
Nutritional Intake and Biomarker Status in Strict Raw Food Eaters


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Blood Sample and 24 h Urine Sample
2.3. Dietary Assessment
2.4. Statistics
3. Results
3.1. Study Population
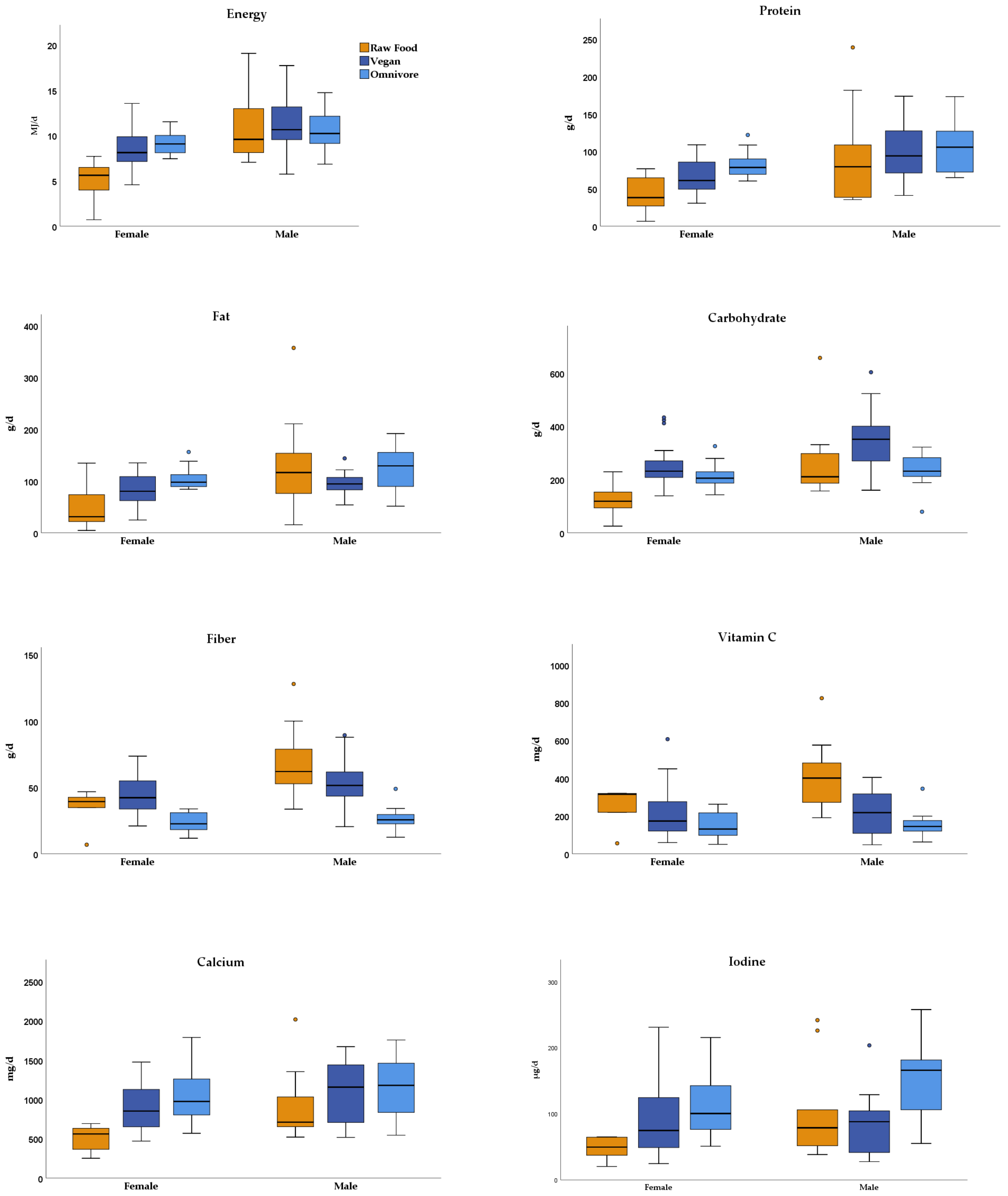
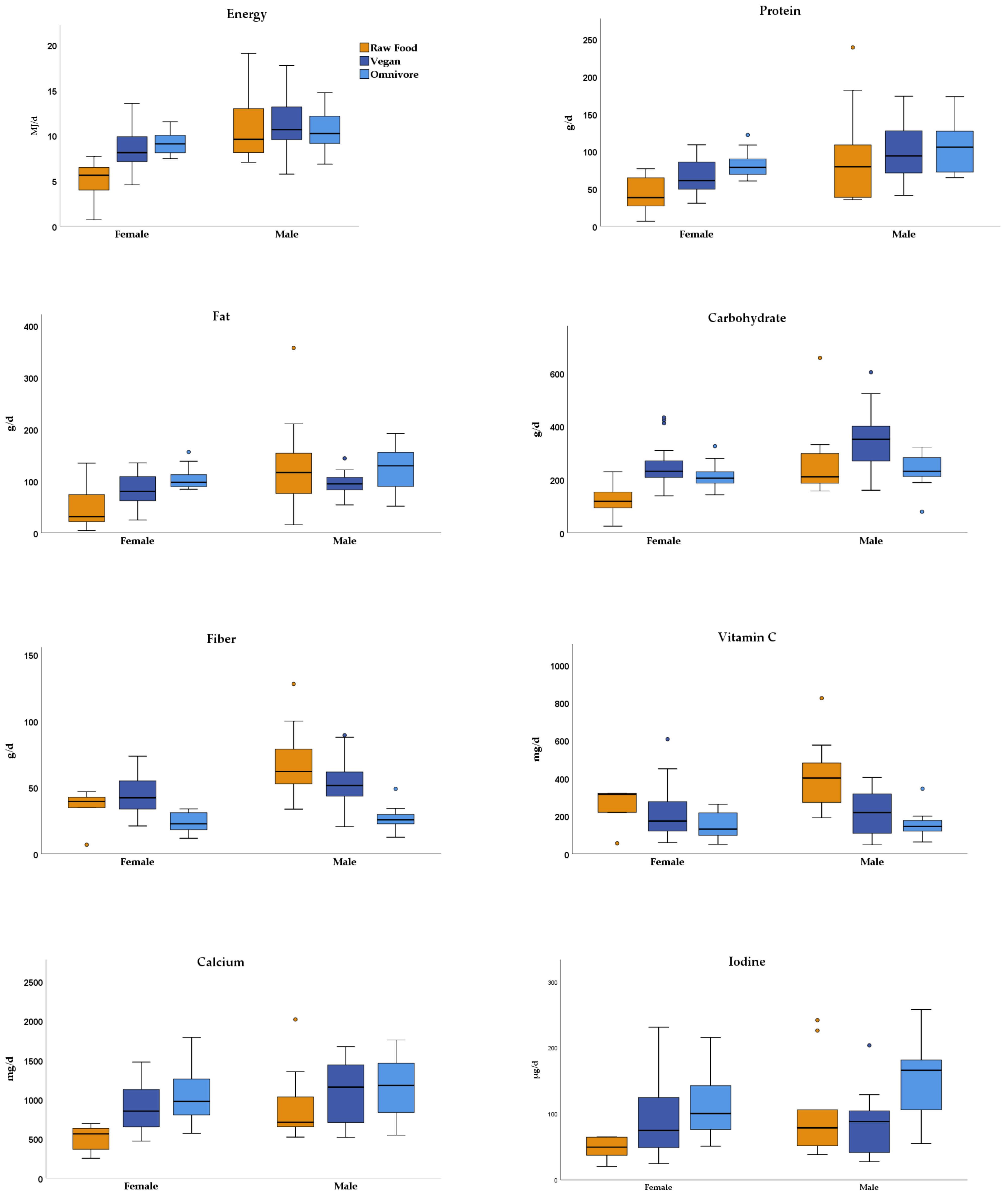
3.2. Dietary Intake
3.3. Laboratory Blood and Serum Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Boekel, M.; Fogliano, V.; Pellegrini, N.; Stanton, C.; Scholz, G.; Lalljie, S.; Somoza, V.; Knorr, D.; Jasti, P.R.; Eisenbrand, G. A review on the beneficial aspects of food processing. Mol. Nutr. Food Res. 2010, 54, 1215–1247. [Google Scholar] [CrossRef]
- Laden, G. The Consequences of Cooking: How the Origin of Cuisine Shaped Human Culture, Ecology, and Biology; Wiley-VCH: Weinheim, Germany, 2007. [Google Scholar]
- Wrangham, R.W.; Jones, J.H.; Laden, G.; Pilbeam, D.; Conklin-Brittain, N. The Raw and the Stolen. Cooking and the Ecology of Human Origins. Curr. Anthropol. 1999, 40, 567–594. [Google Scholar] [CrossRef] [PubMed]
- Koszucka, A.; Nowak, A. Thermal processing food-related toxicants: A review. Crit. Rev. Food Sci. Nutr. 2019, 59, 3579–3596. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Morrissey, P.A. Nutritional and toxicological aspects of the Maillard browning reaction in foods. Crit. Rev. Food Sci. Nutr. 1989, 28, 211–248. [Google Scholar] [CrossRef] [PubMed]
- Koszucka, A.; Nowak, A.; Nowak, I.; Motyl, I. Acrylamide in human diet, its metabolism, toxicity, inactivation and the associated European Union legal regulations in food industry. Crit. Rev. Food Sci. Nutr. 2020, 60, 1677–1692. [Google Scholar] [CrossRef] [PubMed]
- Bakhiya, N.; Abraham, K.; Gürtler, R.; Appel, K.E.; Lampen, A. Toxicological assessment of 3-chloropropane-1,2-diol and glycidol fatty acid esters in food. Mol. Nutr. Food Res. 2011, 55, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Abraham, K.; Andres, S.; Palavinskas, R.; Berg, K.; Appel, K.E.; Lampen, A. Toxicology and risk assessment of acrolein in food. Mol. Nutr. Food Res. 2011, 55, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Koebnick, C.; Garcia, A.L.; Dagnelie, P.C.; Strassner, C.; Lindemans, J.; Katz, N.; Leitzmann, C.; Hoffmann, I. Long-term consumption of a raw food diet is associated with favorable serum LDL cholesterol and triglycerides but also with elevated plasma homocysteine and low serum HDL cholesterol in humans. J. Nutr. 2005, 135, 2372–2378. [Google Scholar] [CrossRef]
- Goempel, K.; Tedsen, L.; Ruenz, M.; Bakuradze, T.; Schipp, D.; Galan, J.; Eisenbrand, G.; Richling, E. Biomarker monitoring of controlled dietary acrylamide exposure indicates consistent human endogenous background. Arch. Toxicol. 2017, 91, 3551–3560. [Google Scholar] [CrossRef]
- Abraham, K.; Hielscher, J.; Kaufholz, T.; Mielke, H.; Lampen, A.; Monien, B. The hemoglobin adduct N-(2,3-dihydroxypropyl)-valine as biomarker of dietary exposure to glycidyl esters: A controlled exposure study in humans. Arch. Toxicol. 2019, 93, 331–340. [Google Scholar] [CrossRef] [Green Version]
- Rietjens, I.; Dussort, P.; Günther, H.; Hanlon, P.; Honda, H.; Mally, A.; O’Hagan, S.; Scholz, G.; Seidel, A.; Swenberg, J.; et al. Exposure assessment of process-related contaminants in food by biomarker monitoring. Arch. Toxicol. 2018, 92, 15–40. [Google Scholar] [CrossRef] [Green Version]
- Rietjens, I.; Michael, A.; Bolt, H.M.; Siméon, B.; Andrea, H.; Nils, H.; Christine, K.; Angela, M.; Gloria, P.; Daniel, R.; et al. The role of endogenous versus exogenous sources in the exposome of putative genotoxins and consequences for risk assessment. Arch. Toxicol. 2022, 96, 1297–1352. [Google Scholar] [CrossRef]
- Weikert, C.; Trefflich, I.; Menzel, J.; Obeid, R.; Longree, A.; Dierkes, J.; Meyer, K.; Herter-Aeberli, I.; Mai, K.; Stangl, G.I.; et al. Vitamin and Mineral Status in a Vegan Diet. Dtsch. Arztebl. Int. 2020, 117, 575–582. [Google Scholar] [CrossRef]
- Peters, T.; Brage, S.; Westgate, K.; Franks, P.W.; Gradmark, A.; Tormo Diaz, M.J.; Huerta, J.M.; Bendinelli, B.; Vigl, M.; Boeing, H.; et al. Validity of a short questionnaire to assess physical activity in 10 European countries. Eur. J. Epidemiol. 2012, 27, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Trefflich, I.; Marschall, H.U.; Giuseppe, R.D.; Ståhlman, M.; Michalsen, A.; Lampen, A.; Abraham, K.; Weikert, C. Associations between Dietary Patterns and Bile Acids-Results from a Cross-Sectional Study in Vegans and Omnivores. Nutrients 2019, 12, 47. [Google Scholar] [CrossRef] [Green Version]
- D-A-CH. Deutsche Gesellschaft für Ernährung, Österreichische Gesellschaft für Ernährung, Schweizerische Gesellschaft für Ernährung. Referenzwerte für die Nährstoffzufuhr. 2. Aufl., 5. Aktualisierte Ausgabe. Available online: https://www.dge.de/wissenschaft/referenzwerte/tool/ (accessed on 7 April 2022).
- Richter, M.; Boeing, H.; Grünewald-Funk, D.; Heseker, H.; Kroke, A.; Leschik-Bonnet, E.; Oberritter, H.; Strohm, D.; Watzl, B. Vegan diet: Position of the German Nutrition Society (DGE). Ernahr. Umsch. 2016, 63, M262. [Google Scholar]
- Schüpbach, R.; Wegmüller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef]
- Smith, A.D.; Refsum, H. Homocysteine—From disease biomarker to disease prevention. J. Intern. Med. 2021, 290, 826–854. [Google Scholar] [CrossRef]
- Kuzan, A. Toxicity of advanced glycation end products (Review). Biomed. Rep. 2021, 14, 46. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, Y.; Fu, L. Dietary advanced glycation end-products: Perspectives linking food processing with health implications. Compr. Rev. Food Sci. Food Saf. 2020, 19, 2559–2587. [Google Scholar] [CrossRef]
- Jallut, O. Instinct therapy-raw food with meat with exclusion of milk products. Report No. 16. Schweiz. Rundsch. Med. Prax. 1989, 78, 697–701. [Google Scholar] [PubMed]
- Koebnick, C.; Strassner, C.; Hoffmann, I.; Leitzmann, C. Consequences of a long-term raw food diet on body weight and menstruation: Results of a questionnaire survey. Ann. Nutr. Metab. 1999, 43, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Shew, J.L.; Holloszy, J.O.; Villareal, D.T. Low bone mass in subjects on a long-term raw vegetarian diet. Arch. Intern. Med. 2005, 165, 684–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Interview/Questionnaire | 3-Day Weighed Food Record (n = 15) | Suppl. | ||||
|---|---|---|---|---|---|---|
| Age | Sex, Duration of Raw Food Diet (Years) | Type of Diet | Main Nutritional Components in Brackets: Food of Animal Origin | Striking Observations Meal Pattern | Vitamin B12 | Vitamin D |
| 20–29 years | male, 1.5 | mixed | Fruits, vegetable, nuts, avocado (egg 1–2 ×/week, infrequent: meat, fish) | Germinated legumes/cereals, meat meals start late in the day | ||
| female, 2.3 | vegetarian | Red millet, buckwheat, lentils, wild herbs, sprouts, fruits (raw milk cheese every 2 weeks) | Seaweed, germinated legumes/cereals | ✓ | ✓ | |
| male, 1.8 | vegan | Fruits, vegetable, nuts | Fresh fruits >1 kg/day, protein bars, fermented vegetables | ✓ | ✓* | |
| 30–39 years | male, 0.75 | vegan | Vegetable, fruits, sprouts, wild herbs | Nuts >300 g/day, raw vegetables >1 kg/day meals start late in the day | ✓ | ✓ |
| male, 10 | vegetarian | Red millet, buckwheat, lentils, wild herbs, sprouts, fruits (raw milk cheese every 2 weeks) | Seaweed, germinated legumes/cereals | ✓ | ✓ | |
| 40–49 years | male, 28 | mixed | Fruits, nuts, avocado, meat (meat, fish, egg 1–2 ×/week) | Fresh fruits >1 kg/day, germinated legumes/cereals, mussel, poultry meals late in evening and night | ✓* | |
| male, 26 | vegetarian | Fruits, vegetable, nuts (infrequent: egg) | No record delivered | ✓ | ✓* | |
| female, 0.33 | vegan | Vegetable, salads | Meals start late in the day, one fasting day | ✓ | ✓* | |
| male, 14 | mixed | Fruits, vegetables, nuts, meat (up to 1 kg/week) (meat, fish, infrequent: egg, liver) | Fresh fruits >1 kg/day, meat meals start late in the day | |||
| female, 16 | mixed | Peas, protein bars, nuts (meat, fish, egg) | Protein bars | ✓ | ||
| >50 years | male, 15 | mixed | Products of raw milk, fruits, salads with vegetable (meat, liver, egg, milk) | Milk >1 L/day, meat, eggs meals start late in the day | ✓ | |
| male, 29 | mixed | Fruits, vegetable, nuts (meat, fish) | Fish >300 g/day, nuts >300 g/day, raw vegetables >1 kg/day meals start late in the day | |||
| female, 0.33 | mixed | Fruits, vegetable (infrequent: fish) | Fresh fruits >1 kg/day | ✓ | ✓ | |
| male, 20 | vegan | Nuts, vegetable, pumpkin, mushrooms, fruits | Fresh fruits >1 kg/day meals start late in the day | |||
| female, 0.33 | vegetarian | Vegetable, fruits, buckwheat, raw milk butter | Fermented vegetables | ✓ | ||
| male, 20 | mixed | Fruits, salads, (meat) | Fresh fruits >1 kg/day, meat >1 kg/day | |||
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Raw Food (n = 5) | Vegan (n = 18) | Omnivore (n = 14) | Raw Food (n = 11) | Vegan (n = 14) | Omnivore (n = 13) | |
| Age (years) | 44.8 ± 14 | 38.9 ± 7.8 | 38.6 ± 8.3 | 44.6 ± 12.2 | 37.6 ± 8.0 | 40.2 ± 7.2 |
| BMI (kg/m2) | 21.4 ± 3.0 | 21.8 ± 3.0 | 23.2 ± 2.2 | 20.7 ± 2.0 | 24.5 ± 3.3 | 24.4 ± 1.8 |
| Waist (cm) | 74.0 (72.0–74.0) | 71.9 (68.2–75.8) | 73.8 (72.8–76.0) | 76.0 (74.0–86.0) | 86.3 (79.9–92.4) | 86.8 (83.7–90.5) |
| Weight (kg) | 60.2 (55.8–65.0) | 59.3 (52.4–67.8) | 65.6 (61.3–72.4) | 65.0 (60.7–71.3) | 81.9 (72.8–92.7) | 81.1 (78.0–85.9) |
| Duration Raw (years) | 3.9 ± 6.8 | 15.1 ± 10.6 | ||||
| Body fat (% of body weight) | 28.7 ± 8.2 | 29.1 ± 6.5 | 30.8 ± 4.9 | 13.9 ± 4.9 *** | 20.8 ± 4.6 | 20.8 ± 2.9 |
| Muscle (% of body weight) | 30.6 ± 2.9 | 29.6 ± 2.8 | 29.7 ± 2.6 | 39.8 ± 3.4 *** | 37.4 ± 2.5 | 37.2 ± 2.2 |
| Blood pressure Diast. (mm Hg) | 71.4 ± 14.7 | 68.5 ± 7.7 | 70.8 ± 5.3 | 69.2 ± 8.5 | 71.9 ± 8.0 | 76.6 ± 7.7 |
| Blood pressure Syst. (mm Hg) | 110.0 ± 12.4 | 105.7 ± 8.4 | 106.1 ± 8.5 | 117.6 ± 13.6 | 117.6 ± 11.9 | 123.2 ± 11.8 |
| High physical activity (n) * | 1 (20%) | 16 (89%) | 12 (86%) | 7 (70%) **** | 12 (86%) | 12 (92%) |
| High education (n) ** | 4 (80%) | 12 (67%) | 9 (64%) | 5 (50%) **** | 9 (64%) | 11 (85%) |
| Any supplementation (n) | 5 (100%) | 17 (94%) | 6 (43%) | 7 (64%) | 14 (100%) | 4 (31%) |
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Raw Food (n = 5) | Vegan (n = 18) | Omnivore (n = 14) | Raw Food (n = 11) | Vegan (n = 14) | Omnivore (n = 13) | |
| Haemoglobin [g/dL] | 13.5 ± 0.7 | 12.8 ± 0.8 | 12.7 ± 0.9 | 13.5 ± 1.5 a,c | 14.5 ± 0.9 a | 15.0 ± 0.6 a,c |
| Haematocrit [%] | 40.1 ± 2.7 | 39.0 ± 2.2 | 38.8 ± 2.7 | 40.8 ± 4.3 | 42.8 ± 2.6 | 43.6 ± 1.8 |
| Erythrocytes [T/L] | 4.6 ± 0.3 | 4.3 ± 0.5 | 4.4 ± 0.3 | 4.5 ± 0.5 | 4.9 ± 0.4 | 5.0 ± 0.3 |
| MCV [fl] | 88.1 (87.5–88.9) a,b | 91.4 (89.3–92.4) a,b | 90.0 (88.8–91.2) a | 90.1 (88.8–93.7) | 88.2 (87.2–92.2) | 88.8 (84.0–89.5) |
| MCHC [g/dL] | 33.6 ± 0.9 | 32.8 ± 0.7 | 32.7 ± 1.1 | 33.1 ± 0.5 | 34.0 ± 0.6 | 34.4 ± 0.7 |
| Leucocytes [G/L] | 3.8 (3.8–5.9) | 5.2 (3.7–6.8) | 4.8 (4.5–5.7) | 5.0 (4.2–6.1) | 4.6 (4.1–5.6) | 4.7 (4.5–5.7) |
| Thrombocytes [G/L] | 225 (216–269) | 225 (191–299) | 241 (220–276) | 247 (199–290) | 196 (147–220) | 217 (184–231) |
| Protein total [g/dL] | 7.1 ± 0.5 | 6.9 ± 0.3 | 7.0 ± 0.4 | 7.5 ± 0.4 a,b,c | 6.8 ± 0.5 a,b | 7.0 ± 0.3 a,c |
| CRP [mg/L] | 0.30 (0.30–0.30) | 0.29 (0.19–0.47) | 0.47 (0.08–0.75) | 0.30 (0.30–0.90) | 0.79 (0.39–1.06) | 0.63 (0.26–1.59) |
| Glucose [mg/dL] | 74 (69–80) | 82 (76–85) | 79 (75–85) | 82 (79–89) | 81 (79–88) | 84 (83–91) |
| HbA1c [%] | 5.3 (5.1–5.3) | 5.1 (5.0–5.2) | 5.1 (5.1–5.2) | 5.1 (5.0–5.3) | 5.1 (5.0–5.2) | 5.2 (5.1–5.4) |
| gamma GT [U/L] | 11 (11–14) | 12 (10–17) | 13 (10–17) | 13 (12–23) a,c | 16 (13–22) a | 24 (18–29) a,c |
| GPT [U/L] | 15 (12–22) | 18 (15–21) | 16 (13–18) | 20 (18–24) | 25 (19–35) | 27 (21–37) |
| Creatinine [mg/dL] | 0.71 ± 0.06 | 0.73 ± 0.09 | 0.83 ± 0.09 | 0.89 ± 0.19 | 0.93 ± 0.13 | 1.01 ± 0.14 |
| TSH [mU/L] | 1.91 (1.88–1.94) | 1.86 (1.28–2.33) | 2.18 (1.64–3.33) | 1.42 (1.10–3.12) | 2.30 (1.72–3.25) | 2.42 (1.95–3.04) |
| Ferritin [ng/mL] | 76 (53–97) a,b | 34 (17–42) a,b | 40 (22–70) a | 110 (45–168) | 81 (67–86) | 121 (68–153) |
| Cholesterol [mg/dL] | 172 (154–185) a | 160 (139–177) a,d | 198 (186–218) a,d | 131 (122–163) a,c | 156 (133–212) a | 195 (168–215) a,c |
| LDL [mg/dL] | 94 (94–111) | 91 (73–96) | 104 (84–116) | 70 (62–94) a,c | 85 (70–125) a | 116 (93–136) a,c |
| HDL [mg/dL] | 54 (51–71) a | 65 (56–74) a,d | 80 (70–83) a,d | 49 (46–52) | 51 (45–56) | 52 (48–60) |
| Triglycerides [mg/dL] | 51 (38–68) | 64 (51–74) | 55 (47–93) | 62 (51–101) | 85 (61–111) | 86 (70–136) |
| Vitamin B12 [pg/mL] | 329 (280–399) | 449 (312–657) | 383 (317–521) | 290 (152–433) | 673 (288–792) | 431 (361–488) |
| Homocysteine [µmol/L] | 10.3 (6.7–15.5) | 8.6 (6.6–10.2) | 7.7 (6.9–8.6) | 12.2 (8.9–19.0) a,b | 8.3 (7.8–11.3) a,b | 9.8 (8.8–10.8) a |
| Vitamin D3 [mmol/L] | 37.2 (28.2–43.9) | 52.2 (23.9–84.2) | 51.8 (28.4–81.8) | 37.0 (26.7–56.6) | 68.6 (18.6–108.5) | 41.4 (36.3–59.2) |
| Calcium [mmol/L] | 2.35 ± 0.09 | 2.33 ± 0.06 | 2.35 ± 0.07 | 2.40 ± 0.12 | 2.36 ± 0.09 | 2.39 ± 0.05 |
| Zinc [µg/dL] | 76 (69–81) | 81 (72–89) | 82 (79–91) | 71 (64–88) | 77 (75–90) | 84 (80–103) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abraham, K.; Trefflich, I.; Gauch, F.; Weikert, C. Nutritional Intake and Biomarker Status in Strict Raw Food Eaters. Nutrients 2022, 14, 1725. https://doi.org/10.3390/nu14091725
Abraham K, Trefflich I, Gauch F, Weikert C. Nutritional Intake and Biomarker Status in Strict Raw Food Eaters. Nutrients. 2022; 14(9):1725. https://doi.org/10.3390/nu14091725
Chicago/Turabian StyleAbraham, Klaus, Iris Trefflich, Fabian Gauch, and Cornelia Weikert. 2022. "Nutritional Intake and Biomarker Status in Strict Raw Food Eaters" Nutrients 14, no. 9: 1725. https://doi.org/10.3390/nu14091725
APA StyleAbraham, K., Trefflich, I., Gauch, F., & Weikert, C. (2022). Nutritional Intake and Biomarker Status in Strict Raw Food Eaters. Nutrients, 14(9), 1725. https://doi.org/10.3390/nu14091725