
Month-of-Birth Effect on Muscle Mass and Strength in Community-Dwelling Older Women: The French EPIDOS Cohort

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Muscle Strength Measure
2.3. Muscle Mass Measure
2.4. Covariates
2.5. Statistical Analysis
2.6. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 25OHD | 25-hydroxyvitamin D |
| ASM | Appendicular skeletal muscle mass |
| BMI | body mass index |
| kg | kilograms |
| DXA | Dual Energy X-ray Absorptiometry |
| IADL | instrumental activities of daily living |
| MoB | month of birth |
| N | Newton |
| SD | standard deviations |
| UV-B | ultraviolet-B rays |
| VDR | vitamin D receptor |
References
- Ceglia, L. Vitamin D and skeletal muscle tissue and function. Mol. Aspects Med. 2008, 29, 407–414. [Google Scholar] [CrossRef]
- Annweiler, C.; Schott, A.M.; Berrut, G.; Fantino, B.; Beauchet, O. Vitamin D-related changes in physical performance: A systematic review. J. Nutr. Health Aging 2009, 13, 893–898. [Google Scholar] [CrossRef]
- Hines, E.A.; Coffey, J.D.; Starkey, C.W.; Chung, T.K.; Starkey, J.D. Improvement of maternal vitamin D status with 25-hydroxycholecalciferol positively impacts porcine fetal skeletal muscle development and myoblast activity. J. Anim. Sci. 2013, 91, 4116–4122. [Google Scholar] [CrossRef]
- Við Streym, S.; Kristine Moller, U.; Rejnmark, L.; Heickendorff, L.; Mosekilde, L.; Vestergaard, P. Maternal and infant vitamin D status during the first 9 months of infant life—A cohort study. Eur. J. Clin. Nutr. 2013, 67, 1022–1028. [Google Scholar] [CrossRef]
- Dovnik, A.; Mujezinović, F.; Treiber, M.; Pečovnik Balon, B.; Gorenjak, M.; Maver, U.; Takač, I. Seasonal variations of vitamin D concentrations in pregnant women and neonates in Slovenia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 181, 6–9. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G.; Ramagopalan, S. The month of birth effect in multiple sclerosis: Systematic review, meta-analysis and effect of latitude. J. Neurol. Neurosurg. Psychiatry 2013, 84, 427–432. [Google Scholar] [CrossRef]
- Krishnaveni, G.V.; Veena, S.R.; Winder, N.R.; Hill, J.C.; Noonan, K.; Boucher, B.J.; Karat, S.C.; Fall, C.H. Maternal vitamin D status during pregnancy and body composition and cardiovascular risk markers in Indian children: The Mysore Parthenon Study. Am. J. Clin. Nutr. 2011, 93, 628–635. [Google Scholar] [CrossRef]
- Sayers, A.; Tobias, J.H. Estimated maternal ultraviolet B exposure levels in pregnancy influence skeletal development of the child. J. Clin. Endocrinol. Metab. 2009, 94, 765–771. [Google Scholar] [CrossRef]
- Dargent-Molina, P.; Favier, F.; Grandjean, H.; Baudoin, C.; Schott, A.M.; Hausherr, E.; Meunier, P.J.; Bréart, G. Fall-related factors and risk of hip fracture: The EPIDOS prospective study. Lancet 1996, 348, 145–149. [Google Scholar] [CrossRef]
- Gillette-Guyonnet, S.; Nourhashemi, F.; Andrieu, S.; Cantet, C.; Albarède, J.L.; Vellas, B.; Grandjean, H. Body composition in French women 75+ years of age: The EPIDOS study. Mech. Ageing Dev. 2003, 124, 311–316. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Dupuy, C.; Lauwers-Cances, V.; van Kan, G.A.; Gillette, S.; Schott, A.M.; Beauchet, O.; Annweiler, C.; Vellas, B.; Rolland, Y. Dietary vitamin D intake and muscle mass in older women. Results from a cross-sectional analysis of the EPIDOS study. J. Nutr. Health Aging 2013, 17, 119–124. [Google Scholar] [CrossRef]
- Annweiler, C.; Schott, A.M.; Beauchet, O. Proposal and validation of a quick question to rate the influence of sun exposure in geriatric epidemiological studies on vitamin D. Int. J. Vitam. Nutr. Res. 2012, 82, 412–416. [Google Scholar] [CrossRef]
- Boland, M.R.; Shahn, Z.; Madigan, D.; Hripcsak, G.; Tatonetti, N.P. Birth month affects lifetime disease risk: A phenome-wide method. J. Am. Med. Inform. Assoc. 2015, 22, 1042–1053. [Google Scholar] [CrossRef]
- Tonetti, L.; Milfont, T.L.; Tilyard, B.A.; Natale, V. Month of birth and mood seasonality: A comparison between countries in the northern and southern hemispheres. Psychiatry Clin. Neurosci. 2013, 67, 133–138. [Google Scholar] [CrossRef]
- Henneberg, M.; Louw, G.J. Height and weight differencies among South African urban school children born in various months of the year. Am. J. Hum. Biol. 1990, 2, 227–233. [Google Scholar] [CrossRef]
- Adair, L.S.; Pollitt, E. Seasonal variation in pre- and postpartum maternal body measurement and infant birthweights. Am. J. Phys. Anthropol. 1983, 62, 325–331. [Google Scholar] [CrossRef]
- Yliharsila, H.; Kajantie, E.; Osmond, C.; Forsen, T.; Barker, D.J.; Eriksson, J.G. Birth size, adult body composition and muscle strength in later life. Int. J. Obes. 2007, 31, 1392–1399. [Google Scholar] [CrossRef]
- Weber, G.W.; Prossinger, H.; Seidler, H. Height depends on month of birth. Nature 1998, 391, 754–755. [Google Scholar] [CrossRef]
- Banegas, J.R.; Rodriguez-Artalejo, F.; Graciani, A.; De La Cruz, J.J.; Gutierrez-Fisac, J.L. Month of birth and height of Spanish middle-aged men. Ann. Hum. Biol. 2001, 28, 15–20. [Google Scholar]
- Deng, J.; Wang, J.; Xiao, C.; Xu, S.; Gao, X.; Pan, F. The influence of birth month on total and cardiovascular mortality: A population-based surveillance study. Chronobiol. Int. 2020, 37, 1772–1777. [Google Scholar] [CrossRef]
- Vaiserman, A. Season-of-birth phenomenon in health and longevity: Epidemiologic evidence and mechanistic considerations. J. Dev. Orig. Health Dis. 2021, 12, 849–858. [Google Scholar] [CrossRef]
- Caci, H.; Robert, P.; Dossios, C.; Boyer, P. Morningness-Eveningness for Children Scale: Psychometric properties and month of birth effect. Encephale 2005, 31, 56–64. [Google Scholar] [CrossRef]
- Annweiler, C.; Legrand, E.; Souberbielle, J.C. Vitamin D in adults: Update on testing and supplementation. Geriatr. Psychol. Neuropsychiatr. Vieil. 2018, 16, 7–22. [Google Scholar] [CrossRef]
- Girgis, C.M.; Clifton-Bligh, R.J.; Hamrick, M.W.; Holick, M.F.; Gunton, J.E. The roles of vitamin D in skeletal muscle: Form, function, and metabolism. Endocr. Rev. 2012, 34, 33–83. [Google Scholar] [CrossRef]
- Zhou, H.; Chen, Y.; Lv, G.; Zhuo, Y.; Lin, Y.; Feng, B.; Fang, Z.; Che, L.; Li, J.; Xu, S.; et al. Improving maternal vitamin D status promotes prenatal and postnatal skeletal muscle development of pig offspring. Nutrition 2016, 32, 1144–1152. [Google Scholar] [CrossRef]
- Harvey, N.C.; Moon, R.J.; Sayer, A.A.; Ntani, G.; Davies, J.H.; Javaid, M.K.; Robinson, S.M.; Godfrey, K.M.; Inskip, H.M.; Cooper, C.; et al. Maternal antenatal vitamin D status and offspring muscle development: Findings from the Southampton Women’s Survey. J. Clin. Endocrinol. Metab. 2014, 99, 330–337. [Google Scholar] [CrossRef]
- Lauridsen, C. Triennial Growth Symposiumdestablishment of the 2012 vitamin D requirements in swine with focus on dietary forms and levels of vitamin D. J. Anim. Sci. 2014, 92, 910–916. [Google Scholar] [CrossRef]
- Fardet, L.; Flahault, A.; Kettaneh, A.; Tiev, K.P.; Généreau, T.; Tolédano, C.; Lebbé, C.; Cabane, J. Corticosteroid-induced clinical adverse events: Frequency, risk factors and patient’s opinion. Br. J. Dermatol. 2007, 157, 142–148. [Google Scholar] [CrossRef]
- Felman, A.L. Immediate effects of exercise on apparent limb mass and circumference. Int. Z. Angew. Physiol. 1963, 20, 38–44. [Google Scholar] [CrossRef]
- Tipton, K.D.; Elliott, T.A.; Cree, M.G.; Wolf, S.E.; Sanford, A.P.; Wolfe, R.R. Ingestion of casein and whey proteins result in muscle anabolism after resistance exercise. Med. Sci. Sports Exerc. 2004, 36, 2073–2081. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.S.; Tao, Y.H.; Huang, K.; Zhu, B.B.; Tao, F.B. Vitamin D and risk of preterm birth: Up-to-date meta-analysis of randomized controlled trials and observational studies. J. Obstet. Gynaecol. Res. 2017, 43, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Kuh, D.; Hardy, R.; Mortality Review Group; FALCon and HALCyon Study Teams. Objectively measured physical capability levels and mortality: Systematic review and meta-analysis. BMJ 2010, 341, c4467. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Cohort | |
|---|---|---|
| Summary Value | (95% CI) | |
| Demographical measures | ||
| Age, years | 80.5 ± 3.8 (70–98) | (80.4; 80.6) |
| Year of birth | 1912 ± 4 (1893–1922) | - |
| Recruitment center, n (%) | ||
| Amiens (49°54′ N) | 1488 (20.9) | (20.0; 21.8) |
| Paris (48°51′ N) | 1457 (20.4) | (19.5; 21.3) |
| Lyon (45°45′ N) | 1365 (19.1) | (18.2; 20.0) |
| Montpellier (43°36′ N) | 1492 (20.9) | (20.0; 21.8) |
| Toulouse (43°36′ N) | 1331 (18.7) | (17.8; 19.6) |
| Season of testing, n (%) | ||
| Spring | 1922 (26.9) | (25.9; 27.9) |
| Summer | 1876 (26.3) | (25.3; 27.3) |
| Fall | 1843 (25.8) | (24.8; 26.8) |
| Winter | 1492 (20.9) | (20.0; 21.8) |
| Clinical measures | ||
| Body mass index, kg/m2 | 25.3 ± 4.0 (14.5–42.1) | (25.2; 25.4) |
| Number of comorbidities, n (%) | 3.4 ± 2.0 (0–24) | (3.36; 3.44) |
| IADL score, /8 | 6.3 ± 1.3 (0–8) | (6.27; 6.33) |
| Regular physical activity, n (%) | 3490 (48.9) | (47.7; 50.1) |
| Sun exposure at midday, n (%) | 3609 (50.6) | (49.4; 51.8) |
| Dietary protein intake, g/day | 69.6 ± 16.2 (8.7–162.3) | (69.2; 70.0) |
| Dietary vitamin D intake, µg/week | 63.1 ± 31.3 (0–278.0) | (62.3; 63.9) |
| Use of vitamin D supplements, n (%) | 985 (13.8) | (13.0; 14.6) |
| History of corticosteroids use, n (%) | 455 (6.4) | (5.8; 7.0) |
| Current use of corticosteroids, n (%) | 146 (2.0) | (1.7; 2.3) |
| Muscles measures | ||
| Mean quadricipital strength, N | 162.3 ± 52.1 (17.3–507.3) | (161.1; 163.5) |
| Total ASM, kg * | 14.86 ± 2.04 (9.33–22.78) | (14.75; 14.97) |
| Month of Birth | Cohort | |||
|---|---|---|---|---|
| n | Percentage | (95% CI) | Cumulative Percentage | |
| January | 630 | 8.83 | (8.17; 9.49) | 8.83 |
| February | 602 | 8.43 | (7.79; 9.07) | 17.27 |
| March | 690 | 9.67 | (7.79; 9.07) | 26.95 |
| April | 568 | 7.96 | (7.33; 8.59) | 34.91 |
| May | 603 | 8.45 | (7.80; 9.10) | 43.36 |
| June | 573 | 8.03 | (7.40; 8.66) | 51.39 |
| July | 625 | 8.76 | (8.10; 9.42) | 60.16 |
| August | 598 | 8.38 | (7.74; 9.02) | 68.54 |
| September | 524 | 7.35 | (6.74; 7.96) | 75.89 |
| October | 527 | 7.39 | (6.78; 8.00) | 83.27 |
| November | 585 | 8.20 | (7.56; 8.84) | 91.48 |
| December | 608 | 8.52 | (7.87; 9.17) | 100.00 |
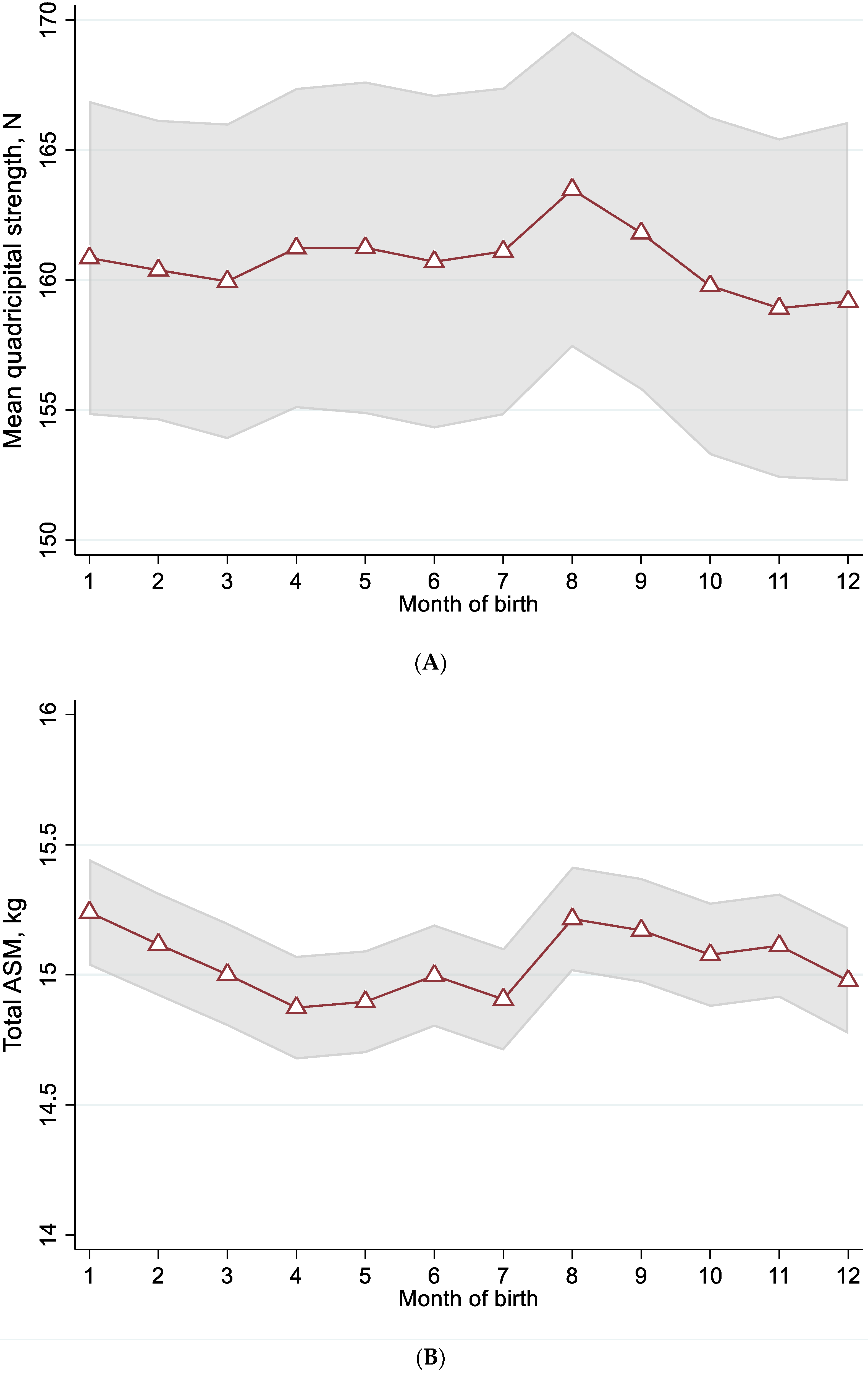
| Month of Birth | Mean Quadricipital Strength, N | Total ASM, kg |
|---|---|---|
| January | 161.0 ± 20.8 | 15.06 ± 1.20 |
| February | 160.0 ± 19.5 | 15.13 ± 1.19 |
| March | 160.0 ± 19.6 | 15.01 ± 1.17 |
| April | 161.0 ± 19.8 | 14.89 ± 1.22 |
| May | 161.2 ± 19.6 | 14.91 ± 1.15 |
| June | 160.9 ± 19.6 | 15.01 ± 1.18 |
| July | 160.6 ± 20.5 | 14.93 ± 1.24 |
| August | 163.4 ± 20.2 | 15.24 ± 1.27 |
| September | 161.6 ± 20.6 | 15.20 ± 1.29 |
| October | 159.8 ± 20.5 | 15.10 ± 1.19 |
| November | 158.8 ± 19.8 | 15.13 ± 1.21 |
| December | 159.0 ± 19.2 | 14.99 ± 1.21 |
| Beta for sin (p-value) | β = −2.1, p = 0.045 | β = −0.2, p = 0.013 |
| Beta for cos (p-value) | β = −0.5, p = 0.025 | β = 0.1, p = 0.092 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duval, G.T.; Schott, A.-M.; Sánchez-Rodríguez, D.; Herrmann, F.R.; Annweiler, C. Month-of-Birth Effect on Muscle Mass and Strength in Community-Dwelling Older Women: The French EPIDOS Cohort. Nutrients 2022, 14, 4874. https://doi.org/10.3390/nu14224874
Duval GT, Schott A-M, Sánchez-Rodríguez D, Herrmann FR, Annweiler C. Month-of-Birth Effect on Muscle Mass and Strength in Community-Dwelling Older Women: The French EPIDOS Cohort. Nutrients. 2022; 14(22):4874. https://doi.org/10.3390/nu14224874
Chicago/Turabian StyleDuval, Guillaume T., Anne-Marie Schott, Dolores Sánchez-Rodríguez, François R. Herrmann, and Cédric Annweiler. 2022. "Month-of-Birth Effect on Muscle Mass and Strength in Community-Dwelling Older Women: The French EPIDOS Cohort" Nutrients 14, no. 22: 4874. https://doi.org/10.3390/nu14224874
APA StyleDuval, G. T., Schott, A.-M., Sánchez-Rodríguez, D., Herrmann, F. R., & Annweiler, C. (2022). Month-of-Birth Effect on Muscle Mass and Strength in Community-Dwelling Older Women: The French EPIDOS Cohort. Nutrients, 14(22), 4874. https://doi.org/10.3390/nu14224874