 2001, 154, 369–387. [Google Scholar] [CrossRef]
- Shah, S.; Hecht, A.; Pestell, R.; Byers, S.W. Trans-repression of β-Catenin Activity by Nuclear Receptors. J. Biol. Chem. 2003, 278, 48137–48145. [Google Scholar] [CrossRef]
- Shah, S.; Islam, M.N.; Dakshanamurthy, S.; Rizvi, I.; Rao, M.; Herrell, R.; Zinser, G.; Valrance, M.; Aranda, A.; Moras, D.; et al. The molecular basis of vitamin D receptor and β-catenin crossregulation. Mol. Cell 2006, 21, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D. Nonclassic actions of vitamin D. J. Clin. Endocrinol. Metab. 2009, 94, 26–34. [Google Scholar] [CrossRef]
- Eisman, J.A.; Macintyre, I.; Martin, T.J.; Moseley, J.M.; Brooks, S. 1,25-dihydroxyvitamin-d receptor in breast cancer cells View all citing articles on Scopus. Lancet 1979, 314, 1335–1336. [Google Scholar] [CrossRef] [PubMed]
- Cannell, J.J.; Vieth, R.; Umhau, J.C.; Holick, M.F.; Grant, W.B.; Madronich, S.; Garland, C.F.; Giovannucci, E. Epidemic influenza and vitamin D. Epidemiol. Infect. 2006, 134, 1129–1140. [Google Scholar] [CrossRef]
- Sly, L.M.; Lopez, M.; Nauseef, W.M.; Reiner, N.E. 1α,25-Dihydroxyvitamin D3-induced Monocyte Antimycobacterial Activity is Regulated by Phosphatidylinositol 3-Kinase and Mediated by the NADPH-dependent Phagocyte Oxidase. J. Biol. Chem. 2001, 276, 35482–35493. [Google Scholar] [CrossRef]
- Cutolo, M.; Straub, R.H. Insights into endocrine-immunological disturbances in autoimmunity and their impact on treatment. Arthritis Res. Ther. 2009, 11, 218. [Google Scholar] [CrossRef]
- Yu, S.; Cantorna, M.T. The vitamin D receptor is required for iNKT cell development. Proc. Natl. Acad. Sci. USA 2008, 105, 5207–5212. [Google Scholar] [CrossRef] [PubMed]
- White, B.E.; Rous, B.; Chandrakumaran, K.; Wong, K.; Bouvier, C.; Van Hemelrijck, M.; George, G.; Russell, B.; Srirajaskanthan, R.; Ramage, J.K. Incidence and survival of neuroendocrine neoplasia in England 1995–2018: A retrospective, population-based study. Lancet Reg. Health Eur. 2022, 23, 100510. [Google Scholar] [CrossRef] [PubMed]
- Robbins, H.L.; Symington, M.; Mosterman, B.; Goodby, J.; Davies, L.; Dimitriadis, G.K.; Kaltsas, G.; Randeva, H.S.; Weickert, M.O. Supplementation of Vitamin D Deficiency in Patients with Neuroendocrine Tumors Using over-the-Counter Vitamin D3 Preparations. Nutr. Cancer 2018, 70, 748–754. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Features | N | % | |||
|---|---|---|---|---|---|
| 172 | 100 | ||||
| Sex | |||||
| Male | 73 | 58 | |||
| Female | 99 | 42 | |||
| Primary Tumor Localization | |||||
| GEP-NEN | Pancreas | 58 | 33.7 | ||
| Ileum | 41 | 23.8 | |||
| Stomach | 12 | 7.0 | |||
| Appendix | 8 | 4.7 | |||
| Colon | 5 | 2.9 | |||
| Total | 124 | 72.1 | |||
| TORACIC-NEN | Lung | 30 | 17.4 | ||
| Thymus | 3 | 1.7 | |||
| Total | 33 | 19.2 | |||
| UNKNOWN | 15 | 8.7 | |||
| Clinical-Pathological Features | |||||
| FUNCTIONING | NF | 113 | 65.7 | ||
| F | 50 | 29.1 | |||
| SYNDROME | NS | 113 | 65.7 | ||
| S | 50 | 29.1 | |||
| METASTASIS | NM | 94 | 54.7 | ||
| M | 76 | 44.2 | |||
| GRADING | G1 | 69 | 40.1 | ||
| G2 | 42 | 24.4 | |||
| G3 | 2 | 1.2 | |||
| Total | 113 | ||||
| Clinical Outcome | |||||
| PROGRESSION | NP | 106 | 61.6 | ||
| P | 53 | 30.8 | |||
| EXITUS | NE | 154 | 89.5 | ||
| E | 18 | 10.5 | |||
| 25(OH)D Levels | |||||
| DEFICIENCY | <20 | 107 | 62.2 | ||
| INSUFFICIENCY | 20-30 | 43 | 25.0 | ||
| DEFICIT | Total | 150 | 87.2 | ||
| SUFFICIENCY | >30 | 22 | 12.8 |
| Mean | Median | Min | Max | P25 | P75 | SE | |
|---|---|---|---|---|---|---|---|
| BMI | 24.304 | 24.300 | 16.400 | 34.100 | 21.000 | 27.175 | 0.321 |
| Age | 59.692 | 62.500 | 13.000 | 89.000 | 70.000 | 70.000 | 1.103 |
| Ki67% | 5.111 | 2.000 | 0.010 | 90.000 | 1.000 | 5.000 | 0.903 |
| PFS (months) | 40.545 | 29.000 | 1.000 | 264.000 | 13.000 | 52.000 | 3.189 |
| OS (months) | 58.351 | 47.000 | 1.000 | 372.000 | 22.000 | 77.000 | 4.110 |
| Follow-up (months) | 52.628 | 37.500 | 1.000 | 372.000 | 17.750 | 73.000 | 4.021 |
| 25(OH)D | 17.099 | 15.050 | 4.000 | 45.900 | 8.375 | 23.425 | 0.757 |
| PTH (ng/L) | 39.459 | 33.000 | 5.700 | 347.000 | 23.000 | 46.250 | 2.721 |
| Calcium (mg/dL) | 9.538 | 9.500 | 7.700 | 11.400 | 9.200 | 9.900 | 0.043 |
| Phosphorus (mg/dL) | 3.085 | 3.100 | 1.600 | 8.900 | 2.675 | 3.400 | 0.064 |
| Creatinine (mg/dL) | 0.945 | 0.900 | 0.500 | 8.000 | 0.700 | 1.000 | 0.050 |
| Size (mm) | 20.485 | 15.000 | 1.000 | 140.000 | 10.000 | 25.000 | 1.684 |
| Number of lesions | 0.405 | 0.000 | 0.000 | 1.000 | 0.000 | 1.000 | 0.390 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | IC95% | p | HR | IC95% | p | |
| Male sex | 1.74 | 0.98–3.1 | 0.058 | Ns | ||
| Multiple lesions | 1.1 | 0.65–2.26 | 0.537 | |||
| Ki67 | 1.03 | 1.02–1.05 | <0.001 | 1.034 | 1.017–1.050 | 0.006 |
| Age | 1.02 | 1.004–1.045 | 0.022 | Ns | ||
| Functioning tumor | 0.97 | 0.54–1.73 | 0.919 | |||
| 25(OH)D < 20 ng/mL | 1.39 | 0.49–3.91 | 0.53 | |||
| 25(OH)D levels | 0.96 | 0.934–0.993 | 0.016 | Ns | ||
| PTH | 1.01 | 1.00–1.02 | 0.056 | Ns | ||
| Calcium | 1.02 | 1.002–1.036 | 0.029 | Ns | ||
| IV stadium | 4.23 | 2.33–7.65 | <0.001 | 4.72 | 2.04–10.91 | <0.001 |
| 25(OH)D supplementation | 0.63 | 0.36–1.10 | 0.103 | Ns | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albertelli, M.; Petolicchio, C.; Brasili, S.; Pogna, A.; Boschetti, M.; Luciano, G.; Campana, D.; Gay, S.; Veresani, A.; Ferone, D.; et al. Impact of Vitamin D Deficiency on Tumor Aggressiveness in Neuroendocrine Neoplasms. Nutrients 2023, 15, 3771. https://doi.org/10.3390/nu15173771
Albertelli M, Petolicchio C, Brasili S, Pogna A, Boschetti M, Luciano G, Campana D, Gay S, Veresani A, Ferone D, et al. Impact of Vitamin D Deficiency on Tumor Aggressiveness in Neuroendocrine Neoplasms. Nutrients. 2023; 15(17):3771. https://doi.org/10.3390/nu15173771
Chicago/Turabian StyleAlbertelli, Manuela, Cristian Petolicchio, Sara Brasili, Andrea Pogna, Mara Boschetti, Giorgio Luciano, Davide Campana, Stefano Gay, Alessandro Veresani, Diego Ferone, and et al. 2023. "Impact of Vitamin D Deficiency on Tumor Aggressiveness in Neuroendocrine Neoplasms" Nutrients 15, no. 17: 3771. https://doi.org/10.3390/nu15173771
APA StyleAlbertelli, M., Petolicchio, C., Brasili, S., Pogna, A., Boschetti, M., Luciano, G., Campana, D., Gay, S., Veresani, A., Ferone, D., & Vera, L. (2023). Impact of Vitamin D Deficiency on Tumor Aggressiveness in Neuroendocrine Neoplasms. Nutrients, 15(17), 3771. https://doi.org/10.3390/nu15173771