Abstract
We performed a systematic review and meta-analysis to investigate the effects of vitamin D (VitD) supplementation on children with allergic diseases. MEDLINE, Embase, Web of Science, the Cochrane library, and three Chinese databases were searched up to 15 August 2022. Randomized controlled trials (RCTs) comparing a VitD supplementation versus a placebo for children with allergic diseases were included. Thirty-two RCTs with 2347 participants were included. VitD supplementation did not reduce the risk of asthma exacerbations in children compared with placebo overall (risk ratio (RR) = 0.84, 95% confidence interval (CI): 0.65 to 1.08, p = 0.18), but reduced the risk of asthma exacerbation in children with baseline serum 25(OH)D of <10 ng/mL compared with placebo (RR = 0.48, 95% CI: 0.28 to 0.83, p = 0.009). VitD supplementation significantly reduced Scoring Atopic Dermatitis or the Eczema Area and Severity Index scores in children with atopic dermatitis compared with placebo (standard mean difference = −0.5, 95% CI: −0.87 to −0.12, p = 0.009). VitD supplementation also reduced the symptom-medication score in children with allergic rhinitis compared with placebo (mean (standard deviation): 43.7 (3.3) vs. 57.8 (4.4), p = 0.001). In conclusion, VitD supplementation did not reduce asthma exacerbation risk in children overall but may reduce asthma exacerbation risk in children with serum 25(OH)D concentration < 10 ng/mL. VitD supplementation reduces the severity of atopic dermatitis and symptoms of allergic rhinitis in children.
1. Introduction
Allergic diseases, mainly involving asthma, allergic rhinitis (AR), atopic dermatitis (AD), and food allergy, now affect approximately 20% of the global population [1]. These diseases impose a tremendous burden on individuals, their families, and societies by reducing quality of life and productivity at work or school and causing considerable economic costs [1]. The prevalence of allergic diseases has continued to increase over the past few decades, especially among children [2]. This could be partially explained by genetic susceptibility, but this is also related to environmental factors, such as vitamin D deficiency [3].
Vitamin D is a pleiotropic hormone [4]. In addition to regulating calcium and phosphorus metabolism, vitamin D has strong immunomodulatory effects [4]. Vitamin D can inhibit type 2 helper T cell (Th2 cell) function [5]. It also inhibits B cell proliferation and differentiation to plasma cells, resulting in the diminished secretion of immunoglobulin (Ig) E [6]. It has been well acknowledged that Th2 response plays a critical role in all allergic diseases [7]. Hence, the growing interest in the effect of vitamin D on allergic diseases has been generated.
Many observational studies have found that vitamin D deficiency was highly prevalent in children with allergic diseases [8,9,10]. However, it is unclear whether vitamin D supplementation can improve the outcomes of children with allergic diseases. The effects of vitamin D supplementation on certain allergic diseases, such as asthma and atopic dermatitis, have been discussed in several systematic reviews (SRs) [11,12,13,14]. However, the effects of vitamin D supplementation on all allergic diseases in children have not been examined. The common comorbidities and shared pathogenesis of allergic diseases have led to the need for a common therapeutic approach [15,16,17]. Therefore, a holistic overview of the treatment effect of vitamin D on childhood allergic diseases is necessary. Some of the previous SRs did not identify the individuals who might derive the greatest benefit from vitamin D supplementation and did not examine the optimal regimen of vitamin D [12,13,14]. To resolve the above issues, we performed an SR and meta-analysis to investigate the effects of vitamin D supplementation on childhood allergic diseases.
2. Materials and Methods
This SR was performed in accordance with the Cochrane Handbook [18]. We reported the results in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [19]. This review has been registered on the PROSPERO (CRD42022299761).
2.1. Search Strategy
We searched MEDLINE, Embase, Web of Science, the Cochrane Library, China Biology Medicine (CBM), China National Knowledge Infrastructure (CNKI), and Wanfang Data databases for eligible studies from inception to 15 August 2022, without language restriction. Further details of the search strategy can be found in Table S1 in the Supplementary Materials. We also searched ClinicalTrials.gov, WHO International Clinical Trial Registry Platform, and Google.com for any relevant randomized controlled trials (RCTs). Searches were supplemented by handsearching through the reference lists of the included publications and previous SRs.
2.2. Eligibility Criteria and Study Selection
RCTs were assessed for eligibility criteria by two groups of experienced investigators (group 1 was QL and QZ; group 2 was ZW and YZ) who studied and evaluated these RCTs after careful consideration. Any discrepancy was resolved through consensus discussion or consultation with a third experienced investigator (ZL). The inclusion criteria were: (1) population: children aged 1 year to 18 years with allergic diseases such as asthma, allergic rhinitis (AR), atopic dermatitis (AD), food allergies, and anaphylaxis; (2) intervention: vitamin D supplementation; (3) control: placebo or no supplementation. We also allowed a maintenance dose of vitamin D (400 IU daily) as a control (compared with a high dose of vitamin D as an intervention) because some authors believe it was unethical to not provide vitamin D to the control group, who were suspected to have low serum 25(OH)D levels at enrollment [20]. We excluded publications that did not present research findings (e.g., narrative reviews, editorials, comments) or did not provide separate data for children.
2.3. Data Extraction
Two groups of investigators (group 1 was QL and QZ; group 2 was GZ, XT, and YL) extracted data in a blinded way. Data from each study were tabulated and checked by a third investigator (ZL) before inclusion in the analysis. The details of the data extraction are shown in Appendix S1 in the Supplementary Materials. The primary outcome for asthma was the number of children with one or more asthma exacerbations. Asthma exacerbation was defined as having at least one of the following: taking systemic corticosteroids for asthma exacerbation; an asthma-related emergency department (ED) visit or hospitalization, or both; taking short-acting β-agonists as quick-relief medication; or a physician-diagnosed exacerbation. The secondary outcomes for asthma include the number of children requiring systemic corticosteroids for asthma exacerbations, the number of children requiring ED visits or hospitalization for asthma exacerbations, the changes in childhood asthma control test (C-ACT) score, total asthma symptom (TAS) score, forced expiratory volume in the first second (FEV1) % predicted, FEV1/forced vital capacity (FVC) ratio, forced expiratory flow between 25% and 75% of vital capacity (FEF25–75), fractional exhaled nitric oxide (FeNO), total IgE, and interleukin 10 (IL-10) before and after an intervention. The primary outcome for AD was the change in Scoring Atopic Dermatitis (SCORAD) or the Eczema Area and Severity Index (EASI) before and after an intervention. The secondary outcomes for AD were Staphylococcus aureus skin colonization, the erythema index, and the skin conductance. The primary outcome for AR was symptoms-medication score. The secondary outcome for AR was symptoms score. Other outcomes include changes in serum 25(OH)D concentration before and after an intervention and adverse events. If data were missing or the reporting format was not suitable for the meta-analysis, we contacted the authors of studies by email or calculated from other reported data according to methods recommended by the Cochrane Handbook (Appendix S1 in the Supplementary Materials) [18].
2.4. Risk of Bias (RoB) Assessment and Quality of Evidence
Two groups of investigators (group 1 was QL and QZ; group 2 was ZW and YZ) independently assessed the RoB using the Cochrane collaboration risk of bias tool [18]. Each domain was graded as ‘low’, ‘high’, or ‘unclear’ risk. We assessed the quality of the evidence with the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach for all outcomes [21,22]. GRADE has four levels of evidence: ‘high’, ‘moderate’, ‘low’, or ‘very low’. The quality of evidence from RCTs starts at high and can be downgraded one or two levels due to risk of bias, imprecision, inconsistency, indirectness, and publication bias (e.g., from high to moderate) [21,22]. The disagreement was resolved by a third investigator (YC). Further details are shown in Appendix S1 in the Supplementary Materials.
2.5. Data Analysis
Dichotomous outcomes were presented as pooled risk ratios (RRs) and 95% confidence intervals (CIs). Continuous variables were presented as pooled mean differences (MDs) or standard mean differences (SMDs) with 95% CIs. We performed a meta-analysis using the random-effect Mantel-Haenszel model due to diverse population characteristics, intervention, and outcome measures. Heterogeneity was assessed by the I2 statistic and the value above 50% was suggested substantial statistical heterogeneity [18].
We performed pre-specified subgroup analyses on the following: baseline vitamin D level (serum 25[OH]D < 10 ng/mL vs. 10–19 ng/mL vs. 20–29 ng/mL vs. ≥30 ng/mL), age (1–5 year vs. ≥5 years), the severity of diseases (mild vs. moderate vs. severe), treatment duration (<6 months vs. ≥6 months), a daily dose of vitamin D (daily dose <2000 IU vs. ≥2000 IU), bolus-dose vitamin D given (without bolus dosing vs. administration of at least one bolus dose of vitamin D), and concomitant treatment (use of corticosteroids vs. not). There is currently no consensus definition of an optimal level of vitamin D [23]. Vitamin D levels were typically defined as deficient (serum 25(OH)D < 20 ng/mL), insufficient (20–29 ng/mL), and sufficient (≥30 ng/mL) [24,25]. A cutoff of <10 ng/mL increased the risk of rickets and osteomalacia dramatically, and vitamin D supplementation protected most strongly against acute respiratory infection in patients with baseline 25(OH)D < 10 ng/mL [26,27]. Therefore, serum 25(OH)D < 10 ng/mL was considered to determine severe vitamin D deficiency [23,28]. Based on the above reasons, we selected the 10 ng/mL, 20 ng/mL, and 30 ng/mL cutoffs for baseline serum 25(OH)D concentration in the subgroup analyses.
We also performed a sensitivity analysis to assess the robustness of our findings by excluding trials assessed as having a high risk of bias in one or more of the domains and trials in which mean or SD, or both of them were imputed for missing data. Publication bias was assessed by funnel plot and Egger’s test when there were at least 10 studies included in the meta-analysis. The threshold for significance for p values was 0.05. We performed our data analyses with STATA15.0 (StataCorp, College Station, TX, USA) and RevMan 5.4 software.
3. Results
3.1. Study Selection and Characteristics
We identified 3372 records with our search strategy, and 115 full-text articles were assessed for eligibility. After excluding 83 articles, 32 RCTs with 2347 participants were included in the review (Figure 1) [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60]. Among the 32 RCTs, 18 RCTs were for children with asthma [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46], 10 RCTs were for children with AD [47,48,49,50,51,52,53,54,55,56], and 4 RCTs were for children with AR [57,58,59,60]. There were no RCTs for children with food allergies and anaphylaxis. The characteristics of each included RCT are shown in Table 1.
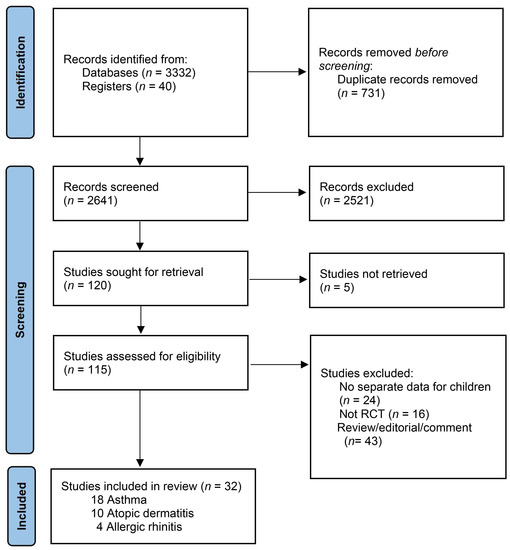
Figure 1.
Study flow diagram.

Table 1.
Study characteristics.
3.2. Risk of Bias
Four open-label RCTs did not blind patients and researchers and therefore had high risk of bias in the blinding domain [29,40,50,57]. Five RCTs had high risk of bias in handling missing data [37,46,55,59,60]. Fourteen RCTs had unclear risk of bias in at least one domain [30,31,34,35,36,38,39,41,49,51,53,54,56,58]. Nine RCTs had low risk in all domains [32,33,42,43,44,45,47,48,52]. Details of the RoB assessment results are provided in Figure S1 in the Supplementary Materials.
3.3. Childhood Asthma
3.3.1. Overall Analysis
Eleven studies with 1143 patients reported the primary outcome. The pooled estimates found that vitamin D supplementation did not reduce the number of children with one or more asthma exacerbations compared with placebo (RR = 0.84, 95% CI: 0.65 to 1.08, I2 = 59%, p = 0.18) (Figure 2). The quality of this evidence was downgraded to moderate due to their relative imprecision (Table S2 in the Supplementary Materials). Vitamin D supplementation was also not significantly associated with any of the secondary outcomes (Figure S2 in the Supplementary Materials).
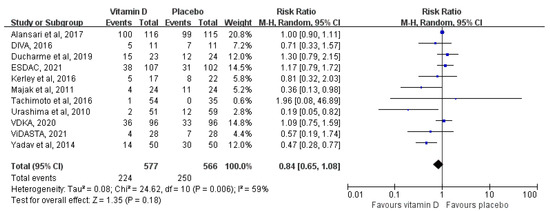
Figure 2.
Meta-analysis of the number of children with one or more asthma exacerbations [29,32,33,35,36,38,42,43,44,45,46].
3.3.2. Additional Analysis
We performed subgroup analyses of the primary outcome. We found a statistically significant interaction between asthma exacerbation risk and baseline serum 25(OH)D level (Pinteraction = 0.04), indicating that baseline serum 25[OH]D levels modified the effects of vitamin D supplementation on asthma exacerbation risk. The protective effect of vitamin D supplementation on asthma exacerbations decreased with the increase of baseline 25[OH]D levels (Figure 3). Vitamin D supplementation significantly reduced the risk of asthma exacerbation in children with baseline serum 25(OH)D of <10 ng/mL (RR = 0.48, 95% CI: 0.28 to 0.83, p = 0.009) (Table S3 in the Supplementary Materials). The quality of this evidence was downgraded to low due to imprecision and a high risk of bias (Table S2 in the Supplementary Materials). However, vitamin D supplementation did not result in a statistically significant reduction in asthma exacerbation risk in children with baseline 25(OH)D between 10 to 19 ng/mL (RR = 0.96, 95% CI: 0.74 to 1.24, I2 = 9%, p = 0.73) or children with baseline 25(OH)D between 20 to 29 ng/mL (RR = 1.10, 95% CI: 0.81 to 1.48, I2 = 0%, p = 0.56) (Table S3 in the Supplementary Materials). We also performed subgroup analyses by age, treatment duration, daily dose of vitamin D, bolus-dose vitamin D given, and concomitant treatment. P values for interaction for these subgroup analyses were higher than 0.05 and no significant protective effects of vitamin D supplementation were found within these subgroups (Table S3 in the Supplementary Materials).
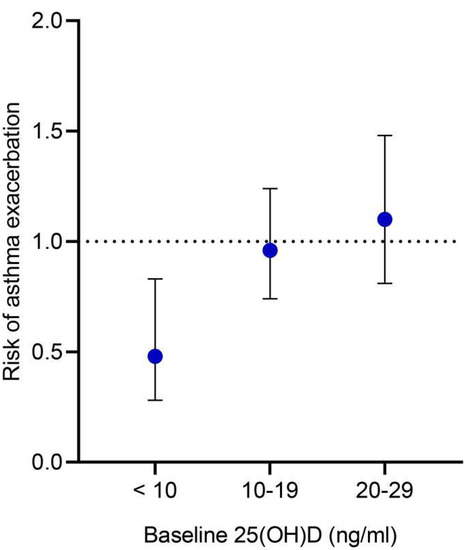
Figure 3.
Subgroup analysis of the number of children with one or more asthma exacerbations by baseline serum 25(OH)D concentration. Risk ratio and 95% confidence intervals are presented. Note: we were unable to assess the subgroup of children with baseline 25(OH)D levels ≥ 30 ng/mL because no trials exclusively enrolled those children. As a result, we only examined subgroups with baseline 25(OH)D levels of < 10 ng/mL, 10–19 ng/mL, and 20–29 ng/mL.
The effect of vitamin D supplementation on the primary outcome remained unchanged when we excluded the trials with a high risk of bias in a sensitivity analysis (RR = 0.88, 95% CI: 0.64 to 1.20, I2 = 40%, p = 0.43) (Figure S3 in the Supplementary Materials). A funnel plot and an Egger’s test (p = 0.137) did not observe publication bias in terms of the primary outcome (Figure S4 in the Supplementary Materials).
We also performed subgroup analyses of FEV1, FEV1/FVC, and total IgE in response to comments from reviewers. Similarly, we did not find protective effects of vitamin D supplementation on these outcomes in each subgroup (Tables S4–S6 in the Supplementary Materials).
3.4. Atopic Dermatitis
3.4.1. Overall Analysis
Eight studies with 483 patients reported the primary outcome. Overall, vitamin D supplementation significantly reduced AD severity assessed by the SCORAD or the EASI score compared with placebo (SMD = −0.5, 95% CI: −0.87 to −0.12, I2 = 73%, p = 0.009) (Figure 4). The quality of this evidence was downgraded to moderate due to inconsistency (Table S2 in the Supplementary Materials). Vitamin D supplementation also improved secondary outcomes. Two studies reported Staphylococcus aureus skin colonization [55,56]. Zulkarnain et al., found that the rate of Staphylococcus aureus skin colonization was significantly lower in the vitamin D supplementation group than in the placebo group [mean (standard deviation, SD): −793.1% (428.5%) vs. −161.5% (787.1%), p = 0.043] [56]. Udompataikul et al., found that the vitamin D supplementation group had a lower colony count of Staphylococcus aureus than those taking placebos at week 4 (p = 0.08) [55]. They also found that the erythema index of those with vitamin D supplement was statistically significantly lower than those with placebo (p = 0.01). Skin conductance was found to be lower in the vitamin D supplementation group, but the difference was not statistically significant (p = 0.08).
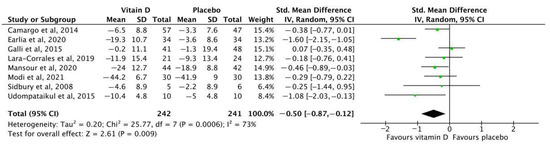
Figure 4.
Meta-analysis of the change in EASI or SCORAD before and after intervention among children with atopic dermatitis [48,49,50,51,52,53,54,55]. EASI: Eczema Area and Severity Index; SCORAD: Scoring Atopic Dermatitis.
3.4.2. Additional Analysis
We performed subgroup analyses of the primary outcome. Vitamin D supplementation significantly reduced atopic dermatitis severity in children with baseline serum 25(OH)D of less than 30 ng/mL (SMD = −0.40, 95% CI: −0.67 to −0.13, I2 = 0%, p = 0.004), but not in children with baseline serum 25(OH)D more than or equal to 30 ng/mL (SMD = 0.07, 95% CI: −0.35 to 0.48, p = 0.75) (Table S7 in the Supplementary Materials). However, the p value for interaction for this subgroup analysis was non-significant (Pinteraction = 0.07). The quality of this evidence was downgraded to moderate due to imprecision (Table S2 in the Supplementary Materials). Subgroup analyses by daily dose of vitamin D and bolus-dose vitamin D given did not reveal evidence of effect modification (Pinteraction > 0.05) (Table S7 in the Supplementary Materials).
The effect of vitamin D supplementation on the primary outcome remained unchanged when we excluded the trials with a high risk of bias (SMD = −0.55, 95% CI: −0.96 to −0.13, I2 = 72%, p = 0.01) and excluded the trials with missing data (SMD = −0.46, 95% CI: −0.88 to −0.04, I2 = 79%, p = 0.03) in the sensitivity analyses (Figure S5 in the Supplementary Materials).
3.5. Allergic Rhinitis
Four studies with 307 patients reported the outcomes of children with allergic rhinitis. Data from these studies could not be pooled because of high heterogeneity in the outcome reporting. Therefore, we performed a qualitative analysis. Jerzynska’s study in 2016 found that when compared with placebo group, the vitamin D group was more effective in the reduction of symptom-medication score (mean (SD): 43.7 (3.3) vs. 57.8 (4.4), p = 0.001), nasal symptoms (mean (SD): 17.3 (1.8) vs. 22.4 (2.5), p = 0.04), and asthma symptoms (mean (SD): 7.7 (1.0) vs. 12.8 (1.7), p = 0.001). No significant difference was found between the groups in medication (p = 0.211) and ocular scores (p = 0.149) [59]. Jerzynska’s study in 2018 found that the symptom-medication score was significantly lower in vitamin D supplementation group compared to placebo group (p = 0.0371) [60]. Akram et al. found that children with AR had a significant lower symptom score of rhinorrhea (p < 0.001), nasal congestion (p = 0.01), sneezing (p < 0.001), and itching (p = 0.016) in the vitamin D supplementation group than in the placebo group [57]. Hassan et al. found that improvement in the average morning and evening total nasal symptom scores was significantly greater in vitamin D supplementation group compared to placebo group (improved mean score: −0.61, 95% CI: −1.05 to −0.18) [58].
3.6. Serum 25(OH)D Concentration Levels
Twenty-one RCTs (n = 1545) reported the changes of serum 25(OH)D levels before and after intervention. The increase of serum 25(OH)D in children with vitamin D supplementation was significantly greater than that in the control group (MD = 16.84, 95% CI: 11.75 to 21.93, p < 0.001) (Figure S6 in the Supplementary Materials). However, after vitamin D supplementation, the mean serum 25(OH)D level of children with asthma was only 33.48 (95% CI: 27.94 to 39.02) ng/mL. The mean post-intervention serum 25(OH)D levels in children with atopic dermatitis and allergic rhinitis were 67.69 (95% CI: 47.19 to 88.19) ng/mL and 75.42 (95% CI: 30.90 to 119.93) ng/mL, respectively (Figure S7 in the Supplementary Materials).
3.7. Adverse Events
Two RCTs giving a bolus dose of 100,000 IU vitamin D reported that eight children had serum 25(OH)D levels greater than 90 ng/mL after taking vitamin D [32,33]. However, urinary Ca:Cr was normal in these children [32,33]. In one study, one child in the vitamin D group and one in the placebo group developed hypercalciuria [32]. No participant had hypercalcemia, renal stones, or suppressed parathyroid hormone. Vitamin D supplementation did not increase the risk of any non-serious or serious adverse events (Table S8 in the Supplementary Materials).
4. Discussion
In this meta-analysis, vitamin D supplementation did not reduce the risk of asthma exacerbation and did not improve asthma control and lung function in children overall but may reduce asthma exacerbation risk in children with serum 25(OH)D concentration less than 10 ng/mL. We also found that vitamin D supplementation can reduce the severity of AD in children, especially children with serum 25(OH)D concentration less than 30 ng/mL. In addition, vitamin D supplementation has been shown to significantly alleviate symptoms in children with allergic rhinitis. Vitamin D supplementation was safe and did not increase the risk of severe adverse events.
Our findings are consistent with those of a recently published meta-analysis, which did not find protective effects of vitamin D supplementation on reducing asthma exacerbation in children either [13]. There are many factors that contribute to the ineffectiveness of vitamin D supplementation in children with asthma. First and foremost, vitamin D supplementation may be effective in particular subgroups, rather than all children. Our subgroup analysis found a protective effect of vitamin D on asthmatic children with baseline 25(OH)D of less than 10 ng/mL, but not in patients with higher baseline 25(OH)D levels. A meta-analysis of individual participant data yielded the same results [11]. Although both meta-analyses found that vitamin D supplementation was effective in asthmatic patients with severe vitamin D deficiency, the sample size of this subgroup was small. More large-sample RCTs are required in the future to confirm this finding. In addition, the influence of vitamin D on childhood asthma may be affected by genetic differences in vitamin D metabolic pathways [61]. Some studies suggested that vitamin D may be more beneficial in severe steroid-resistant asthma and asthmatic children with obesity [62,63]. However, the influence of vitamin D supplementation in these subgroups could not be evaluated in our meta-analysis due to the unavailability of data. Additional large, rigorously designed RCTs in these fields are needed. A second reason may be inadequate vitamin D supplementation. Serum 25(OH)D concentrations more than 30 ng/mL are widely accepted to indicate vitamin D sufficiency [64]. However, this standard is suitable for bone health [64]. Some children with asthma still had recurrent attacks with serum 25(OH)D more than 30 ng/mL [65]. Thus, some experts suggest the optimum serum 25(OH)D level for allergic and inflammatory diseases should be above 40 ng/mL [24,66]. In our meta-analysis, after vitamin D supplementation, the mean serum 25(OH)D level of children with asthma was only 33.48 (95% CI: 27.94 to 39.02) ng/mL, which indicated that nearly half of the patients did not achieve serum 25(OH)D level of 30 ng/mL after vitamin D supplementation, and more than 95% of the patients did not achieve serum 25(OH)D level of 40 ng/mL. In contrast to RCTs on AD and AR, the pooled results of these RCTs showed vitamin D supplementation was effective, and accordingly, the mean serum 25(OH)D levels after vitamin D supplementation in these study populations were much higher than those in children with asthma and also higher than 40 ng/mL. Future RCTs should explore the effectiveness of vitamin D in children with asthma after adequate levels of 25(OH)D have been reached.
Consistent with our findings, vitamin D supplementation has shown to reduce the severity of AD in children in other meta-analyses [14,67,68,69]. However, the three previously published meta-analyses included both pediatric and adult patients [24,67,68]. A recently published meta-analysis only analyzed the results of four trials in pediatric patients and did not conduct subgroup analyses [14]. In our subgroup analysis, we saw a statistically significant reduction in AD severity with baseline 25(OH)D of less than or equal to 30 ng/mL, but not in participants with 25(OH)D of more than 30 ng/mL. However, the p value for interaction for this subgroup analysis was non-significant. Formally, we have not shown that effects are stronger in one group than in the other; alternatively, we might have lacked statistical power to detect the relevant interactions. Further research to clarify whether baseline vitamin D status modifies the effects of vitamin D on AD severity is needed.
There has been no SR evaluating the efficacy of vitamin D supplementation in children with AR. Our SR included four RCTs on children with AR and the results of each RCT showed that vitamin D supplementation significantly reduced the symptoms of AR patients [57,58,59,60]. However, some RCTs had design issues, such as not blinding participants and researchers and not properly addressing missing data [57,59,60]. In addition, we were unable to perform a quantitative analysis because of differences in outcomes between trials. Therefore, in the future, researchers need to design their trials in accordance with the Cochrane Risk-of-bias Tool for Randomized Trials [18] and investigate standardized and patient-relevant outcomes that are comparable across studies.
There has been no RCTs evaluating the efficacy of vitamin D supplementation in children with food allergies and anaphylaxis. Future research on these allergic diseases may be needed. P values for interaction were higher than 0.05 for subgroup analyses relating to vitamin D dosing regimen, treatment duration, and use of corticosteroids. Therefore, we did not find evidence that effects of vitamin D supplementation differed across these subgroups of patients. As a result, the optimum dose and treatment duration of vitamin D and the synergistic effects of vitamin D and corticosteroids are as yet unknown and require additional primary studies to determine.
We provided a comprehensive analysis of the effects of vitamin D supplementation on allergic diseases in children and compared the effects across allergic diseases and populations for the first time. However, we acknowledge several limitations of our study. First, there was variability in the population characteristics, intervention, and outcomes, which may lead to heterogeneity in results. Therefore, we pooled the data using a random-effects model. In addition, we performed subgroup analyses and sensitivity analyses and found the results remained unchanged and statistical heterogeneity was reduced. Second, we could not conduct some of the prespecified subgroup analyses because relevant information was not reported in the primary studies. Individual patient data meta-analysis of existing datasets is needed before definitive clinical recommendations can be made.
5. Conclusions
Vitamin D supplementation did not reduce the risk of asthma exacerbations in children overall but may reduce asthma exacerbation risk in children with serum 25(OH)D concentration less than 10 ng/mL. Vitamin D supplementation can safely reduce the severity of AD and symptoms of AR in children. Large-scale and well-designed RCTs are needed to confirm these conclusions and investigate the optimum regimen of vitamin D and the patients who would benefit most from vitamin D supplementation.
Supplementary Materials
The following supporting information can be downloaded online https://www.mdpi.com/article/10.3390/nu14193947/s1. Table S1: Search strategies, Table S2: GRADE assessment (Summary of Findings table), Table S3: Subgroup analyses of number of children with one or more asthma exacerbations, Table S4: Subgroup analyses of change in forced expiratory volume in the first second (FEV1) % predicted, Table S5: Subgroup analyses of change in FEV1/forced vital capacity (FVC) ratio; Table S6: Subgroup analyses of change in total IgE, Table S7: Subgroup analyses of atopic dermatitis severity, Table S8: Adverse events reported in the included RCTs, Figure S1: Assessment on risk of bias for included RCTs, Figure S2: Meta analyses of secondary outcomes among children with asthma, Figure S3: Sensitivity analyses of number of children with one or more asthma exacerbations, Figure S4: Publication bias of number of children with one or more asthma exacerbations, Figure S5: Sensitivity analyses of atopic dermatitis severity, Figure S6: Meta analyses of change in serum 25(OH)D concentration before and after intervention, Figure S7: Meta analyses of post-intervention serum 25(OH)D concentration in vitamin D group, Appendix S1: Methods [18,21,22].
Author Contributions
Conceptualization, Q.L., Q.Z. and Z.L.; methodology, Q.L., Q.Z. and Y.C.; validation, Z.L. and Y.C.; formal analysis, Q.L., Q.Z., G.Z., X.T., Y.L., Z.W. and Y.Z.; investigation, Q.L. and Q.Z.; resources, Q.L. and Q.Z.; data curation, Q.L., Q.Z., G.Z., X.T., Y.L., Z.W. and Y.Z.; writing—original draft preparation, Q.L. and Q.Z.; writing—review and editing, G.Z., X.T., Y.L., Z.W., Y.Z., Y.C. and Z.L.; visualization, Q.L. and Q.Z.; supervision, Z.L. and Y.C.; project administration, Z.L. and Y.C.; funding acquisition, Q.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Youth Project from National Clinical Research Center for Child Health and Disorders, grant number NCRCCHD-2021-YP-01, and the General Basic Research Project from the Ministry of Education Key Laboratory of Child Development and Disorders, grant number GBRP-202112.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank all the people who participated in the primary randomized controlled trials and the research teams who performed them.
Conflicts of Interest
All authors have completed the ICMJE uniform disclosure form. Qinyuan Li reports that she has received funds from the National Clinical Research Center for Child Health and Disorders (NCRCCHD-2021-YP-01) and Ministry of Education Key Laboratory of Child Development and Disorders (GBRP-202112). The other authors have no conflicts of interest to declare. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Dierick, B.J.H.; van der Molen, T.; Flokstra-de Blok, B.M.J.; Muraro, A.; Postma, M.J.; Kocks, J.W.H.; van Boven, J.F.M. Burden and socioeconomics of asthma, allergic rhinitis, atopic dermatitis and food allergy. Expert Rev. Pharm. Outcomes Res. 2020, 20, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Pawankar, R. Allergic diseases and asthma: A global public health concern and a call to action. World Allergy Organ. J. 2014, 7, 12. [Google Scholar] [CrossRef]
- Mirzakhani, H.; Al-Garawi, A.; Weiss, S.T.; Litonjua, A.A. Vitamin D and the development of allergic disease: How important is it? Clin. Exp. Allergy 2015, 45, 114–125. [Google Scholar] [CrossRef]
- Schrumpf, J.A.; van der Does, A.M.; Hiemstra, P.S. Impact of the Local Inflammatory Environment on Mucosal Vitamin D Metabolism and Signaling in Chronic Inflammatory Lung Diseases. Front. Immunol. 2020, 11, 1433. [Google Scholar] [CrossRef] [PubMed]
- Vasiliou, J.E.; Lui, S.; Walker, S.A.; Chohan, V.; Xystrakis, E.; Bush, A.; Hawrylowicz, C.M.; Saglani, S.; Lloyd, C.M. Vitamin D deficiency induces Th2 skewing and eosinophilia in neonatal allergic airways disease. Allergy 2014, 69, 1380–1389. [Google Scholar] [CrossRef]
- Rolf, L.; Muris, A.H.; Hupperts, R.; Damoiseaux, J. Vitamin D effects on B cell function in autoimmunity. Ann. N. Y. Acad. Sci. 2014, 1317, 84–91. [Google Scholar] [CrossRef]
- Kuruvilla, M.E.; Lee, F.E.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin. Rev. Allergy Immunol. 2019, 56, 219–233. [Google Scholar] [CrossRef]
- Han, Y.Y.; Forno, E.; Celedón, J.C. Vitamin D Insufficiency and Asthma in a US Nationwide Study. J. Allergy Clin. Immunol. Pract. 2017, 5, 790–796.e1. [Google Scholar] [CrossRef] [PubMed]
- Bunyavanich, S.; Rifas-Shiman, S.L.; Platts-Mills, T.A.; Workman, L.; Sordillo, J.E.; Camargo, C.A., Jr.; Gillman, M.W.; Gold, D.R.; Litonjua, A.A. Prenatal, perinatal, and childhood vitamin D exposure and their association with childhood allergic rhinitis and allergic sensitization. J. Allergy Clin. Immunol. 2016, 137, 1063–1070.e2. [Google Scholar] [CrossRef] [PubMed]
- Ahmed Mohamed, A.; Salah Ahmed, E.M.; Farag, Y.M.K.; Bedair, N.I.; Nassar, N.A.; Ghanem, A.I.M. Dose-response association between vitamin D deficiency and atopic dermatitis in children, and effect modification by gender: A case-control study. J. Dermatolog. Treat. 2021, 32, 174–179. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Griffiths, C.J.; Camargo, C.A., Jr.; Kerley, C.P.; Jensen, M.E.; Mauger, D.; Stelmach, I.; Urashima, M.; et al. Vitamin D supplementation to prevent asthma exacerbations: A systematic review and meta-analysis of individual participant data. Lancet Respir. Med. 2017, 5, 881–890. [Google Scholar] [CrossRef]
- Martineau, A.R.; Cates, C.J.; Urashima, M.; Jensen, M.; Griffiths, A.P.; Nurmatov, U.; Sheikh, A.; Griffiths, C.J. Vitamin D for the management of asthma. Cochrane Database Syst. Rev. 2016, 9, CD011511. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Kumar, P.; Goyal, J.P.; Thakur, C.; Choudhary, P.; Meena, J.; Charan, J.; Singh, K.; Gupta, A. Vitamin D supplementation in childhood asthma: A systematic review and meta-analysis of randomised controlled trials. ERJ Open Res. 2021, 8, 00662–02021. [Google Scholar] [CrossRef]
- Hidayati, A.N.; Sawitri, S.; Sari, D.W.; Prakoeswa, C.R.S.; Indramaya, D.M.; Damayanti, D.; Zulkarnain, I.; Citrashanty, I.; Widia, Y.; Anggraeni, S. Efficacy of vitamin D supplementation on the severity of atopic dermatitis in children: A systematic review and meta-analysis [version 1; peer review: 1 approved]. F1000Research 2022, 11, 274. [Google Scholar] [CrossRef]
- Tran, M.M.; Lefebvre, D.L.; Dharma, C.; Dai, D.; Lou, W.Y.W.; Subbarao, P.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; Sears, M.R. Predicting the atopic march: Results from the Canadian Healthy Infant Longitudinal Development Study. J. Allergy Clin. Immunol. 2018, 141, 601–607.e8. [Google Scholar] [CrossRef] [PubMed]
- Giovannini-Chami, L.; Paquet, A.; Sanfiorenzo, C.; Pons, N.; Cazareth, J.; Magnone, V.; Lebrigand, K.; Chevalier, B.; Vallauri, A.; Julia, V.; et al. The “one airway, one disease” concept in light of Th2 inflammation. Eur. Respir. J. 2018, 52, 1800437. [Google Scholar] [CrossRef]
- Lenaeus, M.J.; Hirschmann, J. Primary Care of the Patient with Asthma. Med. Clin. N. Am. 2015, 99, 953–967. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Davidson, B.L. Administration of placebo vitamin D to non-consenting children. Lancet Respir. Med. 2018, 6, e23–e24. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Santesso, N.; Helfand, M.; Vist, G.; Kunz, R.; Brozek, J.; Norris, S.; Meerpohl, J.; Djulbegovic, B.; et al. GRADE guidelines: 12. Preparing summary of findings tables-binary outcomes. J. Clin. Epidemiol. 2013, 66, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0, an update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Cashman, K.D.; Fitzgerald, A.P.; Kiely, M.; Seamans, K.M. A systematic review and meta-regression analysis of the vitamin D intake-serum 25-hydroxyvitamin D relationship to inform European recommendations. Br. J. Nutr. 2011, 106, 1638–1648. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed]
- Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellof, M.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Vitamin D in the healthy European paediatric population. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 692–701. [Google Scholar] [CrossRef]
- Alansari, K.; Davidson, B.L.; Yousef, K.I.; Mohamed, A.N.H.; Alattar, I. Rapid vs. Maintenance Vitamin D Supplementation in Deficient Children With Asthma to Prevent Exacerbations. Chest 2017, 152, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Bar Yoseph, R.; Livnat, G.; Schnapp, Z.; Hakim, F.; Dabbah, H.; Goldbart, A.; Bentur, L. The effect of vitamin D on airway reactivity and inflammation in asthmatic children: A double-blind placebo-controlled trial. Pediatr. Pulmonol. 2015, 50, 747–753. [Google Scholar] [CrossRef]
- Baris, S.; Kiykim, A.; Ozen, A.; Tulunay, A.; Karakoc-Aydiner, E.; Barlan, I.B. Vitamin D as an adjunct to subcutaneous allergen immunotherapy in asthmatic children sensitized to house dust mite. Allergy 2014, 69, 246–253. [Google Scholar] [CrossRef]
- Jensen, M.E.; Mailhot, G.; Alos, N.; Rousseau, E.; White, J.H.; Khamessan, A.; Ducharme, F.M. Vitamin D intervention in preschoolers with viral-induced asthma (DIVA): A pilot randomised controlled trial. Trials 2016, 17, 353. [Google Scholar] [CrossRef]
- Ducharme, F.M.; Jensen, M.; Mailhot, G.; Alos, N.; White, J.; Rousseau, E.; Tse, S.M.; Khamessan, A.; Vinet, B. Impact of two oral doses of 100,000 IU of vitamin D3 in preschoolers with viral-induced asthma: A pilot randomised controlled trial. Trials 2019, 20, 138. [Google Scholar] [CrossRef] [PubMed]
- El-korashi, L.A.; Nafea, O.E.; Zake, L.G.; Arab, F.; Anis, R.H. Effect of Vitamin D Adjuvant and Allergen Specific Immunotherapy on Serum IL-10 and IL-17 Levels in Childhood Asthma: A Controlled Clinical Trial. Egypt J. Med. Microbiol. 2021, 30, 175–181. [Google Scholar] [CrossRef]
- Jat, K.R.; Goel, N.; Gupta, N.; Gupta, C.P.; Datta, S.; Lodha, R.; Kabra, S.K. Efficacy of vitamin D supplementation in asthmatic children with vitamin D deficiency: A randomized controlled trial (ESDAC trial). Pediatr. Allergy Immunol. 2021, 32, 479–488. [Google Scholar] [CrossRef]
- Kerley, C.P.; Hutchinson, K.; Cormican, L.; Faul, J.; Greally, P.; Coghlan, D.; Elnazir, B. Vitamin D3 for uncontrolled childhood asthma: A pilot study. Pediatr. Allergy Immunol. 2016, 27, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.; Fernandez, C.; Nella, A.; Hopp, R.; Gallagher, J.C.; Casale, T.B. Relationship of 25-hydroxyvitamin D and asthma control in children. Ann. Allergy Asthma Immunol. 2012, 108, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Majak, P.; Rychlik, B.; Stelmach, I. The effect of oral steroids with and without vitamin D3 on early efficacy of immunotherapy in asthmatic children. Clin. Exp. Allergy 2009, 39, 1830–1841. [Google Scholar] [CrossRef] [PubMed]
- Majak, P.; Olszowiec-Chlebna, M.; Smejda, K.; Stelmach, I. Vitamin D supplementation in children may prevent asthma exacerbation triggered by acute respiratory infection. J. Allergy Clin. Immunol. 2011, 127, 1294–1296. [Google Scholar] [CrossRef] [PubMed]
- Najmuddin, F.; Lahiri, K. Vitamin D in pediatric asthma and allergic rhinitis: Benefits beyond skeletal health. Insights Allergy Asthma Bronchitis 2017, 3, 1. [Google Scholar] [CrossRef][Green Version]
- Swangtrakul, N.; Manuyakorn, W.; Mahachoklertwattana, P.; Kiewngam, P.; Sasisakulporn, C.; Jotikasthirapa, W.; Kamchaisatian, W.; Benjaponpitak, S. Effect of vitamin D on lung function assessed by forced oscillation technique in asthmatic children with vitamin D deficiency: A randomized double-blind placebo-controlled trial. Asian Pac. J. Allergy Immunol. 2022, 40, 22–30. [Google Scholar] [PubMed]
- Tachimoto, H.; Mezawa, H.; Segawa, T.; Akiyama, N.; Ida, H.; Urashima, M. Improved control of childhood asthma with low-dose, short-term vitamin D supplementation: A randomized, double-blind, placebo-controlled trial. Allergy 2016, 71, 1001–1009. [Google Scholar] [CrossRef]
- Urashima, M.; Segawa, T.; Okazaki, M.; Kurihara, M.; Wada, Y.; Ida, H. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am. J. Clin. Nutr. 2010, 91, 1255–1260. [Google Scholar] [CrossRef]
- Forno, E.; Bacharier, L.B.; Phipatanakul, W.; Guilbert, T.W.; Cabana, M.D.; Ross, K.; Covar, R.; Gern, J.E.; Rosser, F.J.; Blatter, J. Effect of Vitamin D3 Supplementation on Severe Asthma Exacerbations in Children With Asthma and Low Vitamin D Levels: The VDKA Randomized Clinical Trial. JAMA 2020, 324, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Thakur, C.; Kumar, J.; Kumar, P.; Goyal, J.P.; Singh, K.; Gupta, A. Vitamin-D supplementation as an adjunct to standard treatment of asthma in children: A randomized controlled trial (ViDASTA Trial). Pediatr. Pulmonol. 2021, 56, 1427–1433. [Google Scholar] [CrossRef]
- Yadav, M.; Mittal, K. Effect of vitamin D supplementation on moderate to severe bronchial asthma. Indian J. Pediatr. 2014, 81, 650–654. [Google Scholar] [CrossRef]
- Aldaghi, M.; Tehrani, H.; Karrabi, M.; Abadi, F.S.; Sahebkar, M. The effect of multistrain synbiotic and vitamin D3 supplements on the severity of atopic dermatitis among infants under 1 year of age: A double-blind, randomized clinical trial study. J. Dermatol. Treat. 2022, 33, 812–817. [Google Scholar] [CrossRef]
- Camargo, C.A., Jr.; Ganmaa, D.; Sidbury, R.; Erdenedelger Kh Radnaakhand, N.; Khandsuren, B. Randomized trial of vitamin D supplementation for winter-related atopic dermatitis in children. J. Allergy Clin. Immunol. 2014, 134, 831–835.e1. [Google Scholar] [CrossRef] [PubMed]
- Earlia, N.; Maulida, M.; Hidayati, A.; Pratama, R. Pengaruh Pemberian Vitamin D Terhadap Perbaikan Gejala Klinis Pada Penderita Dermatitis Atopik Di Poliklinik Kulit Kelamin RSUD Dr. Zainoel Abidin Banda Aceh Tahun 2018: Uji Klinis Ketersamaran Ganda. J. Med. Sci. 2020, 1, 33–42. [Google Scholar] [CrossRef]
- Galli, E.; Rocchi, L.; Carello, R.; Giampietro, P.G.; Panei, P.; Meglio, P. Serum Vitamin D levels and Vitamin D supplementation do not correlate with the severity of chronic eczema in children. Eur. Ann. Allergy Clin. Immunol. 2015, 47, 41–47. [Google Scholar] [PubMed]
- Lara-Corrales, I.; Huang, C.M.; Parkin, P.C.; Rubio-Gomez, G.A.; Posso-De Los Rios, C.J.; Maguire, J.; Pope, E. Vitamin D Level and Supplementation in Pediatric Atopic Dermatitis: A Randomized Controlled Trial. J. Cutan. Med. Surg. 2019, 23, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Mansour, N.O.; Mohamed, A.A.; Hussein, M.; Eldemiry, E.; Daifalla, A.; Hassanin, S.; Nassar, N.; Ghaith, D.; Mohamed Salah, E. The impact of vitamin D supplementation as an adjuvant therapy on clinical outcomes in patients with severe atopic dermatitis: A randomized controlled trial. Pharmacol. Res. Perspect. 2020, 8, e00679. [Google Scholar] [CrossRef] [PubMed]
- Modi, N.P.; Dash, A.K. Clinico-biochemical relation of Vitamin D3 with the severity of atopic dermatitis and response to supplementation of Vitamin D3: A randomized controlled trial. Ind. J. Child. Health 2021, 8, 412–415. [Google Scholar] [CrossRef]
- Sidbury, R.; Sullivan, A.F.; Thadhani, R.I.; Camargo, C.A., Jr. Randomized controlled trial of vitamin D supplementation for winter-related atopic dermatitis in Boston: A pilot study. Br. J. Dermatol. 2008, 159, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Udompataikul, M.; Huajai, S.; Chalermchai, T.; Taweechotipatr, M.; Kamanamool, N. The Effects of Oral Vitamin D Supplement on Atopic Dermatitis: A Clinical Trial with Staphylococcus aureus Colonization Determination. J. Med. Assoc. Thail. 2015, 98 (Suppl. 9), S23–S30. [Google Scholar]
- Zulkarnain, I.; Rahmawati, Y.W.; Setyaningrum, T.; Citrashanty, I.; Aditama, L.; Avanti, C. Vitamin D3 supplementation reduced Staphylococcus aureus colonization in the skin of pediatric patients with atopic dermatitis. Eur. J. Pediatr. Dermatol. 2019, 29, 143–149. [Google Scholar]
- Akram, S.; Khan, M.A.; Fazil, M.; Kiramatullah Khan, M.Q.; Shah, H.B.U. Effect of Vitamin-D Supplementation in Children with Moderate-Severe Persistent Allergic Rhinitis. Int. J. Pathol. 2020, 18, 92–98. [Google Scholar]
- Hassan, S.M.; Elmageed, M.M.A.; Senosy, M.G.E. Vitamin D Intervention in Children with Allergic rhinitis: A Pilot Randomized Controlled Trial. Int. J. Curr. Microbiol. Appl. Sci. 2016, 5, 544–550. [Google Scholar] [CrossRef][Green Version]
- Jerzynska, J.; Stelmach, W.; Rychlik, B.; Lechańska, J.; Podlecka, D.; Stelmach, I. The clinical effect of vitamin D supplementation combined with grass-specific sublingual immunotherapy in children with allergic rhinitis. Allergy Asthma Proc. 2016, 37, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Jerzyńska, J.; Stelmach, W.; Rychlik, B.; Majak, P.; Podlecka, D.; Woicka-Kolejwa, K.; Stelmach, I. Clinical and immunological effects of vitamin D supplementation during the pollen season in children with allergic rhinitis. Arch. Med. Sci. 2018, 14, 122–131. [Google Scholar] [CrossRef]
- Zhao, D.D.; Yu, D.D.; Ren, Q.Q.; Dong, B.; Zhao, F.; Sun, Y.H. Association of vitamin D receptor gene polymorphisms with susceptibility to childhood asthma: A meta-analysis. Pediatr. Pulmonol. 2017, 52, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Nanzer, A.M.; Chambers, E.S.; Ryanna, K.; Freeman, A.T.; Colligan, G.; Richards, D.F.; Timms, P.M.; Martineau, A.R.; Griffiths, C.J.; Corrigan, C.J.; et al. The effects of calcitriol treatment in glucocorticoid-resistant asthma. J. Allergy Clin. Immunol. 2014, 133, 1755–1757.e4. [Google Scholar] [CrossRef] [PubMed]
- Bose, S.; Diette, G.B.; Woo, H.; Koehler, K.; Romero, K.; Rule, A.M.; Detrick, B.; Brigham, E.; McCormack, M.C.; Hansel, N.N. Vitamin D Status Modifies the Response to Indoor Particulate Matter in Obese Urban Children with Asthma. J. Allergy Clin. Immunol. Pract. 2019, 7, 1815–1822.e2. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Sun, Y.; Zeng, Z.; Liu, Y.; Peng, S. Vitamin D supplementation in pregnant women or infants for preventing allergic diseases: A systematic review and meta-analysis of randomized controlled trials. Chin. Med. J. 2022, 135, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W.; Wagner, C.L.; Drezner, M.K.; Binkley, N.C. Circulating vitamin D3 and 25-hydroxyvitamin D in humans: An important tool to define adequate nutritional vitamin D status. J. Steroid Biochem. Mol. Biol. 2007, 103, 631–634. [Google Scholar] [CrossRef]
- Hattangdi-Haridas, S.R.; Lanham-New, S.A.; Wong, W.H.S.; Ho, M.H.K.; Darling, A.L. Vitamin D Deficiency and Effects of Vitamin D Supplementation on Disease Severity in Patients with Atopic Dermatitis: A Systematic Review and Meta-Analysis in Adults and Children. Nutrients 2019, 11, 1854. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Kim, S.N.; Lee, Y.W.; Choe, Y.B.; Ahn, K.J. Vitamin D Status and Efficacy of Vitamin D Supplementation in Atopic Dermatitis: A Systematic Review and Meta-Analysis. Nutrients 2016, 8, 789. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Bae, J.H. Vitamin D and atopic dermatitis: A systematic review and meta-analysis. Nutrition 2016, 32, 913–920. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).