
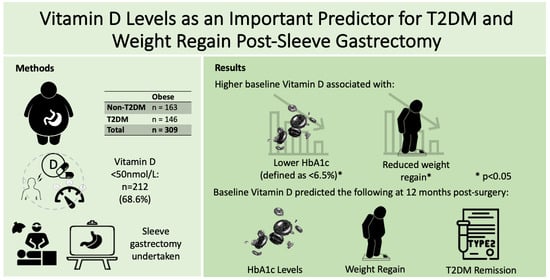
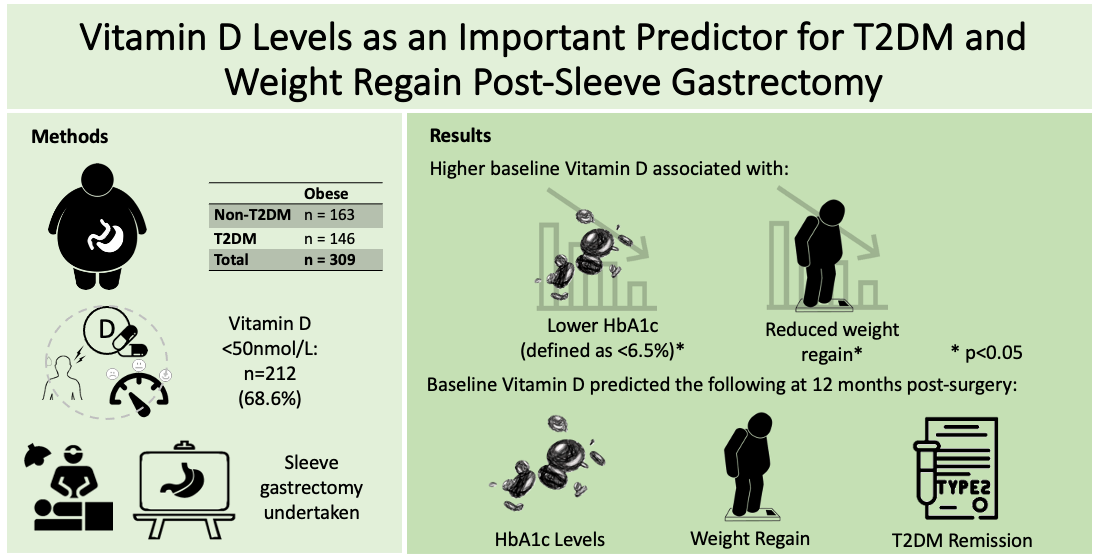
Vitamin D Levels as an Important Predictor for Type 2 Diabetes Mellitus and Weight Regain Post-Sleeve Gastrectomy

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and Study Design
2.2. Anthropometrics, Clinical Data and Blood Biochemistry
2.3. ANN Model Development and Sensitivity Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographics for Patients
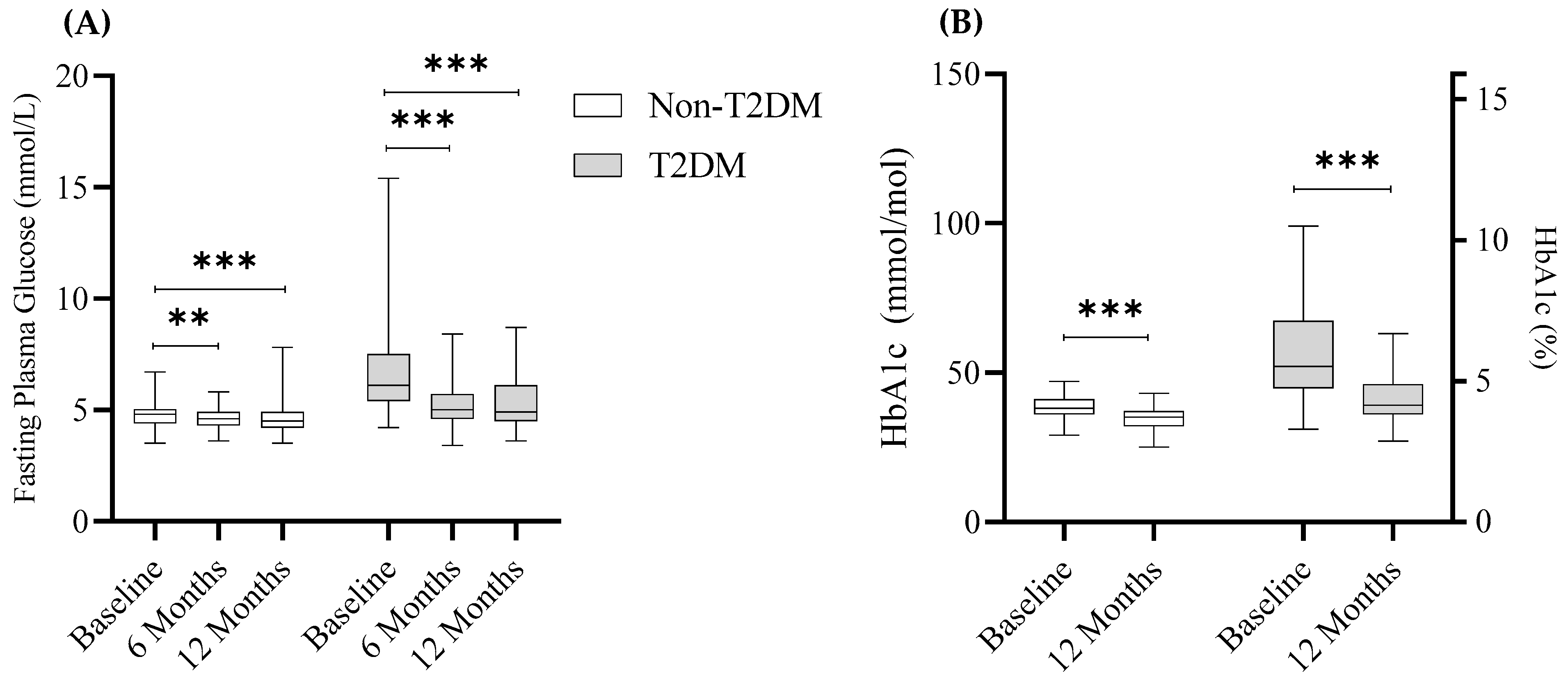
3.2. Metabolic Health Improves Post-SG
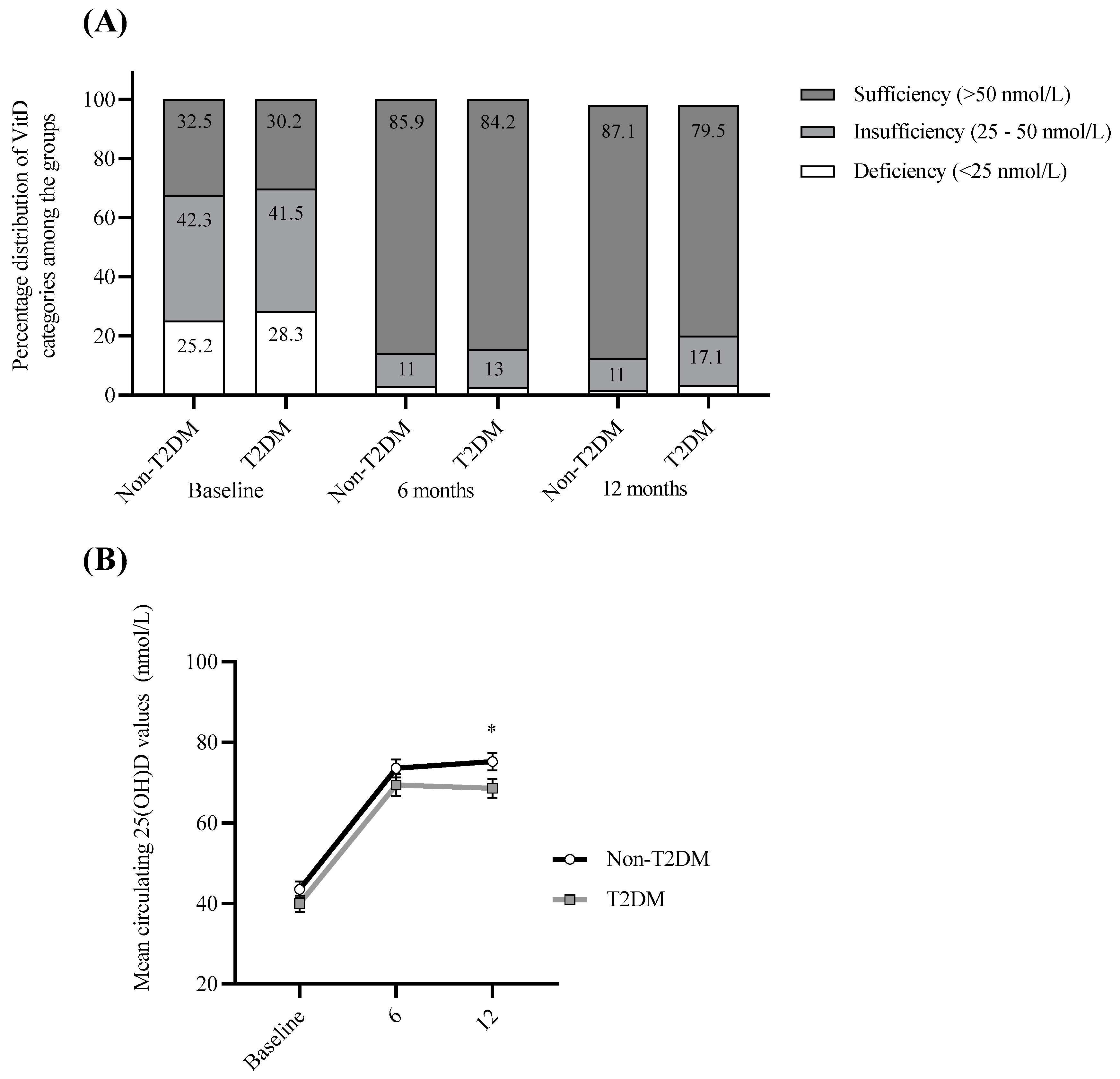
3.3. Impact of 25(OH)D Supplementation Varies Depending on T2DM Status
3.4. 25(OH)D Levels Negatively Correlate with Post-Surgery BMI, Weight and Weight Regain
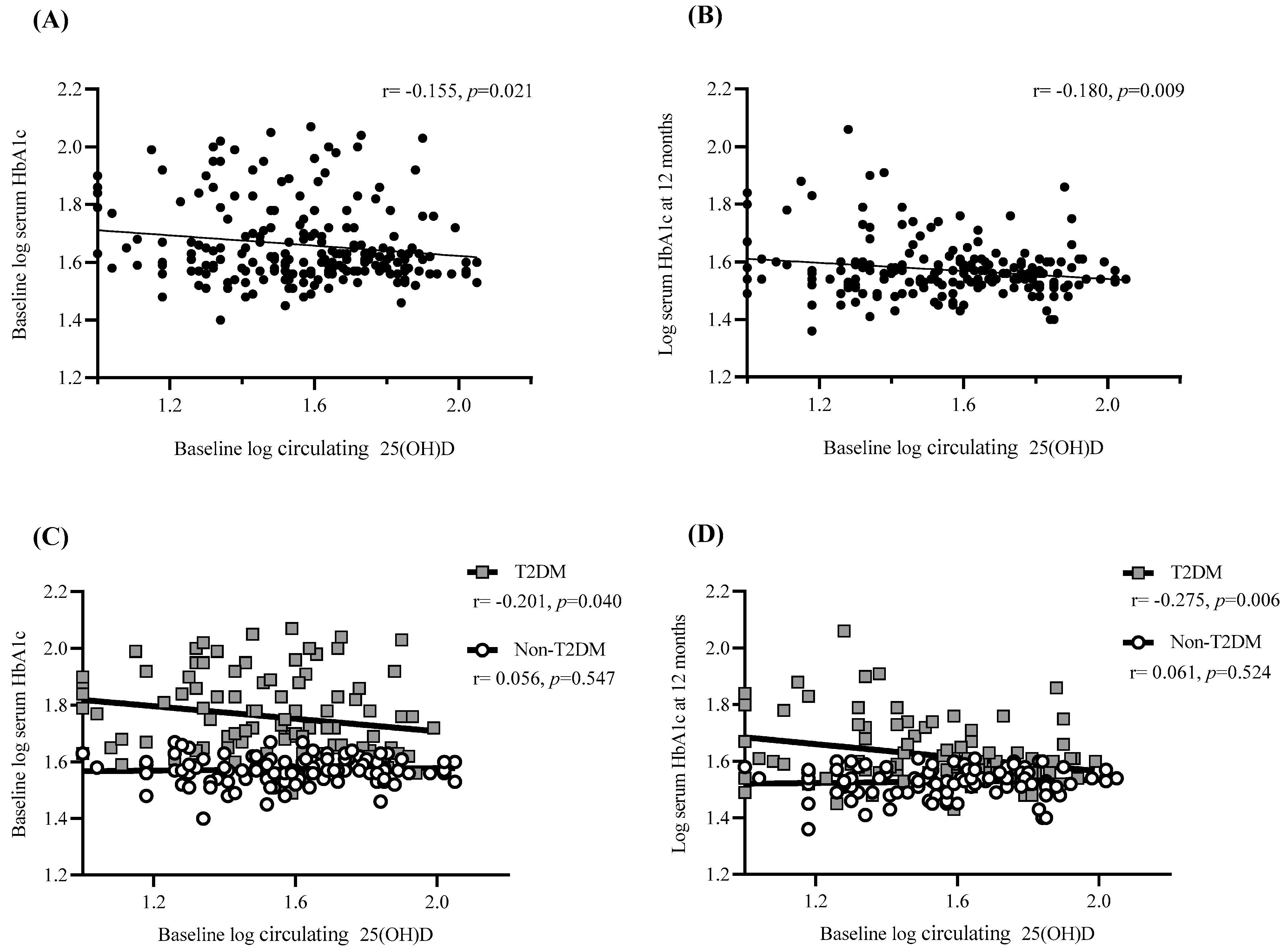
3.5. Baseline 25(OH)D Predicts HbA1c Levels at Baseline and One Year Post-Surgery
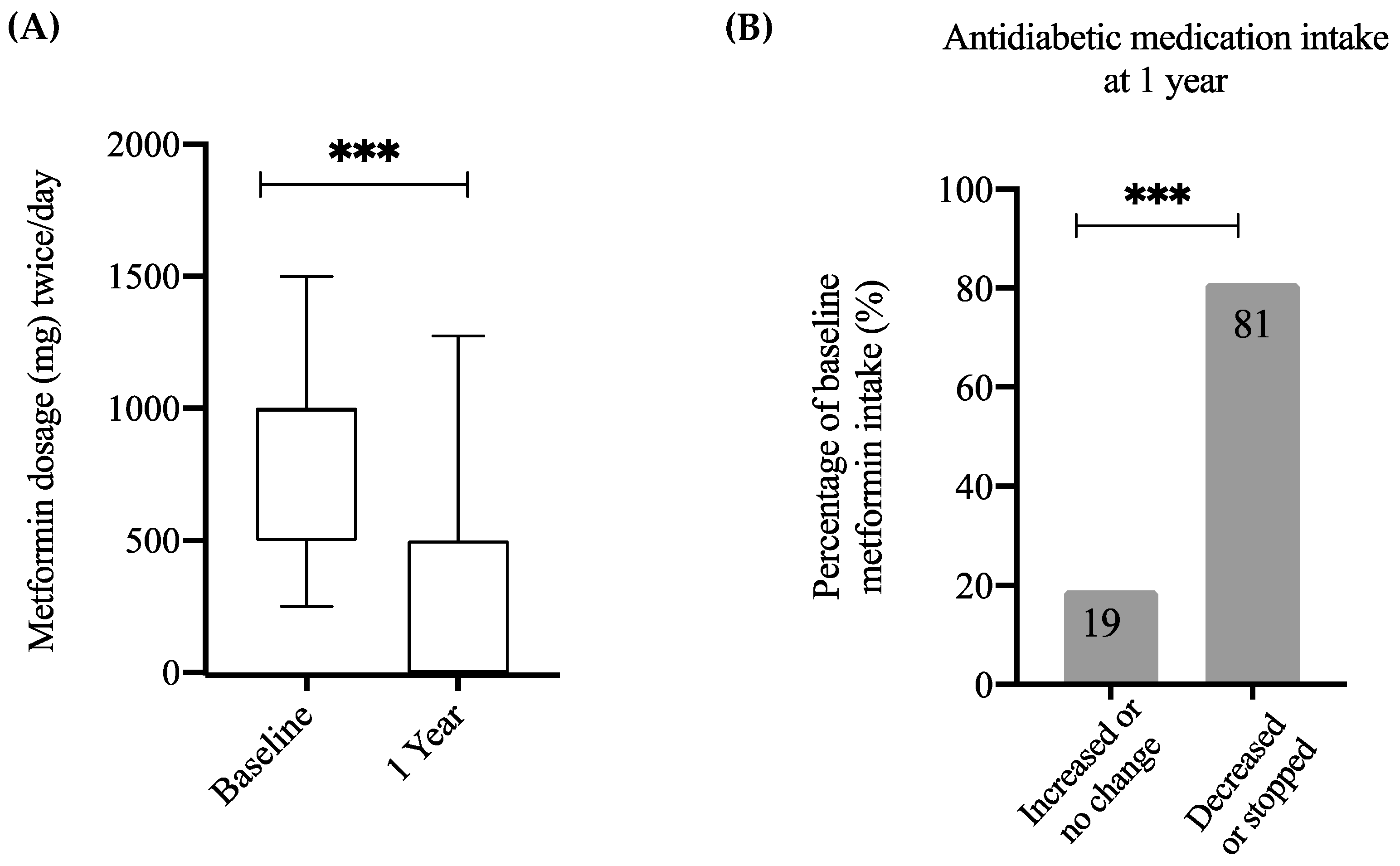
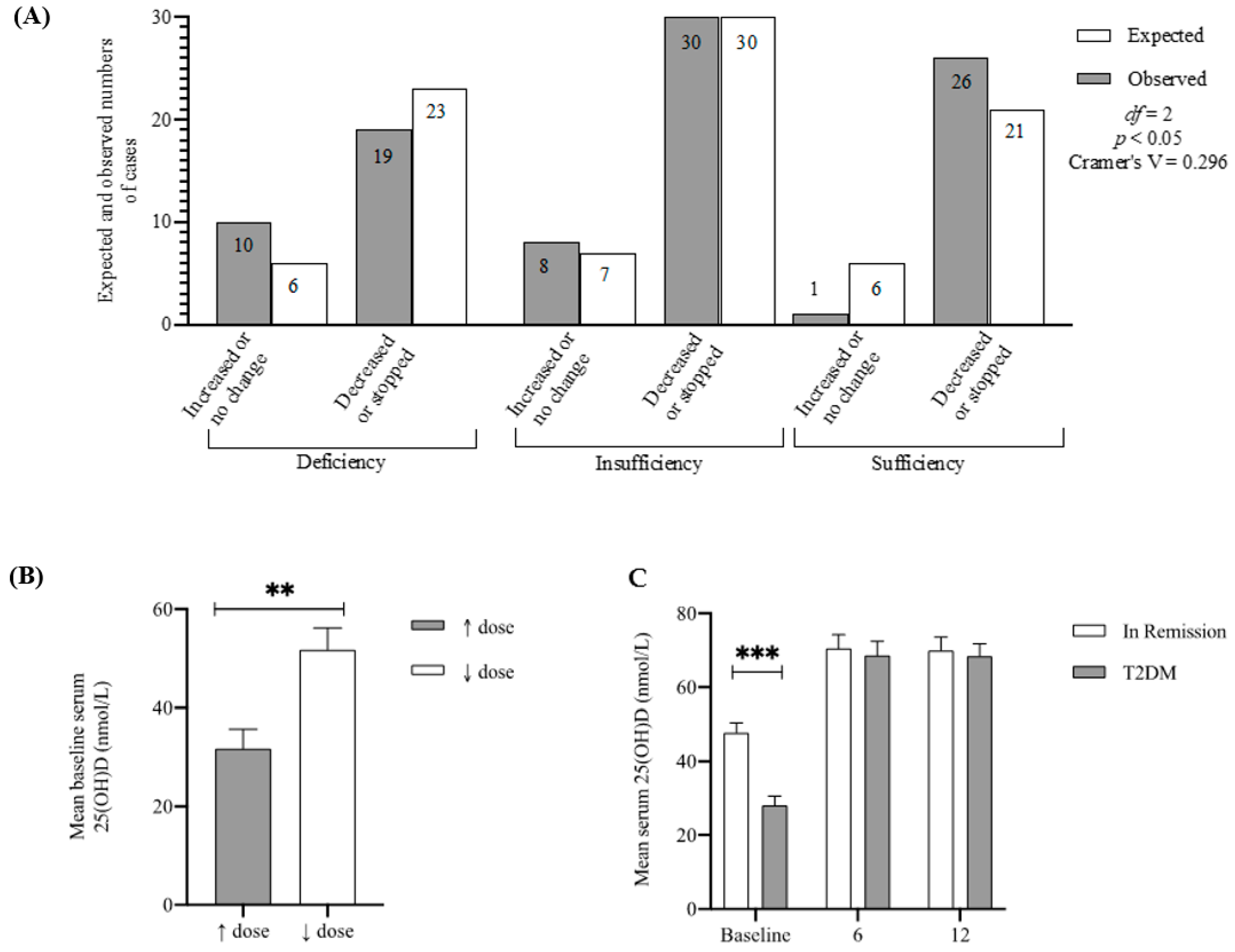
3.6. Baseline 25(OH)D Predicts T2DM Medication Intake One Year Post-Surgery
3.7. Baseline 25(OH)D Is the Second Most Relevant Factor for T2DM Remission Post-Surgery
3.8. Baseline 25(OH)D as an Indirect Factor for Improvements in Glucose Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 3 April 2020).
- Kitahara, C.M.; Flint, A.J.; Berrington de Gonzalez, A.; Bernstein, L.; Brotzman, M.; MacInnis, R.J.; Moore, S.C.; Robien, K.; Rosenberg, P.S.; Singh, P.N.; et al. Association between Class III Obesity (BMI of 40–59 kg/m2) and Mortality: A Pooled Analysis of 20 Prospective Studies. PLoS Med. 2014, 11, e1001673. [Google Scholar] [CrossRef] [PubMed]
- Pantalone, K.M.; Hobbs, T.M.; Chagin, K.M.; Kong, S.X.; Wells, B.J.; Kattan, M.W.; Bouchard, J.; Sakurada, B.; Milinovich, A.; Weng, W.; et al. Prevalence and Recognition of Obesity and Its Associated Comorbidities: Cross-Sectional Analysis of Electronic Health Record Data from a Large US Integrated Health System. BMJ Open 2017, 7, e017583. [Google Scholar] [CrossRef] [PubMed]
- Keramat, S.A.; Alam, K.; Rana, R.H.; Chowdhury, R.; Farjana, F.; Hashmi, R.; Gow, J.; Biddle, S.J.H. Obesity and the Risk of Developing Chronic Diseases in Middle-Aged and Older Adults: Findings from an Australian Longitudinal Population Survey, 2009–2017. PLoS ONE 2021, 16, e0260158. [Google Scholar] [CrossRef] [PubMed]
- Martini, F.; Anty, R.; Schneck, A.S.; Casanova, V.; Iannelli, A.; Gugenheim, J. Predictors of Metabolic Syndrome Persistence 1 Year after Laparoscopic Roux-En-Y Gastric Bypass. Surg. Obes. Relat. Dis. 2015, 11, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Cai, W.; Zhao, H.; Zhu, M.; Cui, J.; Sun, Z. Effect of Gastric Bypass on BMI and Lipid Metabolism in Type 2 Diabetes Mellitus. Artif. Cells Nanomed. Biotechnol. 2020, 48, 903–911. [Google Scholar] [CrossRef]
- Nora, M.; Guimaraes, M.; Almeida, R.; Martins, P.; Goncalves, G.; Santos, M.; Morais, T.; Freitas, C.; Monteiro, M.P. Excess Body Mass Index Loss Predicts Metabolic Syndrome Remission after Gastric Bypass. Diabetol. Metab. Syndr. 2014, 6, 1. [Google Scholar] [CrossRef]
- Wiggins, T.; Guidozzi, N.; Welbourn, R.; Ahmed, A.R.; Markar, S.R. Association of Bariatric Surgery with All-Cause Mortality and Incidence of Obesity-Related Disease at a Population Level: A Systematic Review and Meta-Analysis. PLoS Med. 2020, 17, e1003206. [Google Scholar] [CrossRef]
- Reiber, B.M.M.; Tenhagen, M.; Barendregt, R.; Mekel, M.P.; Cense, H.A.; Demirkiran, A. Total Weight Loss after Laparoscopic Roux-En-Y Gastric Bypass Is Influenced by Preoperative Weight Loss: Can We Predict the Outcome? Surg. Obes. Relat. Dis. 2020, 16, 1850–1856. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Youdim, A.; Jones, D.B.; Timothy Garvey, W.; Hurley, D.L.; Molly McMahon, M.; Heinberg, L.J.; Kushner, R.; Adams, T.D.; Shikora, S.; et al. Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient-2013 Update: Cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Endocr. Pract. 2013, 19, 337–372. [Google Scholar]
- Hoyuela, C. Five-Year Outcomes of Laparoscopic Sleeve Gastrectomy as a Primary Procedure for Morbid Obesity: A Prospective Study. World J. Gastrointest. Surg. 2017, 9, 109. [Google Scholar] [CrossRef]
- Sjöström, L.; Peltonen, M.; Jacobson, P.; Ahlin, S.; Andersson-Assarsson, J.; Anveden, Å.; Bouchard, C.; Carlsson, B.; Karason, K.; Lönroth, H.; et al. Association of Bariatric Surgery with Long-Term Remission of Type 2 Diabetes and with Microvascular and Macrovascular Complications. JAMA J. Am. Med. Assoc. 2014, 311, 2297–2304. [Google Scholar] [CrossRef] [PubMed]
- Panunzi, S.; de Gaetano, A.; Carnicelli, A.; Mingrone, G. Predictors of Remission of Diabetes Mellitus in Severely Obese Individuals Undergoing Bariatric Surgery: Do BMI or Procedure Choice Matter? A Meta-Analysis. Ann. Surg. 2015, 261, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Milone, M.; di Minno, M.N.D.; Leongito, M.; Maietta, P.; Bianco, P.; Taffuri, C.; Gaudioso, D.; Lupoli, R.; Savastano, S.; Milone, F.; et al. Bariatric Surgery and Diabetes Remission: Sleeve Gastrectomy or Mini-Gastric Bypass? World J. Gastroenterol. 2013, 19, 6590–6597. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.B.; O’Brien, P.E.; Playfair, J.; Chapman, L.; Schachter, L.M.; Skinner, S.; Proietto, J.; Bailey, M.; Anderson, M. Adjustable Gastric Banding and Conventional Therapy for Type 2 Diabetes: A Randomized Controlled Trial. JAMA J. Am. Med. Assoc. 2008, 299, 316–323. [Google Scholar] [CrossRef]
- AbdAlla Salman, M.; Rabiee, A.; Salman, A.; Elewa, A.; Tourky, M.; Mahmoud, A.A.; Moustafa, A.; El-Din Shaaban, H.; Ismail, A.A.; Noureldin, K.; et al. Predictors of Type-2 Diabetes Remission Following Bariatric Surgery after a Two-Year Follow Up. Asian J. Surg. 2022, 22, 132–135. [Google Scholar] [CrossRef]
- Xanthakos, S.A. Nutritional Deficiencies in Obesity and After Bariatric Surgery. Pediatric Clin. N. Am. 2009, 56, 1105–1121. [Google Scholar] [CrossRef]
- Wang, C.; Guan, B.; Yang, W.; Yang, J.; Cao, G.; Lee, S. Prevalence of Electrolyte and Nutritional Deficiencies in Chinese Bariatric Surgery Candidates. Surg. Obes. Relat. Dis. 2016, 12, 629–634. [Google Scholar] [CrossRef]
- Roust, L.R.; DiBaise, J.K. Nutrient Deficiencies Prior to Bariatric Surgery. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 138–144. [Google Scholar] [CrossRef]
- Peterson, L.A.; Cheskin, L.J.; Furtado, M.; Papas, K.; Schweitzer, M.A.; Magnuson, T.H.; Steele, K.E. Malnutrition in Bariatric Surgery Candidates: Multiple Micronutrient Deficiencies Prior to Surgery. Obes. Surg. 2016, 26, 833–838. [Google Scholar] [CrossRef]
- Frame-Peterson, L.A.; Megill, R.D.; Carobrese, S.; Schweitzer, M. Nutrient Deficiencies Are Common Prior to Bariatric Surgery. Nutr. Clin. Pract. 2017, 32, 463–469. [Google Scholar] [CrossRef]
- Al-Mutawa, A.; Anderson, A.K.; Alsabah, S.; Al-Mutawa, M. Nutritional Status of Bariatric Surgery Candidates. Nutrients 2018, 10, 67. [Google Scholar] [CrossRef] [PubMed]
- Szymczak-Pajor, I.; Miazek, K.; Selmi, A.; Balcerczyk, A.; Śliwińska, A. The Action of Vitamin D in Adipose Tissue: Is There the Link between Vitamin D Deficiency and Adipose Tissue-Related Metabolic Disorders? Int. J. Mol. Sci. 2022, 23, 956. [Google Scholar] [CrossRef] [PubMed]
- Nimitphong, H.; Park, E.; Lee, M.J. Vitamin D Regulation of Adipogenesis and Adipose Tissue Functions. Nutr. Res. Pract. 2020, 14, 553. [Google Scholar] [CrossRef] [PubMed]
- Nimitphong, H.; Holick, M.F.; Fried, S.K.; Lee, M.-J. 25-Hydroxyvitamin D3 and 1,25-Dihydroxyvitamin D3 Promote the Differentiation of Human Subcutaneous Preadipocytes. PLoS ONE 2012, 7, e52171. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Ashraf, A. Role of Vitamin d in Insulin Secretion and Insulin Sensitivity for Glucose Homeostasis. Int. J. Endocrinol. 2010, 2010, 351385. [Google Scholar] [CrossRef]
- Bouillon, R.; Carmeliet, G.; Lieben, L.; Watanabe, M.; Perino, A.; Auwerx, J.; Schoonjans, K.; Verstuyf, A. Vitamin D and Energy Homeostasis: Of Mice and Men. Nat. Rev. Endocrinol. 2014, 10, 79–87. [Google Scholar] [CrossRef]
- Narvaez, C.J.; Matthews, D.; Broun, E.; Chan, M.; Welsh, J. Lean Phenotype and Resistance to Diet-Induced Obesity in Vitamin D Receptor Knockout Mice Correlates with Induction of Uncoupling Protein-1 in White Adipose Tissue. Endocrinology 2009, 150, 651–661. [Google Scholar] [CrossRef]
- Benetti, E.; Mastrocola, R.; Chiazza, F.; Nigro, D.; D’Antona, G.; Bordano; Fantozzi, R.; Aragno, M.; Collino, M.; Minetto, M.A. Effects of Vitamin D on Insulin Resistance and Myosteatosis in Diet-Induced Obese Mice. PLoS ONE 2018, 13, e0189707. [Google Scholar] [CrossRef]
- Altieri, B.; Grant, W.B.; della Casa, S.; Orio, F.; Pontecorvi, A.; Colao, A.; Sarno, G.; Muscogiuri, G.; della Casa, S. Critical Reviews in Food Science and Nutrition Vitamin D and Pancreas: The Role of Sunshine Vitamin in the Pathogenesis of Diabetes Mellitus and Pancreatic Cancer. Crit. Rev. Food Sci. Nutr. 2017, 57, 3472–3488. [Google Scholar] [CrossRef]
- Wang, M.; Zhou, T.; Li, X.; Ma, H.; Liang, Z.; Fonseca, V.A.; Heianza, Y.; Qi, L. Baseline Vitamin D Status, Sleep Patterns, and the Risk of Incident Type 2 Diabetes in Data From the UK Biobank Study. Diabetes Care 2020, 43, 2776–2784. [Google Scholar] [CrossRef]
- Denos, M.; Mai, X.M.; Åsvold, B.O.; Sørgjerd, E.P.; Chen, Y.; Sun, Y.Q. Vitamin D Status and Risk of Type 2 Diabetes in the Norwegian HUNT Cohort Study: Does Family History or Genetic Predisposition Modify the Association? BMJ Open Diabetes Res. Care 2021, 9, e001948. [Google Scholar] [CrossRef] [PubMed]
- Forouhi, N.G.; Luan, J.N.A.; Cooper, A.; Boucher, B.J.; Wareham, N.J. Baseline Serum 25-Hydroxy Vitamin d Is Predictive of Future Glycemic Status and Insulin Resistance the Medical Research Council Ely Prospective Study 1990–2000. Diabetes 2008, 57, 2619–2625. [Google Scholar] [CrossRef] [PubMed]
- Moizé, V.; Deulofeu, R.; Torres, F.; de Osaba, J.M.; Vidal, J. Nutritional Intake and Prevalence of Nutritional Deficiencies Prior to Surgery in a Spanish Morbidly Obese Population. Obes. Surg. 2011, 21, 1382–1388. [Google Scholar] [CrossRef] [PubMed]
- Bal, B.S.; Finelli, F.C.; Shope, T.R.; Koch, T.R. Nutritional Deficiencies after Bariatric Surgery. Nat. Rev. Endocrinol. 2012, 8, 544–556. [Google Scholar] [CrossRef] [PubMed]
- Goldner, W.S.; Stoner, J.A.; Thompson, J.; Taylor, K.; Larson, L.; Erickson, J.; McBride, C. Prevalence of Vitamin D Insufficiency and Deficiency in Morbidly Obese Patients: A Comparison with Non-Obese Controls. Obes Surg. 2008, 18, 145–150. [Google Scholar] [CrossRef]
- Wamberg, L.; Kampmann, U.; Stødkilde-Jørgensen, H.; Rejnmark, L.; Pedersen, S.B.; Richelsen, B. Effects of Vitamin D Supplementation on Body Fat Accumulation, Inflammation, and Metabolic Risk Factors in Obese Adults with Low Vitamin D Levels—Results from a Randomized Trial. Eur. J. Intern. Med. 2013, 24, 644–649. [Google Scholar] [CrossRef]
- Mitri, J.; Dawson-Hughes, B.; Hu, F.B.; Pittas, A.G. Effects of Vitamin D and Calcium Supplementation on Pancreatic β Cell Function, Insulin Sensitivity, and Glycemia in Adults at High Risk of Diabetes: The Calcium and Vitamin D for Diabetes Mellitus (CaDDM) Randomized Controlled Trial. Am. J. Clin. Nutr. 2011, 94, 486–494. [Google Scholar] [CrossRef]
- Pilz, S.; van den Hurk, K.; Nijpels, G.; Stehouwer, C.D.A.; van’t Riet, E.; Kienreich, K.; Tomaschitz, A.; Dekker, J.M. Vitamin D Status, Incident Diabetes and Prospective Changes in Glucose Metabolism in Older Subjects: The Hoorn Study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 883–889. [Google Scholar] [CrossRef]
- Ji, S.; Doumit, M.E.; Hill, R.A. Regulation of Adipogenesis and Key Adipogenic Gene Expression by 1, 25-Dihydroxyvitamin D in 3T3-L1 Cells. PLoS ONE 2015, 10, e0126142. [Google Scholar] [CrossRef]
- Perticone, M.; Maio, R.; Sciacqua, A.; Suraci, E.; Pinto, A.; Pujia, R.; Zito, R.; Gigliotti, S.; Sesti, G.; Perticone, F. Ketogenic Diet-Induced Weight Loss Is Associated with an Increase in Vitamin D Levels in Obese Adults. Molecules 2019, 24, 2499. [Google Scholar] [CrossRef]
- Bennour, I.; Haroun, N.; Sicard, F.; Mounien, L.; Landrier, J. Recent Insights into Vitamin D, Adipocyte, and Adipose Tissue Biology. Obes. Rev. 2022, e13453. [Google Scholar] [CrossRef] [PubMed]
- Obispo Entrenas, A.; Legupin Tubio, D.; Lucena Navarro, F.; Martin Carvajal, F.; Gandara Adan, N.; Redondo Bautista, M.; Abiles Osinaga, J. Relationship Between Vitamin D Deficiency and the Components of Metabolic Syndrome in Patients with Morbid Obesity, Before and 1 Year After Laparoscopic Roux-En-Y Gastric Bypass or Sleeve Gastrectomy. Obes. Surg. 2017, 27, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Gradillas-García, A.; Álvarez, J.; Rubio, J.A.; de Abajo, F.J. Relationship between Vitamin D Deficiency and Metabolic Syndrome in Adult Population of the Community of Madrid. Endocrinol. Nutr. (Engl. Ed.) 2015, 62, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Mingrone, G.; Panunzi, S.; de Gaetano, A.; Guidone, C.; Iaconelli, A.; Leccesi, L.; Nanni, G.; Pomp, A.; Castagneto, M.; Ghirlanda, G.; et al. Bariatric Surgery versus Conventional Medical Therapy for Type 2 Diabetes. N. Engl. J. Med. 2012, 366, 1577–1585. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Levi, A.M.; Matia, P.; Cabrerizo, L.; Barabash, A.; Sanchez-Pernaute, A.; Calle-Pascual, A.L.; Torres, A.J.; Rubio, M.A. Statistical Models to Predict Type 2 Diabetes Remission after Bariatric Surgery. J. Diabetes 2014, 6, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Schauer, P.R.; Kashyap, S.R.; Wolski, K.; Brethauer, S.A.; Kirwan, J.P.; Pothier, C.E.; Thomas, S.; Abood, B.; Nissen, S.E.; Bhatt, D.L. Bariatric Surgery versus Intensive Medical Therapy in Obese Patients with Diabetes. N. Engl. J. Med. 2012, 366, 1567–1576. [Google Scholar] [CrossRef]
- Tang, X.; Yan, X.; Zhou, H.; Huang, G.; Niu, X.; Jiang, H.; Su, H.; Yang, X.; Li, X.; Zhou, Z. Associations of Insulin Resistance and Beta-Cell Function with Abnormal Lipid Profile in Newly Diagnosed Diabetes. Chin. Med. J. 2022; ahead of pub. [Google Scholar] [CrossRef]
- Jorde, R.; Grimnes, G. Vitamin D and Metabolic Health with Special Reference to the Effect of Vitamin D on Serum Lipids. Prog. Lipid Res. 2011, 50, 303–312. [Google Scholar] [CrossRef]
- Hutchinson, M.S.; Figenschau, Y.; Njølstad, I.; Schirmer, H.; Jorde, R. Serum 25-Hydroxyvitamin D Levels Are Inversely Associated with Glycated Haemoglobin (HbA1c). The Tromsø Study. Scand. J. Clin. Lab. Investig. 2011, 71, 399–406. [Google Scholar] [CrossRef]
- Zittermann, A.; Frisch, S.; Berthold, H.K.; Götting, C.; Kuhn, J.; Kleesiek, K.; Stehle, P.; Koertke, H.; Koerfer, R. Vitamin D Supplementation Enhances the Beneficial Effects of Weight Loss on Cardiovascular Disease Risk Markers. Am. J. Clin. Nutr. 2009, 89, 1321–1327. [Google Scholar] [CrossRef]
- Sai, A.J.; Gallagher, J.C.; Fang, X. Effect of Hormone Therapy and Calcitriol on Serum Lipid Profile in Postmenopausal Older Women: Association with Estrogen Receptor-α Genotypes. Menopause 2011, 18, 1101–1112. [Google Scholar] [CrossRef][Green Version]
- Salehpour, A.; Shidfar, F.; Hosseinpanah, F.; Vafa, M.; Razaghi, M.; Hoshiarrad, A.; Gohari, M. VitD3 and the Risk of CVD in Overweight and Obese Women: A Randomised Controlled Trial. Br. J. Nutr. 2012, 108, 1866–1873. [Google Scholar] [CrossRef] [PubMed]
- Motiwala, S.R.; Wang, T.J. Vitamin D and Cardiovascular Disease. Curr. Opin. Nephrol. Hypertens. 2011, 20, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Busetto, L.; Dicker, D.; Azran, C.; Batterham, R.L.; Farpour-Lambert, N.; Fried, M.; Hjelmesæth, J.; Kinzl, J.; Leitner, D.R.; Makaronidis, J.M.; et al. Practical Recommendations of the Obesity Management Task Force of the European Association for the Study of Obesity for the Post-Bariatric Surgery Medical Management. Obes. Facts 2018, 10, 597–632. [Google Scholar] [CrossRef] [PubMed]
- Lespessailles, E.; Toumi, H. Vitamin D Alteration Associated with Obesity and Bariatric Surgery. Exp. Biol. Med. 2017, 242, 1086–1094. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-T2DM n = 163 | T2DM n = 146 | Non-T2DM vs. T2DM | |||
|---|---|---|---|---|---|
| Mean ± SD | Min–Max | Mean ± SD | Min–Max | p Value | |
| Age (years) | 46.32 ± 9.93 | 26–70 | 48.2 ± 10.6 | 23–70 | 0.261 |
| Height (m) | 1.66 ± 0.1 | 1.48–1.91 | 1.68 ± 0.1 | 1.45–1.91 | 0.076 |
| Pre-Dietary Intervention Weight (kg) | 144.59 ± 22.86 | 98–216 | 144.21 ± 22.9 | 94–225 | 0.884 |
| Baseline Weight (kg) | 129.58 ± 21.4 | 88–187 | 130.7 ± 21.27 | 84–208 | 0.647 |
| BMI (kg/m2) | 52.57 ± 6.65 | 36–74 | 51.15 ± 7.1 | 39–75 | 0.068 |
| IBW (kg) | 78.84 ± 7.73 | 57–91 | 71.67 ± 7.93 | 57–91 | 0.079 |
| Excess Weight (kg) | 75.75 ± 19.1 | 32–143 | 73.54 ± 20 | 36–134 | 0.545 |
| % Excess Weight Loss (%) | 19.45 ± 13.14 | −20–63 | 18.58 ± 11.92 | −6–58 | 0.545 |
| Baseline | 6 Months | 12 Months | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Non-T2DM | T2DM | Non-T2DM | T2DM | Non-T2DM | T2DM | ||||
| Mean ± SD | Mean ± SD | p Value | Mean ± SD | Mean ± SD | p Value | Mean ± SD | Mean ± SD | p Value | |
| 25(OH)D (nmol/L) | 43.47 ± 22.77 | 39.96 ± 21 | N.S | 73.54 ± 25.3 | 69.43 ± 26.28 | N.S | 75.45 ± 25.47 | 68.66 ± 25.6 | <0.05 |
| FPG (mmol/L) | 4.85 ± 0.67 | 7.91 ± 4.39 | <0.005 | 4.72 ± 0.8 | 5.92 ± 2.41 | <0.005 | 4.59 ± 0.7 | 5.84 ± 2.37 | <0.005 |
| HbA1c (mmol/mol) (%) | 38.09 ± 4 (5.6 ± 2.5) | 58.59 ± 18.87 (7.5 ± 3.9) | <0.005 | NA | NA | N.S | 34.28 ± 3.87 (5.3 ± 2.5) | 43.59 ± 12.85 (6.1 ± 3.3) | <0.005 |
| Cholesterol (mmol/L) | 5.13 ± 0.96 | 4.35 ± 0.95 | <0.005 | 4.89 ± 0.95 | 4.3 ± 0.95 | <0.005 | 5.03 ± 0.95 | 4.6 ± 1 | <0.005 |
| HDL-Chol (mmol/L) | 1.33 ± 0.32 | 1.15 ± 0.33 | <0.005 | 1.44 ± 0.44 | 1.35 ± 0.45 | N.S | 1.66 ± 0.38 | 1.45 ± 0.4 | <0.005 |
| TG (mmol/L) | 1.51 ± 0.71 | 1.86 ± 0.9 | <0.005 | 1.34 ± 0.8 | 1.35 ± 0.54 | N.S | 1.16 ± 0.53 | 1.59 ± 0.76 | <0.005 |
| Chol:HDL | 4.02 ± 1 | 4 ± 1.25 | N.S | 3.61 ± 1.1 | 3.39 ± 1 | N.S | 3.15 ± 0.87 | 3.37 ± 1.1 | N.S |
| LDL-Chol (mmol/L) | 3.11 ± 0.86 | 2.29 ± 0.97 | <0.005 | 2.88 ± 0.85 | 2.3 ± 0.86 | <0.005 | 2.86 ± 0.89 | 2.45 ± 0.95 | <0.005 |
| AST (U/L) | 77.25 ± 21.91 | 80.59 ± 25.46 | 74.7 ± 30 | 68.27 ± 16.48 | <0.05 | 70 ± 22.54 | 72.89 ± 21.23 | N.S | |
| ALT (U/L) | 23.28 ± 13.66 | 28.51 ± 18.87 | <0.005 | 15.91 ± 15.32 | 18.49 ± 16 | <0.05 | 13.47 ± 5.57 | 15.14 ± 7 | <0.05 |
| CRP (mg/L) | 12.1 ± 9.7 | 10.88 ± 12.8 | N.S | NA | NA | N.S | NA | NA | N.S |
| * CRP + 1 (mg/L) | 30.65 ± 32.69 | 26.91 ± 22.7 | N.S | NA | NA | N.S | NA | NA | N.S |
| fT4 (ug/dL) | 15.74 ± 3.98 | 16.24 ± 5.46 | N.S | NA | NA | N.S | 15.82 ± 4.2 | 16.22 ± 4.5 | N.S |
| TSH (mIU/L) | 2.37 ± 2 | 2.23 ± 1.7 | N.S | NA | NA | N.S | 2.2 ± 4.11 | 1.57 ± 1.1 | N.S |
| Systolic BP (mmHg) | 140.11 ± 17.2 | 142 ± 18.74 | N.S | NA | NA | N.S | 129.88 ± 19.1 | 131.8 ± 18.44 | N.S |
| Diastolic BP (mmHg) | 76.29 ± 10.47 | 76.94 ± 10.95 | N.S | NA | NA | N.S | 74.65 ± 10.41 | 75 ± 10.75 | N.S |
| Factor | No Remission at 12 Months (n = 56) | Remission at 12 Months (n = 75) | p Value |
|---|---|---|---|
| Sex (F/M) | 38/18 | 48/27 | 0.646 |
| Age (years) | 51.5 ± 8.4 | 49.4 ± 10.7 | 0.228 |
| BMI (kg/m2) | 50.47 ± 7.4 | 51.1 ± 6.3 | 0.615 |
| EWL (%) | 17.2 ± 13.2 | 20.7 ± 11 | 0.098 |
| 25(OH)D (nmol/L) | 28.1 ± 16.1 | 47.5 ± 21.1 | <0.001 *** |
| FPG (mmol/L) | 10 ± 5.5 | 6.6 ± 3.1 | <0.001 *** |
| HbA1c (mmol/mol) (%) | 70.2 ± 20.8 (8.6 ± 4.1) | 50.3 ± 13.5 (6.8 ± 3.4) | <0.001 *** |
| Cholesterol (mmol/L) | 4.1 ± 1 | 4.4 ± 1 | 0.084 |
| HDL-Chol (mmol/L) | 1.1 ± 0.3 | 1.2 ± 0.3 | 0.055 |
| TG (mmol/L) | 2 ± 1 | 1.8 ± 0.9 | 0.092 |
| Chol:HDL | 3.9 ± 1.2 | 3.9 ± 1.2 | 0.893 |
| LDL-Chol (mmol/L) | 2.1 ± 0.9 | 2.3 ± 1 | 0.267 |
| AST (U/L) | 89.1 ± 30.1 | 74.3 ± 19.1 | 0.002 ** |
| ALT (U/L) | 27.3 ± 17.8 | 28.2 ± 19 | 0.527 |
| T4 (ug/dL) | 16.1 ± 5.1 | 16.6 ± 5.8 | 0.759 |
| TSH (mIU/L) | 2.41 ± 1.7 | 1.94 ± 1.3 | 0.749 |
| Systolic BP (mmHg) | 137.3 ± 20.7 | 144.2 ± 17.5 | 0.087 |
| Diastolic BP (mmHg) | 74.8 ± 12 | 78 ± 10.6 | 0.165 |
| Metformin Dose (mg/daily) * | 979.2 ± 286 | 813.64 ± 306.2 | 0.004 ** |
| Hypertension (case no.) | 46 (82.1) | 49 (65.3) | 0.033 * |
| Dyslipidaemia (case no.) | 20 (35.7%) | 23 (30.7%) | 0.543 |
| Factor | β0 | β1 | R2 | OR | 95% CI | p-Value * | |
|---|---|---|---|---|---|---|---|
| Univariate Analysis | |||||||
| Age | −1.418 | 0.022 | 0.015 | 1.023 | 0.227 | ||
| BMI | |||||||
| HbA1c | −4.186 | 0.067 | 0.330 | 1.069 | 1.041–1.098 | <0.001 | |
| 25(OH)D | 1.665 | −0.056 | 0.278 | 0.954 | 0.920–0.971 | <0.001 | |
| FPG | −2.043 | 0.225 | 0.193 | 1.252 | 1.107–1.417 | <0.001 | |
| AST | −2.523 | 0.028 | 0.117 | 1.028 | 1.010–1.046 | 0.002 | |
| Metformin Dose | −2.038 | 0.002 | 0.095 | 1.002 | 1.001–1.003 | 0.006 | |
| Hypertension | −0.956 | 0.892 | 0.047 | 2.441 | 1.061–5.614 | 0.036 | |
| Multivariate Analysis | |||||||
| Model I | 25(OH)D | 0.233 | −0.056 | 0.379 | 0.946 | 0.918–0.974 | <0.001 |
| FPG | 0.173 | 1.189 | 1.048–1.349 | 0.007 | |||
| Model II | 25(OH)D | −3.287 | −0.064 | 0.445 | 0.938 | 0.909–0.969 | <0.001 |
| FPG | 0.203 | 1.225 | 1.081–1.389 | 0.001 | |||
| Age | 0.071 | 1.073 | 1.015–1.135 | 0.013 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aladel, A.; Murphy, A.M.; Abraham, J.; Shah, N.; Barber, T.M.; Ball, G.; Menon, V.; Piya, M.K.; McTernan, P.G. Vitamin D Levels as an Important Predictor for Type 2 Diabetes Mellitus and Weight Regain Post-Sleeve Gastrectomy. Nutrients 2022, 14, 2052. https://doi.org/10.3390/nu14102052
Aladel A, Murphy AM, Abraham J, Shah N, Barber TM, Ball G, Menon V, Piya MK, McTernan PG. Vitamin D Levels as an Important Predictor for Type 2 Diabetes Mellitus and Weight Regain Post-Sleeve Gastrectomy. Nutrients. 2022; 14(10):2052. https://doi.org/10.3390/nu14102052
Chicago/Turabian StyleAladel, Alanoud, Alice M. Murphy, Jenny Abraham, Neha Shah, Thomas M. Barber, Graham Ball, Vinod Menon, Milan K. Piya, and Philip G. McTernan. 2022. "Vitamin D Levels as an Important Predictor for Type 2 Diabetes Mellitus and Weight Regain Post-Sleeve Gastrectomy" Nutrients 14, no. 10: 2052. https://doi.org/10.3390/nu14102052
APA StyleAladel, A., Murphy, A. M., Abraham, J., Shah, N., Barber, T. M., Ball, G., Menon, V., Piya, M. K., & McTernan, P. G. (2022). Vitamin D Levels as an Important Predictor for Type 2 Diabetes Mellitus and Weight Regain Post-Sleeve Gastrectomy. Nutrients, 14(10), 2052. https://doi.org/10.3390/nu14102052