
Eating Speed, Physical Activity, and Cardiorespiratory Fitness Are Independent Predictors of Metabolic Syndrome in Korean University Students



Abstract
:1. Introduction
2. Materials and Methods
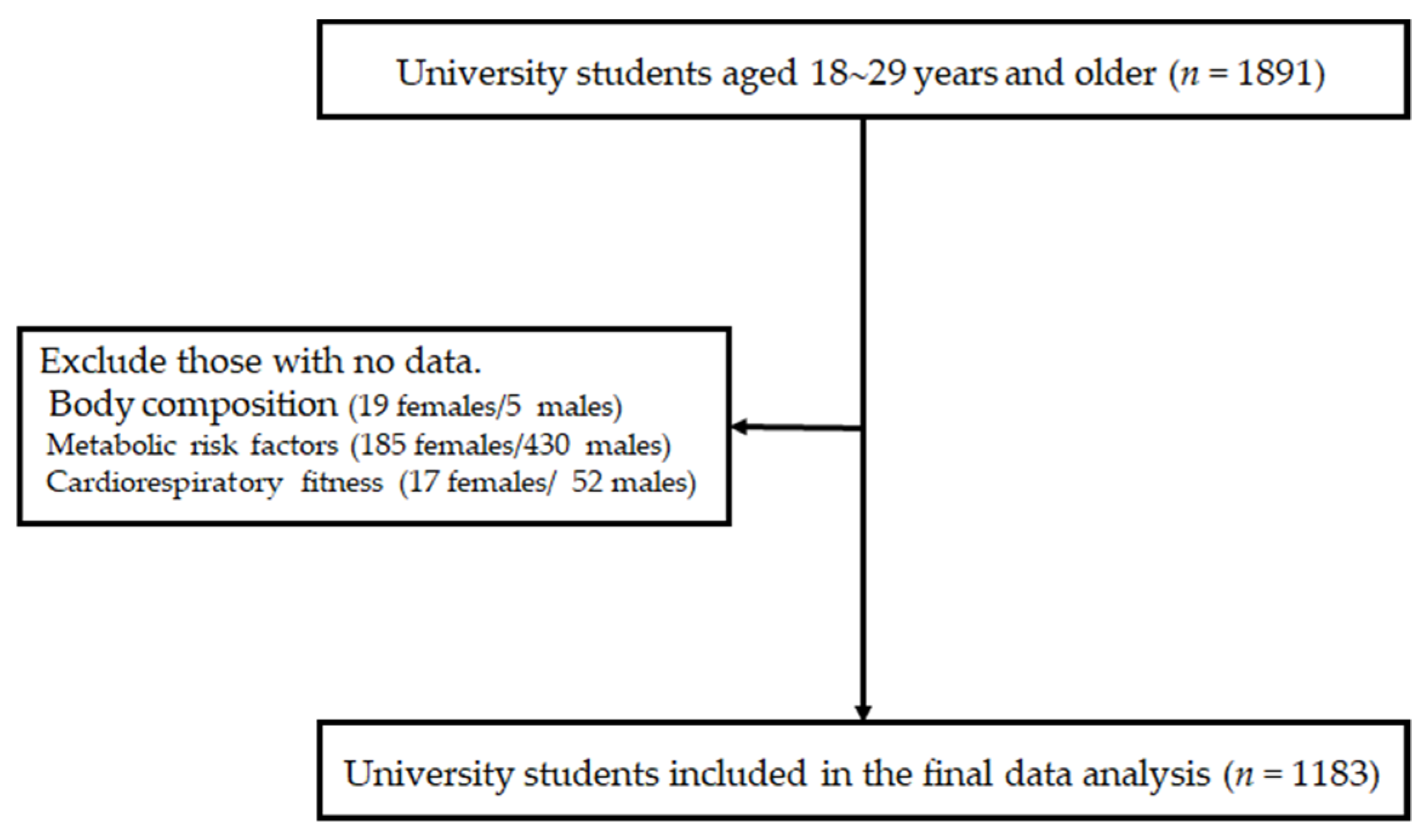
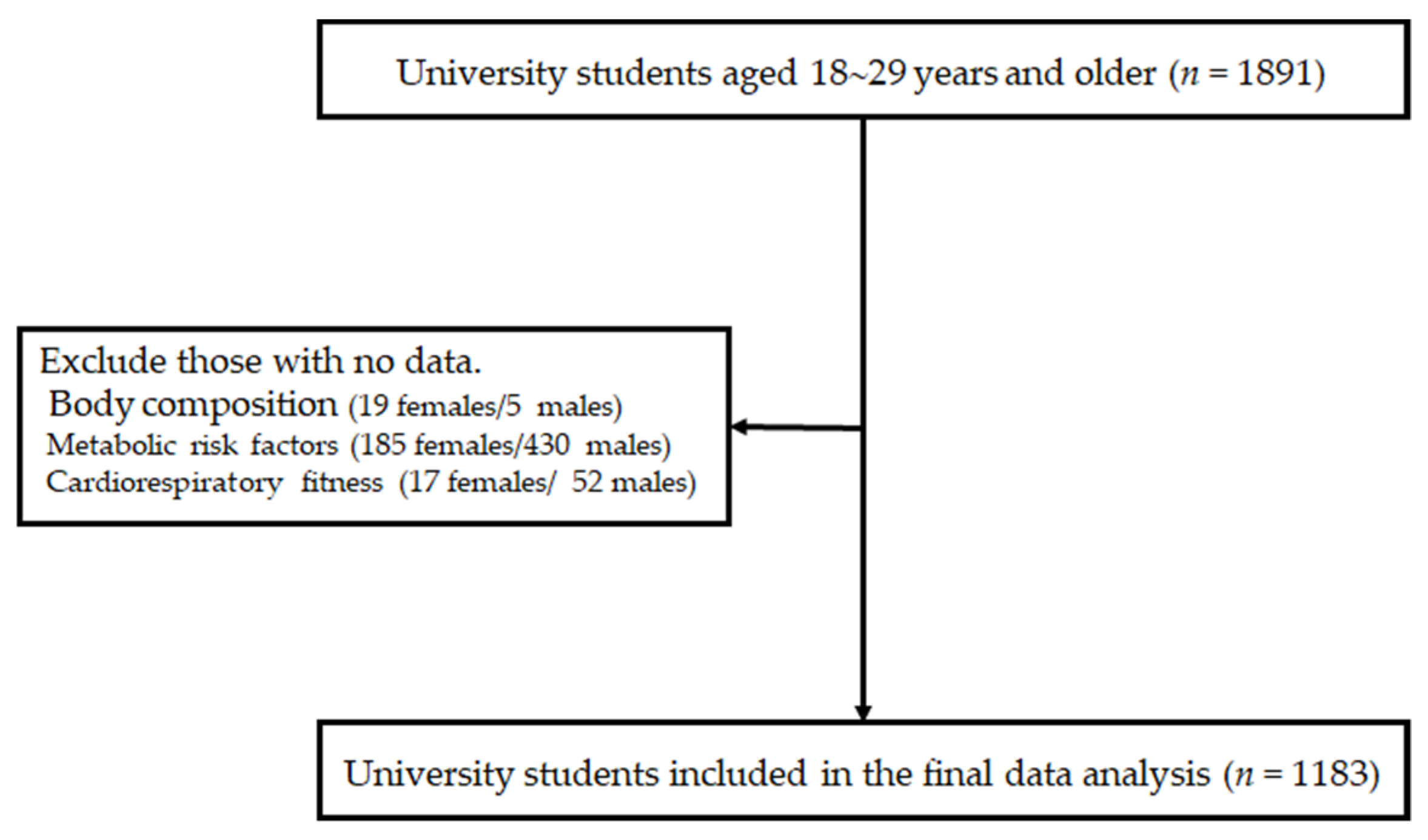
2.1. Subjects
2.2. Variables
2.2.1. Assessment of Anthropometrics and Definition of Metabolic Syndrome
2.2.2. Questionnaire
2.2.3. Measurement of Cardiorespiratory Fitness
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tune, J.D.; Goodwill, A.G.; Sassoon, D.J.; Mather, K.J. Cardiovascular consequences of metabolic syndrome. Transl. Res. 2017, 183, 57–70. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.A.; Lee, J.H.; Lim, S.Y.; Ha, H.S.; Kwon, H.S.; Park, Y.M.; Lee, W.C.; Kang, M.I.; Yim, H.W.; Yoon, K.H.; et al. Metabolic syndrome as a predictor of type 2 diabetes, and its clinical interpretations and usefulness. J. Diabetes Investig. 2013, 4, 334–343. [Google Scholar] [CrossRef]
- Neto, A.S.; Sasaki, J.E.; Mascarenhas, L.P.; Boguszewski, M.C.; Bozza, R.; Ulbrich, A.Z.; da Silva, S.G.; de Campos, W. Physical activity, cardiorespiratory fitness, and metabolic syndrome in adolescents: A cross-sectional study. BMC Public Health 2011, 11, 674. [Google Scholar] [CrossRef] [Green Version]
- Renninger, M.; Hansen, B.H.; Steene-Johannessen, J.; Kriemler, S.; Froberg, K.; Northstone, K.; Sardinha, L.; Anderssen, S.A.; Andersen, L.B.; Ekelund, U.; et al. Associations between accelerometry measured physical activity and sedentary time and the metabolic syndrome: A meta-analysis of more than 6000 children and adolescents. Pediatr. Obes. 2020, 15, e12578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.; Lee, J.; Park, J.; Lee, M.; Kim, J.Y.; Kim, K.C.; Kim, S.H.; Im, J.A.; Chu, S.H.; Suh, S.H.; et al. Association between cardiorespiratory fitness and the prevalence of metabolic syndrome among Korean adults: A cross sectional study. BMC Public Health 2014, 14, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical activity, cardiorespiratory fitness, and the metabolic syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Yang, J.; Su, J.; Qin, Y.; Shen, C.; Li, Y.; Lu, S.; Pan, E.; Gao, Y.; Miao, D.; et al. Physical activity, sedentary time and their associations with clustered metabolic risk among people with type 2 diabetes in Jiangsu province: A cross-sectional study. BMJ Open 2019, 9, e027906. [Google Scholar] [CrossRef]
- Miller, J.M.; Street, B.D. Metabolic syndrome and physical activity levels in college students. Metab. Syndr. Relat. Disord. 2019, 17, 431–435. [Google Scholar] [CrossRef]
- LaMonte, M.J.; Barlow, C.E.; Jurca, R.; Kampert, J.B.; Church, T.S.; Blair, S.N. Cardiorespiratory fitness is inversely associated with the incidence of metabolic syndrome: A prospective study of men and women. Circulation 2005, 112, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Wewege, M.A.; Thom, J.M.; Rye, K.A.; Parmenter, B.J. Aerobic, resistance or combined training: A systematic review and meta-analysis of exercise to reduce cardiovascular risk in adults with metabolic syndrome. Atherosclerosis 2018, 274, 162–171. [Google Scholar] [CrossRef]
- Ostman, C.; Smart, N.A.; Morcos, D.; Duller, A.; Ridley, W.; Jewiss, D. The effect of exercise training on clinical outcomes in patients with the metabolic syndrome: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2017, 16, 110. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, K.; Sato, S.; Ohira, T.; Maeda, K.; Noda, H.; Kubota, Y.; Nishimura, S.; Kitamura, A.; Kiyama, M.; Okada, T.; et al. The joint impact on being overweight of self-reported behaviors of eating quickly and eating until full: Cross sectional survey. Br. Med. J. 2008, 337, a2002. [Google Scholar] [CrossRef] [Green Version]
- Yamane, M.; Ekuni, D.; Mizutani, S.; Kataoka, K.; Sakumoto-Kataoka, M.; Kawabata, Y.; Omori, C.; Azuma, T.; Tomofuji, T.; Iwasaki, Y.; et al. Relationships between eating quickly and weight gain in Japanese university students: A longitudinal study. Obesity 2014, 22, 2262–2266. [Google Scholar] [CrossRef]
- Iwasaki, T.; Hirose, A.; Azuma, T.; Ohashi, T.; Watanabe, K.; Obora, A.; Deguchi, F.; Kojima, T.; Isozaki, A.; Tomofuji, T. Association between eating behavior and poor glycemic control in Japanese adults. Sci. Rep. 2019, 9, 3418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paz-Graniel, I.; Babio, N.; Mendez, I.; Salas-Salvadó, J. Association between eating speed and classical cardiovascular risk factors: A cross-sectional study. Nutrients 2019, 11, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, L.; Yang, K.; Huang, F.; Liu, X.; Li, X.; Luo, Y.; Wu, L.; Guo, X. Association between self-reported eating speed and metabolic syndrome in a Beijing adult population: A cross-sectional study. BMC Public Health 2018, 18, 855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurst, Y.; Fukuda, H. Effects of changes in eating speed on obesity in patients with diabetes: A secondary analysis of longitudinal health check-up data. BMJ Open 2018, 8, e019589. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Copeland, J.; Dart, L.; Adams-Huet, B.; James, A.; Rhea, D. Slower eating speed lowers energy intake in normal-weight but not overweight/obese subjects. J. Acad. Nutr. Diet. 2014, 114, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Min, S.H.; Lee, J.H.; Kim, L.K.; Lee, D.H.; Lee, J.E.; Kim, K.M.; Lee, S.; Park, K.C.; Lee, Y.J. Components of metabolic syndrome in Korean adults: A hospital-based cohort at Seoul National University Bundang Hospital. J. Obes. Metab. Syndr. 2019, 28, 118–128. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ASCM’s Guidelines for Exercise Testing and Prescription, 7th ed.; Lippinocott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 237–240. [Google Scholar]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Lee, S.Y.; Park, H.S.; Kim, D.J.; Han, J.H.; Kim, S.M.; Cho, G.J.; Kim, D.Y.; Kwon, H.S.; Kim, S.R.; Lee, C.B.; et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res. Clin. Pract. 2007, 75, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Katagiri, A.; Tsuji, T.; Shimoda, T.; Amano, K. Self-reported rate of eating correlates with body mass index in 18-y-old Japanese women. Int. J. Obes. 2003, 27, 1405–1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Martínez, S.; Sánchez-López, M.; Solera-Martinez, M.; Arias-Palencia, N.; Fuentes-Chacón, R.M.; Martínez-Vizcaíno, V. Physical activity, fitness, and metabolic syndrome in young adults. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 312–321. [Google Scholar] [CrossRef]
- Díez-Fernández, A.; Martínez-Vizcaíno, V.; Torres-Costoso, A.; Cañete García-Prieto, J.; Franquelo-Morales, P.; Sánchez-López, M. Strength and cardiometabolic risk in young adults: The mediator role of aerobic fitness and waist circumference. Scand. J. Med. Sci. Sports 2018, 28, 1801–1807. [Google Scholar] [CrossRef] [PubMed]
- Salonen, M.K.; Wasenius, N.; Kajantie, E.; Lano, A.; Lahti, J.; Heinonen, K.; Räikkönen, K.; Eriksson, J. Physical activity, body composition and metabolic syndrome in young adults. PLoS ONE 2015, 10, e0126737. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Kim, S.U.; Kang, H.S. Low cardio/respiratory fitness as an independent predictor of metabolic syndrome in Korean young men. Eur. J. Appl. Physiol. 2010, 108, 633–639. [Google Scholar] [CrossRef]
- Kim, D.; Kim, J.; Lee, M.; Lee, H.; Lee, J.; Jeon, S.Y. The relationship between fitness, BMI and risk factors of metabolic syndrome among university students in Korea. Korean J. Obes. 2012, 21, 99–107. [Google Scholar] [CrossRef]
- Ahn, S.H.; Um, Y.J.; Kim, Y.J.; Kim, H.J.; Oh, S.W.; Lee, C.M.; Kwon, H.; Joh, H.K. Association between physical activity levels and physical symptoms or illness among university students in Korea. Korean J. Fam. Med. 2016, 37, 279–286. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Quintero, A.P.; Hernández, E.; Correa-Bautista, J.E.; Izquierdo, M.; Tordecilla-Sanders, A.; Prieto-Benavides, D.; Sandoval-Cuellar, C.; González-Ruíz, K.; Villa-González, E.; et al. Active commuting to and from university, obesity and metabolic syndrome among Colombian university students. BMC Public Health 2018, 18, 523. [Google Scholar] [CrossRef] [Green Version]
- Henriksson, H.; Henriksson, P.; Tynelius, P.; Ekstedt, M.; Berglind, D.; Labayen, I.; Ruiz, J.R.; Lavie, C.J.; Ortega, F.B. Cardiorespiratory fitness, muscular strength, and obesity in adolescence and later chronic disability due to cardiovascular disease: A cohort study of 1 million men. Eur. Heart J. 2020, 41, 1503–1510. [Google Scholar] [CrossRef]
- Jang, I.; Kim, J.S. Risk of cardiovascular disease related to metabolic syndrome in college students: A cross-sectional secondary data analysis. Int. J. Environ. Res. Public Health 2019, 16, 3708. [Google Scholar] [CrossRef] [Green Version]
- Konopka, A.R.; Asante, A.; Lanza, I.R.; Robinson, M.M.; Johnson, M.L.; Dalla Man, C.; Cobelli, C.; Amols, M.H.; Irving, B.A.; Nair, K.S. Defects in mitochondrial efficiency and H2O2 emissions in obese women are restored to a lean phenotype with aerobic exercise training. Diabetes 2015, 64, 2104–2115. [Google Scholar] [CrossRef] [Green Version]
- Solomon, T.P.; Malin, S.K.; Karstoft, K.; Knudsen, S.H.; Haus, J.M.; Laye, M.J.; Kirwan, J.P. Association between cardiorespiratory fitness and the determinants of glycemic control across the entire glucose tolerance continuum. Diabetes Care 2015, 38, 921–929. [Google Scholar] [CrossRef] [Green Version]
- Genders, A.J.; Holloway, G.P.; Bishop, D.J. Are alterations in skeletal muscle mitochondria a cause or consequence of insulin resistance? Int. J. Mol. Sci. 2020, 21, 6948. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, D. Effects of aerobic exercise on lipids and lipoproteins. Lipids Health Dis. 2017, 16, 132. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.; Unoki, H.; Kojima, N.; Sun, H.; Shimoyamada, H.; Deng, H.; Okazaki, M.; Shikama, H.; Yamada, N.; Watanabe, T. Overexpression of lipoprotein lipase in transgenic rabbits inhibits diet-induced hypercholesterolemia and atherosclerosis. J. Biol. Chem. 2001, 276, 40071–40079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, D.J.; Maiorana, A.; O’Driscoll, G.; Taylor, R. Effect of exercise training on endothelium-derived nitric oxide function in humans. J. Physiol. 2004, 561, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Nosarev, A.V.; Smagliy, L.V.; Anfinogenova, Y.; Popov, S.V.; Kapilevich, L.V. Exercise and NO production: Relevance and implications in the cardiopulmonary system. Front. Cell Dev. Biol. 2015, 2, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavie, C.J.; Church, T.S.; Milani, R.V.; Earnest, C.P. Impact of physical activity, cardiorespiratory fitness, and exercise training on markers of inflammation. J. Cardiopulm. Rehabil. Prev. 2011, 31, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Wedell-Neergaard, A.S.; Krogh-Madsen, R.; Petersen, G.L.; Hansen, Å.M.; Pedersen, B.K.; Lund, R.; Bruunsgaard, H. Cardiorespiratory fitness and the metabolic syndrome: Roles of inflammation and abdominal obesity. PLoS ONE 2018, 13, e0194991. [Google Scholar] [CrossRef] [PubMed]
- Ramires, V.V.; Dumith, S.C.; Gonçalves, H. Longitudinal association between physical activity and body fat during adolescence: A systematic review. J. Phys. Act. Health 2015, 12, 1344–1358. [Google Scholar] [CrossRef] [PubMed]
- Augestad, L.B.; Jiang, L. Physical activity, physical fitness, and body composition among children and young adults with visual impairments: A systematic review. Br. J. Vis. Impair. 2015, 33, 167–182. [Google Scholar] [CrossRef]
- Dong, J.Y.; Ikehara, S.; Kimura, T.; Cui, M.; Kawanishi, Y.; Kimura, T.; Ueda, K.; Iso, H.; The Japan Environment and Children’s Study Group. Self-reported eating speed and incidence of gestational diabetes mellitus: The Japan environment and children’s study. Nutrients 2020, 12, 1296. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Cai, L.; Ma, J.; Ma, Y.; Jing, J.; Chen, Y. Eating fast is positively associated with general and abdominal obesity among Chinese children: A national survey. Sci. Rep. 2018, 8, 14362. [Google Scholar] [CrossRef]
- Argyrakopoulou, G.; Simati, S.; Dimitriadis, G.; Kokkinos, A. How important is eating rate in the physiological response to food intake, control of body weight, and glycemia? Nutrients 2020, 12, 1734. [Google Scholar] [CrossRef]
- Lee, S.; Ko, Y.; Kwak, C.; Yim, E. Gender differences in metabolic syndrome components among the Korean 66-year-old population with metabolic syndrome. BMC Geriatr. 2016, 16, 27. [Google Scholar] [CrossRef] [Green Version]
- Yi, Y.; An, J. Sex differences in risk factors for metabolic syndrome in the Korean population. Int. J. Environ. Res. Public Health 2020, 17, 9513. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Total (n = 1183) | Females (n = 351) | Males (n = 832) | p Value |
|---|---|---|---|---|
| Age (years) | 23.2 ± 2.6 | 21.4 ± 2.0 | 24.0 ± 2.4 | <0.001 |
| BMI (kg/m2) | 22.2 ± 3.0 | 20.4 ± 2.5 | 23.0 ± 2.8 | <0.001 |
| Body fat (%) | 21.2 ± 5.4 | 24.5 ± 4.3 | 19.7 ± 5.2 | <0.001 |
| WHR | 0.83 ± 0.05 | 0.80 ± 0.05 | 0.85 ± 0.05 | <0.001 |
| WC (cm) | 79.8 ± 8.1 | 74.3 ± 6.5 | 82.1 ± 7.6 | <0.001 |
| VO2max (mL/kg/min) | 43.4 ± 8.8 | 36.0 ± 5.5 | 46.6 ± 8.0 | <0.001 |
| Smoking, n (%) | 415 (35.1) | 27 (7.7) | 388 (46.6) | <0.001 |
| Alcohol intake, n (%) | 884 (74.7) | 199 (56.7) | 685 (82.3) | <0.001 |
| SBP (mmHg) | 116.6 ± 13.5 | 106.3 ± 10.3 | 121.0 ± 12.2 | <0.001 |
| DBP (mmHg) | 68.5 ± 8.6 | 64.1 ± 7.4 | 70.3 ± 8.5 | <0.001 |
| FBG (mg/dL) | 97.0 ± 12.8 | 93.7 ± 11.5 | 98.3 ± 13.1 | <0.001 |
| TG (mg/dL) | 103.1 ± 52.1 | 82.4 ± 31.4 | 111.9 ± 56.4 | <0.001 |
| HDLC (mg/dL) | 48.8 ± 14.5 | 55.7 ± 14.7 | 45.9 ± 13.4 | <0.001 |
| Mets (n, %) | 104 (8.8) | 12 (3.4) | 92 (11.1) | <0.001 |
| Variable | Eating Speed | Physical Activity | Cardiorespiratory Fitness | |||
|---|---|---|---|---|---|---|
| Slow | Fast | Active | Inactive | Fit | Unfit | |
| Age (years) | 23.0 ± 2.5 | 23.6 ± 2.6 ** | 23.2 ± 2.6 | 23.2 ± 2.5 | 23.1 ± 2.5 | 23.8 ± 2.6 ** |
| BMI (kg/m2) | 21.7 ± 2.8 | 23.3 ± 3.0 ** | 22.4 ± 2.6 | 22.1 ± 3.2 | 21.8 ± 2.6 | 24.0 ± 3.8 ** |
| Body fat (%) | 20.9 ± 5.5 | 21.6 ± 5.2 * | 20.6 ± 5.1 | 21.2 ± 5.6 * | 20.3 ± 5.2 | 24.2 ± 5.0 ** |
| WHR | 0.83 ± 0.05 | 0.85 ± 0.05 ** | 0.83 ± 0.05 | 0.83 ± 0.05 | 0.83 ± 0.05 | 0.86 ± 0.05 ** |
| WC (cm) | 78.4 ± 7.7 | 82.5 ± 8.2 ** | 79.8 ± 7.3 | 79.9 ± 8.7 | 78.4 ± 7.0 | 85.0 ± 9.9 ** |
| Current/past smokers (n, %) | 236 (30.4) | 179 (44.0) ** | 185 (37.4) | 230 (66.6) | 289 (32.5) | 107 (44.0) |
| Alcohol intake (n, %) | 568 (73.2) | 316 (77.6) | 369 (74.7) | 515 (74.7) | 654 (73.5) | 189 (77.8) |
| SBP (mmHg) | 115.1 ± 13.3 | 119.5 ± 13.4 ** | 117.4 ± 13.2 | 116.1 ± 13.7 | 115.5 ± 12.9 | 120.7 ± 15.3 ** |
| DBP (mmHg) | 67.9 ± 8.5 | 69.5 ± 8.8 * | 68.1 ± 7.9 | 68.8 ± 9.1 | 67.8 ± 8.1 | 70.9 ± 10.1 ** |
| FBG (mg/dL) | 96.9 ± 13.2 | 97.1 ± 12.0 | 96.3 ± 11.7 | 97.4 ± 13.5 | 96.3 ± 12.4 | 98.9 ± 13.3 * |
| TG (mg/dL) | 98.1 ± 47.9 | 112.7 ± 58.0 ** | 99.4 ± 48.2 | 105.8 ± 54.5 * | 95.6 ± 43.3 | 130.0 ± 65.7 ** |
| HDLC (mg/dL) | 50.1 ± 14.8 | 46.2 ± 14.5 ** | 49.1 ± 14.4 | 48.5 ± 14.5 | 49.1 ± 14.4 | 47.3 ± 14.8 |
| Metabolic syndrome (n, %) | 55 (7.1) | 49 (12.0) * | 27 (5.5) | 77 (11.2) ** | 43 (4.8) | 59 (24.3) ** |
| Variables | Eating Quickly | Inactive | Unfit | |||
|---|---|---|---|---|---|---|
| Crude OR (95% CI) | Adjusted OR (95% CI) | Crude OR (95% CI) | Adjusted OR (95% CI) | Crude OR (95% CI) | Adjusted OR (95% CI) | |
| Mets | 1.794 * (1.196–2.691) | 1.416 (0.928–2.160) | 2.403 ** (1.503–3.841) | 2.176 * (1.381–3.429) | 6.316 ** (4.133–9.652) | 5.500 ** (3.546–8.528) |
| Abdominal obesity | 2.708 ** (1.916–3.826) | 2.292 ** (1.600–3.282) | 1.846 * (1.268–2.687) | 1.710 * (1.187–2.464) | 7.444 ** (5.143–10.775) | 6.855 ** (4.680–10.041) |
| Elevated BP | 1.717 (0.955–3.084) | 1.370 (0.751–2.499) | 2.319 * (0.939–1.216) | 2.150 * (1.104–4.185) | 3.273 ** (1.799–5.955) | 2.808 * (1.498–5.265) |
| Elevated FBG | 0.953 (0.743–1.222) | 0.785 (0.604–1.020) | 1.281 * (0.999–1.643) | 1.217 (0.956–1.548) | 1.450 * (1.087–1.935) | 1.378 * (1.022–1.859) |
| Elevated TG | 1.989 ** (1.426–2.773) | 1.486 * (1.053–2.098) | 1.470 * (1.033–2.091) | 1.301 (0.925–1.828) | 3.783 ** (2.650–5.399) | 3.533 ** (2.426–5.144) |
| Reduced HDLC | 1.381 * (1.077–1.771) | 1.391 * (1.074–1.800) | 1.310 * (1.022–1.678) | 1.273 (0.997–1.625) | 1.274 (0.952–1.706) | 1.253 (0.931–1.688) |
| Variables | β | Chi-Square | Adjusted OR (95% CI) | p Value | |
|---|---|---|---|---|---|
| Eating quickly | No | Reference | |||
| Yes | 0.523 | 5.591 | 1.687 (1.094–2.601) | 0.018 | |
| Physical activity | Active | Reference | |||
| Inactive | 0.510 | 4.231 | 1.666 (1.024–2.708) | 0.040 | |
| Physical fitness | Fit | Reference | |||
| Unfit | 1.682 | 56.981 | 5.378 (3.475–8.325) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.; Joo, M.; Hong, H.; Kang, H. Eating Speed, Physical Activity, and Cardiorespiratory Fitness Are Independent Predictors of Metabolic Syndrome in Korean University Students. Nutrients 2021, 13, 2420. https://doi.org/10.3390/nu13072420
Kang M, Joo M, Hong H, Kang H. Eating Speed, Physical Activity, and Cardiorespiratory Fitness Are Independent Predictors of Metabolic Syndrome in Korean University Students. Nutrients. 2021; 13(7):2420. https://doi.org/10.3390/nu13072420
Chicago/Turabian StyleKang, Minjeong, Mingyu Joo, Haeryun Hong, and Hyunsik Kang. 2021. "Eating Speed, Physical Activity, and Cardiorespiratory Fitness Are Independent Predictors of Metabolic Syndrome in Korean University Students" Nutrients 13, no. 7: 2420. https://doi.org/10.3390/nu13072420
APA StyleKang, M., Joo, M., Hong, H., & Kang, H. (2021). Eating Speed, Physical Activity, and Cardiorespiratory Fitness Are Independent Predictors of Metabolic Syndrome in Korean University Students. Nutrients, 13(7), 2420. https://doi.org/10.3390/nu13072420