
Identification of the Most Suitable Mobile Apps to Support Dietary Approaches to Stop Hypertension (DASH) Diet Self-Management: Systematic Search of App Stores and Content Analysis

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. App Identification and Selection
2.2. Data Extraction
2.3. In-Depth Analysis
2.3.1. Likelihood of Effectiveness of the DASH Diet App and Theoretical Underpinnings
2.3.2. General App Quality
2.3.3. Privacy and Security
2.4. Statistical Analysis
3. Results
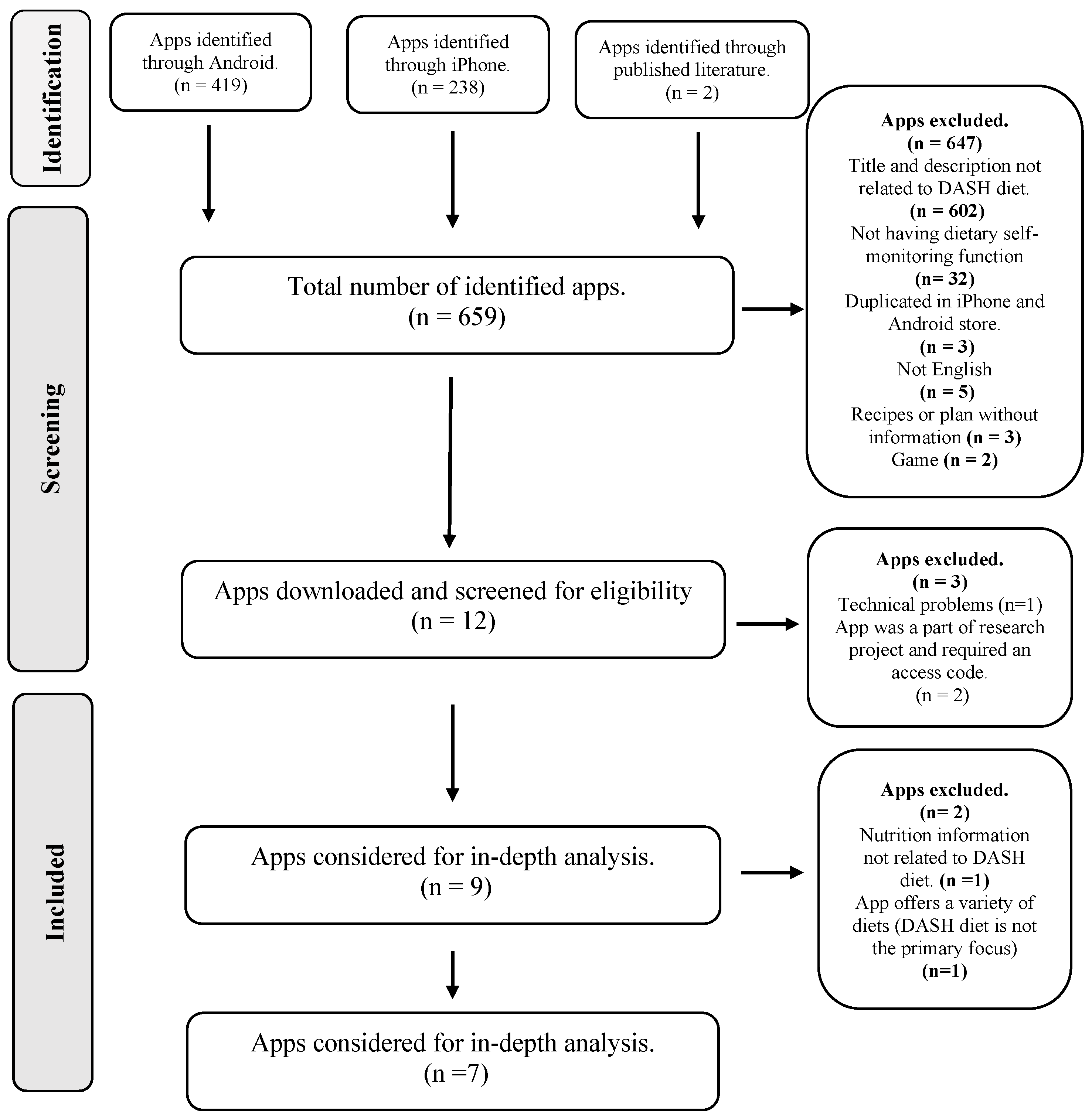
3.1. Identification of DASH Diet Self-Management Apps in the Published Literature and App Stores
3.2. Characteristics of the Selected Apps
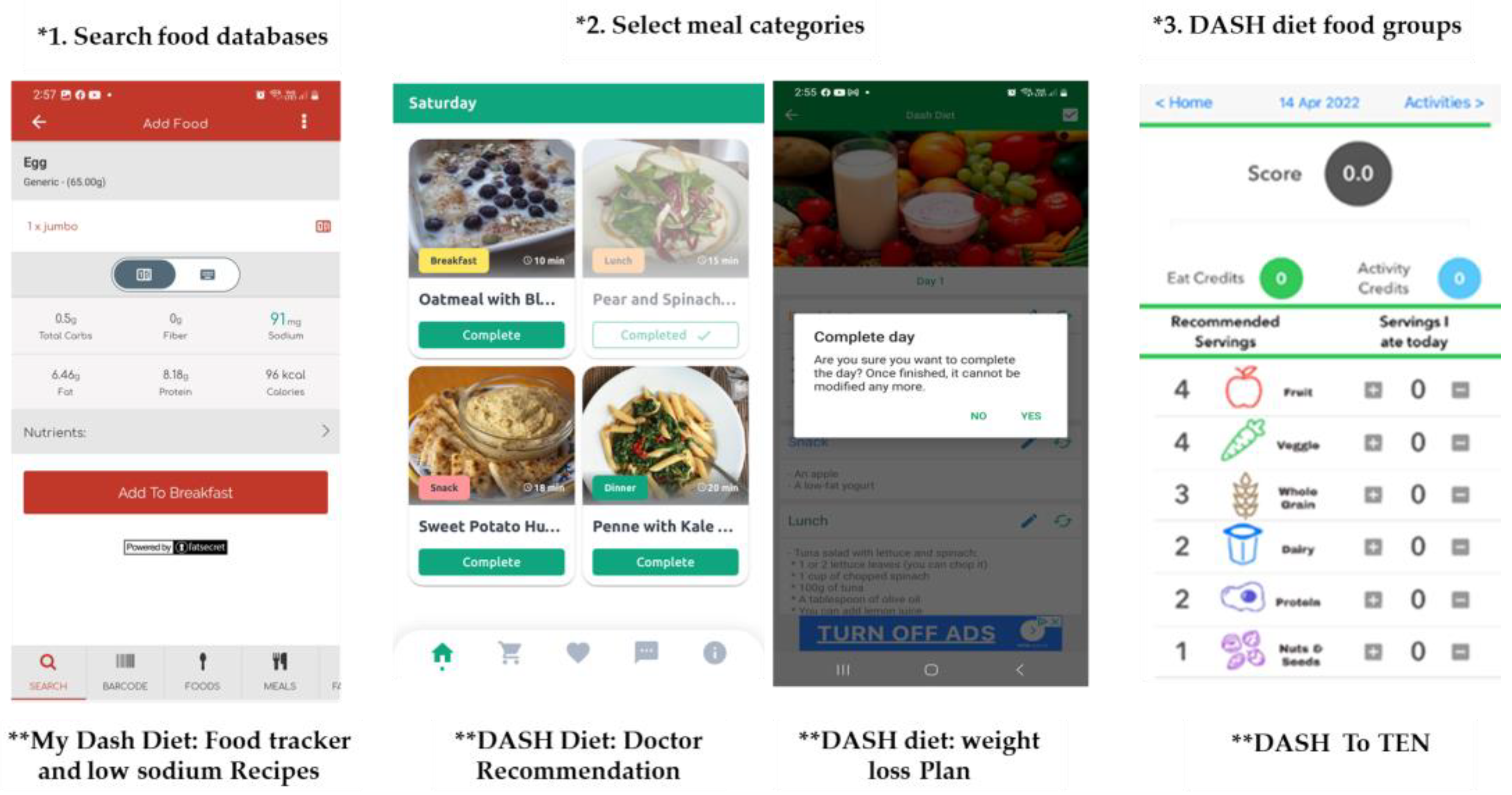
3.3. The Nutritional and General App Functionalities
3.4. Behaviour Change Techniques and Theoretical Domain Framework
3.4.1. The Presence of Behaviour Change Techniques
3.4.2. Mechanisms of Action of the Theoretical Domain Framework
3.5. General App Quality
3.6. Data Privacy and Security
3.6.1. Availability and Accessibility of Privacy Policy
3.6.2. Data Gathering and Sharing
3.6.3. Data Security
3.7. Selection Process
4. Discussion
4.1. Principal Findings
4.2. App Functionalities
4.3. Likelihood of Effectiveness and Theoretical Underpinnings of the DASH Diet Apps
4.4. General App Quality
4.5. Data Privacy and Security
4.6. Strengths and Limitations
4.7. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Hypertension. Available online: https://www.who.int/health-topics/hypertension#tab=tab_1 (accessed on 18 February 2023).
- Mule, G.; Castiglia, A.; Cusumano, C.; Scaduto, E.; Geraci, G.; Altieri, D.; Natale, E.D.; Cacciatore, O.; Cerasola, G.; Cottone, S. Subclinical kidney damage in hypertensive patients: A renal window opened on the cardiovascular system. Focus on microalbuminuria. Hypertens. Basic Res. Clin. Pract. 2016, 956, 279–306. [Google Scholar]
- Alessa, T.; Abdi, S.; Hawley, M.S.; de Witte, L. Mobile apps to support the self-management of hypertension: Systematic review of effectiveness, usability, and user satisfaction. JMIR mHealth uHealth 2018, 6, e10723. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; Green, T.; Harrison, T.N.; Reynolds, K. Dietary approaches to prevent hypertension. Curr. Hypertens. Rep. 2013, 15, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Savica, V.; Bellinghieri, G.; Kopple, J.D. The effect of nutrition on blood pressure. Annu. Rev. Nutr. 2010, 30, 365–401. [Google Scholar] [CrossRef] [PubMed]
- Karanja, N.M.; Obarzanek, E.; Lin, P.-H.; McCullough, M.L.; Phillips, K.M.; Swain, J.F.; Champagne, C.M.; Hoben, K.P.; DASH Collaborative Research Group. Descriptive characteristics of the dietary patterns used in the Dietary Approaches to Stop Hypertension trial. J. Am. Diet. Assoc. 1999, 99, S19–S27. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M. A clinical trial of the effects of dietary patterns on blood pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Viguiliouk, E.; Nishi, S.K.; Blanco Mejia, S.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Kendall, C.W.; Sievenpiper, J.L. DASH dietary pattern and cardiometabolic outcomes: An umbrella review of systematic reviews and meta-analyses. Nutrients 2019, 11, 338. [Google Scholar] [CrossRef]
- Epstein, D.E.; Sherwood, A.; Smith, P.J.; Craighead, L.; Caccia, C.; Lin, P.-H.; Babyak, M.A.; Johnson, J.J.; Hinderliter, A.; Blumenthal, J.A. Determinants and consequences of adherence to the dietary approaches to stop hypertension diet in African-American and white adults with high blood pressure: Results from the ENCORE trial. J. Acad. Nutr. Diet. 2012, 112, 1763–1773. [Google Scholar] [CrossRef]
- Chow, C.K.; Teo, K.K.; Rangarajan, S.; Islam, S.; Gupta, R.; Avezum, A.; Bahonar, A.; Chifamba, J.; Dagenais, G.; Diaz, R. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 2013, 310, 959–968. [Google Scholar] [CrossRef]
- Shahaj, O.; Denneny, D.; Schwappach, A.; Pearce, G.; Epiphaniou, E.; Parke, H.L.; Taylor, S.J.; Pinnock, H. Supporting self-management for people with hypertension: A meta-review of quantitative and qualitative systematic reviews. J. Hypertens. 2019, 37, 264–279. [Google Scholar] [CrossRef]
- Rusin, M.; Årsand, E.; Hartvigsen, G. Functionalities and input methods for recording food intake: A systematic review. Int. J. Med. Inform. 2013, 82, 653–664. [Google Scholar] [CrossRef]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The impact of mHealth interventions: Systematic review of systematic reviews. JMIR mHealth uHealth 2018, 6, e8873. [Google Scholar] [CrossRef]
- Logan, A.G. Transforming hypertension management using mobile health technology for telemonitoring and self-care support. Can. J. Cardiol. 2013, 29, 579–585. [Google Scholar] [CrossRef]
- Mitrea, T.; Borda, M. Mobile security threats: A survey on protection and mitigation strategies. In Proceedings of the International Conference Knowledge-Based Organization, Sibiu, Romania, 11–13 June 2020; pp. 131–135. [Google Scholar]
- Rivera, J.; McPherson, A.; Hamilton, J.; Birken, C.; Coons, M.; Iyer, S.; Agarwal, A.; Lalloo, C.; Stinson, J. Mobile apps for weight management: A scoping review. JMIR mHealth uHealth 2016, 4, e5115. [Google Scholar] [CrossRef]
- McCool, J.; Dobson, R.; Whittaker, R.; Paton, C. Mobile health (mHealth) in low-and middle-income countries. Annu. Rev. Public Health 2022, 43, 525–539. [Google Scholar] [CrossRef]
- El Khoury, C.F.; Karavetian, M.; Halfens, R.J.; Crutzen, R.; Khoja, L.; Schols, J.M. The effects of dietary mobile apps on nutritional outcomes in adults with chronic diseases: A systematic review and meta-analysis. J. Acad. Nutr. Diet. 2019, 119, 626–651. [Google Scholar] [CrossRef]
- Teasdale, N.; Elhussein, A.; Butcher, F.; Piernas, C.; Cowburn, G.; Hartmann-Boyce, J.; Saksena, R.; Scarborough, P. Systematic review and meta-analysis of remotely delivered interventions using self-monitoring or tailored feedback to change dietary behavior. Am. J. Clin. Nutr. 2018, 107, 247–256. [Google Scholar] [CrossRef]
- Chen, J.; Gemming, L.; Hanning, R.; Allman-Farinelli, M. Smartphone apps and the nutrition care process: Current perspectives and future considerations. Patient Educ. Couns. 2018, 101, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, E.M.; Levy, P.D. New approaches to evaluating and monitoring blood pressure. Curr. Hypertens. Rep. 2016, 18, 49. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Khunger, M.; Gupta, A.; Garg, N. A content analysis of smartphone–based applications for hypertension management. J. Am. Soc. Hypertens. 2015, 9, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Alessa, T.; Hawley, M.S.; Hock, E.S.; de Witte, L. Smartphone apps to support self-management of hypertension: Review and content analysis. JMIR mHealth uHealth 2019, 7, e13645. [Google Scholar] [CrossRef]
- Alnooh, G.; Alessa, T.; Hawley, M.; de Witte, L. The Use of Dietary Approaches to Stop Hypertension (DASH) Mobile Apps for Supporting a Healthy Diet and Controlling Hypertension in Adults: Systematic Review. JMIR Cardio 2022, 6, e35876. [Google Scholar] [CrossRef]
- Al-Washali, A.Y.A.; Kadri, H.; Ismail, S.; Rahman, H.A.; Elezzy, Y.A. Systematic review on effectiveness of theory-based intervention on self-care behaviors among patients with type 2 diabetes. Clin. Trials Degener. Dis. 2018, 3, 88. [Google Scholar] [CrossRef]
- Lepard, M.G.; Joseph, A.L.; Agne, A.A.; Cherrington, A.L. Diabetes self-management interventions for adults with type 2 diabetes living in rural areas: A systematic literature review. Curr. Diabetes Rep. 2015, 15, 608. [Google Scholar] [CrossRef] [PubMed]
- Bondaronek, P.; Alkhaldi, G.; Slee, A.; Hamilton, F.L.; Murray, E. Quality of publicly available physical activity apps: Review and content analysis. JMIR mHealth uHealth 2018, 6, e9069. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.A.; Lumsden, J.; Rivas, C.; Steed, L.; Edwards, L.; Thiyagarajan, A.; Sohanpal, R.; Caton, H.; Griffiths, C.; Munafò, M. Gamification for health promotion: Systematic review of behaviour change techniques in smartphone apps. BMJ Open 2016, 6, e012447. [Google Scholar] [CrossRef]
- Steinmo, S.; Fuller, C.; Stone, S.P.; Michie, S. Characterising an implementation intervention in terms of behaviour change techniques and theory: The ‘Sepsis Six’clinical care bundle. Implement. Sci. 2015, 10, 11. [Google Scholar] [CrossRef]
- DiFilippo, K.N.; Huang, W.-H.D.; Chapman-Novakofski, K.M. Mobile apps for the dietary approaches to stop hypertension (DASH): App quality evaluation. J. Nutr. Educ. Behav. 2018, 50, 620–625. [Google Scholar] [CrossRef]
- Huckvale, K.; Prieto, J.T.; Tilney, M.; Benghozi, P.-J.; Car, J. Unaddressed privacy risks in accredited health and wellness apps: A cross-sectional systematic assessment. BMC Med. 2015, 13, 214. [Google Scholar] [CrossRef]
- Karthick, S.; Binu, S. Android security issues and solutions. In Proceedings of the 2017 International Conference on Innovative Mechanisms for Industry Applications (ICIMIA), Bengaluru, India, 21–23 February 2017; pp. 686–689. [Google Scholar]
- Choi, J.; Chung, C.; Woo, H. Diet-related mobile apps to promote healthy eating and proper nutrition: A content analysis and quality assessment. Int. J. Environ. Res. Public Health 2021, 18, 3496. [Google Scholar] [CrossRef]
- Zečević, M.; Mijatović, D.; Koklič, M.K.; Žabkar, V.; Gidaković, P. User perspectives of diet-tracking apps: Reviews content analysis and topic modeling. J. Med. Internet Res. 2021, 23, e25160. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile app rating scale: A new tool for assessing the quality of health mobile apps. JMIR mHealth uHealth 2015, 3, e3422. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; Richardson, M.; Johnston, M.; Ladha, R.; Michie, S. From lists of behaviour change techniques (BCT s) to structured hierarchies: Comparison of two methods of developing a hierarchy of BCT s. Br. J. Health Psychol. 2015, 20, 130–150. [Google Scholar] [CrossRef]
- DiFilippo, K.N.; Huang, W.; Chapman-Novakofski, K.M. A new tool for nutrition app quality evaluation (AQEL): Development, validation, and reliability testing. JMIR mHealth uHealth 2017, 5, e7441. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Lee, J.; Mouhaffel, R.; L’Abbe, M. A Content Analysis of Free, Popular Low FODMAPs Diet mHealth Apps. Curr. Dev. Nutr. 2021, 5, 998. [Google Scholar] [CrossRef]
- Lee, J.; Ahmed, M.; Mouhaffel, R.; L’Abbe, M. A Content Analysis of Free, Popular Plant-Based Mobile Health Apps. Curr. Dev. Nutr. 2021, 5, 1003. [Google Scholar] [CrossRef]
- Online Trust Alliance. Mobile App Privacy & Security. Available online: https://otalliance.org/best-practices/mobile-app-privacy-security (accessed on 12 February 2023).
- Information Comissioner’s Privacy in Mobile Apps. Available online: https://ico.org.uk/media/for-organisations/documents/1596/privacy-in-mobile-apps-dp-guidance.pdf (accessed on 12 February 2023).
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Medica 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Frinzi, A. DASH Diet Food List. Available online: https://www.noom.com/blog/dash-diet-food-list/ (accessed on 24 November 2022).
- Toro-Ramos, T.; Kim, Y.; Wood, M.; Rajda, J.; Niejadlik, K.; Honcz, J.; Marrero, D.; Fawer, A.; Michaelides, A. Efficacy of a mobile hypertension prevention delivery platform with human coaching. J. Hum. Hypertens. 2017, 31, 795–800. [Google Scholar] [CrossRef]
- Akbar, S.; Coiera, E.; Magrabi, F. Safety concerns with consumer-facing mobile health applications and their consequences: A scoping review. J. Am. Med. Inform. Assoc. 2020, 27, 330–340. [Google Scholar] [CrossRef]
- Alessa, T.; Hawley, M.; de Witte, L. Identification of the Most Suitable App to Support the Self-Management of Hypertension: Systematic Selection Approach and Qualitative Study. JMIR mHealth uHealth 2021, 9, e29207. [Google Scholar] [CrossRef] [PubMed]
- Bardus, M.; van Beurden, S.B.; Smith, J.R.; Abraham, C. A review and content analysis of engagement, functionality, aesthetics, information quality, and change techniques in the most popular commercial apps for weight management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- DiFilippo, K.N.; Huang, W.-H.; Andrade, J.E.; Chapman-Novakofski, K.M. The use of mobile apps to improve nutrition outcomes: A systematic literature review. J. Telemed. Telecare 2015, 21, 243–253. [Google Scholar] [CrossRef]
- Bell, L.; Garnett, C.; Bao, Y.; Cheng, Z.; Qian, T.; Perski, O.; Potts, H.W.; Williamson, E. How Notifications Affect Engagement With a Behavior Change App: Results From a Micro-Randomized Trial. JMIR mHealth uHealth 2023, 11, e38342. [Google Scholar] [CrossRef]
- Franco, R.Z.; Fallaize, R.; Lovegrove, J.A.; Hwang, F. Popular nutrition-related mobile apps: A feature assessment. JMIR mHealth uHealth 2016, 4, e5846. [Google Scholar] [CrossRef] [PubMed]
- Tyson, C.C.; Svetkey, L.P.; Lin, P.-H.; Granados, I.; Kennedy, D.; Dunbar, K.T.; Redd, C.; Bennett, G.; Boulware, L.E.; Fish, L.J. Self-Perceived Barriers and Facilitators to Dietary Approaches to Stop Hypertension Diet Adherence Among Black Americans With Chronic Kidney Disease: A Qualitative Study. J. Ren. Nutr. 2023, 33, 59–68. [Google Scholar] [CrossRef]
- König, L.M.; Attig, C.; Franke, T.; Renner, B. Barriers to and facilitators for using nutrition apps: Systematic review and conceptual framework. JMIR mHealth uHealth 2021, 9, e20037. [Google Scholar] [CrossRef]
- Direito, A.; Pfaeffli Dale, L.; Shields, E.; Dobson, R.; Whittaker, R.; Maddison, R. Do physical activity and dietary smartphone applications incorporate evidence-based behaviour change techniques? BMC Public Health 2014, 14, 646. [Google Scholar] [CrossRef] [PubMed]
- Middelweerd, A.; Mollee, J.S.; van der Wal, C.N.; Brug, J.; Te Velde, S.J. Apps to promote physical activity among adults: A review and content analysis. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 97. [Google Scholar] [CrossRef]
- Villinger, K.; Wahl, D.R.; Boeing, H.; Schupp, H.T.; Renner, B. The effectiveness of app-based mobile interventions on nutrition behaviours and nutrition-related health outcomes: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1465–1484. [Google Scholar] [CrossRef] [PubMed]
- Pearson, E.S. Goal setting as a health behavior change strategy in overweight and obese adults: A systematic literature review examining intervention components. Patient Educ. Couns. 2012, 87, 32–42. [Google Scholar] [CrossRef]
- Lieffers, J.R.; Arocha, J.F.; Grindrod, K.; Hanning, R.M. Experiences and perceptions of adults accessing publicly available nutrition behavior-change mobile apps for weight management. J. Acad. Nutr. Diet. 2018, 118, 229–239.e223. [Google Scholar] [CrossRef]
- Webb, T.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010, 12, e1376. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690. [Google Scholar] [CrossRef]
- Van Genugten, L.; Dusseldorp, E.; Webb, T.L.; Van Empelen, P. Which combinations of techniques and modes of delivery in internet-based interventions effectively change health behavior? A meta-analysis. J. Med. Internet Res. 2016, 18, e4218. [Google Scholar] [CrossRef]
- Glanz, K.; Bishop, D.B. The role of behavioral science theory in development and implementation of public health interventions. Annu. Rev. Public Health 2010, 31, 399–418. [Google Scholar] [CrossRef]
- Ferrara, G.; Kim, J.; Lin, S.; Hua, J.; Seto, E. A focused review of smartphone diet-tracking apps: Usability, functionality, coherence with behavior change theory, and comparative validity of nutrient intake and energy estimates. JMIR mHealth uHealth 2019, 7, e9232. [Google Scholar] [CrossRef]
- Thomas, S.; Mackintosh, S. Use of the theoretical domains framework to develop an intervention to improve physical therapist management of the risk of falls after discharge. Phys. Ther. 2014, 94, 1660–1675. [Google Scholar] [CrossRef] [PubMed]
- Morrissey, E.C.; Corbett, T.K.; Walsh, J.C.; Molloy, G.J. Behavior change techniques in apps for medication adherence: A content analysis. Am. J. Prev. Med. 2016, 50, e143–e146. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Sheals, K.; Godinho, C.A. Evaluating the effectiveness of behavior change techniques in health-related behavior: A scoping review of methods used. Transl. Behav. Med. 2018, 8, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Carey, R.N.; Johnston, M.; Rothman, A.J.; De Bruin, M.; Kelly, M.P.; Connell, L.E. From theory-inspired to theory-based interventions: A protocol for developing and testing a methodology for linking behaviour change techniques to theoretical mechanisms of action. Ann. Behav. Med. 2018, 52, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Novak, M.; Costantini, L.; Schneider, S.; Beanlands, H. Approaches to self-management in chronic illness. In Seminars in Dialysis; Blackwell Publishing Ltd.: Oxford, UK, 2013; pp. 188–194. [Google Scholar]
- National Heart, Lung, and Blood Institute. Your Guide to Lowering Blood Pressure. 2003. Available online: https://www.nhlbi.nih.gov/files/docs/public/heart/new_dash.pdf (accessed on 23 May 2023).
- Wicks, P.; Chiauzzi, E. ‘Trust but verify’–five approaches to ensure safe medical apps. BMC Med. 2015, 13, 205. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Behaviour Change: Individual Approaches. Available online: https://www.nice.org.uk/guidance/ph49/chapter/1-Recommendations#recommendation-15-monitor-behaviour-change-interventions (accessed on 22 May 2023).
- Singh, K.; Drouin, K.; Newmark, L.P.; Rozenblum, R.; Lee, J.; Landman, A.; Pabo, E.; Klinger, E.V.; Bates, D.W. Developing a framework for evaluating the patient engagement, quality, and safety of mobile health applications. Issue Brief (Commonw Fund) 2016, 5, 11. [Google Scholar]
- BinDhim, N.F.; Hawkey, A.; Trevena, L. A systematic review of quality assessment methods for smartphone health apps. Telemed. e-Health 2015, 21, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Grainger, R.; Devan, H.; Sangelaji, B.; Hay-Smith, J. Issues in reporting of systematic review methods in health app-focused reviews: A scoping review. Health Inform. J. 2020, 26, 2930–2945. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Name of App | App Functions |
|---|---|
| My DASH Diet: Food Tracker and low sodium Recipes |
|
| NOOM |
|
| Nutritionix Track |
|
| DASH Diet Tracker |
|
| DASH diet: weight loss Plan |
|
| DASH Diet: Doctor Recommendation |
|
| DASH To TEN |
|
| The Theoretical Domain Framework | Behaviour Change Techniques | Frequency of TDF Domain in Apps (N) |
|---|---|---|
| Beliefs about capabilities | Social support | 7 |
| Problem solving | ||
| Action planning | ||
| Goals | Goal setting (outcome) | 7 |
| Goal setting (behaviour) | ||
| Review outcome goal(s) | ||
| Review behaviour goal(s) | ||
| Action planning | ||
| Knowledge | Information about health consequences | 7 |
| Instruction on how to perform a behaviour | ||
| Credible source | ||
| Feedback on behaviour | ||
| Feedback on outcomes of behaviour | ||
| Biofeedback | ||
| Skills | Problem solving | 7 |
| Biofeedback | ||
| Beliefs about consequences | Feedback on behaviour | 7 |
| Feedback on outcomes of behaviour | ||
| Behaviour regulation | Self-monitoring of behaviour | 7 |
| Self-monitoring of outcome(s) of behaviour | ||
| Problem solving | ||
| Memory, attention, and decision processes | Prompts/cues | 5 |
| Habit formation | ||
| Reinforcement | Credible source | 4 |
| Emotion | Reduce negative emotion | 1 |
| App Name | App Quality Evaluation Domain | ||||||
|---|---|---|---|---|---|---|---|
| Behaviour Change Potential | Knowledge Building | Skill Building | Function | App Purpose | Appropriate for Adults | Appropriate for Hypertension | |
| My Dash Diet: Food tracker and low sodium Recipes | 7 (0.2) | 8.2 (0) | 7.4 (0.6) | 7.2 (0.4) | 10 (0) | 9.3 (0.5) | 8.5 (0.4) |
| DASH Diet: Doctor Recommendation | 6.5 (0.9) | 4.4 (1.0) | 6.7 (0) | 7.6 (0.2) | 6.1 (0.9) | 8.6 (0.5) | 3.8 (0) |
| DASH To TEN | 7 (0.2) | 8 (0.2) | 7 (0.6) | 8 (0.6) | 8.3 (0.1) | 8.6 (0.5) | 7.5 (0) |
| DASH Diet Tracker | 2.8 (0.6) | 2.5 (0.2) | 4.4 (1.9) | 4.8 (0.2) | 4.4 (0.9) | 4.3 (0.5) | 0 (0) |
| DASH diet: weight loss Plan | 0.6 (0.2) | 0.9 (0) | 2.9 (2.5) | 4.7 (0.9) | 2.7 (0.9) | 3.6 (0.5) | 0 (0) |
| NOOM | 8.4 (1.2) | 9.2 (0.5) | 7.8 (0) | 9.1 (1.1) | 3.4 (0.2) | 9.6 (0.5) | 7.1 (1.4) |
| Nutritionix track | 5.03 (1.02) | 3.2 (0.42) | 5.5 (1.5) | 7.1 (0.24) | 8.3 (0) | 8 (0.47) | 3.8 (0.24) |
| App Name | Version Type | No of BCTs | TDF Mechanisms of Actions, n | Quality of App, n | Privacy and Security |
|---|---|---|---|---|---|
| My Dash Diet: Food tracker and low sodium Recipes | iPhone and Android | 14 | 7 | 4 domains > 8 | X |
| DASH diet: weight loss Plan | Android | 8 | 8 | 0 domains > 8 | X |
| DASH To TEN | iPhone | 13 | 9 | 4 domains > 8 | ✓ |
| DASH Diet Tracker | iPhone | 9 | 6 | 0 domains > 8 | X |
| DASH Diet: Doctor Recommendation | iPhone | 14 | 8 | 1 domain > 8 | ✓ |
| NOOM | iPhone and Android | 19 | 9 | 4 domains > 8 | ✓ |
| Nutritionix track | iPhone and Android | 12 | 7 | 2 domains > 8 | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alnooh, G.; Alessa, T.; Noorwali, E.; Albar, S.; Williams, E.; de Witte, L.P.; Hawley, M.S. Identification of the Most Suitable Mobile Apps to Support Dietary Approaches to Stop Hypertension (DASH) Diet Self-Management: Systematic Search of App Stores and Content Analysis. Nutrients 2023, 15, 3476. https://doi.org/10.3390/nu15153476
Alnooh G, Alessa T, Noorwali E, Albar S, Williams E, de Witte LP, Hawley MS. Identification of the Most Suitable Mobile Apps to Support Dietary Approaches to Stop Hypertension (DASH) Diet Self-Management: Systematic Search of App Stores and Content Analysis. Nutrients. 2023; 15(15):3476. https://doi.org/10.3390/nu15153476
Chicago/Turabian StyleAlnooh, Ghadah, Tourkiah Alessa, Essra Noorwali, Salwa Albar, Elizabeth Williams, Luc P. de Witte, and Mark S. Hawley. 2023. "Identification of the Most Suitable Mobile Apps to Support Dietary Approaches to Stop Hypertension (DASH) Diet Self-Management: Systematic Search of App Stores and Content Analysis" Nutrients 15, no. 15: 3476. https://doi.org/10.3390/nu15153476
APA StyleAlnooh, G., Alessa, T., Noorwali, E., Albar, S., Williams, E., de Witte, L. P., & Hawley, M. S. (2023). Identification of the Most Suitable Mobile Apps to Support Dietary Approaches to Stop Hypertension (DASH) Diet Self-Management: Systematic Search of App Stores and Content Analysis. Nutrients, 15(15), 3476. https://doi.org/10.3390/nu15153476