
Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis

 ,
, 
 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Methods
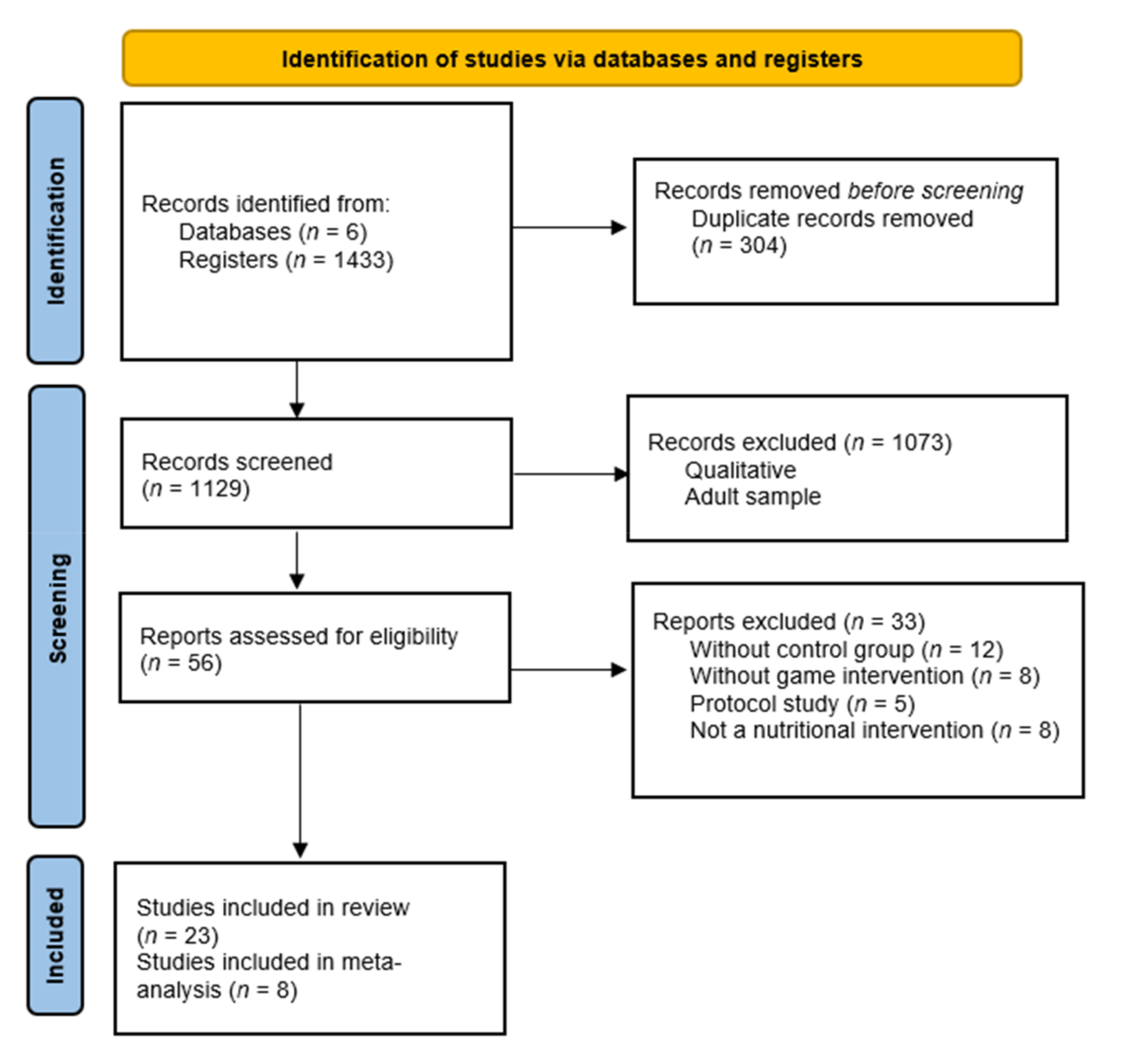
2.1. Design and Search Methods
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection, Quality Appraisal, and Risk of Bias
2.4. Data Abstraction
2.5. Data Analysis
3. Results
3.1. Study Characteristics
3.2. Effects of Gamification on Food Groups and Food Habits
3.3. Effects of Gamification in Body Composition
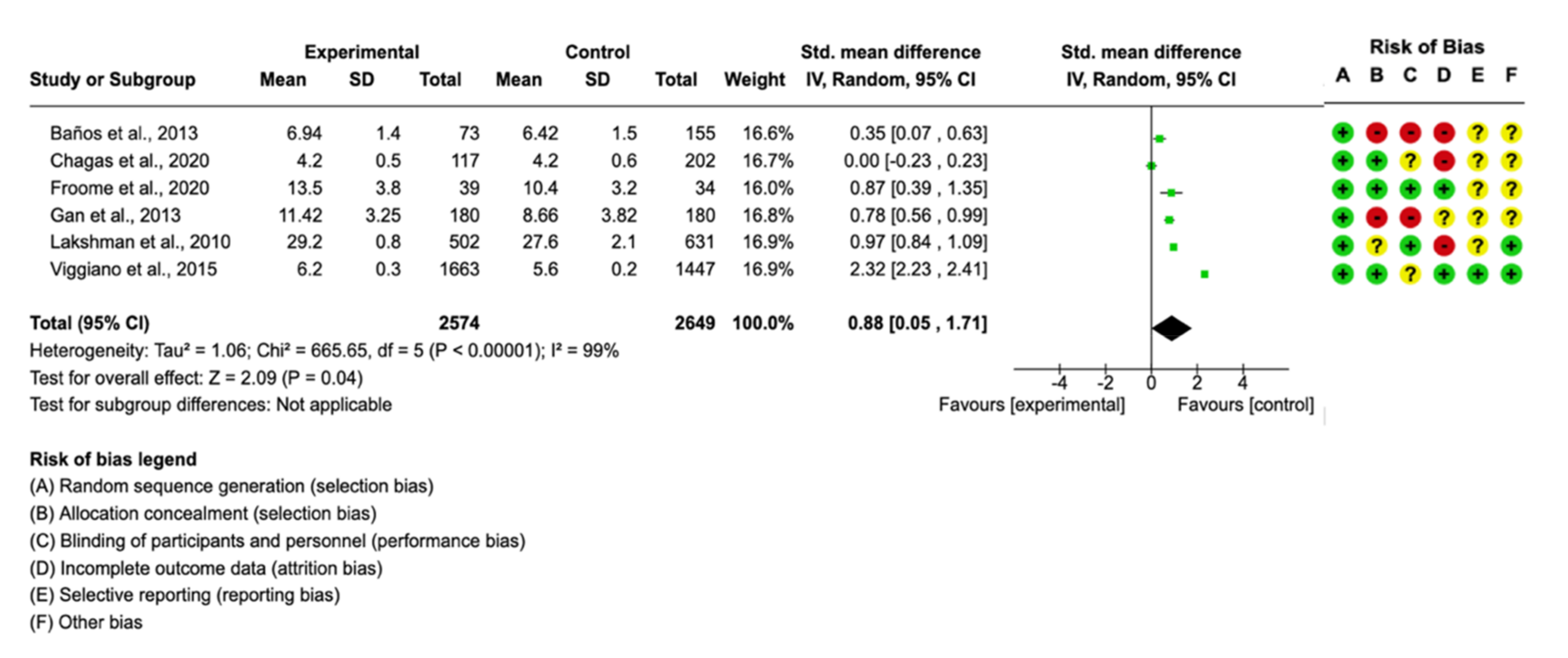
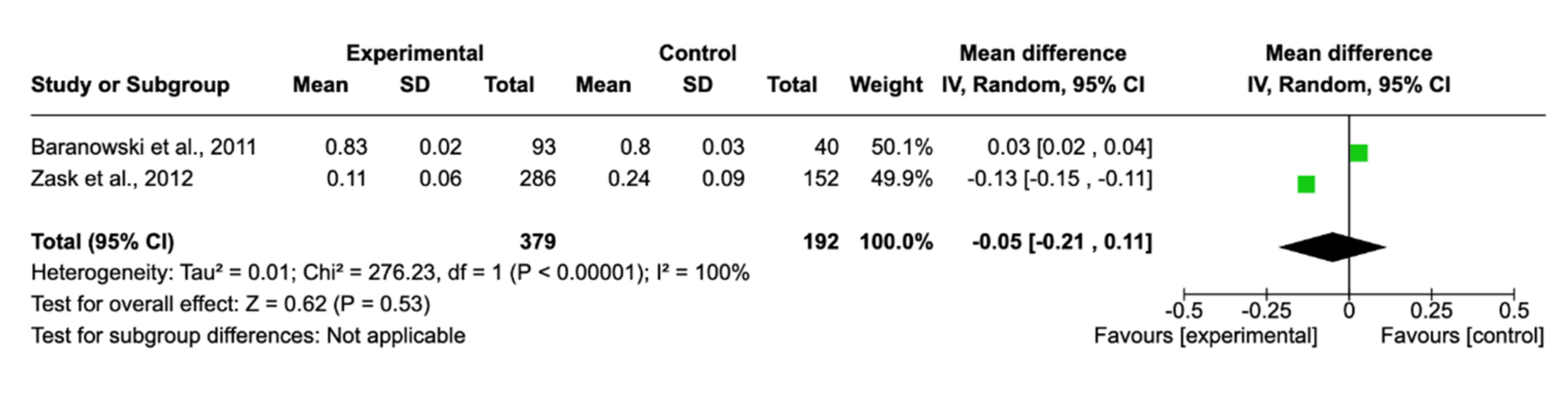
3.4. Meta-Analysis Results and Risk of Bias
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Riley, L.M.; Taddei, C.; Hajifathalian, K.; Lu, Y.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 1 April 2021).
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/handle/10665/94384 (accessed on 1 April 2021).
- Rohde, A.; Duensing, A.; Dawczynski, C.; Godemann, J.; Lorkowski, S.; Brombach, C. An App to improve eating habits of adolescents and young adults (Challenge to Go): Systematic development of a theory-based and target group-adapted mobile app intervention. J. Med. Internet Res. 2019, 21, e11575. [Google Scholar] [CrossRef]
- Schoeppe, S.; Alley, S.; Rebar, A.L.; Hayman, M.; Bray, N.A.; Van Lippevelde, W.; Gnam, J.P.; Bachert, P.; Direito, A.; Vandelanotte, C. Apps to improve diet, physical activity and sedentary behaviour in children and adolescents: A review of quality, features and behaviour change techniques. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 83. [Google Scholar] [CrossRef]
- Kostenius, C.; Hallberg, J.; Lindqvist, A.K. Gamification of health education: Schoolchildren’s participation in the development of a serious game to promote health and learning. Health Educ. 2018, 118, 354–368. [Google Scholar] [CrossRef]
- Kurtzman, G.W.; Day, S.C.; Small, D.S.; Lynch, M.; Zhu, J.; Wang, W.; Rareshide, C.A.L.; Patel, M.S. Social Incentives and Gamification to Promote Weight Loss: The LOSE IT Randomized, Controlled Trial. J. Gen. Intern. Med. 2018, 33, 1669–1675. [Google Scholar] [CrossRef]
- Roche, C.C.; Wingo, N.P.; Westfall, A.O.; Azuero, A.; Dempsey, D.M.; Willig, J.H. Educational Analytics: A New Frontier for Gamification? Comput. Inform. Nurs. 2018, 36, 458–465. [Google Scholar] [CrossRef]
- Klaassen, R.; Bul, K.C.M.; Op den Akker, R.; van der Burg, G.J.; Kato, P.M.; Di Bitonto, P. Design and evaluation of a pervasive coaching and gamification platform for young diabetes patients. Sensors 2018, 18, 402. [Google Scholar] [CrossRef]
- Sera, L.; Wheeler, E. Game on: The gamification of the pharmacy classroom. Curr. Pharm. Teach. Learn. 2017, 9, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.A.; Lohman, E.B.; Thorpe, D.; Johnson, E.G.; Medina, E.; Bradley, B. The effect of virtual reality gaming on dynamic balance in older adults. Age Ageing 2012, 41, 549–552. [Google Scholar] [CrossRef]
- Nicholson, V.P.; McKean, M.; Lowe, J.; Fawcett, C.; Burkett, B. Six weeks of unsupervised Nintendo Wii Fit gaming is effective at improving balance in independent older adults. J. Aging Phys. Act. 2015, 23, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Haruna, H.; Hu, X.; Chu, S.K.W.; Mellecker, R.R.; Gabriel, G.; Ndekao, P.S. Improving sexual health education programs for adolescent students through game-based learning and gamification. Int. J. Environ. Res. Public Health 2018, 15, 2027. [Google Scholar] [CrossRef]
- Desmet, A.; Shegog, R.; Van Ryckeghem, D.; Crombez, G.; De Bourdeaudhuij, I. A Systematic Review and Meta-analysis of Interventions for Sexual Health Promotion Involving Serious Digital Games. Games Health J. 2015, 4, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Williams, W.M.; Ayres, C.G. Can active video games improve physical activity in adolescents? A review of RCT. Int. J. Environ. Res. Public Health 2020, 17, 669. [Google Scholar] [CrossRef]
- Dos Santos, I.K.; da Silva Cunha de Medeiros, R.C.; De Medeiros, J.A.; De Almeida-Neto, P.F.; De Sena, D.C.S.; Cobucci, R.N.; Oliveira, R.S.; de Araújo Tinoco Cabral, B.G.; Dantas, P.M.S. Active video games for improving mental health and physical fitness—An alternative for children and adolescents during social isolation: An Overview. Int. J. Environ. Res. Public Health 2021, 18, 1641. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Sundal, D.; Foster, G.D.; Lent, M.R.; Vojta, D. Effects of a pediatricweight management program with and without active video games a randomized trial. JAMA Pediatr. 2014, 168, 407–413. [Google Scholar] [CrossRef]
- Patel, M.S.; Benjamin, E.J.; Volpp, K.G.; Fox, C.S.; Small, D.S.; Massaro, J.M.; Lee, J.J.; Hilbert, V.; Valentino, M.; Taylor, D.H.; et al. Effect of a game-based intervention designed to enhance social incentives to increase physical activity among families: The BE FIT randomized clinical trial. JAMA Intern. Med. 2017, 177, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Pakarinen, A.; Parisod, H.; Smed, J.; Salanterä, S. Health game interventions to enhance physical activity self-efficacy of children: A quantitative systematic review. J. Adv. Nurs. 2017, 73, 794–811. [Google Scholar] [CrossRef]
- Maddison, R.; Foley, L.; Ni Mhurchu, C.; Jiang, Y.; Jull, A.; Prapavessis, H.; Hohepa, M.; Rodgers, A. Effects of active video games on body composition: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 156–163. [Google Scholar] [CrossRef]
- Coknaz, D.; Mirzeoglu, A.D.; Atasoy, H.I.; Alkoy, S.; Coknaz, H.; Goral, K. A digital movement in the world of inactive children: Favourable outcomes of playing active video games in a pilot randomized trial. Eur. J. Pediatr. 2019, 178, 1567–1576. [Google Scholar] [CrossRef]
- Staiano, A.E.; Marker, A.M.; Beyl, R.A.; Hsia, D.S.; Katzmarzyk, P.T.; Newton, R.L. A randomized controlled trial of dance exergaming for exercise training in overweight and obese adolescent girls. Pediatr. Obes. 2017, 12, 120–128. [Google Scholar] [CrossRef]
- Miguel-Berges, M.L.; Santaliestra-Pasias, A.M.; Mouratidou, T.; Androutsos, O.; De Craemer, M.; Pinket, A.S.; Birnbaum, J.; Koletzko, B.; Iotova, V.; Usheva, N.; et al. Associations between food and beverage consumption and different types of sedentary behaviours in European preschoolers: The ToyBox-study. Eur. J. Nutr. 2017, 56, 1939–1951. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.A.; Lumsden, J.; Rivas, C.; Steed, L.; Edwards, L.A.; Thiyagarajan, A.; Sohanpal, R.; Caton, H.; Griffiths, C.J.; Munafò, M.R.; et al. Gamification for health promotion: Systematic review of behaviour change techniques in smartphone apps. BMJ Open 2016, 6, e012447. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. The Cochrane Collaboration. Available online: https://training.cochrane.org/handbook/current (accessed on 10 May 2021).
- Amaro, S.; Viggiano, A.; Di Costanzo, A.; Madeo, I.; Viggiano, A.; Baccari, M.E.; Marchitelli, E.; Raia, M.; Viggiano, E.; Deepak, S.; et al. Kalèdo, a new educational board-game, gives nutritional rudiments and encourages healthy eating in children: A pilot cluster randomized trial. Eur. J. Pediatr. 2006, 165, 630–635. [Google Scholar] [CrossRef]
- Bannon, K.; Schwartz, M.B. Impact of nutrition messages on children’s food choice: Pilot study. Appetite 2006, 46, 124–129. [Google Scholar] [CrossRef]
- Baños, R.M.; Cebolla, A.; Oliver, E.; Alcañiz, M.; Botella, C. Efficacy and acceptability of an Internet platform to improve the learning of nutritional knowledge in children: The ETIOBE mates. Health. Educ. Res. 2013, 28, 234–248. [Google Scholar] [CrossRef]
- Baranowski, T.; Baranowski, J.; Thompson, D.; Buday, R.; Jago, R.; Griffith, M.J.; Islam, N.; Nguyen, N.; Watson, K.B. Video game play, child diet, and physical activity behavior change a randomized clinical trial. Am. J. Prev. Med. 2011, 40, 33–38. [Google Scholar] [CrossRef]
- Chagas, C.M.D.S.; Melo, G.R.S.; Botelho, R.B.A.; Toral, N. Effects of the Rango Cards game intervention on food consumption, nutritional knowledge and self-efficacy in the adoption of healthy eating practices of high school students: A cluster randomised controlled trial. Public Health Nutr. 2020, 23, 2424–2433. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.W.; Watson, K.; Baranowski, T.; Baranowski, J.H.; Zakeri, I. Squire’s Quest: Intervention changes occurred at lunch and snack meals. Appetite 2005, 45, 148–151. [Google Scholar] [CrossRef]
- Cullen, K.W.; Liu, Y.; Thompson, D.I. Meal-Specific dietary changes from Squires Quest! II: A serious video game intervention. J. Nutr. Educ. Behav. 2016, 48, 326–330.e1. [Google Scholar] [CrossRef]
- Folkvord, F.; Anschütz, D.J.; Buijzen, M.; Valkenburg, P.M. The effect of playing advergames that promote energy-dense snacks or fruit on actual food intake among children. Am. J. Clin. Nutr. 2013, 97, 239–245. [Google Scholar] [CrossRef]
- Froome, H.M.; Townson, C.; Rhodes, S.; Franco-Arellano, B.; LeSage, A.; Savaglio, R.; Brown, J.M.; Hughes, J.; Kapralos, B.; Arcand, J. The effectiveness of the foodbot factory mobile serious game on increasing nutrition knowledge in children. Nutrients 2020, 12, 3413. [Google Scholar] [CrossRef]
- Gan, F.R.; Cunanan, E.; Castro, R. Effectiveness of healthy foodie nutrition game application as reinforcement intervention to previous standard nutrition education of school-aged children: A randomized controlled trial. J. ASEAN Fed. Endocr. Soc. 2019, 34, 144–152. [Google Scholar] [CrossRef]
- Hermans, R.C.J.; Van Den Broek, N.; Nederkoorn, C.; Otten, R.; Ruiter, E.L.M.; Johnson-Glenberg, M.C. Feed the Alien! The effects of a nutrition instruction game on children’s nutritional knowledge and food intake. Games Health J. 2018, 7, 164–174. [Google Scholar] [CrossRef]
- Lakshman, R.R.; Sharp, S.J.; Ong, K.K.; Forouhi, N.G. A novel school-based intervention to improve nutrition knowledge in children: Cluster randomised controlled trial. BMC Public Health 2010, 10, 123. [Google Scholar] [CrossRef]
- Lu, A.S.; Thompson, D.; Baranowski, J.; Buday, R.; Baranowski, T. Story immersion in a health videogame for childhood obesity prevention. Games Health J. 2012, 1, 37–44. [Google Scholar] [CrossRef]
- Mack, I.; Reiband, N.; Etges, C.; Eichhorn, S.; Schaeffeler, N.; Zurstiege, G.; Gawrilow, C.; Weimer, K.; Peeraully, R.; Teufel, M.; et al. The kids obesity prevention program: Cluster randomized controlled trial to Eevaluate a serious game for the prevention and treatment of childhood obesity. J. Med. Internet Res. 2020, 22, e15725. [Google Scholar] [CrossRef]
- Putnam, M.M.; Cotto, C.E.; Calvert, S.L. Character Apps for children’s snacks: Effects of character awareness on snack selection and consumption patterns. Games Health J. 2018, 7, 116–120. [Google Scholar] [CrossRef]
- Sharma, S.V.; Shegog, R.; Chow, J.; Finley, C.; Pomeroy, M.; Smith, C.; Hoelscher, D.M. Effects of the Quest to Lava Mountain Computer Game on dietary and physical activity behaviors of elementary school children: A pilot group-randomized controlled trial. J. Acad. Nutr. Diet. 2015, 115, 1260–1271. [Google Scholar] [CrossRef]
- Sharps, M.; Robinson, E. Encouraging children to eat more fruit and vegetables: Health vs. descriptive social norm-based messages. Appetite 2016, 100, 18–25. [Google Scholar] [CrossRef]
- Rosi, A.; Dall’Asta, M.; Brighenti, F.; Del Rio, D.; Volta, E.; Baroni, I.; Nalin, M.; Coti Zelati, M.; Sanna, A.; Scazzina, F. The use of new technologies for nutritional education in primary schools: A pilot study. Public Health 2016, 140, 50–55. [Google Scholar] [CrossRef]
- Spook, J.; Paulussen, T.; Kok, G.; Van Empelen, P. Evaluation of a serious self-regulation game intervention for overweight-related behaviors (“Balance It”): A pilot study. J. Med. Internet Res. 2016, 18. [Google Scholar] [CrossRef]
- Thompson, D.; Ferry, R.J.; Cullen, K.W.; Liu, Y. Improvement in fruit and vegetable consumption associated with more favorable energy density and nutrient and food group intake, but not kilocalories. J. Acad. Nutr. Diet. 2016, 116, 1443–1449. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, A.; Viggiano, E.; Di Costanzo, A.; Viggiano, A.; Andreozzi, E.; Romano, V.; Rianna, I.; Vicidomini, C.; Gargano, G.; Incarnato, L.; et al. Kaledo, a board game for nutrition education of children and adolescents at school: Cluster randomized controlled trial of healthy lifestyle promotion. Eur. J. Pediatr. 2015, 174, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, E.; Viggiano, A.; Di Costanzo, A.; Viggiano, A.; Viggiano, A.; Andreozzi, E.; Romano, V.; Vicidomini, C.; Di Tuoro, D.; Gargano, G.; et al. Healthy lifestyle promotion in primary schools through the board game Kaledo: A pilot cluster randomized trial. Eur. J. Pediatr. 2018, 177, 1371–1375. [Google Scholar] [CrossRef]
- Zask, A.; Adams, J.K.; Brooks, L.O.; Hughes, D.F. Tooty Fruity Vegie: An obesity prevention intervention evaluation in Australian preschools. Health Promot. J. Aust. 2012, 23, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.A.; Madden, G.J.; Wengreen, H.J. The FIT Game: Preliminary evaluation of a gamification approach to increasing fruit and vegetable consumption in school. Prev. Med. 2014, 68, 76–79. [Google Scholar] [CrossRef]
- Torkar, G.; Pintarič, M.; Koch, V. Fruit and vegetable playing cards: Utility of the game for nutrition education. Nutr. Food Sci. 2010, 40, 74–80. [Google Scholar] [CrossRef]
- Farrow, C.; Belcher, E.; Coulthard, H.; Thomas, J.M.; Lumsden, J.; Hakobyan, L.; Haycraft, E. Using repeated visual exposure, rewards and modelling in a mobile application to increase vegetable acceptance in children. Appetite 2019, 141, 104327. [Google Scholar] [CrossRef]
- Desmet, A.; Liu, Y.; De Bourdeaudhuij, I.; Baranowski, T.; Thompson, D. The effectiveness of asking behaviors among 9–11 year-old children in increasing home availability and children’s intake of fruit and vegetables: Results from the Squire’s Quest II self-regulation game intervention. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 51. [Google Scholar] [CrossRef]
- Del Río, N.G.; González-González, C.S.; Martín-González, R.; Navarro-Adelantado, V.; Toledo-Delgado, P.; García-Peñalvo, F.; Del Río, N.G.; González-González, C.S.; Martín-González, R.; Navarro-Adelantado, V.; et al. Effects of a gamified educational program in the nutrition of children with obesity. J. Med. Syst. 2019, 43, 198. [Google Scholar] [CrossRef] [PubMed]
- Folkvord, F.; Anastasiadou, D.T.; Anschütz, D. Memorizing fruit: The effect of a fruit memory-game on children’s fruit intake. Prev. Med. Rep. 2017, 5, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Bhatt, R.; Vazquez, I.; Cullen, K.W.; Baranowski, J.; Baranowski, T.; Liu, Y. Creating action plans in a serious video game increases and maintains child fruit-vegetable intake: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Beemer, L.R.; Ajibewa, T.A.; DellaVecchia, G.; Hasson, R.E. A pilot intervention using gamification to enhance student participation in classroom activity breaks. Int. J. Environ. Res. Public Health 2019, 16, 4082. [Google Scholar] [CrossRef] [PubMed]
- Pampaloni, B.; Cianferotti, L.; Gronchi, G.; Bartolini, E.; Fabbri, S.; Tanini, A.; Brandi, M. Growing strong and healthy with Mister Bone: An educational program to have strong bones later in life. Nutrients 2015, 7, 9985–9998. [Google Scholar] [CrossRef]
- Majumdar, D.; Koch, P.A.; Lee, H.; Contento, I.R.; Islas-Ramos, A.D.L.; Fu, D. “Creature-101”: A serious game to promote energy balance-related behaviors among middle school adolescents. Games Health J. 2013, 2, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Ezezika, O.; Oh, J.; Edeagu, N.; Boyo, W. Gamification of nutrition: A preliminary study on the impact of gamification on nutrition knowledge, attitude, and behaviour of adolescents in Nigeria. Nutr. Health 2018, 24, 137–144. [Google Scholar] [CrossRef]
- Pérez López, I.J.; Delgado Fernández, M. Un juego de cartas durante los recreos escolares mejora los hábitos alimentarios en adolescentes. Nutr. Hosp. 2012, 27, 2055–2065. [Google Scholar] [CrossRef]
- Peng, W. Design and evaluation of a computer game to promote a healthy diet for young adults. Health Commun. 2009, 24, 115–127. [Google Scholar] [CrossRef]
- Ashton, L.M.; Morgan, P.J.; Hutchesson, M.J.; Rollo, M.E.; Collins, C.E. Feasibility and preliminary efficacy of the ’HEYMAN healthy lifestyle program for young men: A pilot randomised controlled trial. Nutr. J. 2017, 16, 2. [Google Scholar] [CrossRef]
- Gómez-del-Río, N.; González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; García-Peñalvo, F. Health promotion for childhood obesity: An approach based on self-tracking of data. Sensors 2020, 20, 3778. [Google Scholar] [CrossRef]
- Dias, M.; Agante, L. Can advergames boost children’s healthier eating habits? A comparison between healthy and non-healthy food. J. Consum. Behav. 2011, 10, 152–160. [Google Scholar] [CrossRef]
- Hassanzadeh-Rostami, Z.; Mirshekari, M.; Ranjbaran, H.; Khosravi, S.; Faghih, S. Effect of game-based nutrition education on nutritional knowledge of preschool children nutrition education knowledge game children. Int. J. Nutr. Sci. March. 2018, 3, 50–55. [Google Scholar]
- Azevedo, J.; Padrão, P.; Gregório, M.J.; Almeida, C.; Moutinho, N.; Lien, N.; Barros, R. A web-based gamification program to improve nutrition literacy in families of 3- to 5-year-old children: The Nutriscience Project. J. Nutr. Educ. Behav. 2019, 51, 326–334. [Google Scholar] [CrossRef]
- Gómez-García, G.; Marín-Marín, J.A.; Romero-Rodríguez, J.-M.; Ramos Navas-Parejo, M.; Rodríguez Jiménez, C. Effect of the flipped classroom and gamification methods in the development of a didactic unit on healthy habits and diet in primary education. Nutrients 2020, 12, 2210. [Google Scholar] [CrossRef] [PubMed]
- Blok, A.C.; Sadasivam, R.S.; Amante, D.J.; Kamberi, A.; Flahive, J.; Morley, J.; Conigliaro, J.; Houston, T.K. Gamification to motivate the unmotivated smoker: The “Take a Break” digital health intervention. Games Health J. 2019, 8, 275–284. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Shellenbarger, T. Gamification of nursing education with digital badges. Nurse Educ. 2018, 43, 78–82. [Google Scholar] [CrossRef]
- De Lepeleere, S.; De Bourdeaudhuij, I.; Cardon, G.; Verloigne, M. The effect of an online video intervention ‘Movie Models’ on specific parenting practices and parental self-efficacy related to children’s physical activity, screen-time and healthy diet: A quasi experimental study. BMC Public Health 2017, 17, 366. [Google Scholar] [CrossRef]
- Villasana, M.V.; Pires, I.M.; Sá, J.; Garcia, N.M.; Zdravevski, E.; Chorbev, I.; Lameski, P.; Flórez-Revuelta, F. Promotion of healthy nutrition and physical activity lifestyles for teenagers: A systematic literature review of the current methodologies. J. Pers. Med. 2020, 10, 12. [Google Scholar] [CrossRef]
- Bell, B.M.; Martinez, L.; Gotsis, M.; Lane, H.C.; Davis, J.N.; Antunez-Castillo, L.; Ragusa, G.; Spruijt-Metz, D. Virtual sprouts: A virtual gardening pilot intervention increases self-efficacy to cook and eat fruits and vegetables in minority youth. Games Health J. 2018, 7, 127–135. [Google Scholar] [CrossRef]
- Hawkes, C.; Demaio, A.R.; Branca, F. Double-duty actions for ending malnutrition within a decade. Lancet Glob. Health 2017, 5, e745–e746. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors, (Year), Country | Design | Sample | Aim | Intervention | Duration | Measurement | Main Outcomes M(SD) | EL/RG |
|---|---|---|---|---|---|---|---|---|
| Amaro et al. [27] (2006), Italy | RCT | N = 241 children Age 11–14 year n CG = 88 n IG = 153 | To test the changes in nutrition knowledge and dietary behaviour | CG: no intervention IG: “Kalèdo” Nutrition board-game (play session 15–30 min) | 24 weeks | Questionnaires on nutritional knowledge and food intake BMI | Nutrition knowledge Significant difference between IG and CG at post-assessment (p < 0.05). Adjusted means were 11.24 (95% CI 10.68–11.80) for the IG and 9.24 (95% CI 8.50–9.98) for CG Dietary intake Significant difference between IG and CG at post-assessment (p < 0.01) for the variable vegetable intake. Adjusted mean number of servings per week was 3.7 (95% CI 3.5–4.1) for IG and 2.8 (95% CI 2.4–3.3) for CG BMI No significant difference between IG and CG at post-assessment. Adjusted means were 0.345 (95% CI 0.29–0.39) for IG and 0.405 (95% CI 0.34–0.46) for CG | 1b/A |
| Bannon et al. [28] (2006), USA | RCT | N = 50 children Mean age 5 years n CG = 18 n IG1 = 14 n IG2 = 18 | To test the influence of nutrition message framing on snack choice among children | CG: control video IG1: gain-framed nutrition video message IG2: loss-framed nutrition video message | 60 s video time | Food preference questionnaire Healthy food questionnaire | Gain- and loss-framed messages promoting healthy snacks have the potential to positively influence children’s behaviour In IG, 56% chose apples rather than animal crackers; in CG, only 33% chose apples | 1b/A |
| Baños et al. [29] (2013), Spain | RCT | N = 228 children Age 10–13 years n CG = 155 n IG = 73 | To study an online game to improve children’s nutritional knowledge | CG: paper–pencil intervention IG: “ETIOBE Mates” broader e-therapy platform educational website including serious games | 2 weeks (unlimited sessions) | Nutritional knowledge questionnaire | Baseline Nutritional knowledge CG: 6.25 (1.3) IG: 6.46 (1.3) 2 weeks follow-up Nutritional knowledge CG: 6.42 (1.5) IG: 6.94 (1.4) | 1b/A |
| Baranowski et al. [30] (2011), USA | RCT | N = 133 children Age 10–12 years n CG = 40 n IG = 93 | To promote behaviour change on children’s diet | CG: games on popular websites IG: “Escape from Diab” + “Nanoswarm: Invasion from Inner Space” Video-games (9 sessions of 40 min) | 2 months | BMI Mean levels of FV, non-fat vegetables, total energy | Baseline CG Body Composition BMI %: 75.12 (1.04) BMI z-score: 0.78 (0.03) Diet (Servings) FV: 1.56 (0.18) Total Energy (kcal): 1657 (58) IG Body Composition BMI %: 77.41 (0.74) BMI z-score: 0.85 (0.02) Diet (Servings) FV: 1.88 (0.13) Total Energy (kcal): 1604 (41) 2 months follow-up CG Body Composition BMI %: 75.98 (1.09) BMI z-score: 0.80 (0.03) Diet (Servings) FV: 1.48 (0.19) Total Energy (kcal): 1653 (63) IG Body Composition BMI %: 77.28 (0.75) BMI z-score: 0.83 (0.02) Diet (Servings) FV: 2.15 (0.13) Total Energy (kcal): 1632 (42) | 1b/A |
| Chagas et al. [31] (2020), Brazil | RCT | N = 319 adolescents Mean age 15.8 years n CG = 202 n IG = 117 | To assess the impact of a game-based nutritional intervention on food consumption, nutritional knowledge, and self-efficacy | CG: no intervention IG: “Rango Cards”, a digital game (unlimited session) | 17 days | Nutritional knowledge questionnaire | Baseline Nutritional knowledge CG: 4.3 (0.5) IG: 4.2 (0.4) Follow-up Nutritional knowledge CG: 4.2 (0.6) IG: 4.2 (0.5) | 1b/A |
| Cullen et al. [32] (2005), USA | RCT | N = 1489 children Age 8–12 years n CG = 740 n IG = 749 | To assess changes in nutritional practices | CG: no intervention IG: “Squire’s Quest!” multimedia game (10 sessions of 25 min) | 5 weeks | Servings of fruit, 100% juice, and vegetables consumed | After intervention, at snacks, the difference in means between IG and CG was significantly higher for fruit and 100% fruit juice, and for regular non-fried vegetables but not for other juice and vegetables | 1b/A |
| Cullen et al. [33] (2016), USA | RCT | N = 387 children Age 9–11 years n CG = 97 n IG1 action plans = 98 n IG2 coping plans = 95 n IG3 action + coping plans = 97 | To examine an online video-game to promote fruit-vegetable consumption changes | CG: no intervention IG: “Squire’s Quest II” online video-game. 10 sessions (25 min each) for 5 weeks | 5 weeks 6 months follow up | Servings of fruit, 100% juice, and vegetables consumed | At 6 months, vegetable intake at dinner was significantly increased in action and coping groups. Overall, there were significant increases in fruit consumption at breakfast (p = 0.009), lunch (p = 0.014), and as a snack (p < 0.001) | 1b/A |
| Folkvord et al. [34] (2013), Netherlands | RCT | N = 270 children Age 8–10 years n CG = 69 n IG1 = 69 n IG2 = 67 n IG3 = 65 | To examine the effect of advergames that promote intake of energy-dense snacks or fruit on children | CG: no intervention IG1: advergame that promoted energy-dense snacks IG1: advergame that promoted fruit IG3: non-food products | - | Caloric intake | Children who played an advergame that promoted food (energy-dense snacks or fruit) ate significantly more than did the children who played an advergame that promoted non-food products (p < 0.01) and also ate. Sex (male) (p < 0.05), hunger (p < 0.01), and age (p < 0.05) were significantly related to energy-dense calorie intake | 1b/A |
| Froome et al. [35] (2020), Canada | RCT | N = 73 children Age 8–10 years n CG = 34 n IG = 39 | To determine improvement in children’s nutritional knowledge | CG: cooking game “My Salad Shop Bar” IG: game mobile application Foodbot Factory (learning module of drinks, whole-grain food, vegetables and fruits, animal protein, plant-based protein + voiceover) (10–15 min each day) | 5 days | Nutrition knowledge | Baseline Nutrition knowledge CG: 10.2 (3.1) IG: 10.3 (2.9) Day 5 Nutrition knowledge CG: 10.4 (3.2) IG: 13.5 (3.8) | 1b/A |
| Gan et al. [36] (2019), Philippines | RCT | N = 360 children Age 7–10 years n CG = 180 n IG = 180 | To increase nutrition knowledge | CG: no intervention IG: “Healthy Foodie” nutrition game (25 to 40 min to complete the game) | 2 weeks | Nutrition knowledge questionnaire | Baseline Food Group Knowledge score CG: 9.55 (3.72) IG: 9.08 (3.48) Food Frequency Knowledge score CG: 9.67 (2.79) IG: 9.16 (2.55) 2 weeks follow-up Food Group Knowledge score CG: 8.66 (3.82) IG: 11.42 (3.25) Food Frequency Knowledge score CG: 9.22 (2.75) IG: 10.55 (2.28) | 1b/A |
| Hermans et al. [37] (2018), USA | RCT | N = 108 children Age 10–13 years n CG = 58 n IG = 50 | To test the short-term effectiveness of a videogame designed to teach elementary school children about nutrition and healthy food choices | CG: web-based nutrition game “Super Shopper” (not designed to educate children in healthy food choices) IG: gameplay of An Alien Health Game “Feed the Alien!” (designed to educate children in healthy food choices and the main function of the five most important macronutrients). 1 h of gameplay (30 min session) | 2 weeks | Nutritional knowledge Food intake | Nutritional knowledge IG had better knowledge at immediate post-test, (p < 0.001) but not at 2-week follow-up (p = 0.999) Food intake Participants in both conditions ate more energy-dense foods at 2-week follow-up than at immediate post-test (p < 0.001). | 1b/A |
| Lakshman et al. [38] (2010), UK | RCT | N = 1133 children Age 9–11 years n CG = 631 n IG = 502 | To increase nutrition knowledge | CG: traditional healthy eating curriculum IG: “Top Grub”: card nutrition game | 9 weeks | Nutrition knowledge questionnaire Attitudes to healthy eating | Baseline Nutrition knowledge Total score CG: 27.3 (2) IG: 28.3 (1.1) Balanced diet domain (max 0.15 points) CG: 11.3 (0.9) IG: 11.6 (0.4) Ability to identify healthier foods CG: 11.6 (0.9) IG: 12.1 (0.6) 9 weeks Nutrition knowledge Total score CG: 27.6 (2.1) IG: 29.2 (0.8) Balanced diet domain (max 0.15 points) CG: 11.5 (0.9) IG: 12.1 (0.5) Ability to identify healthier foods CG: 11.6 (1.0) IG: 12.1 (0.4) | |
| Lu et al. [39] (2012), USA | RCT | N = 153 children Age 10–12 years n CG = 50 n IG = 103 | To analyse positive health outcomes | CG: no intervention IG: health videogame “Escape from Diab”. 9 sessions of 40 min | 2 months | Fruit, vegetables, and water consumption | Baseline vs. 2 months follow-up (Only for IG) Fruit/Vegetables Preference 68.36 (13.53)/71.54 (15.49) Water Preference 2.64 (0.65)/2.59 (0.72) Intrinsic Motivation for Fruit 5.89 (1.94)/6.15 (2.18) Intrinsic Motivation for Vegetable 3.76 (1.82)/3.73 (1.94) Intrinsic Motivation for Water 5.19 (1.95)/5.51 (1.91) Fruit Self-Efficacy 9.49 (2.12)/10.39 (2.29) Vegetable Self-Efficacy 4.69 (2.24)/5.32 (2.22) Water Self-Efficacy 3.56 (1.39)/3.69 (1.54) Story immersion correlated positively (p < 0.03) with an increase in Fruit and Vegetable Preference (r = 0.27), Intrinsic Motivation for Water (r = 0.29), Vegetable Self-Efficacy (r = 0.24) | 1b/A |
| Mack et al. [40] (2020), Germany | RCT | N = 82 children Age 9–12 year n CG = 40 n IG = 42 | To evaluate the gain in knowledge about important lifestyle factors with the focus on nutrition | CG: brochure healthy lifestyle IG: nutrition games modules (2 sessions of 45 min) | 2 weeks | Maintenance of knowledge questionnaire Food frequency questionnaire Healthy nutrition index | Baseline Knowledge score % Food pyramid score CG: 49 (14) IG: 50 (13) % of dietary energy-density score CG: 41 (19) IG: 51 (18) Healthy nutrition index (reported by children) CG: 8.9 (2.2) IG: 8.8 (2.1) 4 weeks follow-up Knowledge score% Food pyramid CG: 54 (12) IG: 77 (12) % of dietary energy-density score CG: 46 (22) IG: 64 (17) Healthy nutrition index (reported by children) CG: 9.3 (2.5) IG: 9.5 (2.2) | 1b/A |
| Putnam et al. [41] (2018), USA | RCT | N = 132 children Age 4–5 years n CG = 44 n IG = 88 | To encourage healthier snack selection and consumption | CG: game adventure app IG: game adventure app with “Dora the Explorer” | - | Snack choices | Children who were aware of Dora were 10.34 times more likely to select healthier snack items than those who were unaware of her (p = 0.008) | 1b/A |
| Sharma [42] (2015), USA | RCT | N = 94 children Age 8–12 years n CG = 50 n IG = 44 | To evaluate dietary behaviours | CG: usual programs IG: “Quest to Lava Mountain” adventure game (90 min play game) | 6 weeks | Dietary Intake | Baseline Dietary intake fruit (servings per 1000 kcal) CG: 0.81 (0.67) IG: 0.84 (0.67) Vegetables (servings per 1000 kcal) CG: 0.51 (0.33) IG: 0.56 (0.42) Dietary fibre (g/1000 kcal) CG: 8.82 (2.46) IG: 8.29 (2.59) Sugars (g/1000 kcal) CG: 55.33 (16.94) IG: 55.35 (13.47) Total fat (g/1000 kcal) CG: 32.31 (6.01) IG: 32.84 (5.45) Energy (kcal) CG: 1632.51 (443.37) IG: 1415.49 (412.02) Carbohydrates (g/1000 kcal) CG: 51.83 (7.97) IG: 49.79 (6.98) Protein (g/1000 kcal) CG: 15.86 (3.71) IG: 17.37 (3.80) Calcium (mg/1000 kcal) CG: 520.92 (180.32) IG: 597.36 (186.07) 6 weeks follow-up Dietary intake fruit (servings per 1000 kcal) CG: 0.79 (0.68) IG: 0.71(0.67) Vegetables (servings per 1000 kcal) CG: 0.45 (0.37) IG: 0.50 (0.44) Dietary fibre (g/1000 kcal) CG: 7.96 (2.82) IG: 8.35 (2.61) Sugars (g/1000 kcal) CG: 60.94 (15.97) IG: 50.45 (18.93) Total fat (g/1000 kcal) CG: 31.90 (6.83) IG: 34.78 (6.83) Energy (kcal) CG: 1331.46 (524.92) IG: 1304.11 (571.60) Carbohydrates (g/1000 kcal) CG: 52.40 (8.31) IG: 48.49 (9.03) Protein (g/1000 kcal) CG: 15.70 (4.21) IG: 16.72 (5.72) Calcium (mg/1000 kcal) CG: 561.83 (262.32) IG: 538.15 (168.55) | 1b/A |
| Sharps et al. [43] (2016), UK | RCT | N = 143 children Age 6–11 years n CG = 46 n IG1 = 49 n IG2 = 48 | To increase intake of fruit and vegetables through board games | CG: non-food-related game IG1: descriptive social norm-based message. Fruit and vegetables related game IG2: health message and image condition. Fruit and vegetables related game 7 min of playtime every day | - | Food intake | Food intake Significant main effect of condition on fruit and vegetable intake (p = 0.01). IG2 ate significantly more fruit and vegetables than children in CG (p = 0.009). There was no significant main effect of conditioning on high-calorie snack food intake (p = 0.99) | 1b/A |
| Rosi et al. [44] (2016), Italy | RCT | N = 145 children Age 8–10 years n CG = 33 n IG1 = 58 n IG2 = 54 | To improve nutritional education | CG: no intervention IG1: “Master of Taste” nutritional educator IG2: “Master of Taste” supported by a humanoid robot | 1 year | Cultural–nutritional awareness factor (score of the nutritional knowledge level) | Baseline Cultural–nutritional awareness factor CG: 5.5 (1.5) IG1: 6.2 (1.7) IG2: 5.9 (1.3) 1 year follow-up Cultural–nutritional awareness factor CG: 6.1 (1.4) IG1: 6.9 (1.1) IG2: 6.9 (1.1) | 1b/A |
| Spook et al. [45] (2016), Netherlands | RCT | N = 231 adolescents Mean age 17.28 years n CG = 126 n IG = 105 | To assess dietary intake | CG: no intervention IG: “Balance It”, interactive multimedia game (unlimited sessions) | 4 weeks | Dietary intake (fruit and vegetable consumption, snack consumption, and soft drink consumption) | Baseline Behavioural outcomes (mean portion/day) Fruit intake CG: 0.80 (0.68) IG: 0.81 (0.68) Vegetable intake CG: 1.32 (0.38) IG: 1.26 (0.33) Snack consumption CG: 0.98 (0.51) IG: 0.91 (0.50) Soft drink consumption CG: 1.11 (0.59) IG: 1.07 (0.53) 4 weeks follow-up Behavioural outcomes (mean portion/day) Fruit intake CG: 0.81 (0.62) IG: 1.05 (0.75) Vegetable intake CG: 1.28 (0.36) IG: 1.21 (0.41) Snack consumption CG: 0.90 (0.48) IG: 0.86 (0.51) Soft drink consumption CG: 1.07 (0.57) IG: 0.92 (0.57) | 1b/A |
| Thompson et al. [46], (2016) USA | RCT | N = 387 children Aged 9–11 years n CG = 97 n IG1 action = 98 n IG2 coping = 95 n IG3 action + coping = 97 | To evaluate the dietary intake of healthy children | CG: no intervention Intervention: serious game “Squire’s Quest! II” (10 sessions of 25 min) IG1 Action: set a goal and then created an action plan to meet the goal. IG2: Coping, a goal to eat more FV and then to create a coping plan IG3: Both IG1 + IG2 | 5 weeks | Fruit and vegetable intake | Baseline Energy (kcal) CG: 1496 (34.71) IG1: 1477 (34.93) IG2: 1487 (35.04) IG3: 1476 (35.13) Vitamin C (mg) CG: 96.89 (7.97) IG1: 74.25 (8.01) IG2: 73.37 (8.03) IG3: 84.99 (8.04) Sodium (mg) CG: 2655 (45.33) IG1:2626 (45.58) IG2: 2646 (45.71) IG3: 2623 (45.81) Potassium (mg) CG: 1732 (38.1) IG1: 1668 (38.35) IG2: 1693 (38.48) IG3: 1823 (38.59) Total dietary fibre (g) CG: 11.02 (0.34) IG1: 11.33 (0.35) IG2: 11.16 (0.35) IG3: 11.4 (0.35) Added sugars (g) CG: 54.74 (2.25) IG1: 58.69 (2.26) IG2: 56.83 (2.26) IG3: 58.16 (2.27) 6 months follow-up Energy (kcal) CG: 1523 (39.09) IG1: 1444 (38.94) IG2: 1510 (39.79) IG3: 1482 (39.31) Vitamin C (mg) CG: 92.66 (11.98) IG1: 87.22 (11.91) IG2: 96.91 (12.11) IG3: 104.47 (11.98) Sodium (mg) CG: 2740 (50.96) IG1: 2562 (50.70) IG2: 2667 (51.91) IG3: 2670 (51.14) Potassium (mg) CG: 1789 (45.66) IG1: 1905 (45.47) IG2: 1854 (46.42) IG3: 1858 (45.86) Total dietary fibre (g) CG: 11.5 (0.42) IG1: 12.75 (0.42) IG2: 12.14 (0.42) IG3: 12.15 (0.42) Added sugars (g) CG: 48.2 (2.25) IG1: 50.79 (2.24) IG2: 53.83 (2.29) IG3: 50.13 (2.26) | 1b/A |
| Viggiano et al. [47] (2015), Italy | RCT | N = 3110 children Age 9–19 years n CG = 1447 n IG = 1663 | To promote nutrition education and to improve dietary behaviour | CG: no intervention IG: “Kalèdo” nutrition board-game (15–30 min session) | 20 weeks | BMI z-score Nutrition Knowledge | Baseline Normal Weight CG: 52.55% IG: 51.6% Overweight CG: 32.6% IG: 34.9% Obesity CG: 14.8% IG: 13.3% BMI z-score CG: 0.59 IG: 0.58 Nutrition Knowledge CG: 4.4 (4.2–4.5) IG: 4.2 (4.1–4.4) Food Habits CG: 27.3 IG: 27.2 18 months follow-up Normal Weight CG: 52.55% IG: 63.55% Overweight CG: 32% IG: 27.8% Obesity CG: 15.45% IG: 8.65% BMI z-score CG: 0.58 IG: 0.34 Nutrition Knowledge CG: 5.6 (5.4–5.7) IG: 6.2 (6.1–6.4) Food Habits CG: 28.6 IG: 29.3 | 1b/A |
| Viggiano et al. [48] (2018), Italy | RCT | N = 1007 children Age 7–11 years n CG: 356 n IG: 651 | To improve knowledge in nutrition and to promote a healthy lifestyle | CG: no intervention IG: “Kalèdo” nutrition board-game. 20 sessions of 15–30 min | 20 weeks | Food frequency consumption BMI z-score | 8 months follow-up IG significantly increased the consumption of healthy food (p < 0.01) compared to CG 18 months follow-up The increase in the consumption of healthy foods in GI was maintained over time (p < 0.01). Significantly higher consumption of healthy food in girls (mean 9.41; CI 95% 7.61–11.22) compared to boys (mean 7.11; CI 95% 5.46–8.76). IG decreased junk food consumption (p < 0.01) compared to the CG | 1b/A |
| Zask et al. [49] (2012), Australia | RCT | N = 1005 children Age 3–6 years n CG = 537 n IG = 468 | To increasing fruit and vegetable intake and decreasing unhealthy food consumption | CG: no intervention IG: “Tooty Fruity Vegie” a game health promotion program | 10 months | Dietary intake BMI | Baseline Number of fruit and vegetables serves CG: 1.95 (0.17) IG: 1.91 (0.13) BMI z-scores CG: 0.11 (0.08) IG: 0.14 (0.06) Mean waist circumference in cm CG: 52.33 (0.29) IG: 52.54 (0.23) 10 months follow-up Number of fruit and vegetables serves CG: 1.73 (0.12) IG: 2.31 (0.11) BMI z- scores CG: 0.24 (0.09) IG: 0.11 (0.06) Mean waist circumference in cm CG: 53.49 (0.28) IG: 52.89 (0.29) | 1b/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suleiman-Martos, N.; García-Lara, R.A.; Martos-Cabrera, M.B.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A.; Gómez-Urquiza, J.L. Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2478. https://doi.org/10.3390/nu13072478
Suleiman-Martos N, García-Lara RA, Martos-Cabrera MB, Albendín-García L, Romero-Béjar JL, Cañadas-De la Fuente GA, Gómez-Urquiza JL. Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(7):2478. https://doi.org/10.3390/nu13072478
Chicago/Turabian StyleSuleiman-Martos, Nora, Rubén A. García-Lara, María Begoña Martos-Cabrera, Luis Albendín-García, José Luis Romero-Béjar, Guillermo A. Cañadas-De la Fuente, and José L. Gómez-Urquiza. 2021. "Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis" Nutrients 13, no. 7: 2478. https://doi.org/10.3390/nu13072478
APA StyleSuleiman-Martos, N., García-Lara, R. A., Martos-Cabrera, M. B., Albendín-García, L., Romero-Béjar, J. L., Cañadas-De la Fuente, G. A., & Gómez-Urquiza, J. L. (2021). Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients, 13(7), 2478. https://doi.org/10.3390/nu13072478