
Validity of the Food Frequency Questionnaire—Estimated Intakes of Sodium, Potassium, and Sodium-to-Potassium Ratio for Screening at a Point of Absolute Intake among Middle-Aged and Older Japanese Adults

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Ethics Approval and Consent to Participate
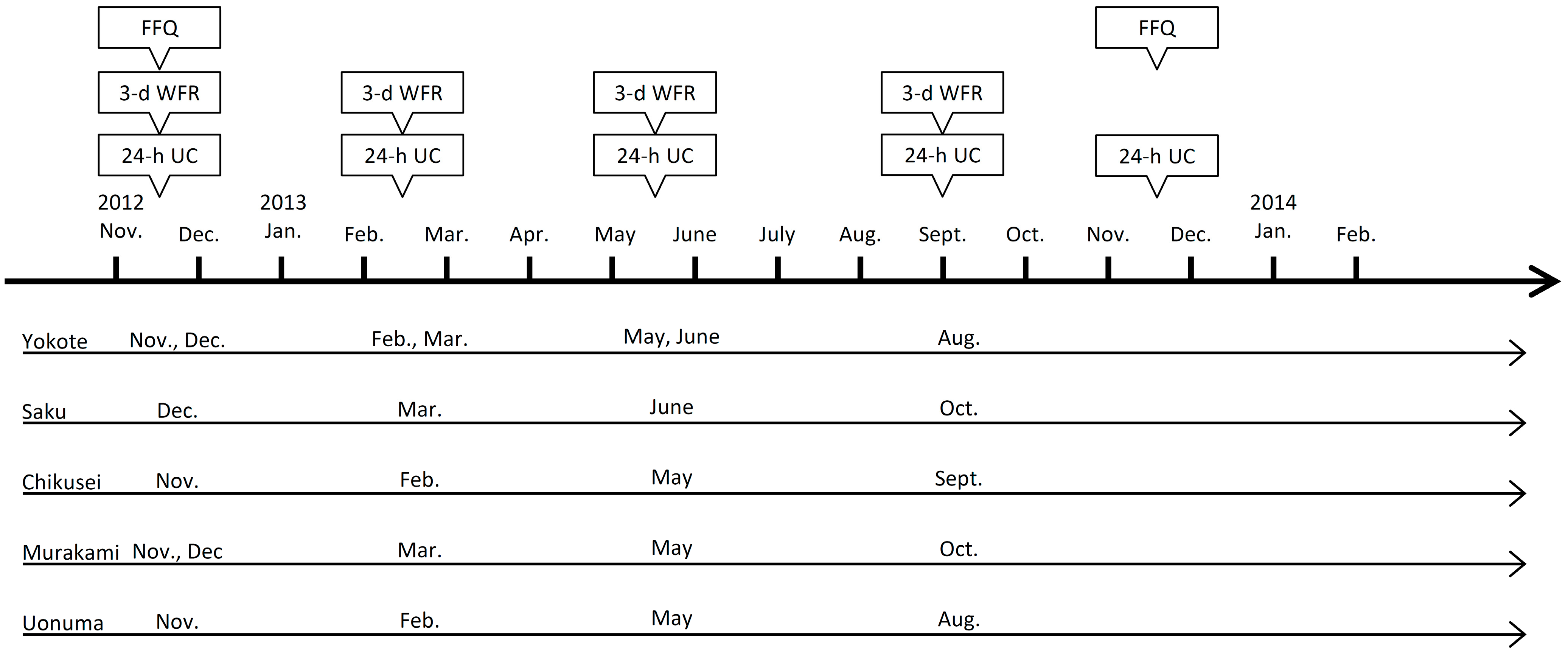
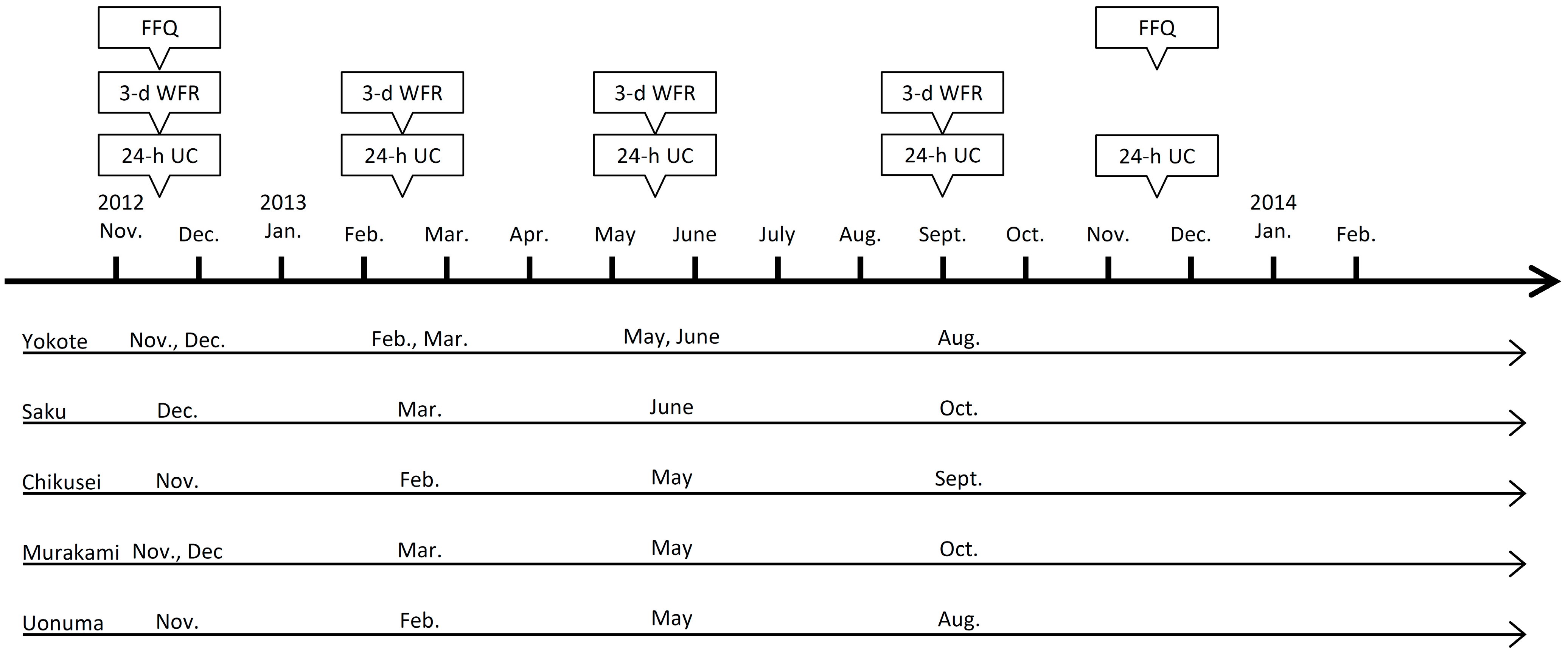
2.3. Data Collection and Time Window
2.4. 12-d WFR
2.5. 24-h Urinary Collection
2.6. FFQs
2.7. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Correlation between Intake Estimated Using the FFQ and That Using 12-d WFR or 24-h Urinary Excretion
3.3. Validity of the Absolute Intake Estimated Using the FFQ to Determine the DRIs Compared with That of 12-d WFR or 24-h Urinary Excretion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Wakai, K. A review of food frequency questionnaires developed and validated in Japan. J. Epidemiol. 2009, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoyama, Y.; Takachi, R.; Ishihara, J.; Ishii, Y.; Sasazuki, S.; Sawada, N.; Shinozawa, Y.; Tanaka, J.; Kato, E.; Kitamura, K.; et al. Validity of Short and Long Self-Administered Food Frequency Questionnaires in Ranking Dietary Intake in Middle-Aged and Elderly Japanese in the Japan Public Health Center-Based Prospective Study for the Next Generation (JPHC-NEXT) Protocol Area. J. Epidemiol. 2016, 26, 420–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimm, E.B.; Giovannucci, E.L.; Stampfer, M.J.; Colditz, G.A.; Litin, L.B.; Willett, W.C. Reproducibility and validity of an expanded self-administered semiquantitative food frequency questionnaire among male health professionals. Am. J. Epidemiol. 1992, 135, 1114–1126. [Google Scholar] [CrossRef] [PubMed]
- Mori, N.; Sawada, N.; Ishihara, J.; Kotemori, A.; Takachi, R.; Murai, U.; Kobori, M.; Tsugane, S. Validity of a food frequency questionnaire for the estimation of total polyphenol intake estimates and its major food sources in the Japanese population: The JPHC FFQ Validation Study. J. Nutr. Sci. 2021, 10, e35. [Google Scholar] [CrossRef] [PubMed]
- Intersalt Cooperative Research Group. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. BMJ 1988, 297, 319–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Cogswell, M.E.; Gillespie, C.; Fang, J.; Loustalot, F.; Dai, S.; Carriquiry, A.L.; Kuklina, E.V.; Hong, Y.; Merritt, R.; et al. Association between usual sodium and potassium intake and blood pressure and hypertension among U.S. adults: NHANES 2005–2010. PLoS ONE 2013, 8, e75289. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; He, F.J.; Sun, Q.; Yuan, C.; Kieneker, L.M.; Curhan, G.C.; MacGregor, G.A.; Bakker, S.J.L.; Campbell, N.R.C.; Wang, M.; et al. 24-Hour Urinary Sodium and Potassium Excretion and Cardiovascular Risk. N. Engl. J. Med. 2022, 386, 252–263. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare. The National Health and Nutrition Survey in Japan (2019). Available online: https://www.mhlw.go.jp/content/000710991.pdf (accessed on 15 March 2022). (In Japanese)
- World Health Organization. Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting, Paris, France, 5–7 October 2006; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Perez, V.; Chang, E.T. Sodium-to-potassium ratio and blood pressure, hypertension, and related factors. Adv. Nutr. 2014, 5, 712–741. [Google Scholar] [CrossRef]
- Iwahori, T.; Miura, K.; Ueshima, H. Time to Consider Use of the Sodium-to-Potassium Ratio for Practical Sodium Reduction and Potassium Increase. Nutrients 2017, 9, 700. [Google Scholar] [CrossRef]
- Stamler, J.; Rose, G.; Stamler, R.; Elliott, P.; Dyer, A.; Marmot, M. INTERSALT study findings. Public health and medical care implications. Hypertension 1989, 14, 570–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cappuccio, F.P.; Sever, P.S. The importance of a valid assessment of salt intake in individuals and populations. A scientific statement of the British and Irish Hypertension Society. J. Hum. Hypertens. 2019, 33, 345–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Center. The Japan Public Health Center-based prospective Study for the Next Generation (JPHC-NEXT). Available online: http://epi.ncc.go.jp/jphcnext/ (accessed on 15 March 2022).
- Tanaka, T.; Okamura, T.; Miura, K.; Kadowaki, T.; Ueshima, H.; Nakagawa, H.; Hashimoto, T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J. Hum. Hypertens. 2002, 16, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turck, D.; Bresson, J.-L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; Mangelsdorf, I.; McArdle, H.; Neuhäuser-Berthold, M.; et al. Dietary reference values for potassium. EFSA J. 2016, 14, e04592. [Google Scholar] [CrossRef]
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck, D.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; et al. Dietary reference values for sodium. EFSA J. 2019, 17, e05778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucko, A.M.; Doktorchik, C.; Woodward, M.; Cogswell, M.; Neal, B.; Rabi, D.; Anderson, C.; He, F.J.; MacGregor, G.A.; L’Abbe, M.; et al. Percentage of ingested sodium excreted in 24-hour urine collections: A systematic review and meta-analysis. J. Clin. Hypertens. (Greenwich) 2018, 20, 1220–1229. [Google Scholar] [CrossRef] [Green Version]
- McLean, R.M.; Farmer, V.L.; Nettleton, A.; Cameron, C.M.; Cook, N.R.; Campbell, N.R.C. Assessment of dietary sodium intake using a food frequency questionnaire and 24-hour urinary sodium excretion: A systematic literature review. J. Clin. Hypertens. (Greenwich) 2017, 19, 1214–1230. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare. Dietary Reference Intakes for Japanese. 2020. Available online: https://www.mhlw.go.jp/content/10904750/000586553.pdf (accessed on 15 March 2022). (In Japanese)
- Tsubono, Y.; Ogawa, K.; Watanabe, Y.; Nishino, Y.; Tsuji, I.; Watanabe, T.; Nakatsuka, H.; Takahashi, N.; Kawamura, M.; Hisamichi, S. Food frequency questionnaire and a screening test. Nutr. Cancer 2001, 39, 78–84. [Google Scholar] [CrossRef]
- Kelly, C.; Geaney, F.; Fitzgerald, A.P.; Browne, G.M.; Perry, I.J. Validation of diet and urinary excretion derived estimates of sodium excretion against 24-h urine excretion in a worksite sample. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 771–779. [Google Scholar] [CrossRef]
- Sasaki, S.; Takada, T.; Fukuma, S.; Imamoto, M.; Hasegawa, T.; Nishiwaki, H.; Iida, H.; Fukuhara, S. Screening tool for identifying adults with excessive salt intake among community-dwelling adults: A population-based cohort study. Am. J. Clin. Nutr. 2020, 111, 814–820. [Google Scholar] [CrossRef]
- Monntoya, L.M.; Ducher, M.; Florens, N.; Fauvel, J.P. Evaluation of the ExSel® self-questionnaire to screen for an excess salt intake in patients followed in a nephrology consultation. Ann. Cardiol. Angeiol. (Paris) 2019, 68, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Mason, B.; Ross, L.; Gill, E.; Healy, H.; Juffs, P.; Kark, A. Development and validation of a dietary screening tool for high sodium consumption in Australian renal patients. J. Ren. Nutr. 2014, 24, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Ishihara, J.; Tsugane, S. Validity of a self-administered food frequency questionnaire in the 5-year follow-up survey of the JPHC Study Cohort I to assess sodium and potassium intake: Comparison with dietary records and 24-hour urinary excretion level. J. Epidemiol. 2003, 13, S102–S105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. The National Health and Nutrition Survey in Japan (2012). Available online: http://www.e-stat.go.jp/SG1/estat/GL08020103.do?_toGL08020103_&listID=000001118468&requestSender=dsearch (accessed on 15 March 2022). (In Japanese)
- Sun, Q.; Bertrand, K.A.; Franke, A.A.; Rosner, B.; Curhan, G.C.; Willett, W.C. Reproducibility of urinary biomarkers in multiple 24-h urine samples. Am. J. Clin. Nutr. 2017, 105, 159–168. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Men | Women | |||
|---|---|---|---|---|
| Age, years * | 57.3 | (8.6) | 57.1 | (8.5) |
| Body height, cm * | 168.3 | (6.9) | 156.6 | (5.7) |
| Body weight, kg * | 67.3 | (9.2) | 56.0 | (8.0) |
| BMI, kg/m² * | 23.7 | (2.8) | 22.8 | (3.1) |
| Current smoker, % | 25.5 | 1.4 | ||
| Heavy drinker, % † | 40.4 | 5.0 | ||
| CCs Compared with | Cross-Classification | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | (SD) | Median | Interquartile Range | 24-h Urinary Excretion | 12-d WFR | vs. 24-h Urine (%) || | ||||
| Same/ | Extreme | |||||||||
| Crude | Adjusted *,† | Crude | Adjusted *,† | Adjacent | ||||||
| Men (n = 94) | ||||||||||
| Sodium, mg | ||||||||||
| 24-h urine | 4650 | (1196) | 4589 | 3896–5350 | - | - | - | - | - | - |
| 12-d WFR | 4579 | (1112) | 4453 | 3748–5283 | 0.61 | 0.55 | - | - | 70 | 0 |
| FFQ | 4378 | (2061) | 3918 | 2897–5529 | 0.33 | 0.36 | 0.37 | 0.33 | 67 | 3 |
| Potassium, mg ‡ | ||||||||||
| 24-h urine | 2944 | (874) | 2832 | 2332–3433 | - | - | - | - | - | - |
| 12-d WFR | 3113 | (902) | 3085 | 2527–3606 | 0.62 | 0.52 | - | - | 68 | 2 |
| FFQ | 3182 | (1286) | 2944 | 2253–3939 | 0.26 | 0.38 | 0.43 | 0.49 | 71 | 4 |
| Na/K ratio §, mmol/mmol | ||||||||||
| 24-h urine | 3.68 | (1.12) | 3.42 | 2.86–4.40 | - | - | - | - | - | - |
| 12-d WFR | 3.37 | (0.80) | 3.35 | 2.76–3.74 | 0.70 | 0.76 | - | - | 79 | 0 |
| FFQ | 3.04 | (0.81) | 2.96 | 2.50–3.56 | 0.30 | 0.32 | 0.22 | 0.24 | 65 | 5 |
| Women (n = 141) | ||||||||||
| Sodium, mg | ||||||||||
| 24-h urine | 3922 | (989) | 3738 | 3336–4540 | - | - | - | - | - | - |
| 12-d WFR | 3807 | (924) | 3697 | 3155–4314 | 0.64 | 0.71 | - | - | 75 | 0 |
| FFQ | 4508 | (2060) | 4031 | 3063–5833 | 0.17 | 0.26 | 0.30 | 0.41 | 62 | 7 |
| Potassium, mg ‡ | ||||||||||
| 24-h urine | 3028 | (900) | 2956 | 2354–3607 | - | - | - | - | - | - |
| 12-d WFR | 2979 | (792) | 2949 | 2389–3454 | 0.63 | 0.67 | - | - | 79 | 1 |
| FFQ | 3631 | (1573) | 3170 | 2479–4776 | 0.35 | 0.30 | 0.48 | 0.54 | 62 | 4 |
| Na/K ratio §, mmol/mmol | ||||||||||
| 24-h urine | 3.03 | (0.91) | 2.99 | 2.33–3.55 | - | - | - | - | - | - |
| 12-d WFR | 2.91 | (0.71) | 2.87 | 2.41–3.26 | 0.79 | 0.87 | - | - | 88 | 0 |
| FFQ | 2.78 | (0.67) | 2.74 | 2.32–3.07 | 0.27 | 0.30 | 0.39 | 0.42 | 62 | 4 |
| Criteria Based on DRIs | n * | AUC (95% CI) | Cutoff Values in the FFQ | %Dif † | At Cutoff Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sensitivity, % | Specificity, % | Youden’s Index | Distance to Corner | |||||||
| Salt equivalent | ||||||||||
| Multiple 24-h urinary excretion as reference standard | ||||||||||
| men (n = 94) | ||||||||||
| DG | ≥7.5 g | 87 | 0.76 | (0.56–0.95) | 7.48 | −0.2 | 75 | 71 | 0.46 | 0.38 |
| 9.32 | 24.3 | 63 | 86 | 0.49 | 0.39 | |||||
| Women (n = 141) | ||||||||||
| DG | ≥6.5 g | 134 | 0.60 | (0.37–0.82) | 6.55 | 0.8 | 85 | 29 | 0.14 | 0.73 |
| 9.93 | 52.8 | 54 | 71 | 0.26 | 0.54 | |||||
| 12-d WFR as reference standard | ||||||||||
| men (n = 94) | ||||||||||
| DG | ≥7.5 g | 88 | 0.80 | (0.62–0.98) | 7.48 | −0.2 | 74 | 67 | 0.41 | 0.42 |
| 7.40 | −1.4 | 76 | 67 | 0.43 | 0.41 | |||||
| Women (n = 141) | ||||||||||
| DG | ≥6.5 g | 131 | 0.71 | (0.50–0.91) | 6.55 | 0.8 | 86 | 40 | 0.26 | 0.62 |
| 6.90 | 6.2 | 86 | 60 | 0.46 | 0.42 | |||||
| Potassium ‡ | ||||||||||
| Multiple 24-h urinary excretion as reference standard | ||||||||||
| Men (n = 94) | ||||||||||
| AI | <2500 mg | 34 | 0.60 | (0.47–0.73) | 2475 | −1.0 | 50 | 73 | 0.23 | 0.57 |
| 2591 | 3.6 | 56 | 72 | 0.28 | 0.52 | |||||
| DG | <3000 mg | 57 | 0.66 | (0.55–0.77) | 3025 | 0.8 | 61 | 57 | 0.18 | 0.58 |
| 2817 | −6.1 | 60 | 70 | 0.30 | 0.50 | |||||
| Women (n = 141) | ||||||||||
| AI | <2000 mg | 14 | 0.71 | (0.54–0.87) | 1991 | −0.5 | 36 | 90 | 0.25 | 0.65 |
| 2625 | 31.2 | 71 | 75 | 0.46 | 0.38 | |||||
| DG | <2600 mg | 47 | 0.68 | (0.58–0.77) | 2609 | 0.3 | 45 | 79 | 0.23 | 0.59 |
| 2970 | 14.2 | 64 | 67 | 0.31 | 0.49 | |||||
| 12-d WFR as reference standard | ||||||||||
| Men (n = 94) | ||||||||||
| AI | <2500 mg | 23 | 0.73 | (0.61–0.85) | 2475 | −1.0 | 61 | 73 | 0.34 | 0.47 |
| 2452 | −1.9 | 61 | 76 | 0.37 | 0.46 | |||||
| DG | <3000 mg | 44 | 0.71 | (0.60–0.81) | 3025 | 0.8 | 66 | 56 | 0.22 | 0.56 |
| 2591 | −13.6 | 57 | 78 | 0.35 | 0.48 | |||||
| Women (n = 141) | ||||||||||
| AI | <2000 mg | 8 | 0.72 | (0.57–0.86) | 1991 | −0.5 | 25 | 88 | 0.13 | 0.76 |
| 2837 | 41.8 | 75 | 62 | 0.37 | 0.45 | |||||
| DG | <2600 mg | 48 | 0.76 | (0.68–0.85) | 2609 | 0.3 | 52 | 83 | 0.35 | 0.51 |
| 2874 | 10.5 | 71 | 74 | 0.45 | 0.39 | |||||
| Na/K ratio § | ||||||||||
| Men and women (n = 235) | ||||||||||
| Multiple 24-h urinary excretion as reference standard | ||||||||||
| -- | ≥2.00 | 215 | 0.59 | (0.48–0.70) | 2.01 | 0.5 | 91 | 10 | 0.01 | 0.90 |
| mmol/mmol | 3.00 | 49.8 | 40 | 85 | 0.25 | 0.61 | ||||
| 12-d WFR as reference standard | ||||||||||
| -- | ≥2.00 | 224 | 0.57 | (0.39–0.75) | 2.01 | 0.5 | 91 | 18 | 0.09 | 0.82 |
| mmol/mmol | 2.55 | 27.3 | 69 | 45 | 0.15 | 0.63 | ||||
| Criteria Based on DRIs | n † | AUC (95% CI) | Cutoffs in the 12-d WFR | %Dif ‡ | At Cutoff Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sensitivity, % | Specificity, % | Youden’s Index | Distance to Corner | |||||||
| Salt equivalent | ||||||||||
| Men (n = 94) | ||||||||||
| DG | ≥7.5 g | 87 | 0.90 | (0.83–0.97) | 7.51 | 0.1 | 95 | 29 | 0.24 | 0.72 |
| 9.30 | 24.0 | 83 | 86 | 0.68 | 0.22 | |||||
| women (n = 141) | ||||||||||
| DG | ≥6.5 g | 134 | 0.84 | (0.75–0.93) | 6.46 | −0.7 | 94 | 14 | 0.08 | 0.86 |
| 8.41 | 29.3 | 72 | 86 | 0.57 | 0.32 | |||||
| Potassium § | ||||||||||
| Men (n = 94) | ||||||||||
| AI | <2500 mg | 34 | 0.78 | (0.67–0.88) | 2527 | 1.1 | 53 | 90 | 0.43 | 0.48 |
| 2879 | 15.2 | 74 | 77 | 0.50 | 0.35 | |||||
| DG | <3000 mg | 57 | 0.82 | (0.74–0.91) | 3000 | 0.0 | 67 | 81 | 0.48 | 0.38 |
| 3237 | 7.9 | 77 | 76 | 0.53 | 0.33 | |||||
| women (n = 141) | ||||||||||
| AI | <2000 mg | 14 | 0.93 | (0.87–0.98) | 2001 | 0.1 | 43 | 98 | 0.40 | 0.57 |
| 2391 | 19.6 | 93 | 81 | 0.74 | 0.20 | |||||
| DG | <2600 mg | 47 | 0.79 | (0.72–0.87) | 2605 | 0.2 | 60 | 78 | 0.37 | 0.46 |
| 2719 | 4.6 | 72 | 74 | 0.47 | 0.38 | |||||
| Na/K ratio || | ||||||||||
| Men and women (n = 235) | ||||||||||
| ≥2.00 mmol/mmol | 215 | 0.97 | (0.94–1.00) | 2.00 | 0.0 | 100 | 50 | 0.50 | 0.50 | |
| 2.32 | 16.2 | 92 | 95 | 0.87 | 0.10 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuno, T.; Takachi, R.; Ishihara, J.; Ishii, Y.; Kito, K.; Maruya, S.; Nakamura, K.; Tanaka, J.; Yamagishi, K.; Yamaji, T.; et al. Validity of the Food Frequency Questionnaire—Estimated Intakes of Sodium, Potassium, and Sodium-to-Potassium Ratio for Screening at a Point of Absolute Intake among Middle-Aged and Older Japanese Adults. Nutrients 2022, 14, 2594. https://doi.org/10.3390/nu14132594
Matsuno T, Takachi R, Ishihara J, Ishii Y, Kito K, Maruya S, Nakamura K, Tanaka J, Yamagishi K, Yamaji T, et al. Validity of the Food Frequency Questionnaire—Estimated Intakes of Sodium, Potassium, and Sodium-to-Potassium Ratio for Screening at a Point of Absolute Intake among Middle-Aged and Older Japanese Adults. Nutrients. 2022; 14(13):2594. https://doi.org/10.3390/nu14132594
Chicago/Turabian StyleMatsuno, Tomoka, Ribeka Takachi, Junko Ishihara, Yuri Ishii, Kumiko Kito, Sachiko Maruya, Kazutoshi Nakamura, Junta Tanaka, Kazumasa Yamagishi, Taiki Yamaji, and et al. 2022. "Validity of the Food Frequency Questionnaire—Estimated Intakes of Sodium, Potassium, and Sodium-to-Potassium Ratio for Screening at a Point of Absolute Intake among Middle-Aged and Older Japanese Adults" Nutrients 14, no. 13: 2594. https://doi.org/10.3390/nu14132594
APA StyleMatsuno, T., Takachi, R., Ishihara, J., Ishii, Y., Kito, K., Maruya, S., Nakamura, K., Tanaka, J., Yamagishi, K., Yamaji, T., Iso, H., Iwasaki, M., Tsugane, S., & Sawada, N., on behalf of the JPHC-NEXT Protocol Validation Study Group. (2022). Validity of the Food Frequency Questionnaire—Estimated Intakes of Sodium, Potassium, and Sodium-to-Potassium Ratio for Screening at a Point of Absolute Intake among Middle-Aged and Older Japanese Adults. Nutrients, 14(13), 2594. https://doi.org/10.3390/nu14132594